2009년 스트레스와 간암에 대한 고찰
advertisement

직업적 스트레스와 간암발생에 대한 검토
직업적 스트레스와 과로가 간암의 발생에 영향을 미쳤는가?라는 질문에 답을 하기 위하여서
다음과 같은 세부적인 질문을 검토하도록 함
1.
직업적 스트레스와 과로가 면역력의 변화를 초래하여 염증을 악화시킴으로써 만성
간질환의 진행 및 악화를 초래하는지에 대한 검토
1) 스트레스는 면역력의 변화를 초래하여 염증을 악화시키는가?
2) 일반적으로 스트레스가 면역력의 변화를 초래한다면, 직업적 스트레스도 면역력의
변화를 초래하여 염증을 악화시키는가?
3) 스트레스로 인한 면역력의 변화는 간장질환에서 보이는 염증도 악화시키는가?
4) 직업적 과로와 스트레스도 간장질환의 염증도 악화시킬 수 있는가?
2.
직업적 과로와 스트레스로 초래된 만성 간질환의 진행 및 악화가 궁극적으로 간암의
발생을 초래할 수 있는지에 대한 검토
1) 만성 간질환의 진행과 악화가 간암의 발생을 초래할 수 있는가?
2) 스트레스로 인한 만성 간질환의 진행과 악화가 간암의 발생을 초래할 수는 있는가?
3) 직업적 과로와 스트레스도 만성 간질환의 진행과 악화를 통하여 간암의 발생을
초래할 수 있는가?
1.
직업적 과로와 스트레스가 면역력의 변화를 초래하여 염증을 악화시킴으로써 만성
간질환의 진행 및 악화를 초래하는지에 대한 검토
1) 스트레스는 면역력의 변화를 초래하여 염증을 악화시키는가?
스트레스, 특히 사회심리적인 스트레스가 면역력에 영향을 미친다는 것은 다음과 같은 관찰들에
근거하여 잘 알려져 있음
과로나 긴장을 하고 난 이후 헤르페스, 대상포진 등의 바이러스성 질환이 호발 한다는
점,
예방주사를 맞고 형성되는 질환 대항 항체의 생성여부도 스트레스에 따라 달라진다는 점
한편 스트레스가 면역력에 영향을 미치는 현상은 스트레스로 인한 신체의 일차적인 반응으로서
자율신경계의
교감신경
흥분을
통한
신경전달물질(epinephrine,
norepinephrine)의
분비가
염증세포의 변화를 가져오며, 또한 스트레스 호르몬으로 알려진 뇌하수체-부신피질에서 분비되는
부신피질호르몬 등이 염증의 유발과 조절에 관여한다는 것에 근거하여 그 기전이 설명되고 있음
이러한 스트레스로 인한 면역력의 변화는 스트레스의 종류 혹은 그 기간이나 정도에 따라 서로
다른 양상을 보이고 있으나, 스트레스를 체계적으로 구분할 때, 면역력 변화도 일정한 양상을
보인다는 점이 설명되고 있음
지난 30년 동안의 스트레스와 면역력의 관계에 대한 조사결과를 종합 분석하였을 때, 다음과
같은 결과가 제시됨:
Psychological Stress and the Human Immune System: A Meta-Analytic
Study of 30 Years of Inquiry (Segerstrom and Miller 2004)
수 분에서 수십 분 동안의 급성 스트레스 (예: 대중연설)
면역세포의 재배치를 통한 비특이 면역세포들의 증가
수 일에서 수십 일 간 제한된 기간 동안의 자연적 스트레스 (예: 기말시험준비)
특이 면역세포 기능의 변화를 통하여 세포면역기능(Th1) 감소와 항체면역기능(Th2) 증강
몇 달 혹은 몇 년에 걸쳐 그 종료가 기약 없이 만성적으로 지속되는 스트레스 (예:
신분의 변경, 만성질환자의 간호)
특이 및 비특이 면역 기능 모두 감소하여 세포면역기능 및 항체면역기능을 포함한 모든
면역기능의 약화
2) 스트레스가 면역력의 변화를 초래한다면, 직업적 과로와 스트레스도 면역력의 변화를
초래하여 염증을 악화시키는가?
일반적으로 간염환자에게 규칙적인 운동을 권하는 것은 수 십분 정도의 짧은 시간 동안 급격한
신체적 정신적 긴장이 면역세포의 재배치를 통한 비특이적 면역세포의 증가와 같은 적응기전을
통하여 면역을 일시적으로 항진시키기 때문임
그러나
이와
같은
신체적
정신적
긴장이
수일
이상
지속되는
자연적
스트레스는
세포면역기능(Th1)의 감소와 항체면역기능(Th2)의 증가를 가져와 세포면역기능과 항체면역기능의
불균형을 초래한다는 사실이 알려져 있으며, 이러한 기전은 스트레스로 인한 염증의 악화, 특히
천식, 아토피성 질환 등과 같은 만성적인 염증질환의 악화를 설명하는 근거를 제공하고 있음
(Kemeny and Schedlowski 2007)
한편 직업적 과로와 스트레스의 경우에도 다른 일반적인 스트레스와 같은 면역력의 변화를
초래하는 것으로 보고되고 있으며, 단지 직업적 과로와 스트레스의 경우 앞서 예시한 단기간의
시험을 앞두고 경험하는 스트레스와 같은 급성적 스트레스와는 달리 비교적 만성적으로 지속하는
스트레스로서, 좀 더 많은 보고에서 비특이적 면역 및 특이면역 모두, 그리고 특이면역 중에서도
세포면역과 항체면역기능 모두를 저하시키는 효과를 가져오는 것으로 보고되고 있음 (De Gucht,
Fischler et al. 1999; Nakamura, Nagase et al. 1999; Yang, Koh et al. 2002)
특히 이러한 직업적 스트레스와 관련하여 교대근무가 면역력에 미치는 영향에 대한 조사가
이루어지고 있으며, 일반적으로 교대근무가 신체대사활동의 변화를 가져와 부신피질호르몬과
같은 면역반응에 작용하는 호르몬의 변화도 가져오는 것으로 알려져 있는 만큼, 교대근무로 인한
세포면역반응의 변화가 다양하게 보고되고 있음 (Di Donato, Di Giampaolo et al. 2006)
3) 스트레스로 인한 면역력의 변화는 간장질환에서 보이는 염증도 악화시키는가?
스트레스로 인한 면역력의 변화는 간장질환의 악화를 설명하는 기전을 또한 제공하고 있음
특히 육체적인 스트레스는 물론 사회정신적인 스트레스를 받고 나서 그 증세가 더 나빠지는 것을
보고하고 있으며, 이러한 사회정신적인 스트레스가 간질환을 악화시키는지, 그리고 그러한 악화의
기전은 무엇인지에 대한 연구는 최근 그 깊이를 더하여 기본적인 병리상태에 대한 설명을 아래와
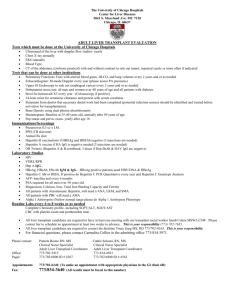
같이 자세히 제시하고 있음 (Yoichi Chida 2006)
Figure
3
A
simplified
of
the
representation
schematic
pathophysiological
interaction of the brain with the liver. The
hypothalamic–pituitary–adrenal (HPA) axis,
together with the autonomic nervous system,
represents the salient transducers of stress
into effects on liver diseases. Stressful stimuli
can activate the HPA axis and the efferent
hypothalamus–adrenal medulla–epinephrine
and
hypothalamus–hepatic
sympathetic
nerve–norepinephrine axes, which in turn
release glucocorticoids and catecholamines,
respectively. In addition to the established
sensory role of the afferent nerves in the
hepatic
inflammation,
parasympathetic
pathway
inflammatory effect,
stress-induced
the
has
efferent
an
anti-
which suggests that
impairment
of
such
an
inhibition may exacerbate liver diseases.
