Biology 221 - CCBC Faculty Web
advertisement

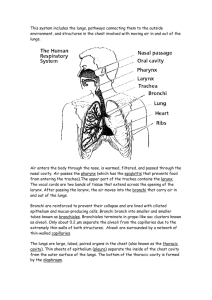
Biology 221 Anatomy & Physiology II TOPIC 7 Respiratory System Chapter 23 pp. 834-879 E. Lathrop-Davis / E. Gorski / S. Kabrhel 1 Functions • The main function of the respiratory system is exchange gases, especially O2 and CO2. • Other functions of the respiratory system include: – maintaining acid-base (pH) balance (CO2 + H2O H2CO3); – sound production (vocalizations); – neurotransmitter removal; – conversion of angiotensin I to angiotensin II; – housing olfactory receptors for smell; and – trapping and dissolving small clots before they reach the systemic circulation. 2 Basic Processes of Respiration The four basic processes of respiration are: • ventilation, which moves air into and out of the lungs; • external respiration, which is the exchange of gases between blood and air in lungs; • blood gas transport, which is the transport of gases between lungs and body tissues; and • internal respiration, which is the exchange of gases between blood and body tissues. Fig. 23.17, p. 860 3 Basic Airway Organization There are two major groups of passageways. • Conducting passageways move air into and out of body but are not involved in actual gas exchange – Conducting passageways include the nose, pharynx, trachea, larynx, bronchi, bronchioles, and terminal bronchioles. • Respiratory passageways are involved in the exchange of gases between air and blood. – Respiratory passageways include the respiratory bronchioles, alveolar ducts, and alveoli. Fig. 23.1, p. 836 4 Lung Anatomy • The lungs are located in the thoracic cavity lateral to mediastinum. • Each lungs consists of lobes. There are 3 on the right and 2 on left. Lobes are served by secondary bronchi. • Each lobe consists of several bronchopulmonary segments, sections of lobes separated by connective tissue. – Each bronchopulmonary segment is served by its own tertiary (segmental) bronchus. – Each bronchopulmonary segment is supplied by its own artery, vein, and lymphatics. – Each segment can be removed surgically with limited affects on the surrounding segments. See Fig. 23.10, p. 848 5 Lung Anatomy • Bronchopulmonary segment are divided into lobules, which are the smallest visible subdivisions of lung tissue. Lobules are served by large bronchioles. • Lung tissue consists of air passageways and respiratory surfaces embedded in elastic connective tissue. • The hilus is an indentation on the medial surface of the lung through which bronchi, blood vessels, lymphatics and nerves pass. See Fig. 23.10, p. 848 6 Lung Anatomy (con’t) • Serous membranes cover the lungs and line the thoracic cavity. – The visceral (= pulmonary) pleura covers lungs. – The parietal pleura lines the thoracic cavity. – The “space” between them is pleural cavity. This space is filled with serous fluid. ° Think About It: What is one important function of this fluid? (See A&P I Unit 2 – Tissues) See Fig. 23.10, p. 848 7 Conducting Passageways: Nose and Nasal Cavity • The functions of the nose and nasal cavity include: – serving as airways for ventilation; – moistening, warming, and filtering air; – resonance of sounds produced for speech; – housing olfactory receptors for smell. Fig. 23.3, p. 838 8 Conducting Passageways: Nose and Nasal Cavity • Several special structures are associated with the nasal cavity. – The paranasal sinuses aid resonance of sound and lighten the skull. (Covered in lab) – The nasal conchae are covered with mucous membranes and increase the surface area for warming and moistening the air. – The nasal septum separates right and left and helps keep an open passage even when one side is blocked. Fig. 23.3, p. 838 9 Conducting Passageways: Nose and Nasal Cavity – The palate separates the nasal cavity from the oral cavity. This permits breathing while eating. ° The hard palate consists of the palatine process of the maxilla and the palatine bones and is useful during chewing. ° The soft palate consists of muscle and closes the opening to the nasopharynx during swallowing. Fig. 23.3, p. 838 10 Conducting Passageways: Pharynx • The pharynx connects the nose and mouth to the larynx. • The three “parts” of the pharynx are distinguished by landmarks. – The nasopharynx carries air only. ° It is located posterior to the nasal cavity, superior to soft palate. ° It contains the pharyngeal tonsils (adenoids; see Topic 5). ° The auditory tubes (also called the pharyngotympanic or eustachian tubes) open into the nasopharynx. (See A&P I Unit 10) Fig. 23.3, p. 838 11 Conducting Passageways: Pharynx – The oropharynx is a passage for air and food. ° It is posterior to oral cavity, inferior to soft palate. ° It is lined with stratified squamous epithelium, which protects against abrasion. ° The lingual and palatine tonsils protect against food and air borne particles. (See Topic 5) – The laryngopharynx is a passage for air and food ° It is inferior to oropharynx and posterior to the larynx. ° It is also lined with stratified squamous epithelium. Fig. 23.3, p. 838 12 Conducting Passageways: Larynx • The opening into larynx is called the glottis. • The epiglottis is a piece of mucosa-covered elastic cartilage. – It covers the glottis and keeps food out of larynx during swallowing. • The walls of the larynx are formed by pieces of hyaline cartilage including: – the thyroid cartilage, which is the largest, – the cricoid cartilage, and – the arytenoid cartilages, which are important to sound production. 