Performance Report – July 2015 - Hinchingbrooke Health Care NHS

V
Oversight – Performance
Report
23 July 2015
June reporting period
Overview
The purpose of this presentation is to provide context/word so support the performance of the metrics reported in CQC Dashboard in response to address the compliance areas of the
CQC Action Plan as listed below:
•
Compliance Action 1 : Staffing
•
Compliance Action 2 : Care and Welfare of People
•
Compliance Action 3 : Assessing and Monitoring
•
Compliance Action 4 : Safeguarding
•
Compliance Action 5 : Infection Control
•
Compliance Action 6 : Respecting and involving patients
•
Must Do’s
•
Should Do’s
Oversight Report
Published Data for June 2015
Version 1.4
Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Total
ID
3
4
9
Compliance Action 2 - Care amd Welfare of People
Mixed Sex Breaches
PEWS Observation Completion - 20% sample patients.
MEWS and MEOWs completion
No. of pressure Ulcers on all wards
10 Fluid chart compliance
11
15
17
Metric
% of delegates Completed HII catheter Training,
% of delegates attending improving water low training,
% of delegates Completed HII VIP training
No. of HCAI Cdif
No. of MRSA
% of catheter related UTI's - All
Target Notes
1
6
7
12
Compliance Action 1 - Staffing
% of Paed staff working in department from 7am to 12pm in line with required number
% of Child ED arrival to assessment within 15 Mins
No. of Clinical CAMH Breaches - ED
PLANNED V ACTUAL for all Nursing Staff (to show staffing arrangements in place to meet needs of patients) Perm +
Agency
Contract Hours % greater 80% ( green ) Percentage of Patients
0 greater 90% ( green ) HCA
( Contract Hours % )
13
32
Staff Turnover by Professional Group
No. of staff attending QELCA Training
(Quality End of Life Care for all) greater 90% ( green ) Nursing & Midwifery
( Contract Hours % )
Less 10% ( green ) Medical & dental
Less 10% ( green ) Nursing & midwifery
Less 10% ( green ) Other clinical incl HCAs
Less 10% ( green ) Non-clinical greater 2 ( green )
Trajectory
Target 2 per month, YTD 25
N/A 74.00% 81.00% 80.00%
92.41% 87.59% 87.37% 78.58% 80.40% 84.38%
0 0 1 2 3 0
114.49% 113.23% 93.53% 107.22% 110.74% 109.37%
101.06% 96.30% 103.00% 100.98% 97.59% 97.66%
11.04% 10.91% 10.53% 10.23% 11.11% 11.17%
9.62% 10.82% 12.09% 13.05% 12.68% 11.78%
17.86% 18.11% 17.48% 12.88% 13.32% 13.76%
15.90% 15.55% 17.74% 18.39% 20.73% 19.91%
5 0 4
0 greater 95% ( green )
0 0 0 1 0 1
96.00%
greater 80% (green) Data collection has commenced in May
0 Avoidable ( 1/2)
0
100%
Avoidable ( 3/4)
Data collection has commenced in May. Initial 2 wards
YTD 11
0
Includes SKINN Training
Employee Mapping underway, % data due June.
No of Cases
No of Cases
1
0
1
0
2
0
2
0
1
0
83.00%
0
0
87.00%
2
0
0
0
0
0
1.29% 2.94% 2.90%
40.29% 43.17% 42.30%
21
0
0
0.82% 1.50% 1.69% 4.51%
59
0
0
3.30%
95
1
0
6.51%
5 2 2 2 2 2
78.33%
85.12%
6
108.10%
99.43%
10.83%
11.67%
15.57%
18.04%
9
2
96.00%
83.00%
7
0
87.00%
2.38%
41.73%
95
3
0
3.06%
% of catheter related UTI's - New 1% 0.00% 0.77% 0.42% 1.23% 0.47% 0.93% 0.64%
18
19
% compliance with Ward Audit - Recording of Waterlow
DNAR audit - Engagement with Carers
Data collection has commenced in May
greater 80% ( green) Available from April, 2
Monthly
73.00%
93.00%
90.00% 81.50%
24
25
Compliance Action 3 - Assessing and Monitoring
No. of complaints at Local level and progressing to ombudsman Level
No. of incidents reported monthly
New cases in the month that the Trust is aware of.