Solid
lines,
inhibition.
stimulation;
Ach,
dashed
acetylcholine;
lines,
ACTH,
adrenocorticotropic hormone; DMN, dorsal
motor
nuclei;
E,
epinephrine;
GCs,
glucocorticoids; HBF, hepatic blood flow; IL-6,
interleukin-6;
LC,
locus
ceruleus;
NE,
norepinephrine; NKT, natural killer T cells;
NTS, nucleus tractus solitarii; TNF-, tumor
necrosis factor-.
4) 직업적 과로와 스트레스는 간장질환의 염증도 악화시킬 수 있는가?
기존 만성간염, 간경화 등을 비롯한 만성 간질환 환자들의 대부분은 스트레스를 받고 나서
간장질환의 증세가 악화되는 것을 보고하고 있으며 (Fukudo, Suzuki et al. 1989; Swain 2000), 특히
만성 B 형 간염 환자들에게서 스트레스로 인한 우울증세의 정도를 조사하였을 때, 그 증세의
정도와 비례하여 간장기능의 변화가 관찰되고 있음 (Kunkel, Kim et al. 2000)
한편 성격적 특성과 만성 간염의 정도를 조사하였을 때, 강박적으로 다른 사람들에게 잘 보여야
하며, 자신을 엄격하게 다스리고, 높은 애국심을 보이는 등의 특징을 갖고 있는 1 형 성격의
보유자에게서 그 성격적 특성이 강할수록 간염의 정도가 심한 것이 보고되고 있음 (Nagano,
Nagase et al. 2004)
특정 직업과 간장질환의 염증 악화를 직접적으로 조사한 의학적 보고는 아직 없으나, 직업적
과로 및 스트레스의 지표로서 혈중 부신피질호르몬을 측정하고, 한편 그 영향지표로 간기능을
측정하였을 때, 두 가지 지표 사이에 역방향의 밀접한 관련성이 보고되고 있어 (H?enstam and
Theorell 1990), 직업성 스트레스 또한 스트레스 발생의 일반적인 원인으로서 가장 큰 비중을
차지하는 원인의 하나라는 점에서 직업성 스트레스로 인한 간장질환의 악화가 예상되고 있음
2.
직업적 과로와 스트레스로 초래된 만성 간질환의 진행 및 악화가 궁극적으로 간암의
발생을 초래할 수 있는지에 대한 검토
1) 만성 간질환의 진행과 악화가 간암의 발생을 초래할 수 있는가?
일반적으로 B 형 간염에 걸린 사람들 중의 일부가 보균자로 남으며, 이러한 보균자들 중의
일부에서 만성 간질환이 발생 진행을 함
만성 B 형 간염의 경우 다음과 같은 세 가지 기전으로 인하여 간암발생이 많은 것으로 파악되고
있는 바, 이러한 기전 중에서 가장 중요한 기전은 일부 B 형 간염 보균자에게 만성적인
면역상태의 저하가 발생하고, 이를 통하여 변형된 세포가 제거되지 못하고 간암으로 진행하는
기전이 가장 유력하게 제시되고 있음 (Cougot, Neuveut et al. 2005; Lupberger and Hildt 2007)
B 형 간염을 통한 간암의 발생기전
① 정상 세포에 B 형 간염의 유전자가 삽입되어 유전자 변형을 통해 암이 발생
② B 형 간염 바이러스에 의하여 만들어진 단백질을 통해 변형이 일어남
③ 만성간염과 그에 따른 세포재생, 그리고 간경변이 발생하는 과정에서 비특이적으로 암이
발생
특히 간암발생에 이르는 만성 B 형 바이러스성 간염의 발생과 지속에 있어 비특이적 면역상태의
변화가 중요한 역할을 한다는 증거는 간이식, 그리고 후천성면역결핍증 등과 같은 비특이적
면역상태의 변화가 초래된 상태에서 B 형 바이러스성 간염이 재/병발하거나 진행되어 간암이
발생한다는 관찰에 근거하고 있음
간이식 수술환자 (조직거부반응을 낮추기 위해 면역억제제 사용) -> B 형 바이러스성
간염의 재발 (Olivera-Mart?ez and Gallegos-Orozco 2007)
후천성 면역결핍증 (Acquired Immune Deficiency Syndrome, AIDS) 환자 -> B 형
바이러스성 간염에 동시에 감염 -> 간암의 발생 (E. Herrero Mart?ez 2001; Sulkowski
2008)
2) 스트레스로 인한 만성 간질환의 진행과 악화가 간암의 발생을 초래할 수는 있는가?
스트레스가 만성 간질환을 악화시키고, 또한 이를 통하여 간암이 발생하거나 확산되는 현상을
설명하는 기전으로 스트레스로 인한 면역상태의 변화가 최종적으로 간장에의 염증을 야기하며,
또한 이러한 과정을 거쳐 암세포를 비롯한 비정상세포의 발생과 확산이 저지되지 못하여 간암이
발생/악화하는 증거들이 제시되고 있음
The role of psychosocial factors in the progression of hepatocellular carcinoma (Steel,
Carney et al. 2004)
스트레스로 비롯된 간장질환의 악화로 인한 간암발생의 근거로서 간암발생과 치료에 영향을
미치는 면역상태의 변화가 조사되고 있으며, 특히 만성 바이러스성 간염 환자 중 간암으로
이행되거나 혹은 이행되지 않고 다른 경과를 밟는 사례들을 비교하였을 때, 면역상태의 변화,
특히 세포면역상태의 변화가 간암발생과 치료에 선행한다는 관찰 등이 바이러스성 간염의
간암으로 진행에 스트레스로 인한 비특이적 면역상태의 변화가 관여한다는 증거로 제시되고 있음
만성간염 -> Natural Killer (NK) cell 활동의 감소 -> 간암의 발생 (Ono, Yamanaga et al.
1996)
만성간염 -> 세포면역세포 (CD8+ 임파구) 활동감소 -> 간암 (Chavan and Chiplunkar
1997; Hagihara, Shimura et al. 1997; Yoshito Wada 1998)
만성간염 -> Interleukin-2 감소 -> 간암 (Huang, Chen et al. 1996; K Wadamori 1996)
만성간염 -> Lymphokine-activated killer (LAK) 활동 감소 -> 간암 (Shirai, Watanabe et al.
1990; Haruta, Yamauchi et al. 1996)
최종적으로
스트레스로
인한
면역력의
변화가
직접적으로
간암의
발생과
진행에
영향을
미치는지에 대한 여부를 조사하였을 때, 우울증의 정도에 따라 면역세포, 특히 Natural Killer Cell
(NK cell)의 개수와 활동이 변화되며, 그에 따라 간암환자의 생존율이 달라지는 것이 보고되고
있음 (Steel, Geller et al. 2007)
3) 직업적 과로와 스트레스도 만성 간질환의 진행과 악화를 통하여 간암의 발생을
초래할 수 있는가?
