Gastrointestinal Haemorrhage
advertisement

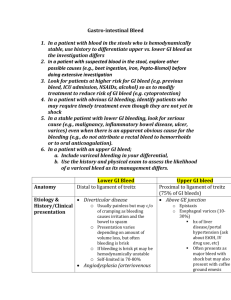
Gastrointestinal Haemorrhage Rebecca Shields Clinical Teaching Fellow UHCW Acute Block Objectives - Outline GI Bleeds Explain the likely causes of upper GI bleeds from history and examination. Demonstrate an understanding of initial management of acute upper GI bleeds Distinguish common causes of lower GI bleeds from history and examination. Initiate appropriate investigations for lower GI bleeds. Assessment of the acutely unwell patient Resuscitation Recognise a GI Bleed History Amount Difficult Usually under estimated Appearance What colours can blood be? Why does it change colour? Duration Associated Sx Risk factors Blood loss exercise Estimate the volume of blood loss in each picture What colour can blood be? Why does it change? Always visible? Colours of Blood Colour Vomit Stool Bright Red √ √ Dark Red x √ Green x x Black x √ Brown √ x? No motion / vomit ? ? Why does blood change colour? Stomach – Acid Bright Red brown / coffee ground Small Bowel – Digestive enzymes Bright Red Dark Red Colon – Bacteria Bright Red Dark Red Black PR Bleeds (haematochezia) Upper GI Black, Tar-like (Malaena) Caecum / Transverse colon Dark Red, Loose stools Mixed with stools Sigmoid / Anus / Rectum Bright red Mixed or separate Massive upper GI bleed Consider occult GI blood loss when: Unexplained anaemia Sudden hypotension and tachycardia, often fluid responsive Shocked patient - PMH of GI bleeds or risk factors Urgency of Management Severe bleeds Resuscitation IP investigation +/- treatment Moderate bleeds IP observation until bleed stops Often OP investigation +/- treatment Mild / low risk bleeds Early discharge OP investigation +/- treatment Severe Bleeds Severe / significant bleed if any of the following: Tachycardia >100 Systolic BP <100 (prior to fluid resuscitation) Postural hypotension Symptoms of dizziness Decreasing urine output Evidence of recurrent melaena / haematemesis / PR bleeding (haematochezia) Resuscitation Assess for signs of hypovolaemic shock A&B Large clots can block airway Risk of aspiration O2 15l Attach monitoring Circulation - Interventions 2 large bore IV cannulae (14 or 16 G) Send blood for FBC, clotting, G&S or Xmatch, inform blood bank IV fluids to maintain BP>100 systolic Start with up to 2l 0.9% Sodium Chloride STAT Then progress to blood IV FFP if variceal bleed suspected or INR>1.3 Urinary catheter D E Blood Blood O Negative immediately shock not responding to IV fluids Type specific (red label ...) 20 mins transient response, ongoing bleed Fully X matched 40 mins plus responded to fluids, but significant blood loss Speak to lab technician they will know exact times! Consider massive haemorrhage alert protocol Massive Haemorrhage Protocol Blood loss of 1 blood volume (5l) within 24hrs or of 50% blood volume (2.5l) within 3hrs or at rate of 150 mls/min Medical Management Stop Antihypertensives NSAIDS Anticoagulants Give 10mg IV vitamin K if INR >1.3 Consider 2mg IV Terlipressin (stat then QDS) Broad spectrum antibiotics (e.g. Tazocin 4.5g tds) 40mg IV Omeprazole bd 40mg oral Omeprazole od Prescribing exercise Emma Smith unstable in A&E resus with a massive upper GI bleed DOB 01/07/55 Hospital Number AA111000 5 Carrington Close Coventry Prescribe 3units red cells Causes of GI Bleed 3 tasks! Brainstorm all causes of GI bleeds Divide into Upper & Lower GI causes Rank from most common to least common Causes - Upper GI (80%) Peptic ulcer disease – 50% Erosive Gastritis / Oesophagitis – 18% Varices – 10% Mallory Weiss tear – 10% Cancer – Oesophageal or Gastric – 6% Coagulation disorders Other Aorto-enteric fistula Benign tumours Congenital – Ehlers-Danlos, Osler-Weber-Rendu Causes - Lower GI (20%) Upper GI bleed! Diverticular disease (angiodysplasia) - 