Acute Medicine
Theatres & Critical Care
ISMR
GI & GS
EENT
Musculoskeletal
Womens Services
Support Services
Non-Clinical Services
0
6
46
61
5
12
94
39
91
43
0
4
52
43
8
6
65
28
67
50
0
9
35
72
18
11
88
34
54
48
0
3
47
37
10
10
98
26
49
46
0
13
39
82
12
15
121
32
60
49
0
10
44
79
18
13
93
39
51
48
0 0 0 0 0 0 0
45
263
374
71
67
559
198
372
284
21
Compliance Action 4 - Safeguarding
% of delegates attending MCA and DoLs Training
22 Adult Safeguarding Audit completion
16
Compliance Action 5 - Infection Control
Compliance with Handwashing Audit - (Unchallenged 5 minutes of Handwashing)
5
20
2
Compliance Action 6 - Respecting and Involving People
Response to Call Bells ( inside 2 mins )
Fluid and Nutrition Assessments for Adults ( screening )
23
Audit of Intentional Rounding Document
Friends and Family Test Responses received - Emergency
Friends and Family Test Responses received - Maternity
Friends and Family Test Responses received - In patients
Friends and Family satisfaction score - Emergency
Friends and Family satisfaction score - Maternity
Friends and Family satisfaction score - In patients
Quarterly YTD
Trajectory
Quarterly - report being collated.
0%
30%
57.00%
26%
35%
44%
44%
48%
48%
66.00%
51%
44%
56%
54% 63% 70% 80% 90%
38%
100% 100%
66.00%
greater 80% ( green
)
Audits greater 90% ( green ) Audits greater 90% ( green ) Qrtly - All Wards greater 80% ( green ) Data collection has commenced in May
Response Rates
Response Rates
Response Rates
99.19% 99.21% 99.75% 100.00% 100.00% 100.00%
91.98% 97.37% 95.83% 98.81% 96.25% 98.04%
91% 93%
86.00% 80.00%
10.00% 13.00% 14.00% 13.00% 17.00% 23.68%
40.00% 11.00% 75.00% 74.00% 55.00% 64.64%
41.00% 53.00% 43.00% 43.00% 47.00% 52.82%
94.00% 94.00% 95.32%
98.00% 97.00% 97.44%
97.00% 96.00% 95.77%
90%
99.69%
96.38%
100% 92.00%
83.00%
15.11%
53.27%
46.64%
94.44%
97.48%
96.26%
31 Compliance against Training needs Analysis for statutory, mandatory and essential clinical skills training greater 90% ( green ) IPC Refresher
(Clinical Staff) - 1 Year greater 90% ( green ) IPC Refresher
(Non Clinical Staff) - 2 Years greater 90% ( green ) M&H High Risk (Non Clinical)
Practical + Theory - 2 Year greater 90% ( green ) M&H Low Risk (Clinical)
Practical + Theory - 2 Year greater 90% ( green ) M&H Low Risk (Non Clinical) e-learning - 3 Year greater 90% ( green ) Moving & Handling for
People Handlers - 1 Year greater 90% ( green ) Fire Safety - 1 Year greater 90% ( green ) Mental Capacity Act - 3 Years greater 90% ( green ) Prevent Basic Awareness - 3
Years greater 90% ( green ) PREVENT - 3 Years greater 90% ( green ) Safeguarding Adults Level 1 -
3 Years greater 90% ( green ) Safeguarding Children Level 1
- 3 Years greater 90% ( green ) Safeguarding Children Level 2
- 1 Year greater 90% ( green ) Equality, Diversity and
Human Rights - 3 Years greater 90% ( green ) Information Governance - 1
Year
New dashboard available with July data
86.26% 82.57% 83.06%
98.25% 97.25% 97.45%
20.54% 19.23% 19.23%
38.19% 76.17% 76.39%
92.15% 96.46% 96.68%
58.19% 69.59% 70.86%
83.44% 81.35% 82.61%
46.66% 49.89% 50.32%
17.55% 17.89% 18.10%
27.88% 26.21% 26.47%
92.77% 93.61% 94.18%
95.92% 95.89% 96.36%
78.19% 54.75% 55.16%
89.97% 90.26% 90.60%
85.60% 85.40% 85.90%
26
27
28
29
30
33
34
Must Do
% of wards reporting Drug Cupboard/Trolley secure
Compliance with Medicine Administration Audits
Medicines Audit - Security/Storage
Medicines Audit - Clinical safety/Admin
Drug fridge temps and range incorrect daily – monthly aggregate
Medication omissions
% of completed appraisals
% of Doctors Revalidation
Should Do
Compliance with daily Resuscitation Equipment Checks
(Audit)
No. of avoidable transfers in the Trust after 10pm.