13 Larynx: Sound Production • The true vocal cords (folds) are folds of mucosa containing elastic vocal ligaments that vibrate to produce sound. – Tension is controlled by arytenoid cartilages – The vocal cords tighten during exhalation and air movement causes vibration of cords. ° Pitch (frequency) is controlled by changing length and tension of cords. - Tighter stretch produces higher frequency. ° Loudness depends on force of vibration. • Vestibular folds, located superior to the vocal folds, protect the vocal folds. 14 Conducting Passageways: Trachea • The airways from from the larynx to the level of the T5 vertebra in the chest are patent. That is, they are kept open to allow free flow of air. • The trachea contains 16-20 hyaline cartilage rings. – These rings are incomplete in back, which makes for easier passage of food through the esophagus. Fig. 23.5, p. 843 15 Conducting Passageways: Trachea There are 3 layers in trachea wall. • The mucosa consists of ciliated pseudostratified columnar epithelium with goblet cells and an underlying lamina propria of areolar connective tissue. – Goblet cells in the epithelium produce mucus that helps trap airborne particles. – Cilia form ciliary escalator, which moves the particle-laden mucus upwards. • The submucosa consists of connective tissue layer. – Seromucous glands secrete additional mucus. 16 Conducting Passageways: Trachea • The adventitia consists of elastic connective tissue and hyaline cartilage rings. – The rings are incomplete posteriorly. – The trachealis muscle consists of smooth muscle and bridges the rings posteriorly. 17 Bronchial Tree • The bronchial tree includes both conducting and respiratory passageways. – Conducting passageways include the primary bronchi through the terminal bronchioles. – Respiratory passageways include the respiratory bronchioles, which lead to the alveoli. • General trends include: – a decrease in and eventual loss of cartilage rings; – the gradual addition of smooth muscle to control airway diameter; and – flattening of the epithelium, which goes from pseudostratified columnar to simple squamous. 18 Conducting Passageways: Primary Bronchi • One primary bronchus goes to each lung. • The walls have cartilage with some smooth muscle. • The bronchi are lined with pseudostratified ciliated columnar epithelium with numerous goblet cells. Fig. 23.7, p. 844 19 Conducting Passageways: Secondary Bronchi • Secondary bronchi are branches of the primary bronchi. These serve the lobes of lungs; there are 3 on right and 2 on left. (See pg. 5) • Walls have less cartilage and more smooth muscle than do the primary bronchi. • The secondary bronchi are lined with pseudostratified ciliated epithelium in which cell height is smaller than in the primary bronchi. http://www.pul.unimaas.nl//respir.htm#lower%20tract Fig. 23.7, p. 844 20 Conducting Passageways: Tertiary Bronchi • Tertiary bronchi are branches of the secondary bronchi and serve the bronchopulmonary segments. • The walls have irregular rings of cartilage and much more smooth muscle. • Cells of the pseudostratified ciliated epithelium lining are very short. Fig. 23.7, p. 844 http://www.pul.unimaas.nl//respir.htm#lower%20tract 21 Conducting Passageways: Bronchioles • Bronchioles are small branches of the tertiary bronchi. – There are many subdivisions and levels of bronchioles. • The walls consist mainly of smooth muscle with little or no cartilage. This muscle will be important to control of airway diameter. • Bronchioles are lined with cuboidal epithelium. Fig. 23.7, p. 844 http://www.pul.unimaas.nl//respir.htm#lower%20tract 22 Conducting Passageways: Terminal Bronchioles • Terminal bronchioles are branches deep in the lungs. • They lack cartilage and smooth muscle is scattered. • Terminal bronchioles are lined with cuboidal epithelium. • Terminal bronchioles are the last of the conducting passageways and lead to respiratory bronchioles. Fig. 23.7, p. 844 http://www.pul.unimaas.nl//respir.htm#lower%20tract 23 Respiratory Zone (Passageways) Respiratory Bronchioles • Respiratory bronchioles are the smallest and thinnest of air passageways leading to respiratory surfaces of lung. • They are lined with low simple cuboidal epithelium. Fig. 23.8, p. 845 http://www.kumc.edu/instruction/medicine/anatomy/histoweb/resp/resp.htm 24 Respiratory Zone: Alveoli • Alveolar ducts are