Behavioural Safety at the Carrington Site - EPSC
advertisement

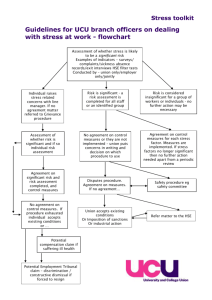
Behavioural Safety at the Carrington Site From a plateau to an iceberg, trying to avoid a few crevasses Peter Webb, HSEQ Manager, Basell Polyolefins Carrington Site Outline • What is behavioural safety • How we implemented a behavioural programme • Some key learning points Safety …. A potted history INCIDENTS Technological Improvements Management Systems We are here! Human Factors TIME Why Behavioural Safety? It’s just another tool in the human factors tool box What does a Behavioural Approach Comprise? All behavioural safety programmes have a system of OBSERVATION and FEEDBACK The observations can be done by anybody on anybody It’s all about people talking to each other about safety The Observation Process • • • • • Stop and observe Put the person being observed at ease Explain what you are doing and why Discuss the job being carried out Observe the work activity for a few minutes • Praise safe behaviours • Discuss any “at risk” behaviours – What – Why – Discuss what the worst consequences could have been • Ask what corrective action is required • Get commitment to act • Finally record the observation - but no names! Why do we behave the way we do? Values Attitudes Behaviours Our behaviour is driven by our attitudes and values What Are Behaviours? Value: “I think safety’s important” Attitude: “I’m going to use the right tools for the job” Behaviour: “*$%^&£!!! I’ve brought the wrong tool out with me. But I’m not going to use it, because that would be unsafe. I’m going to walk back to the workshop and get the right one.” Our behaviour is driven by our attitudes and values How can you modify “At Risk” Behaviours? • At risk behaviours are driven by attitudes and values • But you can’t modify people’s values and attitudes directly ……. They are too deep within us. • So you use a system of observations which address the “at risk” behaviours. • If you work on modifying the “at risk” behaviours, eventually the “at risk” attitudes and values change too. We used to feel it was safe to ride in a car without a seat belt. Modify the behaviour and the value will follow Value: “I feel safe in my car without a seat belt” Value: “I feel uncomfortable and exposed in my car without a seat belt” Attitude: “Wearing seat belts is unnecessary” Attitude: “Wearing seat belts is a responsible thing to do” Behaviour: ”I don’t wear my seat belt in my car”. Behaviour: ”I wear my seat belt in my car”. Behaviour modification: You must wear your seat belt, it’s the law! Carrington Site How did we come to BBS 1980’s • “Systems” initiatives in HSE. • Total recordable injury rate reduced from ~18 to ~10 injuries per million hours worked. Mid 1990’s • Safety performance had plateaued • 1996 became aware of behavioural programmes • Decision was taken to pilot it on one plant (Styrocell) • Engaged BS provider to assist in implementation • Started with observations in January 1997. BBS Programme Carrington implementation followed “classical” approach ... Implementation Observation and Feedback Process Assess cultural maturity or readiness Modify environment, equipment or systems Gain management & workforce support & ownership Behavioural safety training Specify critical behaviours Monitor performance Review & goal setting Review critical behaviours Provide feedback Establish baseline Ref HSE CRR 430/2002 Conduct observations BBS Programme Some specifics of our implementation: List of critical behaviours • Developed by reviewing near miss reports. Follow up • We don’t wait for trends to develop. We follow up on the individual at risks - prioritised short list. Facilities vs behaviour • We don’t limit the at risks to behaviour related • We allow at risks which are related to the facilities as well • The most important thing is that people are doing the observations face to face BBS Programme • • • • • • • Styrocell programme was a great success. Great enthusiasm amongst (most/enough) technicians. Programme was rolled out to rest of site in 1997/8. Steering groups set up in each dept Separate list of critical behaviours in each dept Cross site facilitators group Approx 10 - 15% of workforce were observers (now it’s 100% plus contractors) • A lot of creativity and energy put into it WHAT IS ZAP ? ZERO ACCIDENT POTENTIAL Total Recordable Injury Rate (per 106 hrs) 20 18 > 18 Before 1990 16 Total Recordable Rate 14 BBS introduced 12 10 8 6 4 2 0 1990 1991 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 Resuscitation In 1999 it was clear there were problems • Fall off in observations • Technicians were saying: “The same observations are being done on the same tasks” “People can’t be bothered” “It’s the same people being observed all the time” “Observation process is too formal” “Carrington is already safe, so why bother?” “What’s coming out of it?” “Data input to database is difficult” Resuscitation Managers were saying the same as the technicians, and – “There’s not enough visible output.” – “We need more performance metrics – contact rate, observation quality” – “Vision is that everybody needs to be an observer.” – “Whole process needs to become part of the existing HSE system.” – “We need to move on from the original concept and make BBS our own.” Resuscitation • • • • It was not delivering to its full potential But we thought the approach was fundamentally sound So we launched a “resuscitation” Decision to work without the original BS provider ……………….. A representative team identified 4 issues Resuscitiation Issue 1: Organisation Issue • Need to make line supervisors part of the process. • Need to integrate BBS into the site HSE systems. Resuscitiation Issue 1: Organisation The BBS organisation we started with Traditional HSE Structure BBS Organisation Site HSE Council Facilitators' Committee Department HSE Committees (x4) Contractors' HSE Committee Made