greater 90% ( green ) Audits greater 90% ( green ) Quarterly greater 90% ( green ) Quarterly greater 80% ( green ) Initial Data from 4 wards, then from all wards
Drugs not given greater 80% ( green )
98.93% 98.03% 98.21% 98.15% 95.00% 96.08%
74.00% 78.00%
88.00% 97.00%
96.00% 83.00%
18 9 11 4 14 11
56.00% 76.00% 91.00% 84.34% 80.00% 75.60%
100% greater 90% ( green ) Specific wards each month.
All wards each Quarter.
Number of Moves 89 82 70
95.00% 83.00% 89.00%
80 34 55
97.40%
76.00%
92.50%
89.50%
67
77.16%
100%
89.00%
410
Ward Dashboard
Indicator
Percentage of compliance with hand hygiene standards
Compliance with sharps audit
Compliance with outcome 8 standards
Compliance with saving lives urinary catheter care bundle
VTE Assessment score
Prophylaxis score
Staff appraisals (by all groups)
Sickness (by all groups)
Staff mandatory training (by professional group)
Percentage of relevant staff trained in safeguarding children processes (by professional group and level of training)
Percentage of relevant staff trained in safeguarding adults processes, including Mental Capacity Act
Audit score documentation standards
Number of medication incidents
Central Venous Catheter - Insertion
Central Venous Catheter - Ongoing
Peripheral Lines
Peripheral Lines Ongoing
Ventilated Pats - Ongoing
Ventilated Pats - Observe
Urinary Cathater Insertion
Urinary Cathater Ongoing
Red Apple Tree
Red < 90% 100.00%
Red < 90% 92.00%
Red < 85% 95.00%
Red < 90% 95.00%
Red < 100% 100.00%
Red < 100%
Red < 75% 49.00%
Red > 4% 5.57%
Red < 75% 77.00%
Red < 75% 91.00%
Red < 75% 81.00%
Red <60% 80.00%
Red > 3 1
Red < 95%
Red < 95%
Red < 95% 95.00%
Red < 95% 95.00%
Red < 95%
Red < 95%
Red < 95% 100.00%
Red < 95% 90.00%
ATSU Birch
95.00%
CCU
100.00%
92.00%
Cherry Tree OutPatients PRUNET Short Stay Walnut
97.00%
100.00% 100.00% 100.00%
100.00%
100.00%
94.00%
100.00%
95.00%
100.00%
100.00%
100.00%
100.00%
100.00%
92.00%
100.00%
96.00% 88.31% 100.00% 100.00%
100.00% 100.00%
90.00%
4.41%
100.00%
73.00%
5.46%
87.00%
85.00%
98.00%
90.00%
95.00%
100.00%
100.00%
80.00%
4.00%
90.00%
96.00%
94.00%
80.00%
88.00%
100.00% 100.00% 100.00% 100.00% 90.00%
100.00% 100.00% 100.00% 100.00%
100.00%
0
95.00%
0
80.00%
1
100.00%
100.00%
100.00% 100.00% 100.00%
100.00% 100.00% 100.00%
100.00%
100.00%
100.00% 100.00% 100.00%
100.00% 100.00% 100.00%
1
90.00%
100.00%
0
95.00% 80.00%
4
100.00% 100.00% 100.00%
100.00% 100.00% 100.00%
100.00% 100.00% 100.00%
100.00% 100.00%
Staffing
Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15
ID
13
Metric
Staff Turnover by Professional Group
Target Notes
Less 10% ( green ) Medical & dental
Less 10% ( green ) Nursing & midwifery
Less 10% ( green ) Other clinical incl HCAs
Less 10% ( green ) Non-clinical
11.04% 10.91% 10.53% 10.23% 11.11% 11.17%
9.62% 10.82% 12.09% 13.05% 12.68% 11.78%
17.86% 18.11% 17.48% 12.88% 13.32% 13.76%
15.90% 15.55% 17.74% 18.39% 20.73% 19.91%
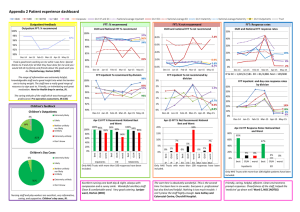
Actions taken
• In the period April to June 19 exit surveys have been completed ; 1-2 years was the most common length of service (31.58%) with 6-12 months being the second most common (26.32%) We are starting a campaign to ensure more exit interviews are completed.