passageways from the respiratory bronchioles to the alveolar sacs and alveoli. • Alveolar sacs are groups of alveoli with a common opening. • Alveoli (singular = alveolus) are the individual air sacs. http://www.usc.edu/hsc/dental/ghisto/lng/d_28.html Fig. 23.8, p. 845 25 Respiratory Zone: Alveoli • Thin-walled structures across which gases are exchanged • Barrier to diffusion respiratory gases (CO2 and O2) • Adjacent alveoli joined by alveolar pores http://www.usc.edu/hsc/dental/ghisto/lng/d_28.html Fig. 23.8, p. 845 26 Respiratory Zone: “Respiratory Membrane” • The respiratory membrane is the surface across which gases are exchanged. – It consists of the alveolar epithelium, the capillary epithelium, and the basement membrane between them. • Alveolar endothelium consists of two types of cells. – Type I cells are simple squamous epithelium (blue arrow in the linked image) and function in gas exchange. – Type II cells are scattered simple cuboidal cells (green arrow in the linked image) and secrete surfactants. http://www.kumc.edu/instruction/medicine/anatomy/histoweb/resp/resp.htm (#15) 27 Respiratory Zone: “Respiratory Membrane” • The basal lamina is the basement membrane that joins the two epithelial layers. • Capillary endothelium consists of simple squamous epithelium. http://www.kumc.edu/instruction/medicine/anatomy/histoweb/resp/resp.htm 28 Nerve Supply to Lungs • Nerves enter and leave through the hilus. • Pulmonary plexuses provide autonomic (ANS) innervation to smooth muscle of the bronchi and bronchioles. There are two kinds of plexuses – one for each division of the ANS. – The sympathetic pulmonary plexus provides sympathetic innervation that leads to dilation of bronchi and bronchioles. ° Think About It: Why would this be important to the fight or flight response? Fig. 14.4, p. 519 29 Nerve Supply to Lungs – Parasympathetic innervation from the pulmonary plexus of the Vagus (X) nerve causes constriction of bronchi and bronchioles. ° Think About It: Which division (sympathetic or parasympathetic) would be involved in responses to airborne irritants? - (HINT: The response to irritants is to decrease the size of the airways.) Fig. 14.4, p. 517 30 Blood Supply to Lungs • Vessels enter and leave through the hilus. • Two systems serve the lungs. – The pulmonary circulation carries blood to the respiratory surfaces of the lungs for gas exchange with air in alveoli. ° Pulmonary arteries bring blood to the lungs. ° Alveolar capillaries are sites of exchange of gases between air in the alveoli and blood. ° Pulmonary veins carry blood from the lungs to the heart. ° Recall: Which of these vessels carry oxygenated blood? Which ventricle pumps into this system? Which atrium receives blood from it? 31 Blood Supply to Lungs – The bronchial circulation carries blood to all lung tissues except the alveoli. ° This circulation goes from the aorta to bronchial arteries to capillaries to bronchial veins. ° Most blood returns via pulmonary veins due to numerous anastomoses. ° Recall: Which of these vessels carry oxygenated blood? Which ventricle pumps into this system? Which atrium receives blood from it? 32 Ventilation • Ventilation is the movement of air into or out of lungs. – Inspiration is movement of air into the lungs. – Expiration is movement of air into the lungs. • Air flow is directly related to the pressure gradient; and inversely related to resistance. – Air moves from areas of higher pressure to areas of lower pressure. – The pressure gradient moves air and gases between nose (or mouth) and the terminal bronchioles. – Between the terminal bronchioles and alveoli, individual gas movement is driven by diffusion. 33 Ventilation: Pressures 3 pressures are involved in ventilation. • Atmospheric pressure (PA) is the same as air pressure. – It is the external pressure of the air around the body. • Intrapleural (intrathoracic) pressure is the pressure within the pleural cavity. – Intrapleural pressure is always less than intrapulmonary pressure (within alveoli) by about 4 mm Hg. – If intrapleural pressure equals or exceeds atmospheric pressure, the lungs collapse. • Intrapulmonary (intra-alveolar) pressure (PL) is the pressure within the alveoli. 34 Ventilation: Pressures • Atmospheric pressure normally stays roughly the same at any given altitude. • Since atmospheric pressure doesn’t change, ventilation (breathing) involves changing intrapulmonary pressure. 35 Boyle’s Law • Boyle’s law states that gas pressure is inversely proportional to volume (V). – Increasing volume decreases the pressure on the gas. – Decreasing volume increases the pressure on the gas. • Air moves from higher pressure to lower pressure. 