일반적으로 스트레스로 인한 암의 발생과 진행은 그 기전에 있어 면역상태의 변화를 통하여
초래되는 것으로 파악되고 있어, 암 중에서도 특히 바이러스의 활동에 의한 암의 발생과 진행에
그 영향이 더 클 것으로 파악되고 있음
기존의 사회심리적 스트레스와 암의 발생 및 악화에 대하여 종합적으로 정리하였을 때, 일부
스트레스, 특히 주관적으로 느끼게 되는 부정적인 감정, 무기력감, 혹은 이러한 감정들의 억압
등이 암의 발생과 진행에 밀접한 영향을 미치고 있는 것으로 보고되고 있음 (Garssen 2004)
한편
스트레스
반응과
연관하여
교대근무
또한
일중주기(circadian
rhythm)의
혼선을
가져옴으로써 면역체계와 호르몬체계의 신체조절기능의 손상을 가져와 결과적으로 발암작용을
촉진하는 것으로 알려져 있으며(Sephton and Spiegel 2003), 지난 2007 년도에 세계보건기구(WHO)
산하 국제암연구소(IARC, International Agency for Research on Cancer)에서 발암물질(Probable
Carcinogen, 2A)로 분류하였음 (http://monographs.iarc.fr/ENG/Meetings/vol98-pressrelease.pdf)
아직까지 경찰, 특히 과학수사대원으로서의 복무로 인한 스트레스가 만성 간질환의 진행과
악화를 통하여 간암의 발생에 영향을 미칠 수 있는지에 대한 직접적인 조사결과가 학계에서
조사되어 보고되고 있지 않음
그러나 다음과 같은 점들에 근거하여 본 사례에서 직업으로부터의 과도한 스트레스를 야기하는
복무가 간암의 발생에 영향을 미칠 수 있었다고 판단됨
① 본 사례에서 복무하면서 수행하여야 하는 특수업무가 갖는 심리적 압박감, 3 년 동안
하루 평균 2 회 정도 출동하여 조사하여야 하였던 복무시간의 과도함 등에 근거하여
복무로 인한 스트레스가 상당하였을 것으로 판단된다는 점
② 한편 본 사례에서 기존의 간질환을 악화시킬 수 있는 독성물질에의 노출이 현직에
복무하면서 상당하였다는 점
③ 또한 본 사례에서 불규칙적인 교대근무를 복무기간 동안 계속 수행하여야 하였다는
점에서 생리적 균형을 깨는 스트레스가 상당하였을 것으로 판단된다는 점
④ 그리고 일반적으로 바이러스의 활동에 의한 암의 발생과 진행에 면역상태의 변화가
영향을 미치며, 특히 만성 간질환의 진행 및 악화는 비특이적 면역기전을 통하여
궁극적으로 간암의 발생을 증가시킨다는 사실
⑤ 이상 종합적으로 보았을 때, 업무상 수행하여야 하는 복무내용 및 복무시간, 복무 중의
간독성유해물질 노출, 그리고 생리적인 부담을 초래하는 교대근무 등으로 인하여 발생한
면역학적 변화가 만성 간질환의 진행을 촉진하여 간암의 발생과 진행을 초래하였을
것으로 판단되고 있음
참고문헌
Chavan, S. S. and S. V. Chiplunkar (1997). "Immunophenotypes and cytotoxic functions of
lymphocytes in patients with hepatocellular carcinoma." Tumorigenesis 83(4): 762-767.
AIMS AND BACKGROUND: Hepatocellular carcinoma (HCC) is one of the most common
cancers in Asia. Immunological mechanisms are thought to play an important role in the
control of tumor progression. The immune responses in HCC patients are poorly
understood. In the present study, the proliferation and cytotoxic functions of lymphocytes
from tumor tissues and peripheral blood of HCC patients were analysed. Simultaneously,
the microcultures were phenotyped in order to determine the involvement of different
lymphocyte subsets in mediating the cytotoxic function. METHODS: The frequencies of
proliferating and cytotoxic lymphocytes from three tumor tissues and peripheral blood
from ten HCC patients and nine healthy individuals were assessed by limiting dilution
microculture analysis. These microcultures were phenotyped by single and dual color flow
cytometry using monoclonal antibodies specific for CD4, CD8, CD56 and HLA-DR markers.
RESULTS: The precursor frequencies of both proliferating and cytotoxic lymphocytes were
found to be comparable in the peripheral blood of HCC patients and healthy individuals.
Compared to peripheral blood, a marked reduction in the precursor frequencies of
proliferating and cytotoxic lymphocytes was observed in the tumor tissues of HCC patients.
In the tumor tissues, a significantly higher frequency of cytotoxic T cells compared to
natural killer cells was observed. Dual color flow cytometric analysis revealed increased
percentages of CD8+ HLA-DR+ lymphocytes compared to CD4+ HLA-DR+ cells in the
tumor tissues. CONCLUSIONS: Our results suggest that depressed immune responses at
the tumor site might be responsible for the escape of tumor cells from the immune
surveillance of the host.
Cougot, D., C. Neuveut, et al. (2005). "HBV induced carcinogenesis." Journal of Clinical Virology
34(Supplement 1): S75-S78.
Hepatocellular carcinoma (HCC) is one of the rare human neoplasms associated with viral
infections. Hepatitis B virus (HBV) and hepatitis C virus (HCV) are the most important
etiological factors of HCC, accounting for more than 70% of cases worldwide. The risk of
HCC development is greatly increased in chronic viral carriers exposed to other recognized
risk factors, including exposure to aflatoxin B1, alcoholic cirrhosis and diabetes. The
importance of HBV genotypes and precore or core promoter mutants remains
incompletely understood. The role of HBV in tumour formation appears to be complex
and may involve both direct and indirect mechanisms. Integration of HBV DNA into the
host genome occurs at early steps of clonal tumour expansion, and it has been shown to
induce direct insertional mutagenesis of diverse cancer-related genes in a number of cases.
Chronic liver inflammation and hepatic regeneration induced by cellular immune
responses may favour the accumulation of genetic alterations in infected hepatocytes.
Prolonged expression of the viral regulatory protein HBx and the large envelope protein
LHBs may contribute in deregulating the cellular transcription program and proliferation
control, and sensitize liver cells to carcinogenic factors. Recent genetic studies have
provided insight into the mechanisms underlying viral-associated hepatocarcinogenesis. It
has been shown that the rate of chromosomal alterations is significantly increased in HBVrelated tumours compared with tumours associated with other risk factors. HBV might
therefore play a role in enhancing genomic instability. Inactivation of p53 by mutations
and regional allelic deletions is found more frequently in tumours associated with HBV
infection. By contrast, HBV related tumours harbour a low rate of [beta]-catenin mutations.
Together, these data strongly support the notion that chronic HBV infection might trigger
specific oncogenic pathways, thus playing a role beyond stimulation of host immune
responses and chronic necro-inflammatory liver disease.
De Gucht, V. o., B. Fischler, et al. (1999). "Immune dysfunction associated with chronic professional
stress in nurses." Psychiatry Research 85(1): 105-111.