60% Colitis (IBD & ischaemic) – 13% Benign anorectal (haemorrhoids, fissures, fistulas) – 11% Malignancy – 9% Coagulopathy – 4% Angiodysplasia – 3% Post surgical / polypectomy Case 1 PC/HPC 18F Vomited x4 tonight, now streaks of red blood on 3rd and 4th vomits Has been out with friends tonight, had “a few drinks” PMH – Fit and well Drugs & Allergies – Nil O/E Pulse 80 reg, BP 110/80 (no postural drop) Abdomen soft, non-tender, no organomegaly PR - empty rectum Rest of examination normal Case 1 Diagnosis Mallory Weiss tear Severity Mild Ix and Mx Senior r/v with view to discharge and OP OGD How can we predict mortality? Blatchford Score (pre endoscopy) Predicts need for hospital based treatment Score of 6 or more over 50% risk of requiring intervention Lack of subjective variables (e.g. severity of systemic diseases) Lack of a need for OGD to complete the score. Systolic BP Pulse Melena Syncope Coborbidity Urea Hb Not as good as Rockall in predicting overall mortality Rockall Score (post endoscopy) Score Variable 0 1 2 Age <60 years 60-79 years >80 years Shock No shock Tachycardia Hypotension Co-morbidity No major comorbidity Diagnosis (Post OGD) Mallory-Weiss tear, no lesion identified, no SRH Major stigmata of recent haemorrhage (Post OGD) None or dark spot only CCF, IHD, major comorbidity All other diagnoses Malignancy of upper GI tract Blood in GI tract, adherent clot, visible or spurting vessel 3 Renal failure, liver failure, malignancy Endoscopy – Upper GI Bleeds Minor bleeds / unproven Consider OP OGD Moderate bleeds IP OGD within 24hrs Severe bleeds Urgent OGD, Inform Surgeons and Critical Care Suspected Variceal bleed Continued bleeding, >4u blood to keep BP >100 Continuing fresh melaena / haematemesis Re-bleed / unstable post resuscitation If fails, may need emergency surgery Mallory Weiss tear Mallory Weiss tear Hx Vomiting (++) prior to haematemesis Often associated with alcohol Small volume blood “streaks”, mixed with vomit Ex Normal examination Minor Bleeds – Anorectal Bright red blood on toilet paper, not mixed with stools Diagnosed by typical PR appearances Haemorrhoids Feel “lump”, Itch Anal Fissure Anal pain +++ with motions Fistula in ano Soiling on underwear, recurrent abscesses Anal Fissure Haemorrhoids Fistula in ano Moderate & Severe Bleeds Resuscitation including Transfusion Medical Management Haemostasis Treatment of underlying disease Investigations - Why Confirm presence of bleeding Allow safe blood transfusion Plan treatment Assess degree of blood loss Locate bleeding Confirm suspected diagnosis Assess extent (staging) of disease Assess risk factors for bleeding Bedside Faecal Occult Blood (FOB) Not commonly available now as bedside test Still used in lab for bowel cancer screening Proctoscopy Anal canal Rigid Sigmoidoscopy Rectum and distal sigmoid colon Up to 20cm max Blood tests FBC Hb level ? Chronic microcytic anaemia LFTs & Clotting Clotting disorders and risk factors for these Liver failure, and risk of varacies Tumour Markers CEA if suspected colon cancer Ca19.9, Ca125 & CEA if suspected gastric cancer G&S / Crossmatch Allows transfusion Imaging - location of bleed All during active bleed CT Angiogram Non invasive, sensitivity & specificity 85-90% Angiogram Bleeds >0.5 ml/min Therapeutic & diagnostic Red Cell Scan - Tc-99m RBC scintigraphy Slow volume bleeds, >0.1ml/min Imaging – cause of bleed CT abdomen & pelvis with contrast Acutely unwell, for cause including ?colitis Staging suspected cancers Barium Enema Diverticular disease, Colon Cancer CT Colon As for Ba Enema Barium meal / follow-through Investigate possible small bowel causes (Crohn’s) Endoscopy Rigid scopes – see bedside tests OGD (Oesophago-gastro-duodenoscopy, Gastroscopy, Upper GI endoscopy) For all Upper GI bleeds Flexible Sigmoidoscopy Suspected left