36 Boyle’s Law • Given the pressures: – PL = intrapulmonary pressure – PA = atmospheric pressure – And that air moves from higher to lower pressure. • For inspiration: PL < PA – That is, pressure in the lungs must be less than atmospheric pressure for air to move into the lungs. – Volume, V, must increase so that PL can decrease. • For expiration: PL > PA – That is, pressure in the lungs must be more than atmospheric pressure for air to move out of the lungs. – V must decrease so that PL can increase 37 Processes of Ventilation • The process of ventilation involves contraction of skeletal muscle. (Review notes from A&P I muscle lab.) – This allows voluntary control as well as subconscious control. • Muscles whose contraction increases the size of the thoracic cavity will cause inspiration. – Relaxation of these muscles will cause passive expiration as they return to their resting state. • Muscles whose contraction decreases the size of the thoracic cavity will add to expiration. 38 Processes of Ventilation Inspiration 1. The diaphragm and/or external intercostal muscles contract (innervated by phrenic and intercostal nerves, respectively). 2. Thoracic volume increases. 3. Intrapleural pressure decreases. 4. Lungs expand into the lower pressure thoracic (pleural) cavity. 5. Intrapulmonary pressure decreases. 6. Air moves in. 39 Processes of Ventilation Expiration 1. The diaphragm and external intercostal muscles relax (passive process) and lungs recoil. 2. Thoracic volume decreases. 3. Intrapleural pressure increases. 4. Lungs are compressed by the increased pressure in thoracic (pleural cavity). 5. Intrapulmonary pressure increases. 6. Air moves out. – Expiration is normally passive 40 “Forced” Air Movements: Expiration • Forced expiration expels more than the normal amount of air. • Forced expiration is accomplished by increasing intrapleural pressure beyond normal breathing by making thoracic cavity even smaller. • The muscles that contribute to forced expiration are: – abdominal muscles – external and internal obliques, transversus abdominis; and – thoracic muscles – internal intercostals, latissimus dorsi, quadratus lumborum. 41 “Forced” Air Movements: Inspiration • Forced inspiration involves inhaling more than normal amount of air. • This is accomplished by decreasing intrapleural pressure beyond normal breathing by increasing the thoracic cavity even more. • Muscles involved are the: – pectoralis minor, scalenes, sternocleidomastoid muscles. 42 Promoting Lung Expansion • Inspiration (when inspiratory muscles contract) is aided by two things: compliance and surface tension within the pleural cavity. – Compliance is the ability of the lungs to expand. ° Decreased compliance makes it more difficult to inflate the lungs. ° Causes of reduced compliance include: - loss of elasticity of lung tissue; and - increased alveolar surface tension. 43 Promoting Lung Expansion – Surface tension within the pleural cavity is caused by pleural fluid. ° Pleural fluid (serous fluid within the pleural cavity) creates negative intrapleural pressure between the pleural membranes (not unlike water between two pieces of glass). ° Excess fluid is normally removed by the lymphatic system. ° Failure to remove fluid results in a build up of fluid (pulmonary edema), which increases the intrapleural pressure (i.e., it becomes less negative) making it difficult to inflate the lungs. 44 Promoting Lung Compression • Expiration when inspiratory muscles are relaxing is aided by alveolar fluid surface tension and elastic recoil of the lungs. – Alveolar fluid surface tension causes the lungs to “want” to collapse by pulling the sides of the alveoli closer together. ° Surfactant decreases alveolar surface tension, thus preventing collapse. - Respiratory distress syndrome (RDS; also known as hyaline membrane disease of the newborn) occurs in a premature babies that have insufficient amounts of surfactant in lung; the lungs collapse during expiration and must be reinflated. 45 Promoting Lung Compression – Elasticity is the elastic recoil of lungs due to elastic tissue in the walls of the lungs. ° Elasticity helps the lungs become smaller like the deflating of a stretched balloon. ° Emphysema is a disease that decreases elasticity. This makes exhalation difficult and instead of being passive, it becomes an active process. 46 Resistance to Airflow • Resistance to airflow opposes movement of flow into/out of lungs. • Resistance is related to size (radius [r] and length) of the air passageways and viscosity of the “fluid” (air). – Resistance (length of tube x viscosity of fluid) / r4 – Resistance is: ° directly related to tube length; ° directly related to viscosity; and ° indirectly related to radius4 (i.e., 1/r4). • Resistance is greatest in medium-sized bronchioles. Fig. 23.5, p. 854 Means “is approximately equal to” 47 Factors Increasing Airflow Resistance Increased airflow resistance decreases flow. Things that increase resistance include: • Bronchoconstriction, which makes airways narrower – Bronchoconstriction is caused by: ° the parasympathetic response to inhaled irritants; ° acetylcholine administration; and ° decreased PCO2 (partial pressure of CO2). • Other factors that decrease size of airways include: – solid obstructing tumors; – mucus accumulation; and – inflammation. 