The relationship between chronic professional stress in nurses and immunity as well as the
possible impact of psychopathology upon this relationship have been examined. Sixty
subjects were selected on the basis of high/low scores on professional stress and
psychopathology. Chronic professional stress appeared to be associated with immune
dysfunction including signs of immune activation (increased numbers of cells expressing
the interleukin-2 receptor, especially CD4+CD25+ cells) and possibly immune suppression
(decrease in percentage of natural killer cells). The increase in activation markers,
CD3+CD16CD56+ cells and serum neopterin was most pronounced in the group with
high stress/low psychopathology whereas the decrease in CD8+CD11b+ cells was most
pronounced in the group with high stress/high psychopathology. It is hypothesized that in
the presence of chronic stress distinct psychological mechanisms are associated with
specific immune dysfunctions.
Di Donato, A., L. Di Giampaolo, et al. (2006). "Effect of occupational stress and anxiety on natural
killer lymphocyte activity of men and women employed in a university." Int J Immunopathol
Pharmacol 19(4 Suppl): 79-84.
The aim of this study is the immune response of the staff of a university and a museum
(referent group). 46 women and 40 men with similar mean age (44 years) were
investigated. The first group of women (A) worked in libraries, B in offices in contact with
students, C as secretaries and D in a museum. One group of men (E) was composed of
employees of the university, one worked in a library temporarily located underground (F)
and the last group (G) in a museum. STAI I and II (state and trait anxiety, respectively), and
occupational stress were measured by questionnaires. Blood samples were collected for
determining NK cytotoxic activity vs human erythroleukaemia cells and the lymphocyte
subsets CD45+, CD45+-CD3+, CD45+-CD3+-CD4+, CD45+-CD3+-CD8+, CD45+-CD3CD8+, CD3+-CD16+-56+ and CD3+-CD19+. Group B showed significantly higher score of
occupational stress and STAI I (but not of STAI II) than the other groups of women. Group
F of men showed higher levels of occupational stress and both STAI I and II than groups E
and G. Group B of women and F of men also showed significantly lower values of blood
cytotoxic activity. The scores of STAI I and II were negatively correlated with the cytotoxic
activity expressed per ml of blood and/or total lymphocytes. and/or NK CD45+-CD16+CD56+ cells. In conclusion, this study shows that occupational stress may increase anxiety
which is negatively correlated with blood cytotoxic activity. This is a useful tool for
determining the health effects of stress.
E. Herrero Mart?ez (2001). "Hepatitis B and hepatitis C co-infection in patients with HIV." Reviews
in Medical Virology 11(4): 253-270.
An Erratum has been published for this article in HAART has increased the life expectancy
of patients with HIV. However, as their life expectancy increases, it becomes increasingly
important to focus on the management of concurrent illnesses such as chronic HBV and
HCV infections which have the potential to increase mid to long term morbidity and
mortality. Shared epidemiological risks have resulted in the HIV infected population having
a higher incidence of both HBV and HCV than those uninfected with HIV. Co-infection
with HIV modifies the natural history of HBV infection, increasing the rate of viral
replication,
risk
of
carriage
and
chronic
hepatitis
but
without
increasing
liver
necroinflammatory processes. In chronic HCV infection, the presence of HIV enhances the
risk of severe liver disease. There is no evidence as yet that HBV directly impacts on HIV
disease progression but HCV infection increases the risk of death or an AIDS defining
illness and impairs CD4+ T cell recovery during antiretroviral therapy. Treatment of either
hepatitis virus is complex because of pharmacokinetic interactions with components of
HAART regimens. Copyright ?2001 John Wiley & Sons, Ltd.
Fukudo, S., J. Suzuki, et al. (1989). "Impact of stress on alcoholic liver injury; a histopathological
study." Journal of Psychosomatic Research 33(4): 515-521.
Certain behaviors can have an influence on the cause and progression of liver disorders.
To clarify the relation between histopathological change of the liver and psychosocial
stress, behavioral traits, and psychological state, patients with fatty liver (n = 14) were
compared with patients with chronic hepatitis (n = 16). Both groups were alcohol-induced
without other causes and consumed the same dose of alcohol. By morphometric methods,
fat deposit ratio (FDR) and degree of liver damage (DLD) which reflects lobular fibrosis,
inflammatory cell infiltration, and necrosis were evaluated. Life Change Unit scores from
the Social Readjustment Rating Scale were significantly higher in chronic hepatitis than in
fatty liver (p < 0.001). DLD was significantly correlated with Life Change Unit (r = 0.59, p <
0.01). It is suggested that psychosocial stress is one of the aggravating factors of fibrosis
and inflammatory change of the liver which is previously damaged by alcohol in man just
like the rat liver following stress.
Garssen, B. (2004). "Psychological factors and cancer development: Evidence after 30 years of
research." Clinical Psychology Review 24(3): 315-338.
The question whether psychological factors affect cancer development has intrigued both
researchers and patients. This review critically summarizes the findings of studies that have
tried to answer this question in the past 30 years. Earlier reviews, including meta-analyses,
covered only a limited number of studies, and included studies with a questionable design
(group-comparison, cross-sectional or semiprospective design). This review comprises only
longitudinal, truly prospective studies (N=70). It was concluded that there is not any
psychological factor for which an influence on cancer development has been convincingly
demonstrated in a series of studies. Only in terms of [`]an influence that cannot be totally
dismissed,' some factors emerged as [`]most promising': helplessness and repression
seemed to contribute to an unfavorable prognosis, while denial/minimizing seemed to be
associated with a favorable prognosis. Some, but even less convincing evidence, was
found that having experienced loss events, a low level of social support, and chronic
depression predict an unfavorable prognosis. The influences of life events (other than loss
events), negative emotional states, fighting spirit, stoic acceptance/fatalism, active coping,
personality factors, and locus of control are minor or absent. A methodological
shortcoming is not to have investigated the interactive effect of psychological factors,
demographic, and biomedical risk factors.
H?enstam, A. and T. e. Theorell (1990). "Cortisol elevation and serum [gamma]-glutamyl
transpeptidase in response to adverse job conditions: How are they interrelated?" Biological
Psychology 31(2): 157-171.
This study explores the use of plasma cortisol as an indicator of psychologically straining
work. As plasma cortisol and liver function might be associated through biological
mechanisms, this paper has a secondary object, namely to explore the interaction between
cortisol and liver function. As an index of liver function the serum level of [gamma]glutamyl transpeptidase (GT) was used. The study sample was 2,000 prison employees
from 67 different prisons in Sweden. Questionnaires and health examinations were used as
well as measurements of plasma cortisol and serum GT. Very few work-related factors were
associated with plasma cortisol unless analyzed separately for high and low level of serum
GT. Two-way analyses of variance showed significant differences in the physiological
"responses" to straining work with regard to psychic strain at work (men), social support
at work (men), job role (men), loneliness at work (men and women), management style
(women) and overtime work (women) between "low serum GT" and "high serum GT"
individuals. Aggregated analyses showed that prison means of work-related factors were in
some respects associated with prison means of plasma cortisol. The conclusion is that in
individually based analyses plasma cortisol is difficult to use as an indicator of straining
work, especially if the level of serum GT is unknown.
Hagihara, M., T. Shimura, et al. (1997). "Serum concentrations of soluble HLA-class I and CD8
forms in patients with viral hepatic disorders." Journal of Gastroenterology 32(3): 338-343.
