ICD-10 Education Session
Preparing for the Change
January 29th & 30th, 2015
Agenda
Topic
Timeframe
Presenter/s
Welcome
15 minutes
Anupam Goel, MD
Documenting for ICD-10
90 minutes
Thomas Kravis, MD
Clinical Informatics/Clinical
Documentation Improvement
(CD)/Coding- How can we help
you?
30 minutes
Cheryl Hager
Stephen Crouch, MD & Kelly Tarpey
Lou Ann Schraffenberger & Dawn
Monegato
Break
15 minutes
Using CareConnection to
Improve Documentation
30 minutes
Anupam Goel, MD
Case Examples Discussion
45 minutes
Thomas Kravis, MD
2
WELCOME
Housekeeping Items
• Sign In Sheets
• Restrooms
• Cafeteria
• Eureka Conference Room
4
ICD-10 Resources
You can access the ICD-10 Website from the
Advocate Home Page:
5
What is available?
•
•
•
•
•
6
FAQ’s
Documentation Tip Sheets
3M Specialty Focused Training Videos
EMR Specific Videos
Leadership Materials
3M Health Information Systems, Inc.
Advocate CDI
Thomas C Kravis MD
January 29 and 30 2015
Innovating
Innovating
the
the
Language Language
of Health of Health
3M provides these slides to better understand 3M's software and/or services.
These slides contain 3M confidential information and are for customer’s internal review only.
Clinical Documentation Improvement Goals and
Objectives
Clear concise accurate documentation
Across the continuum of care: inpatient and outpatient
Capture the severity of illness (SOI) and the Risk of Mortality (ROM)
Support hospital and physician reimbursement
Improve quality report cards and clinical outcomes
Reduce denials and queries
Prepare for ICD-10
8
Value of Accurate and Complete Documentation
MD and
Hospital
Quality
Reports
Core
Measures
ICD-9-CM
ICD-10
POA
HACs
Preventable
Readmission
Complications
PSIs
Compliance
Fraud Abuse
RAC
Value
Base
Purchasing
Care
Coordination
Team
Medical
Necessity
2 MIDNIGHT
RULE
E&M Pro fees
Denial related
claims
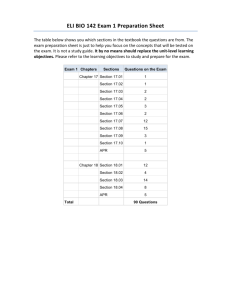
Documentation Across the Continuum of Care
Pre Hospital
Ambulatory
Physician
Practices
Population at Risk
Ambulatory
Surgery Ctr
Urgent Care Ctr
Fed Qualified HC
Employer Clinic
OP Facility/
Comprehensive
OP Rehab Fac.
Hospital
Outpatient
Inpatient
Critical Access
Hospital
Outpatient
Critical Access
Hospital
Inpatient
Free-standing
Diagnosis Center
Indian Health Services
Community Mental
Health Clinic
Home Health
Agency
Day Surgeries
Emergency
Clinic visits
Observation
Hospital-Based
ancillary services
Rural Health Clinic
Retail Clinic
Hospital –
Inpatient
Psych
Inpatient
Rehab
Hospice
End Stage Renal Disease
Physician Evaluation and Management
Skilled Nursing Facility
Home
Hospice
Hospital Outpatient
•
•
•
•
•
Post Acute Care
Home
Healthcare
Physician
Office
Clinic
General Guidelines for Documentation
•
Document all diagnoses and procedures
•
Licensed hands-on treating practitioner in the body of the EMR and discharge summary
•
All medications, treatments and diagnostic studies and the corresponding medical
diagnoses for each and the clinical significance
•
Conditions cannot be coded from lab, x-ray, other diagnostic test results or symbols (↑, ↓)
without practitioner documentation.