up of Managers and technicians Department Steering Committees (x4) Only Technicians Resuscitiation Issue 1: Organisation And the organisation we changed to …. Site HSE Council It’s fully Managers supervisors and technicians Department HSE Committees (x4+ contractors) integrated! BBS Subgroup 1 per department Cell Cell Cell Cell Site divided into cells of 6 - 8 people Everybody is an observer, including contractors Subgroup made up of Improvement Leader and cell focal points Key person Resuscitiation Issue 2: Perceptions Issue • Overcome the complacency – “It’s already safe at Carrington” • People don’t see the value. Response • At the end of the observation, during the feedback, if there are “at risks” to discuss, jointly agree what was the worst consequence which could have happened. • Jointly agree a ranking (L, M, H) for the potential outcome on a defined scale ranging from slight injury (first aid), through to fatality. Gets people to visualise what could go wrong Resuscitation Issue 3: Reporting Issue • Need to pull out learning points. • Need to give feedback to observers. • Integrate into the business – link with near miss reporting. Response Every month ….. • Overall KPI’s reviewed by site HSE Council (chaired by Site Manager) • Department HSE committees review performance against KPI’s • Cell members receive a report showing status of the at risks Resuscitation Issue 4: Observations Issue • People should want to carry out observations. • Need to simplify the observation process. • Need to make recording simpler. Response • Original programme design comprised a different list of critical behaviours in each department • Created a generic list to be used by everybody • Allows any observer to carry out observations anywhere on site • The generic list is quite short, observation time can be as short as 5 minutes • Some people even do it without the checklist! Other things we’ve learned! Key Performance Indicators • Currently have 3 KPI’s: – Number of observations, 1 per person per month (all employees and contractors) – Quality, Percent of observations for which the “what” and the “why” are filled out > 80% – Close-out of “High” at risks, 100% in < 3 months Number of observations forms part of bonus scheme 1800 observations in 2001, 2400 in 2002 …. We don’t have a KPI on % safe! If you get 100% safe, does that mean you’ve finally made it? A safe work place at last? Or does it mean people aren’t looking hard enough? With our generic list of critical behaviours, it’s hard to imagine we could reach 100% safe. Other things we’ve learned! Management Commitment Everybody knows its important, but what can they do to show it – By taking an active interest – Management team must be active observers – Use managers to coach in the observer training Other things we’ve learned! Hold an away day in a nice hotel! • Organised by the BBS department focal points • Attended by site management team, cell focal points, term contractors • Generated several action items for enhancing the programme • Demonstrates management commitment, generates good ideas, gets buy in. Other things we’ve learned! Organisational readiness • Implementing BBS is a big commitment - you don’t want it to fail! • Organisational readiness (climate/culture) is a key factor which influences likelihood of success. • HSE CRR 430/2002 - of 8 providers interviewed, 3 said they would proceed regardless of readiness. • To avoid a costly failure, discuss up front, or conduct independent culture survey. Other things we’ve learned! Can be extended to other areas e.g. We have now included environmentally critical behaviours in the programme – – – – – Is environmental protection equipment available Is pollution prevention achieved Releases controlled Waste disposed of appropriately Energy used efficiently Other things we’ve learned! Major Accident Hazards • Behavioural safety has been driven by injury frequency • Our inventory of critical behaviours was developed by reviewing near miss/incident reports -> focus on workplace safety • It doesn’t follow that a reduction in the risks due to major accident hazards will occur • It depends on the list of critical behaviours • Here’s an example of how BBS added to the major accident hazard risk! Major Accident Hazards Handle Bolts • Manlid was not only used for process reasons, but was also a relief device • Handle had been fitted to solve a manual handling “at risk” after a BBS observation. • Plant change procedure was not followed • Bolts interfered with sealing surface • Pentane vapour leakage • Completely lost sight of the MAH risks Major Accident Hazards • Incident investigations indicated “Procedures” were often a root cause • Procedures often relate to controlling major accident hazards (plant change, safe operation, permit to work etc.) • We’ve added “procedures” to our inventory of critical behaviours” Major Accident Hazards Was there a procedure for the activity? NO At risk Yes Was the procedure appropriate? NO At risk Procedures: •permit to work •safe operation •plant change •control of contractors •etc Yes Was the procedure followed? Yes Safe NO At risk You can substitute the word Training for Procedure References •Health & Safety Executive (2002). Strategies to promote safe behaviour as part of a health and safety management system, Contract Research Report 430/2002, www.hse.gov.uk •PRISM (2002). Behavioural Safety Application Guide, www.prism-network.org Summary • • • • • The organisation must be ready for it Management commitment is essential It needs to be easy to carry out the observations Needs to be integrated into the HSE MS Need at least a few enthusiastic people to keep things going in their departments • People need to see some output • Make sure the programme addresses all the issues which are important for your organisation - Don’t forget about major accident hazards • We think BBS works, but it’s not easy The End!