Soluble HLA-class I and CD8 molecules were determined by sandwich ELISA in patients
with viral-induced hepatic disorders. As a whole, the patients with hepatic disorders (acute
hepatitis: AH; chronic hepatitis: CH; liver cirrhosis: LC; hepatocellular carcinoma: HCC)
showed higher sHLA-class I and sCD8 levels than normal controls (P < 0.001). AH patients
had the highest sHLA-class I levels (mean, 3513 +/- 2112 ng/ml), followed by CH (2896
+/- 1290 ng/ml), LC (2293 +/- 1266 ng/ml), and HCC (2221 +/- 1212 ng/ml) sCD8 levels
wer highest in AH, followed by HCC, LC, and CH, in that order. Among histologically
defined C virus-positive patients, sHLA-I levels were higher in those with chronic active
hepatitis (CAH) 2A (3802 +/- 1124 ng/ml) than in those with chronic persistent hepatitis
(CPH; 2200 +/- 711 ng/ml; P < 0.01), the levels then decreased as the disease progressed
(CAH2B, 3564 +/- 1783 ng/ml, LC, 2376 +/- 1265 ng/ml). In contrast, sCD8 values showed
little difference among the disorders. sHLA-class I levels showed a positive correlation with
sCD8 values both in whole patients and in patients with AH (P < 0.01), but no correlation
was shown, in any patients, with biochemical parameters such as GPT and GOT. These
findings, taken together, suggest that hepatic destruction is not the only cause of sHLAclass I production, but that sHLA-class I levels, together with sCD8 levels, may reflect
immunological activity in hepatic disorders.
Haruta, I., K. Yamauchi, et al. (1996). "Analytical study of the clinical response to two distinct
adoptive immunotherapies for advanced hepatocellular arcinoma: comparison between LAK cell
and CTL therapy." J Immunother Emphasis Tumor Immunol 19(3): 218-223.
To evaluate the effect of two distinct adoptive immunotherapies, tumor-specific cytotoxic
T-cell (CTL) therapy and lymphokine-activated killer (LAK) cell therapy, the clinical
responses of patients with stage IV primary hepatocellular carcinoma (HCC) treated with
these therapies were studied. Of 18 patients treated with CTL, 3 had complete regression
(CR), 2 had partial regression, and 3 had minor regression (MR). Their median survival was
21 months after the end of therapy, and 1 CR patient survived for > 6 years. On the other
hand, in the LAK-cell-treated group of eight patients, four had MR and their median
survival was only 2 months. No survival was observed 27 months after the end of LAK cell
therapy. These results indicate that tumor-specific CTL therapy is more effective than LAK
cell therapy and that it might be a promising therapeutic tool for advanced HCC patients.
Huang, H., S. H. Chen, et al. (1996). "Gene therapy for hepatocellular carcinoma: long-term
remission of primary and metastatic tumors in mice by interleukin-2 gene therapy in vivo." Gene
Therapy 3(11): 980-987.
To explore gene therapy as a new treatment modality for hepatocellular carcinoma, a preclinical animal model was established by intrahepatic implantation of a mouse
hepatocellular carcinoma cell line (MH134) in syngeneic recipients. The resulting hepatic
tumors were treated with a recombinant adenoviral vector expressing the murine
interleukin-2 (IL-2) gene, and long-term remission was achieved in 50% of the animals.
The remaining animals died of malignant ascites, which also occurs in some human
patients. Those animals were treated with a second dose of the recombinant adenoviral
vector by direct inoculation into the peritoneal cavity, and long-term remission of the
disseminated disease was achieved in 55% of the animals. Thus, a combined cure rate of
greater than 75% for primary- and disseminated hepatocellular carcinoma was achieved
by
successive
adenovirus-mediated
IL-2
gene
treatments.
Histopathological
and
immunocytochemical analyses showed massive infiltration of the tumor by macrophages
and T lymphocytes in IL-2 vector treated animals. The surviving animals developed
systemic antitumoral cellular immunity that protected them against challenges of parental
hepatoma cells implanted at distant sites. The results suggest that IL-2 gene therapy may
be a strategy applicable for the treatment of both primary and metastatic hepatocellular
carcinomas in man.
K Wadamori, M. O., N Tokuda, Y Fujikura, S Hazama, T Fukumoto, T Suzuki, (1996). "Influence of
continuous interleukin-2 administration via the portal vein on liver regeneration following partial
hepatectomy in rats." Hepatology 23(6): 1578-1583.
We have reported the efficacy of intraarterial-combined immunochemotherapy including
interleukin-2 (IL-2) for unresectable hepatocellular carcinoma (HCC). To further test this
therapy for prevention of intrahepatic recurrence after hepatectomy, the influence of IL-2
on liver regeneration was examined using mitotic index (MI) and the bromodeoxyuridine
(BrdU) labeling index (LI) in 70% hepatectomized Donryu rats. In addition, gap junction
appearance, which may change during liver regeneration, was analyzed using a
monoclonal antibody (HAM8). Serum albumin, alanine transaminase, and total bilirubin (TB)
levels were also evaluated. IL-2 (45,000 Japanese reference units [JRU]/d) or saline was
administered continuously via the portal vein immediately after hepatectomy using an
infusion pump. We also examined the influence of IL-2 on liver regeneration after
hepatectomy with splenectomy. No difference in the weight of the liver, serum albumin,
alanine transaminase, or TB was observed in any groups at 1, 2, or 4 days after
hepatectomy. Neither IL-2 nor splenectomy influenced MI and BrdU LI at all three points.
Gap junctions began to disappear after hepatectomy and reached a minimum on day 2 in
all groups. Four days after hepatectomy, the density of the reappearing gap junctions was
markedly lower in groups treated with IL-2 than in those receiving saline with or without
splenectomy. However, the density returned to close to preoperative levels 6 days after
hepatectomy in all groups. Continuous portal infusion of IL-2 transiently disturbed gap
junction reappearance during liver regeneration. However, no other parameters of liver
regeneration or liver functions differed. These results suggest that the liver regeneration
after partial hepatectomy may be suppressed by the administration of IL-2, even though
the suppression may not be harmful for overall recovery of the resected liver. However, it
seems that hepatic IL-2 administration can be performed without serious complications
after hepatectomy.
Kemeny, M. E. and M. Schedlowski (2007). "Understanding the interaction between psychosocial
stress and immune-related diseases: A stepwise progression." Brain, Behavior, and Immunity 21(8):
1009-1018.
For many years, anecdotal evidence and clinical observations have suggested that
exposure to psychosocial stress can affect disease outcomes in immune-related disorders
such as viral infections, chronic autoimmune diseases and tumors. Experimental evidence
in humans supporting these observations was, however, lacking. Studies published in the
last 2 decades in Brain, Behavior and Immunity and other journals have demonstrated that
acute and chronic psychological stress can induce pronounced changes in innate and
adaptive immune responses and that these changes are predominantly mediated via
neuroendocrine
mediators
from
the
hypothalamic-pituitary-adrenal
axis
and
the
sympathetic-adrenal axis. In addition, psychological stress has predicted disease outcomes
using sophisticated models such as viral challenge, response to vaccination, tracking of
herpesvirus latency, exploration of tumor metastasis and healing of experimental wounds,
as well as epidemiological investigations of disease progression and mortality. These
studies have contributed significantly to our understanding that the neuroendocrineimmune interaction is disturbed in many pathophysiological conditions, that stress can
contribute to this disturbance, and that malfunction in these communication pathways can
play a significant role in the progression of disease processes. There are, however,
significant gaps in the extant literature. In the coming decade(s), it will be essential to
further analyze neuroendocrine-immune communication during disease states and to
define the specific pathways linking the central nervous system to the molecular events
that control important disease-relevant processes. This knowledge will provide the basis
for new therapeutic pharmacological and non-pharmacological behavioral approaches to
the treatment of chronic diseases via specific modulation of nervous system-immune
system communication.