• Main 5 reasons for leaving were - better career opportunities, higher pay, career change, take up training/education and improved work life balance. Staff friendliness and colleague appreciation both scored 100% and 73.68% would recommend Hinchingbrooke as an employer.
• Internal Recruitment and Retention Surveys are being set up.
• Successful recruitment campaign for Band 5 ward based nurses in Italy has resulted in 16 offers of employment, 12 of which will be joining the Trust during July / August and the remainder in October.
• A recruitment team will be travelling to the Philippines at the end of August, looking to recruit 45 nurses in three cohorts from April 2016.
• HCAs fully established - not currently in post - 31 going through recruitment process starting between July and August.
• Establishment of Workforce Effectiveness Project to address attraction, retention with a view to reducing temporary staff spend.
• “Grow our own” – collaborative with Health Education England
Care and Welfare of People
ID Metric
Mixed Sex Breaches
Target
0
Notes
Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15
0 0 0 1 0 1
Issue
Single sex breach occurred on CCC as no bed to transfer patients to and delay in recognition of issue by nurse in charge of CCC on the day.
Action taken
Flow chart devised with easy to follow actions and awareness of issue raised within CCC.
Now located in new unit with individual rooms, so no single sex breaches will occur in future
Care and Welfare of People
ID
10
Metric
Fluid chart compliance
Target
100%
Notes
Data collection has commenced in May. Initial 2 wards
Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15
87.00%
Fluid Chart Compliance
The Trust is undertaking a phased implementation of an electronic system for capturing patient observations via electronic handover tool. Additionally the Trust is implementing an electronic dashboard to capture clinical KPI’s from ward to board level.
The fluid balance documentation assessment was rolled out on two wards in June, four wards in July, and the remaining wards in August.
The implementation of these solutions, will improve metric collation and ultimately patient observation tracking on the wards. It is anticipated that live alerts will be functional as soon as mobile phones are purchased.
Care and Welfare of People
ID Metric
No. of MRSA
Target
0
Notes
No of Cases
Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15
0 0 0 0 0 0
Number of MRSA
The one MRSA that was reported in April 2015 has been removed following arbitration with NHS England as unavoidable.
Care and Welfare of People
ID
15
Metric
No. of HCAI Cdif
Target
YTD 11
Notes
No of Cases
Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15
2 0 0 0 0 1
Issue:
This years target is from April to end March. According to our monthly trajectory we are below the ceiling.
At the end of July we have had no more than 5 cases. To date we have reported 2.
Action taken
C.diff policy reviewed and implemented.
Isolation policy reviewed and implemented.
IPCN allocated specific wards and visit all patients with diarrhoea every day to support and guide staff.
Respecting and Involving People
ID
31
Metric
Compliance against Training needs Analysis for statutory, mandatory and essential clinical skills training
Target Notes greater 90% ( green ) IPC Refresher
(Clinical Staff) - 1 Year greater 90% ( green ) M&H High Risk (Non Clinical)
Practical + Theory - 2 Year greater 90% ( green ) M&H Low Risk (Clinical)
Practical + Theory - 2 Year greater 90% ( green ) Moving & Handling for
People Handlers - 1 Year greater 90% ( green ) Fire Safety - 1 Year
Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15
86.26% 82.57% 83.06%
20.54% 19.23% 19.23%
38.19% 76.17% 76.39%
58.19% 69.59% 70.86%
83.44% 81.35% 82.61% greater 90% ( green ) Mental Capacity Act - 3 Years greater 90% ( green ) Prevent Basic Awareness - 3
Years greater 90% ( green ) PREVENT - 3 Years
46.66% 49.89% 50.32%
17.55% 17.89% 18.10%
27.88% 26.21% 26.47% greater 90% ( green ) Safeguarding Children Level 2
- 1 Year greater 90% ( green ) Information Governance - 1
Year
78.19% 54.75% 55.16%
85.60% 85.40% 85.90%
Respecting and Involving People
Assignm ents for
Positions w ith
Com petence
Requirem ents
% Assignm ents that Fulfil
Com petence