48 Factors Decreasing Airflow Resistance Decreased airflow resistance increases flow. • Bronchodilation makes airways larger. Bronchodilation is caused by: – sympathetic innervation; – epinephrine administration; and – increased PCO2. 49 Regulation of Ventilation • Ventilation is controlled by the respiratory center located in the medulla oblongata (as part of the reticular formation). • The respiratory center consists of: – inspiratory center (dorsal respiratory group or DRG); and the – expiratory center (ventral respiratory group or VRG). • Under quiet breathing at rest, breathing is controlled primarily by the DRG. 50 Mechanism of Basic Control • The active DRG sends impulses to inspiratory muscles to stimulate contraction (also simultaneously sends inhibitory impulses to the VRG). – The phrenic nerve (from the cervical plexus) goes to the diaphragm. – Intercostals nerves (from thoracic spinal cord segments) go to the external intercostals. • After about 2 seconds, the DRG becomes inactive, impulses are no longer sent, and expiration occurs as the inspiratory muscles relax. • After about 3 more seconds, the DRG becomes active again. Fig. 23.24, p. 868 51 Other Coordinating Centers • The pneumotaxic center located in pons inhibits the DRG leading to shortened breaths leading to increased breathing rate (e.g., panting). • The apneustic center is a hypothetical center in pons thought to prolong inspiration by stimulating the DRG. 52 Factors Affecting Ventilation Rates • Pulmonary irritants (air-borne chemicals) are detected by chemoreceptors in lungs that send impulses via Vagus nerve. The resulting efferent parasympathetic impulses (also from the Vagus nerve) cause bronchoconstriction. Efferent somatic impulses result in coughing or sneezing See Fig. 23.25, p. 869 53 Factors Affecting Ventilation Rates • In the Hering-Breuer (inflation) reflex stretch receptors in the visceral pleura and conducting portions of airways respond to inflation of lungs and send afferent impulses via Vagus nerve to the DRG. These impulses inhibit the DRG, thus preventing over inflation of the lungs. See Fig. 23.25, p. 869 54 Factors Affecting Ventilation Rates • Cortical controls allow conscious control over skeletal muscles involved in inspiration and expiration. • The hypothalamus influences the medullary centers in response to emotions (e.g., pain, fear, anger) or increased body temperature. • Chemical controls are based on chemistry of arterial blood. – Chemicals are sensed by peripheral chemoreceptors in the carotid arteries and aorta and by central chemoreceptors in the medulla oblongata. See Fig. 23.25, p. 869 55 Chemical Controls: PCO2 • The PCO2 of normal arterial blood is 40 mm Hg + 3 mm Hg. • Peripheral chemoreceptors located in the carotid arteries and aorta are not very sensitive to arterial PCO2. – Sensory (afferent) input is sent to the medulla via the glossopharyngeal nerves (from carotid arteries) and vagus nerves (from aorta). 56 See Fig. 23.25, p. 869 Chemical Controls: PCO2 • Central chemoreceptors located in the medulla are sensitive to changes in PCO2 (as pH changes). • CO2 diffuses readily across membranes (enters CSF). – Increased PCO2 in the CSF leads to increased carbonic acid (H2CO3), which increases H+ concentration and lowers pH. – Increased H+ stimulates receptors in the medulla leading to increases in the depth (and/or rate) of breathing. This increase is hyperventilation. 57 See Fig. 23.25, p. 869 Chemical Controls: PCO2 ° Hyperventilation increases CO2 exchange (loss), thereby returning levels to normal. ° The effect of PCO2 on central receptors works even when arterial blood pH and PO2 are normal. – Low PCO2 leads to decreased H+ in the CSF (which increases pH). The result is slower breathing, or hypoventilation, which decreases CO2 exchange (loss), thereby returning levels to normal. 58 See Fig. 23.25, p. 869 Chemical Controls: PO2 • The PO2 of normal arterial blood is around 105 mm Hg. • The central respiratory center is less sensitive to PO2. • Peripheral chemoreceptors are sensitive to PO2. – BUT receptors are only stimulated when PO2 falls below 60 mm Hg. This is because hemoglobin is still more than 80% saturated even at a PO2 of 60 mm Hg. 59 Chemical Controls: pH • The pH of normal arterial blood is around pH 7.4 (slightly alkaline). The normal range is pH 7.35-7.45. – Decreased arterial pH stimulates peripheral receptors resulting in increased ventilation even if PCO2 and PO2 are normal. • Think About It: What would happen to breathing if: – Arterial pH increased above 7.45? – Decreased below 7.35? 60 Terms • • • • • Eupnea is normal, quiet breathing. Dyspnea is difficult, labored breathing. Apnea is the cessation of breathing (e.g., sleep apnea). Hypopnea is abnormally slow &/or shallow breathing Hyperpnea is deep, vigorous breathing (may also be faster, but main thing is increased depth). • Tachypnea is rapid breathing. 