Kunkel, E. J. S., J. S. Kim, et al. (2000). "Depression in Korean Immigrants With Hepatitis B and
Related Liver Diseases." Psychosomatics 41(6): 472-480.
The authors evaluated 50 Korean immigrants who had chronic viral hepatitis or who were
healthy carriers for the hepatitis B virus in terms of the relationships between their
depression scores, psychosocial stressors, social support, and biological markers of
dysfunction. All participants completed a questionnaire, describing their worries and
concerns, and the short form of the Beck Depression Inventory (BDI-sf). Hepatic
transaminases, albumin levels, and prothrombin times were measured during routine clinic
follow-up visits and were abstracted from the medical record. Values recorded within 3
months before and within 3 months after the psychiatric interview were correlated with
BDI scores. BDI-sf total scores were significantly associated with transaminase elevations
(P<0.001) both before and after BDI-sf administration. BDI scores were not associated with
other measures of liver dysfunction or other medical causes of depression. Patients with
higher BDI-sf total scores had more psychosocial stressors (P=0.008) and lower Global
Assessment of Functioning (GAF) scores (P=0.000).
Lupberger, J. and E. Hildt (2007). "Hepatitis B virus-induced oncogenesis." World J Gastroenterol
13(1): 74-81.
Hepatocellular carcinoma (HCC) is one of the most common cancers in the world with an
annual incidence of more than 500 000 in the year 2000. Its incidence is rising in many
countries. Recently, it has been estimated that about 53% of HCC cases in the world are
related to hepatitis B virus (HBV). The epidemiological association of HBV with HCC is well
established. In recent studies, it was revealed that HBsAg carriers have a 25-37 times
increased risk of developing HCC as compared to non-infected people. At present, HBVassociated carcinogenesis can be seen as a multi-factorial process that includes both
direct and indirect mechanisms that might act synergistically. The integration of HBV DNA
into the host genome occurs at early steps of clonal tumor expansion. The integration has
been shown in a number of cases to affect a variety of cancer-related genes and to exert
insertional mutagenesis. The permanent liver inflammation, induced by the immune
response, resulting in a degeneration and regeneration process confers to the
accumulation of critical mutations in the host genome. In addition to this, the regulatory
proteins HBx and the PreS2 activators that can be encoded by the integrate exert a tumor
promoter-like function resulting in positive selection of cells producing a functional
regulatory protein. Gene expression profiling and proteomic techniques may help to
characterize the molecular mechanisms driving HBV-associated carcinogenesis, and thus
potentially identify new strategies in diagnosis and therapy.
Nagano, J., S. Nagase, et al. (2004). "Psychosocial Stress, Personality, and the Severity of Chronic
Hepatitis C." Psychosomatics 45(2): 100-106.
This cross-sectional study examined the association between the severity of chronic
hepatitis C and the type 1 personality, which has been shown by Grossarth-Maticek to be
strongly related to the incidence of cancer and mortality. Sixty-nine patients with chronic
hepatitis C completed the Stress Inventory, a self-report questionnaire to measure
psychosocial stress and personality, and were classified into three groups according to
hepatitis
severity:
aminotransferase
group
level;
A,
group
chronic
B,
hepatitis
chronic
C
hepatitis
with
C
a
normal
with
an
serum
alanine
elevated
alanine
aminotransferase level; and group C, liver cirrhosis. Each of four scales related to the type
1 personality--low sense of control, object dependence of loss, unfulfilled need for
acceptance, and altruism--was significantly and positively associated with hepatitis severity.
The type 1 score, calculated as the average of these scales, was also strongly related to
hepatitis severity (p<0.0001), and adjustment for age, sex, education level, smoking,
drinking, and duration brought no attenuation into the association. Chronic psychosocial
stress relevant to the type 1 personality may also influence the course of chronic hepatitis
C.
Nakamura, H., H. Nagase, et al. (1999). "Natural killer (Nk) Cell activity and nk cell subsets in
workers with a tendency of burnout." Journal of Psychosomatic Research 46(6): 569-578.
The involvement of cellular immunity in the burnout syndrome remains to be elucidated.
We assessed three components of burnout of the Maslach Burnout Inventory: emotional
exhaustion; depersonalization (DP); and personal accomplishment, as well as natural killer
cell activity (NKCA) and NK cell subsets in 42 male workers. Workers with a higher DP
score showed a lower NKCA and a lower proportionality of CD57+CD16+ to total
lymphocytes. There were no differences in any of the health behaviors (e.g., smoking,
alcohol, or obesity) between workers showing higher burnout and those showing lower
burnout. A stepwise multiple regressions analysis demonstrated that NKCA was closely
correlated with DP, independent of other variables, including a stress index. These results
suggest that the relationship between reduced cellular immunity and DP is not due to
traditional work stress or health behavioral problems. Further studies on DP as a
psychosomatic disorder as well as an occupational health problem should be performed in
the future.
Olivera-Mart?ez, M. A. and J. F. Gallegos-Orozco (2007). "Recurrent Viral Liver Disease (Hepatitis B
and C) after Liver Transplantation." Archives of Medical Research 38(6): 691-701.
Hepatitis C represents more than 35% of liver transplant candidates worldwide. Meanwhile,
hepatitis B continues to be an important cause of end-stage liver disease and
hepatocellular carcinoma in Asia and Africa. Recurrent viral liver disease is a significant
event after liver transplantation and continues to be one of the main causes of graft
dysfunction and loss in the middle and long-term follow-up. Mechanisms of liver
reinfection and disease recurrence vary between these two viruses and pre-emptive as
well as the therapeutic approaches are different. Hepatitis B patients can be managed with
immune globulin immediately after liver transplant and various agents such as nucleotide
and nucleoside analogues can be associated. As a result, disease recurrence has been
delayed or prevented in these patients. Individuals transplanted for hepatitis C are known
to have universal reinfection and a high rate of disease recurrence has been reported in
the literature. Strategies to treat hepatitis C recurrence are limited to the use of pegylated
interferon and ribavirin when disease is demonstrated histologically and biochemically,
although other strategies have been described with limited or no success. We herein
review the mechanisms of disease recurrence and the current as well as the쟣uture
therapeutic approaches to prevent and to treat these diseases.
Ono, K., K. Yamanaga, et al. (1996). "Natural killing activities in chronic liver diseases and
hepatocellular carcinoma." Journal of Clinical Immunology 16(1): 41-45.
Previously we proposed a new analysis of natural killing activity, for comparison,
employing an individual effector/target cell ratio according to the peripheral number of
effector cells. Using this analysis, we studied natural killing activities in chronic liver
diseases and hepatocellular carcinoma (HCC). The activity in chronic persistent hepatitis
remained nearly at the level of the nonactivated state, but that was significantly elevated
in chronic active hepatitis. The activity in liver cirrhosis (LC) of Child's A or B grade was at
the level of a nonactivated or reduced-activity state, while LC patients with impaired
general conditions showed significantly elevated activities. In HCC, each of which was
accompanied by LC in our cases, the activity appeared to be associated with the
progression of HCC. Thus, natural killing activity showed a close relationship with the
condition of chronic liver diseases.