sided colonic bleeds To splenic flexure, aprox 40-60cm Colonoscopy Suspected right sided colonic bleeds Whole colon visualised Surgery Last resort When location not found, and ongoing significant bleed Can locate most proximal part of bowel with blood in lumen, & Limited resection If unclear, and colonic, occasionally total colectomy Case Studies Small groups, same colour cases For Case 2, list and justify: Diagnosis & 2 main differentials Severity of Bleed Blatchford or Rockall Score (pre endoscopy) if appropriate Investigations & Management Red case 2 PC/HPC 73M Bright red blood with dark clots in last 4 bowel motions (all today) Mixed with stool (liquid) initially, now only blood No abdominal pain PMH – nil Drugs – Movicol 1-2 satchets PRN O/E BP 130/70 (no postural drop), P85, Hb 10.2 Abdomen soft, non tender PR – Bright red blood plus darker clots+ in rectum Case Red 2 Diagnosis Diverticular bleed Severity Moderate Blatchford Score n/a – only for upper GI bleeds Ix and Mx ABCDE resuscitation Bloods (Hb level, exclude infection),?CT abdo, Flexi sig once settled Observe, ?antibiotics Treatment – Lower GI Bleeds Haemostasis Most stop spontaneously +/- medical management Angiogram Embolisation Occasionally surgery Generalised colonic bleeds (eg colitis) Endoscopy rarely Can’t see clearly Treatment of underlying disease Definitive treatment of Cancers Ulcers Diverticular disease Conservative, Medical or Surgical Urgent or Elective Diverticular Disease Diverticular Disease Hx Prone to constipation Loose motion, then blood mixed in, then only blood Often out of the blue Known history Ex Abdomen usually non tender Blood PR, no masses, no anorectal pathology Inflammatory Bowel Disease Hx Known IBD Loose motions, up to 20x/day Now mucus and blood, increased frequency Ex Thin Tender abdomen Systemic signs of IBD Ulcerative Colitis Crohn’s Disease Yellow 2 PC/HPC 70 F 24hrs increasing generalised abdo pain (now severe++) and diarrhoea Now blood mixed with stools, bright and dark red PMH AF, otherwise well O/E Pulse 130 Ireg Ireg, BP 110/60 lying, 90/50 sitting, RR 24, looks pale and clammy, Abdomen soft, no localised tenderness PR – blood mixed with mucus and liquid stool on finger ABG – Lactate 5.1, pO2 12.4, pCO2 3.0, pH 7.35 Case Yellow 2 Diagnosis Ischaemic colitis Severity Severe Blatchford score n/a Ix and Mx ABCDE resuscitation ECG, Rigid sigmoidoscopy, Bloods (Hb, Trop I, U&Es, inflammatory markers), CT abdomen Colonoscopy NBM, IVI, Antibiotics, +/- Surgery Ischaemic Colitis Hx AF / IHD Generalised pain Colitic symptoms Deteriorating rapidly Ex “Pain out of proportion with signs” No localised signs (until perforation) Acidosis Case Blue 2 PC/HPC 45 M attends A&E 3 episodes haematemesis today, bright red blood++ no other complaints from patient PMH – admits nil SH – 4 cans strong larger / day Drugs – Thiamine, Vit B Co Strong O/E HR 110bpm reg, BP 98/60, Urea 6.6, Hb119g/l mildly confused (GCS 14/15) Jaundiced, 3x spider nevi on chest and abdomen Abdomen soft, non tender. RUQ tender mass, smooth, 1 finger breath below costal margin, moves with respiration PR – Dark red blood in rectum, no visible stools Case Blue 2 Diagnosis Bleeding varices Severity Severe Blatchford Score BP 2, P 1, Melena 1, syncope 0, Comorbidities 0, Urea 2, Hb 3 = 9 Ix and Mx ABCDE resuscitation, inc up to 2l fluids, FFP, ? blood Terlipressin, IV Antibiotics, ?Vitamin K, Urgent senior r/v, urgent endoscopy (within 8hrs) Case Blue 2 OGD Results: Large oesophageal varices, no active bleeding. Clots in stomach. Varices banded. What is the Rockall Score? Rockall Score Score Post endoscopy? Variable 0 1 2 Age <60 years 60-79 years >80 years Shock No shock Tachycardia Hypotension Co-morbidity No major cormorbidity Diagnosis (Post OGD) Mallory-Weiss tear, no lesion identified, no SRH