61 Overview of External and Internal Respiration and Gas Transport • External Respiration is the exchange of gases between air and blood. • Gas Transport is accomplished by blood (by red blood cells and plasma). • Internal Respiration is the exchange of gases between blood and interstitial fluid (of tissues). • Important respiratory gases are: – CO2 (the product of aerobic metabolism) and – O2 (which is needed for aerobic metabolism). 62 Dalton’s Law of Partial Pressures • Dalton’s Law of partial pressures states that the pressure exerted by a single gas in a mixture is directly proportional to the percentage of that gas in the mixture – At sea level, the amount O2 accounts for approximately 20.9% of the gas in air. – At sea level, total gas pressure is approximately 760 mm Hg. – Therefore, PO2 is 20.9% x 760 mm Hg = 159 mm Hg. See Table 23.4, p. p. 859 63 Dalton’s Law of Partial Pressures • Approximate Percentages of Gases at Sea Level N2 79.6% O2 20.9% CO2 0.04% H2O 0.46% • Total pressure decreases with altitude, therefore, PO2 decreases (see next slide). See Table 23.4, p. p. 859 64 Oxygen and Altitude Altitude – ft above sea level 0 6000 Atmospheric pressure (mmHg) Partial Pressure of oxygen (mmHg) Partial Pressure of O2 in alveoli 760 609 160 127 105 84 8000 564 118 79 10,000 523 109 74 15,000[1] 430 90 60 18,000[2] 380 ~75 ~48 24,000 300 ~60 ~42 29,028[3] 240 ~48 ~20 [1] ~ Pike’s Peak summit [2] Mt. Everest base camp [3] Mt. Everest summit http://www.udel.edu/Biology/dion/SicknessComments.html 65 Think-Pair-Share: Altitude Sickness • What happens to atmospheric oxygen levels as you go up in altitude? • If someone were hiking in Colorado on Pike’s Peak (~14,900 feet above sea level), how much oxygen would be available in the atmosphere? In the alveoli? • How would this affect the arterial oxygen levels? • How would the body respond to the decreased arterial oxygen? (How does the body normally respond to hypoxia?) – What “disorder” of the blood results from this? • What is pulmonary edema? 66 Henry’s Law • Henry’s law states that when a mixture of gases comes into contact with a liquid, individual gases will diffuse into the liquid in proportion to their partial pressures • Therefore, Diffusion Rate = gas solubility X membrane surface area X gradient X oF membrane thickness X square root of molecular wt. “gradient” = difference in partial pressures Which of these would you expect to control? 67 Factors Governing Diffusion Rate • Gas solubility in liquid depends on temperature, which is normally held relatively constant. • Molecular weight of the gas is a constant. • Temperature of the liquid is body temperature, which normally stays within narrow range. • Membrane thickness refers to the capillary and alveolar walls; this normally stays same but is changed by diseases such as emphysema and pulmonary edema. • Membrane surface area normally stays the same, but is decreased by diseases like lung cancer and emphysema. http://pathhsw5m54.ucsf.edu/case25/image253.html http://www-medlib.med.utah.edu/WebPath/LUNGHTML/LUNG059.html http://www-medlib.med.utah.edu/WebPath/LUNGHTML/LUNG124.html 68 Factors Governing Diffusion Rate • The partial pressure gradient* is controlled – maintained by ventilation. • Partial pressures in the alveoli are different from atmospheric partial pressures. Gas Partial Pressure Atmospheric Air, mm Hg Alveolar Air, mm Hg PO2 159 104 PCO2 0.03 40 PH2O 3.5 47 69 Partial Pressure Gradient • Reasons for difference between atmospheric and alveolar partial pressures include: – Humidification (addition of H2O) of inhaled air. ° As H2O is added, its partial pressure increases and all other partial pressures decrease. – Gas movements between air and blood. ° Movement of CO2 into the alveoli from the blood increases alveolar PCO2; and ° Movement of O2 from the alveoli into the blood decreases alveolar PO2 70 Partial Pressure Gradient – Mixing of old and new air within the alveoli and conducting passageways also keeps alveolar air higher in CO2 and lower in O2. ° Not all alveolar air is exchanged with each breath. ° Air in the conducting passages is called “dead air” and does not participate in exchange of gases between air and blood. ° This air is higher in O2 and lower in CO2 than alveolar air. 71 External Respiration: Gas Movements • O2 is loaded into blood from the alveoli. • CO2 is unloaded out of blood into the alveoli. Arteriole end Venule end 72 Ventilation-Perfusion Coupling: PO2 • The circulatory system works in coordination with respiratory system to maximize effectiveness of gas exchange. • PO2 affects the diameter of arterioles (arteriolar diameter). – Low airflow in a bronchiole results in decreased PO2 in the airway. This causes vasoconstriction of the pulmonary arterioles serving the alveoli