Segerstrom, S. and G. Miller (2004). "Psychological Stress and the Human Immune System: A MetaAnalytic Study of 30 Years of Inquiry." Psychological Bulletin 130(4): 601-630.
The present report meta-analyzes more than 300 empirical articles describing a relationship between
psychological stress and parameters of the immune system in human participants. Acute stressors
(lasting minutes) were associated with potentially adaptive upregulation of some parameters of natural
immunity and downregulation of some functions of specific immunity. Brief naturalistic stressors (such
as exams) tended to suppress cellular immunity while preserving humoral immunity. Chronic stressors
were associated with suppression of both cellular and humoral measures. Effects of event sequences
varied according to the kind of event (trauma vs. loss). Subjective reports of stress generally did not
associate with immune change. In some cases, physical vulnerability as a function of age or disease
also increased vulnerability to immune change during stressors.
Sephton, S. and D. Spiegel (2003). "Circadian disruption in cancer: a neuroendocrine-immune
pathway from stress to disease?" Brain, Behavior, and Immunity 17(5): 321-328.
Psychosocial factors may modulate the course of cancer, but few data have been gathered
on the biological mechanisms by which these effects may be mediated. We briefly review
evidence of psychosocial effects on cancer progression and discuss one potential pathway
that may underlie these effects: the disruption of neuroendocrine and immune circadian
rhythms. Circadian system alterations occur in tumor tissue, tumor-bearing animals, and
cancer patients with greater disruption seen in more advanced cases. Rhythm alterations
include diminished amplitude, phase shifts, period changes, and erratic peaks and troughs
in endocrine, metabolic, immunological, and rest- activity cycles. Psychosocial factors can
engender dysregulation of circadian function. Cancer-related circadian dysregulation may
also be driven by genetic factors, environmental and behavioral influences, and effects of
the tumor on host clock regulation. There are several mechanisms by which circadian
disruption might hasten tumor growth: via direct effects of altered hormone levels on
tumor cells, effects on tumor versus host metabolism, neuroimmune effects resulting in
cancer-relevant immunosuppression, or reduced efficacy and tolerability of cancer
treatments for which the timing of administration is based upon the assumption of normal
circadian rhythms. Emerging data in the human and animal literature suggest that
circadian regulation may be an important prerequisite for the maintenance of host
defenses against cancer. Thus, stress-related circadian disruption may have negative
implications for cancer prognosis. Psychosocial effects on cancer progression may be
measured, and possibly mediated, by disruption of circadian function.
Shirai, M., S. Watanabe, et al. (1990). "Depressed lymphokine-activated killer activity and analysis
of the precursor cells in peripheral blood of patients with hepatocellular carcinoma."
Hepatogastroenterology 37(5): 465-68.
The in vitro lymphokine-activated killer activity and natural killer activity of peripheral
blood mononuclear cells from 33 patients with hepatocellular carcinoma were investigated.
Lymphokine-activated killer and natural killer activities of patients were significantly
decreased compared with those of healthy volunteers. Peripheral blood mononuclear cells
showed significantly lower lymphokine-activated killer and natural killer activities in
patients with larger tumors (greater than or equal to 5 cm in diameter) than in patients
with smaller tumors (less than 5 cm in diameter). Of 20 patients with larger tumors, 8 and
6 generated very little or no lymphokine-activated killer and natural killer activities.
respectively. Lymphokine-activated killer precursors and natural killer cells were present
mainly in the Leu-11+ fraction and partially in the Leu-7+ fraction in patients and normal
volunteers. A flow cytometric study showed that the percentage of Leu-7+ 11+ and Leu7-11+ fractions in peripheral blood mononuclear cells was lower in patients than in
normal volunteers. The percentages of Leu-7-11+ and Leu-7+ 11+ fractions were
diminished in the peripheral blood mononuclear cells of the patients with little or no
lymphokine-activated killer activity. It is suggested that deficient lymphokine-activated
killer and natural killer activities partially results from a reduction in the number of their
precursor cells in patients with hepatocellular carcinoma.
Steel, J., M. Carney, et al. (2004). "The role of psychosocial factors in the progression of
hepatocellular carcinoma." Medical Hypotheses 62(1): 86-94.
The number of deaths per year from hepatocellular carcinoma (HCC) exceeds 250,000,
placing it sixth as the cause of death from cancer worldwide. The primary etiology of most
cases of HCC in the US is hepatitis B and/or C. Extensive research has demonstrated that
the relationship between hepatitis B infection and the progression to HCC is mediated by
the immune system. A substantial, but unrelated literature, describes the relationship
between psychosocial factors (e.g., stress, psychiatric morbidity), immune system reactivity,
and disease progression in patients with cancer. However, the role of these factors in the
progression of HBV-HCC has not been explored. An understanding of the relationship
among virology, immunology, and behavior in the development and recurrence of HCC
may provide alternative methods for secondary prevention of HCC (e.g., behavioral) until a
vaccine and/or pharmacological treatments are developed, feasible, and affordable.
Steel, J. L., D. A. Geller, et al. (2007). "Depression, Immunity, and Survival in Patients With
Hepatobiliary Carcinoma." J Clin Oncol 25(17): 2397-2405.
Purpose The aims of the present study were to assess the prevalence of depressive
symptoms at diagnosis, test the association between depressive symptoms and survival,
and preliminarily test a mediational model of depression, immunity, and survival in
patients with hepatobiliary carcinoma (HBC).
Patients and Methods One hundred one patients diagnosed with HBC were prospectively
studied. Depressive symptoms were measured at diagnosis using the Center for
Epidemiological Studies Depression Scale (CES-D). Sociodemographic and disease-specific
data were gathered from the patients' charts. In a subsample of patients, stress; alcohol,
tobacco, and drug use; sleep quality; physical activity; social support; natural killer (NK)
cell number and cytotoxicity; and plasma levels of interleukin (IL) -4, IL-5, tumor necrosis
factor alpha, and interferon gamma were measured. Survival was measured from date of
diagnosis to death.
Results At diagnosis, 37% of patients reported a CES-D score of [&ge;] 16 (clinical range). Using
Cox regression analysis, sociodemographic and disease-specific variables and CES-D score
significantly predicted survival (Breslow {chi}2 = 32.4, P = .006). Only vascular invasion (P
= .001) and CES-D score [&ge;] 16 (P = .03) were significant predictors. In a subsample of
23 patients, patients who reported a CES-D score of [&ge;] 16 were found to have
significantly lower NK cell numbers than patients who reported a CES-D score of less than
16 (F1,21 = 9.39, P = .003). A robust trend was found in which NK cell number was
associated with survival. A mediational model linking depressive symptoms and survival,
with NK cell number as a mediator, was preliminarily supported.
Conclusion Secondary to the high prevalence of depressive symptoms and impact on survival,
psychological and pharmacologic interventions should be designed and implemented in
patients diagnosed with HBC.
Sulkowski, M. S. (2008). "Viral hepatitis and HIV coinfection." Journal of Hepatology 48(2): 353-367.