Requirem ents for
Position
Notes:
Com petence Nam e
291|LOCAL|IPC Refresher (Clinical Staff) - 1 Year|
291|LOCAL|IPC Refresher (Non Clinical Staff) - 2 Years|
291|LOCAL|M&H Low Risk (Non Clinical) e-learning - 3 Year|
291|LOCAL|M&H High Risk (Non Clinical) Practical + Theory - 2 Year|
291|LOCAL|M&H Low Risk (Clinical) Practical + Theory - 2 Year|
NHS|MAND|Moving & Handling for People Handlers - 1 Year|
NHS|MAND|Fire Safety - 1 Year|
NHS|MAND|Inform ation Governance - 1 Year|
NHS|MAND|Equality, Diversity and Hum an Rights - 3 Years|
NHS|MAND|Safeguarding Children Level 1 - 3 Years|
NHS|MAND|Safeguarding Children Level 2 - 1 Year|
NHS|MAND|Safeguarding Adults Level 1 - 3 Years|
NHS|MAND|Mental Capacity Act - 3 Years|
291|LOCAL|Prevent Basic Aw areness - 3 Years|
NHS|MAND|PREVENT - 3 Years|
1,214
473
426
76
215
977
1,709
1,709
1,709
1,709
1,228
1,709
923
1,709
105
82.21%
96.83%
95.77%
18.42%
76.74%
74.62%
80.81%
83.73%
88.82%
95.79%
57.41%
92.98%
59.15%
19.37%
25.71%
Recovery will be via intense communication. We need to check the mapping for accuracy elearning in place elearning in place
Change of competence and frequency. Communication required. Remapping for accuracy required
Change of competence and frequency. Communication required. Remapping for accuracy required
Remapping for accuracy required. Currently increasing capacity to ensure adequate provision
Fire Safety for Non Clinical Staff moved to E Learning - communication complete.
Scheduled onto Partnership Days.
Elearning and self assessment booklet available. Communication complete for nonclinical staff
Elearning and self assessment booklet available. Communication complete for nonclinical staff
Compliant
Only applicable to staff with regular clinical patient contact . We need to check the mapping accuracy for this group. Elearning also availlable.
Compliant
Target of 90% is by October. Currently exceeding trajectory
New competency. Compliance required by 2017. Elearning package to be introduced
Only required by personnel who need safeguarding children level 3. Compliance required by 2017
Data run - 17.07.15
We have recently revised our whole Training Needs Analysis to ensure that staff attend the appropriate training and have appropriate refresher periods suitable to their requirements
We have begun to undertake intensive communication to all staff and the redeveloped Statutory, Mandatory and Essential Training day has begun.
We are doing a final check that we have the competencies mapped to the correct personnel and from the 1 July 2015 we will be doing a campaign to raise awareness about what people need to do, when and how so that the compliance increases. Obviously when new competencies have been introduced we are playing "catch up" and we are looking at flexible ways of learning so that we can produce training trajectories.
There have been some identified issues in respect of mapping accuracy and further intensive work is commencing to review original mapping. Inaccurate mapping can affect compliance rates, therefore there will be some adjustments.
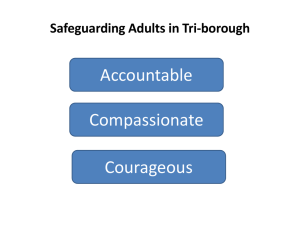
Safeguarding
ID
21
Metric
Compliance Action 4 - Safeguarding
% of delegates attending MCA and DoLs Training
Target Notes
Quarterly YTD
Trajectory
MCA & DOLS Compliance – 30 June 2015
Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15 Jul-15 Aug-15 Sep-15 Oct-15 Nov-15 Dec-15 Total
0%
30%
26%
35%
44%
44%
48%
48%
51%
44%
56%
54% 63% 70% 80% 90% 100% 100%
38%
Safeguarding
• Restrictive physical intervention – covered under mandatory MCA/DoLs Training
• Best Interest decisions and Advocacy service for patients - emphasised during training to reduce variation
January – Cycle 1 & July Audit Cycle 2
Control Measure
Awareness of types of abuse and indicators
How to make a referral
Understanding of restrictive physical intervention
Aware of the Intranet pages
Awareness of who to contact for advice.
How to access the Mental Capacity Act and DOLs procedure
How and when to perform a mental capacity assessment
Jan 2015
100%
100%
27%
82%
91%
45%
0%
June 2015
100%
100%
45%
Trust wide training compliance For
MCA/DOLS
January 22%
June 2015 51%
July 2015 56%
(Trajectory for July was set at 54%)
82%
82%
64%
45%
64%
55%
How to make a best interests decision for a patient who lacks capacity.