associated with that bronchiole. ° Therefore, less blood goes to where alveolar oxygen will be low. 73 Ventilation-Perfusion Coupling: PO2 – High airflow in a bronchiole results in increased PO2 in the airway leading to alveoli. This causes vasodilation of the pulmonary arterioles serving that area. ° Therefore, more blood goes to where alveolar PO2 will be high. 74 Ventilation-Perfusion Coupling: PCO2 • PCO2 affects bronchiolar diameter (diameter of bronchioles) – High PCO2 in an airway results in bronchodilation, which results in increased airflow. ° Increased airflow clears CO2 from the airway. – Low PCO2 in an airway results in bronchoconstriction, which results in decreased airflow. ° Decreased airflow prevents loss of too much CO2, which would affect pH. 75 Blood Gas Transport: Oxygen • Most oxygen – around 98.5 % of it – is carried attached to iron atoms of hemoglobin (Hb). – Iron (Fe) is part of the heme. There is one Fe per heme. – There are 4 heme per hemoglobin molecule. ° Therefore, 4 O2 are carried per molecule. - Hb with O2 is called oxyhemoglobin [Hb(O2)4] - Deoxyhemoglobin (HHb) is Hb without oxygen. It combines with 4 O2 to become Hb(O2)4 • The remaining O2 – around 1.5% – is carried as dissolved oxygen in plasma. This exerts the partial pressure of oxygen. http://www.pul.unimaas.nl//respir.htm#lower20%tract 76 Blood Gas Transport: Oxygen • Because there are 4 chains in Hb, oxygen binding is cooperative. – That is, once one molecule of O2 is bound, others bind more easily. – It also means that at the tissues, O2 release is enhanced. • Oxygen saturation curves demonstrate the effect of PO2 and cooperative binding. • Systemic venous blood is still at least (>) 70% saturated with oxygen. Fig. 23.20, p. 863 77 Oxygen Saturation Curves Hb saturation depends on: • PO2 and PCO2; • temperature; • pH; and • blood bis-phosphoglycerate (BPG) levels. Fig. 23.20, p. 863 Fig. 23.21, p. 864 78 Oxygen Saturation Curves: PO2 & PO2 • The effect of PO2 is due to cooperative binding. As O2 binds, the protein (globin) changes shape, making it easier for the next O2 to bind. • CO2 binds to a different part of the Hb molecule. As it binds, it causes a change in the shape (conformation) of the Hb molecule. (See Chapter 2 for more on protein configurations.) – This shape (conformational) change makes it less favorable for oxygen binding (i.e., makes it easier for Hb to give up its oxygen). Fig. 23.20, p. 863 79 Oxygen Saturation Curves: pH and Temperature • pH is due to H+ concentration. – The Bohr effect refers to effect of pH on affinity of Hb for O2. ° The more H+, the lower the affinity of Hb for O2. – H+ results from carbonic acid or lactic acid, both of which are associated with active tissues. • Temperature also changes the shape of Hb. – Higher temperatures reduce the affinity of Hb for O2, making O2 release easier. – Higher temperatures are also associated with active tissues. Fig. 23.21, p. 864 80 Affect of NO • NO (nitric oxide) is secreted by endothelial cells of blood vessels and lungs. • Although it does not affect oxygen transport directly, it does affect vessel diameter, and therefore flow. – NO causes vasodilation of pulmonary and tissue capillaries and, thus, enhances gas exchange by increasing blood flow. 81 Metabolism Review • Aerobic Respiration uses O2 and produces CO2 – Glucose + 6 O2 6 CO2 + 6 H2O + 36 ATP – Aerobic respiration (also called cellular respiration) has three stages: ° glycolysis; ° the Kreb’s (citric acid or TCA) cycle; ° and electron transport coupled with chemiosmosis. • Anaerobic Respiration occurs in the absence of oxygen. – Glucose lactic acid + 2 ATP 82 Metabolism Review • By-products of glucose catabolism through glycolysis include: – BPG (bis-phosphoglycerate), an intermediate of glycolysis; – heat because the reactions are inefficient; and – H+, which lowers pH, from: ° carbonic acid, which is produced when CO2 combines with H2O, or ° lactic acid, which is a result of anaerobic respiration. 83 Summary of Factors Affecting O2 Transport Factors Affecting Association Favoring Hb-O2 Association Favoring Hb-O2 Dissociation Temperature Low High PO2 High Low PCO2 Low High pH High Low BPG Low High 84 Blood Gas Transport: Carbon Dioxide • 7-10% of CO2 is carried as dissolved carbon dioxide. • 20-30% is carried attached to the globin part of hemoglobin to form carbaminohemoglobin. • About 70% is converted to bicarbonate ions (HCO3-) for transport in plasma because of the reversible reaction between CO2 and H2O. – CO2 + H2O <=> H2CO3 <=> H+ + HCO3– This reaction occurs spontaneously in plasma. – This reaction occurs much more rapidly in RBCs due to presence of the enzyme carbonic anhydrase. 