Persons at high risk for human immunodeficiency virus (HIV) infection are also likely to be
at risk for other infectious pathogens, including hepatitis B virus (HBV) or hepatitis C virus
(HCV). These are bloodborne pathogens transmitted through similar routes; for example,
via injection drug use (IDU), sexual contact, or from mother to child during pregnancy or
birth. In some settings, the prevalence of coinfection with HBV and/or HCV is high. In the
context of effective antiretroviral therapy (ART), liver disease has emerged as a major
cause of morbidity and mortality in HIV-infected persons. Further, coinfection with viral
hepatitis may complicate the delivery of ART by increasing the risk of drug-related
hepatoxicity and impacting the selection of specific agents (e.g., those dually active
against HIV and HBV). Expert guidelines developed in the United States and Europe
recommend screening of all HIV-infected persons for infection with HCV and HBV and
appropriate management of those found to be chronically infected. Treatment strategies
for HBV infection include the use of nucleos(t)ide analogues with or without anti-HIV
activity and/or peginterferon alfa (PegIFN) whereas HCV treatment is limited to the
combination of PegIFN and ribavirin (RBV). Current approaches to management of HIVinfected persons coinfected with HBV or HCV are discussed in this review.
Swain, M. G. (2000). "Stress and the Gastrointestinal Tract: I. Stress and hepatic inflammation." Am
J Physiol Gastrointest Liver Physiol 279(6): G1135-1138.
Stress is an ever-present part of modern life. The "stress response" constitutes an
organism's mechanism for coping with a given stress and is mediated via the release of
glucocorticoids and catecholamines. Patients often complain of stress-related worsening of
their liver disease; however, the interrelationship between stress and hepatic inflammation
is incompletely understood and has received little scientific attention. Considering the
broad impact glucocorticoids and catecholamines have on immune cell function, it is very
likely that stress has a significant impact on the hepatic inflammatory response. This
themes article discusses studies of the stress response and its peripheral effectors
(glucocorticoids and catecholamines) in liver disease and their impact on hepatic
inflammation and outlines potential areas for future scientific investigation.
Yang, Y., D. Koh, et al. (2002). "Self perceived work related stress and the relation with salivary IgA
and lysozyme among emergency department nurses." Occup Environ Med 59(12): 836-841.
Aims: To assess and compare the self perceived work related stress among emergency
department (ED) and general ward (GW) nurses, and to investigate its relation with
salivary IgA and lysozyme. Methods: One hundred and thirty two of 208 (63.5%)
registered female ED and GW nurses participated in the study. A modified mental health
professional stress scale (PSS) was used to measure self perceived stress. ELISA methods
were used to determine the salivary IgA and lysozyme levels. Results: On PSS, ED nurses
had higher scores (mean 1.51) than GW nurses (1.30). The scores of PSS subscales such as
organisational structure and processes (OS), lack of resources (RES), and conflict with other
professionals (COF) were higher in ED than in GW nurses. ED nurses had lower secretion
rates of IgA (geometric mean (GM) 49.1 {micro}g/min) and lysozyme (GM 20.0
{micro}g/min) than GW nurses (68.2 {micro}g/min, 30.5 {micro}g/min). Significant
correlations were observed between PSS and log IgA and lysozyme secretion rates. OS,
RES, and COF were correlated with log IgA and lysozyme levels. Conclusion: ED nurses,
who reported a higher level of professional stress, showed significantly lower secretion
rates of salivary IgA and lysozyme compared to GW nurses. Salivary IgA and lysozyme
were inversely correlated with self perceived work related stress. As these salivary
biomarkers are reflective of the mucosal immunity, results support the inverse relation
between stress and mucosal immunity.
Yoichi Chida, N. S., Chiharu Kubo, (2006). "Does stress exacerbate liver diseases?" Journal of
Gastroenterology and Hepatology 20(1): 202-208.
Although anecdotal comments on detrimental effects of psychosocial stress on liver
diseases can be found even in the early literature, only recently has scientific evidence
been reported. The present article reviewed such evidence to demonstrate how stress
exacerbates liver diseases. A search of the literature from the last two decades was
performed using MEDLINE by pairing 'psychological stress' with 'liver' or 'hepatitis.'
Additional research was conducted by screening the bibliographies of articles retrieved in
the MEDLINE search. The search results showed that the principal effectors of the
activated hypothalamic2013pituitary2013adrenal (HPA) axis, glucocorticoids, can exert a
facilitative effect on the hepatic inflammatory response and even increase the risk of
developing hepatocellular carcinoma. For certain liver diseases, defective HPA axis
activation, which probably contributed to the exacerbation of the liver disease, has been
reported. The efferent sympathetic/adrenomedullary system mainly contributes to the
stress-induced exacerbation of liver diseases via its neurotransmitters, the catecholamines.
In contrast, the efferent parasympathetic nervous system elicits an inhibitory effect on the
development of hepatic inflammation. In conclusion, the pathophysiological interaction
between stress and the liver appears to be regulated by the complex, dynamic networks
of both the endocrine and autonomic nervous systems, which implies a further need for
basic research into the involved mechanisms and for clinical evidence to apply
psychosocial support to patients with chronic liver diseases.
Yoshito
Wada,
O.
N.,
Rumiko
Kutami,
Osamu
Yamamoto,
Masamichi
Kojiro,
(1998).
"Clinicopathological study on hepatocellular carcinoma with lymphocytic infiltration." Hepatology
27(2): 407-414.
We examined the clinicopathologic features of 11 surgically resected hepatocellular
carcinomas (HCCs) less than 3 cm in diameter with marked inflammatory cell infiltration
(LHCCs). In comparison with the other 152 HCCs without such an infiltration (controls),
there were no significant differences in male/female ratio, age, serum alpha-fetoprotein
levels, and laboratory and imaging findings. All the 11 LHCC cases were hepatitis B surface
antigen (HBsAg) negative and hepatitis C virus antibody positive. Among the 152 controls,
116 cases were also HBsAg negative and HCVAb positive and were referred to as HCVonly controls. The clinical features were not significantly different between the LHCC and
the HCV-only controls. The LHCC group tended to have higher numbers of lymphocytes
and monocytes in pre- and post-operative peripheral blood, but there were no significant
group differences. Recurrence rate was 9.1% in the LHCC group, 47.7% in the controls and
47.5% in the HCV-only controls (P?lt;?01). Five-year survival rate was 100% in the LHCC
group, 65.1% in the controls and 68.1% in the HCV-only controls (P &lt; .01). Histologically,
remarkable inflammatory cell infiltration, mostly lymphocytic, was observed in the
cancerous tissue of the LHCC group. Varying degrees of piecemeal necrosis of cancer
nests produced by infiltrating lymphocytes were observed in all the 11 cases. Lymph
follicle formation was also found in 10 of 11 cases (90.9%). Liver cirrhosis was associated
in 6 LHCC cases (54.5%), in 117 control cases (77.0%), and in 91 HCV-only controls (78.4%).
Tumor invasion into the portal vein in the vicinity of the tumor was found in 1 LHCC case
(9.1%),
in
54
controls
(35.5%),
and
in
34
HCV-only
controls
(29.3%).
Immunohistochemically, most of the infiltrating lymphocytes, other than those in the
lymph follicle, were identified as T lymphocyte, and CD8+ T lymphocyte was more
predominant than CD4+ T lymphocyte. Better prognosis of the LHCC group could
attribute to the anti-tumor effect induced by cellular immunity of CD8+ and CD4+ T
lymphocytes, and partly by humoral immunity of B cells which formed lymph follicles.