How to access the advocacy service for patients who are vulnerable
When DoLs Safeguards should be considered and who should be contacted
45%
18%
36%
55%
Must Do
ID
27
Metric
Compliance with Medicine Administration Audits
Medicines Audit - Security/Storage
Target Notes greater 90% ( green ) Quarterly
Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15
74.00% 78.00%
Issue:
1.
Retaining straps for drug trolleys not available (on order – awaiting delivery)
2.
Medicine cupboard and fridge doors left unlocked on three wards (3 wards out of 12)
3.
Medicines left unattended on work surfaces (isolated incident)
Action taken:
1.
Straps ordered by Facilities to be fitted when delivered to trust.
2.
Policy requirements highlighted on all wards. Performance monitored at Senior Nurse Meetings with sanctions as per Trust Policy. Pharmacy staff raising issues with senior nurses during visits.
3.
Action in place to ensure Lockable TTO cupboards on all wards. Ordered and awaiting delivery
4.
New secure pharmacy returns bins to be installed. Currently on order and awaiting delivery.
5.
From July Pharmacy now undertaking monthly medicine storage and security audits across all wards reporting through nurse management & medication safety committee
Must Do
ID
28
Metric Target Notes
Drug fridge temps and range incorrect daily – monthly aggregate greater 90% ( green ) Initial Data from 4 wards, then from all wards
Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15
96.00% 83.00%
Issue:
1.
Awareness of daily monitoring requirement
Action taken:
1.
Fridge temperature monitoring form updated with escalation process and requirement for daily monitoring
2.
Pharmacy staff checking compliance with monitoring requirements on ward visits and prompting compliance
3.
Nurse in charge daily checklist implemented in ward areas and monitored as part of the electronic clinical assurance tool/dashboard
4.
Performance monitored at Senior Nurse Meetings with sanctions as per Trust Policy.
Should do
ID
33
Metric
Compliance with daily Resuscitation Equipment Checks
(Audit)
Issue
1.
Compliance with daily checks
Target Notes greater 90% ( green ) Specific wards each month.
All wards each Quarter.
Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15
95.00% 83.00% 89.00%
Action taken
1.
Wards with non compliant areas are rechecked on a monthly basis until performance returns within target
2.
Escalated to Patient Safety Group 14 July 2015
3.
Performance monitored at Senior Nurse Meetings with sanctions as per Trust Policy.
4.
Performance is predicted to be 95% compliant in August
Must Do
ID
34
Metric
No. of avoidable transfers in the Trust after 10pm.
Target Notes
Number of Moves
Jan-15 Feb-15 Mar-15 Apr-15 May-15 Jun-15
89 82 70 80 34 55
SOP introduced 30/4/15
1. The Moving Patients at night SOP was launched formally on 30 April 2015.
2. Escalation is via the Site Manager to GM and a Director on Call
3. Variation in avoidance of moves is directly related to Trust activity and available capacity.
4. The Trust continues to implement improvements associated with ECIST recommendations and management of medically fit in order to create bed capacity earlier in the day
5. Performance improvement is in line with the agreed trajectory as part of our CQINN scheme w/c
06/04/2015
13/04/2015
20/04/2015
27/04/2015
04/05/2015
11/05/2015
18/05/2015
25/05/2015
01/06/2015
08/06/2015
15/06/2015
22/06/2015
29/06/2015
All moves
22
37
23
35
7
14
26
21
31
12
43
33
17
Avoidable moves
11
16
1
2
9
12
25
24
7
9
15
11
15
Q1 cquin target (For July)
20
20
20
20
20
20
20
20
20
20
20
20
20
Variation Report - as at 17 July 2015
Compliance Action
Ref
Area Action Milestone
Development of operational task and finish group
Accountable Responsible
Date to be delivered
Deputy DIPC,
DHON's and Ward
Matrons
28/02/2015
Revised Estimated delivery date
2.1
2.3
Reason for Delay
Complete
The Trust is failing to plan and deliver care that meets the needs of service users who are at risk due to pressure area, catheter care, intravenous care, and the risk associated with bed rails.