Major stigmata of recent haemorrhage (Post OGD) None or dark spot only CCF, IHD, major comorbidity All other diagnoses Pre OGD Score 0-1 next available list (Mortality <2.5%) >=2 urgent OGD (Mortality 5%) 3 Renal failure, liver failure, malignancy Malignancy of upper GI tract Blood in GI tract, adherent clot, visible or spurting vessel Post OGD Score <3 good prognosis, early discharge >8 high risk of death Oesophageal Varices Hx Known liver disease Known varices High alcohol intake Ex Stigmata of liver disease Smell of alcohol on breath Yellow sclera Caput Medusae Gynaecomastia Palmar erythema Dupuytren’s contracture Case Green 2 PC/HPC 35M, GP admission to CDU Diarrhoea today, and feeling a little faint at times, but hasn’t passed out. Mild epigastric pain 1/7, settles with antacids. PMH – Sports injury 10/7 ago, ?ACL damage Drugs – nil regular, on pain relief for knee Allergies - nil O/E Pulse 100 reg, BP 110/60, (lying), 80/40 (standing) Tender epigastrum, no guarding, slightly distended, no organomegaly PR – black, tarry motion, no red blood or faeces Other examination normal Case Green 2 Diagnosis Duodenal Ulcer Severity Severe Rockall Score Age 0, Shock 2, Co-morbidity 0= Total 2 Ix and Mx ABCDE, 2L fluids, +/- blood IV Omeprazole, endoscopy within 24hrs, close monitoring, ?Erect CXR Case Green 2 OGD after 2hrs (pt deteriorated) Blood in stomach ++ Large duodenal ulcer, spurting blood What is the new Rockall Score? Rockall Score (Upper GI only) Score Post endoscopy score? Variable 0 1 2 Age <60 years 60-79 years >80 years Shock No shock Tachycardia Hypotension Co-morbidity No major cormorbidity Diagnosis (Post OGD) Mallory-Weiss tear, no lesion identified, no SRH Major stigmata of recent haemorrhage Pre(Post OGDOGD) Score None or dark spot only CCF, IHD, major comorbidity All other diagnoses 0-1 next available list (Mortality <2.5%) >=2 urgent OGD (Mortality 5%) 3 Renal failure, liver failure, malignancy Malignancy of upper GI tract Blood in GI tract, adherent clot, visible or OGD Score spurting vessel Post <3 good prognosis, early discharge >8 high risk of death Gastric and Duodenal Ulcers Gastritis Peptic ulcers and Erosions Hx Associated with typical pain NSAID use Previous gastritis / ulcers Stress (including operations) Ex Epigastric tenderness / guarding Perforated ulcers Ulcers rarely bleed and perforate simultaneously Suspect perforation if any abdominal guarding Localised epigastric guarding Generalised peritonitis If suspicious get Erect CXR Surgical input Other Bleeds Post op Complications Very rare Must be considered if recent intervention More commonly, rebleeds post haemostatic interventions Can be very large bleeds, clots+++ Dieulafoy’s lesion AV malformation Very difficult to see at endoscopy Frequently re-bleeds after intervention Can be missed, so can bleed after “negative” endoscopy Colon Cancer Colorectal Malignancy Hx Weight loss, loss of appetite, lethargy Right sided – often only iron deficiency anaemia Left side – change in bowel habit, blood mixed with stool, mucus, tenesmus Ex Palpable mass (abdominal / PR) Visible weight loss Craggy liver edge May be normal Gastric Cancer Oesophageal cancer Oesophageal & Gastric Malignancies Hx Weight loss, loss of appetite, general lethargy Dysphagia Vomiting ++ Known malignancy Recent stent insertion Ex Emaciated Palpable craggy liver edge Palpable neck LN (rare) Visible metastases (rare) Summary (1) Colour of blood important for location of bleed Assess severity of bleed (including Rockall Score) to decide urgency of management Simultaneous Resuscitation, investigations & management if unwell Targeted investigations for less sick patients Summary (2) Likely diagnosis from history and examination Use guidelines / pathways to aid management ASK FOR HELP when needed!!! ANY QUESTIONS?