85 Carbon Dioxide Transport: Chloride Shift • CO2 enters RBCs at the body tissues where levels are relatively high; CO2 leaves RBCs at the lungs where it is released into the alveoli. • The chloride shift is the exchange of ions (Cl- and HCO3-) between plasma and RBCs. – At body tissues, Cl- enters the RBC and HCO3produced by the carbonic anhydrase reaction (previous slide) leaves. – At the lung, HCO3- enters RBCs as the carbonic anhydrase reaction reverses to produce CO2, Clleaves the RBC. (CO2 also leaves the RBC.) Fig. 23.22, p. 866 86 Carbon Dioxide Transport: Haldane effect • CO2 binds to reduced Hb more efficiently than to oxyhemoglobin. Therefore, – more CO2 is carried by Hb when O2 is low; and – as CO2 increases, O2 dissociation increases. Fig. 23.23, p. 867 87 Internal Respiration: Gas Movements • Internal respiration occurs between tissues and blood. • O2 enters the tissues from blood. • CO2 leaves the tissues to enter blood. 88 Factors Affecting Internal Respiration Factors affecting internal respiration include: • the surface area for exchange; – Surface area depends on the size of the capillary bed[s] serving the specific tissue; – The size of the capillary bed varies from tissue to tissue. For example, red twitch muscle has more capillaries than white twitch (see A&P I Unit 13 – Muscle) 89 Factors Affecting Internal Respiration • the partial pressure gradient, which is maintained in the lungs by ventilation; – hyperpnea and hypopnea change the gradients. – Think About It: What effect would each have on O2 levels? On CO2 levels? • the rate of blood flow, which varies with needs of tissue. – Blood flow increases during activity when O2 decreases and CO2 increases (see Topic 4). – Blood flow decreases when tissue is inactive and O2 is not removed nor CO2 produced as quickly. 90 Restrictive Pulmonary Disease • Restrictive Pulmonary Disease are ones in which total lung volume is reduced. • These diseases result in reduced total lung capacity, vital capacity and resting lung volume. • Causes of restrictive pulmonary disease include: – changes to lung tissue that reduce volume (e.g., pulmonary fibrosis, tuberculosis, pneumonia, pulmonary edema); and – changes to the pleurae, chest wall or respiratory musculature or nerves that reduce compliance. 91 Chronic Obstructive Pulmonary Disease (COPD) • COPDs are chronic diseases in which breathing is difficult and gets progressively worse; coughing and pulmonary infection are common. • Ventilation is impaired and the ability to exhale rapidly and forcefully is diminished. • Patient eventually develops respiratory failure. • COPDs are often (but not always) caused by long-term smoke inhalation • COPDs include: – cystic fibrosis, – emphysema, and – chronic bronchitis 92 COPDs • Cystic fibrosis (CF) is a congenital defect of the Cltransport protein in the plasma membrane. – The inability to transport Cl- into the lumen of the airways results in overproduction of thick mucus. This mucus reduces the usable diameter of the airways. – Gene therapy is ineffective because no one knows exactly what the stem cells are. http://www.vh.org/Providers/TeachingFiles/ITTR/CysticFibrosis/CFPA.html 93 COPDs • Emphysema results from the breakdown of intraalveolar walls. This causes permanent enlargement of the alveoli (which decreases surface area for gas exchange). The lungs become fibrous and inelastic • Chronic bronchitis is a chronic irritation and infection of the bronchi. • Both are associated with long-term smoking. http://www-medlib.med.utah.edu/WebPath/LUNGHTML/LUNG059.html http://pathhsw5m54.ucsf.edu/case25/image253.html 94 Inflammatory Respiratory Disorders • Pleurisy is an inflammation of pleural membranes results either in decreased fluid (increases friction) or fluid build up (increased intrathoracic = intrapleural pressure) • Asthma is an inflammation of the airways usually as an allergic reaction to airborne particles. – Asthma may be made worse by autonomic factors, infection (inflammation), exercise, and cold. – Asthma results in coughing, sneezing, dyspnea, wheezing, and tightness in the chest. 95 Infant Respiratory Distress Syndrome (RDS) • RDS is also known as hyaline membrane disease or HMD. • Lack of sufficient surfactants allows surface tension in the alveoli to increase resulting in collapse of alveoli on exhalation. Normal lung: http://www.usc.edu/hsc/dental/ghisto/lng/d_28.html RDS lung: http://axon.sote.hu/KKK/DESCRIPT/0131/0131001E.HTM 96 Infectious Respiratory Disorders • Pneumonia is a viral or bacterial infection of the lungs. • Bronchitis is a viral or bacterial infection of the bronchi. • Tuberculosis is a bacterial infection caused by Mycobacterium tuberculosis 97 Other Respiratory Disorders • Pneumothorax is presence of air in intrapleural space, as from a puncture wound. This allows the lung to collapse. Because the lungs are in separate cavities, one may collapse while the other stays inflated. • Lung cancer is a cancerous tumor. Cancer is often related to inhaled carcinogens (as are found in tobacco smoke). http://medicine.creighton.edu/medschool/VideoAtlas/Respiratory/Thoracic%2 0Neoplasia/webstuff/chestcancer1.html 98