Task and Finish group to review current documentation and develop revised format
Three Phased approach:
Complete Revised document
1) Risk Assessment
Complete revised
Complete revised
Midwifwery and
Quality documentation
2) HII's
Director of Nursing, documentation
3) Nursing Care Plans
Deputy DIPC,
DHON's and Ward
Matrons
31/05/2015
31/07/2015
31/07/2015
31/07/2015
Risk Assessment Booklet revised -out for comment. - Comments received and amendments required before going to the printers. Next step will be to work with printers and produce revised Risk Assessment
Booklet, before implemention on wards. revised date for completion of milestone 31
July 2015
HII process reviewed over the last couple of weeks. HIII document to be presented at IIC on
22 July and is on track to be completed by milestone deadline
Action Plan for revision of Nursing Plans received. Milestone on track to deliver.
Monitoring Audit Tool 30/07/2015
Electronic Monitoring Tool in line with the HII and Nursing Care Plans have been revised/developed with support of Information team. To be tested 02/06/2015. Trial, Pilot and rollout 30/7/2015
To Develop a
Strategy for dementia
(BAF 14)
Strategy written and ratified
Ensure action is taken to improve the communication with involved in making decisions regarding treatment, and that these discussions are reflected in
Care Plans. This review should include ED
Engagement with Local
Interested Voluntary Groups
Clinical Lead - ISMR
Led by DHON - ISMR for Trust wide implementation
31/03/2015
31/03/2015
31/03/2015
Strategy produced. Consulation with widerstakeholder group required.
01/08/2015
Health Watch and Alzhiemers Group have reviewed the strategy and have provided positive feedback. Document to be put out for consultation on HHCT website, plus consultation exercise to be undertaken at dementia forum to be held 20 May 2015. Closing date for consultation 30 June 2015. Collation of responses and amendements to policy will be agreed during July with an expected launch date 1 August 2015
Compliance Action
Ref
Area Action Milestone
Review current provision of suitable room
Accountable Responsible
Date to be delivered
Revised Estimated delivery date
31/01/2015
Reason for Delay
AISD6
To review the pathway for
Management of
TOPS
Appropriate environment for the care and treatment of women undergoing TOP within the Acute Service
Area
Produce and Options paper for
Board review
Clinical Lead -
Women's Health
Clinical Lead - ED and Emergency
Medicine/ Lead
Consultant - Early
Pregnancy Care
28/02/2015
Options paper discussed at the Women's Health
Clincal Governance July meeting . Proposal for change of pathway to be discussed at
Management Committee on 22 July 2015
Present to Programme Board 30/08/2015
Cherry Tree Ward
Actions following recent Whistleblowing incident
•
Escalated to external stakeholders
•
Registered as Serious Incident
•
Commenced internal HR investigation
•
Duty of candour as appropriate
•
Sanctions as per Trust protocol including exclusion from duty
•
Strengthened Site Management Team/Exec scrutiny
•
Beds reduced from 30 to 20
•
Interim Senior Nurse Leader deployed
•
CPFT Learning and Development support for intensive dementia training
•
Dayroom facilities in development to allow for recreational and diversional activities.
•
Opportunity for developmental /rotational posts with CPFT
•
Exploration of opportunity to develop activity co-ordinators
Further learning from the SI report will be shared following report submission
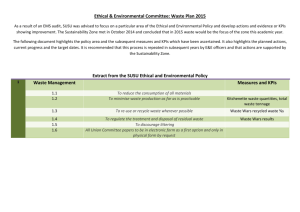
Unannounced Visits, Peer Reviews, Health watch feedback
Analysis against CQC Composite Action Plan
Data period: Sept 2014 to 15 July 2015
CQC CAP
Reference
1.1
2.1
2.1
2.1
2.2
2.2
2.3
3.3
4.1
6.1
6.2
AIMD 2
AIMD 3
AISD 3
Other
Area
Adult Safeguarding
Call Bell
Communication
Documentation
Equipment Checking
Governance
Medicines Adminstration
Medicines Security
Nutrition and Hydration
SHOULD DO
Staff supervision and training
Staffing
Training
Ward Handover process
Other
Occurrences
1
1
1
19
1
3
4
4
8
2
1
1
2
7
27
•
•
•
Hot spots
Medicines Security
Adult Safeguarding
Staffing
The attached report is an analysis of the feedback received from unannounced visits, Peer Reviews, and Health
Watch. This has been analysed against the Actions and Milestones being delivered in the CQC Composite Action
Plan, and therefore are being addressed. The 27 other items are “one off” themes that have been addressed as part of the wider quality improvement agenda.