•
‘Cut and pasted’ documentation must accurately reflect the clinical condition of the patient
at the time of the documentation
•
To capture SOI and ROM and assign an appropriate code a “condition” in the inpatient
setting must meet at least one of the following criteria:
–
–
–
–
–
11
Clinical evaluation
Therapeutic treatment
Diagnostic procedures
Extended length of hospital stay
Increased nursing care and/or monitoring
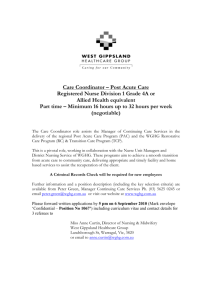
Documentation & Coding Issues at Advocate
Physician
Document in
CLINICAL terms
Two separate
languages
Documentation for
coding, profiling &
compliance requires
specificity in
DIAGNOSIS terms
This gap will be increased with ICD-10
Documentation
Improvement can help bridge the gap
Clinical
Diagnostic
Unable to Code
Able to Code
Multi-system organ failure
Liver failure, renal failure, resp failure
Severe respiratory distress
Respiratory failure : acute, acute on chronic
Hemodynamically unstable
Hypotension, shock-cardiogenic/septic
Will rehydrate
Dehydration, hypovolemia
Rhythm stable today
Ventricular tachycardia
“Urosepsis”
Simple UTI
↓ K = 2.0, will give KCL
Hypokalemia
Chest X infiltrate
Pneumonia Left Lower Lobe
↓ Platelets ↓ Wbc ↓Hct
Pancytopenia secondary to Chemotherapy
↓ HgB 5.2, Transfuse
Acute/Chronic Blood Loss Anemia
Altered Mental Status
Coma, Encephalopathy
Emaciated, Total Protein/Albumin Low
Protein Calorie Malnutrition
Emergency Medicine
Clinical Terms
Diagnostic Statement
(Documentation needs clarification)
(Accurate code may be assigned)
Cardiac enzymes elevated, elevated troponin, EKG
positive
Acute myocardial infarction (specify type such as STEMI or
NSTEMI; specific artery involved such as LAD, left circumflex;
exact date of any recent AMI)
Acute coronary syndrome (ACS)
Document intended diagnosis such as
intermediate/insufficiency syndrome, unstable angina,
coronary slow flow syndrome, myocardial infarction
Chest pain will treat with IV nitro and evaluate by
cath
Specify cardiac cause such as CAD (known or suspected),
stable angina, unstable angina, AMI, aortic stenosis,
hypertension, CHF
Chest pain, noncardiac, treated with NSAID and H2blockers
Specify diagnosis being treated even if considered probable or
suspected such as chest wall pain, GERD, costochondritis
1. Rales & rhonchi lung bases, lungs sound wet, RR
= 30, Ejection fraction 24%, JVD
2. History of CHF, will continue furosemide, ACE
inhibitors
Heart failure (specify type such as systolic, diastolic, combined
systolic and diastolic; specify acuity such as acute, chronic,
acute on chronic)
↓BP, hemodynamically unstable, IV fluid bolus
started, dopamine ordered
Shock, hypotension (specify type and etiology such as chronic,
drug-induced, iatrogenic, idiopathic, intra-dialytic, orthostatic,
intraoperative or postoperative)
Unresponsive to painful stimuli, obtunded, GCS=8
Coma/comatose (document specific cause, if known or
suspected)
A code may not be assigned based on abnormal laboratory results or diagnostic report findings alone. The physician
must document the corresponding diagnosis in the body of the medical record.
General and Internal Medicine
Clinical Terms
Diagnostic Statement
(Documentation needs clarification)
(Accurate code may be assigned)
Continue home medications such as furosemide,
HCTZ, ACE inhibitor
Document specific diagnosis such as chronic
systolic/diastolic heart failure, CAD, atrial fibrillation,
angina, HTN
History of CHF, will continue home meds
Specify acuity (chronic, acute, acute on chronic); specify
type (systolic, diastolic, combined systolic and diastolic)
Cardiac enzymes elevated, elevated troponin, EKG
positive
Acute myocardial infarction (specify type such as STEMI
or NSTEMI; document specific artery involved such as
LAD, left circumflex; exact date of any recent AMI)
Acute coronary syndrome (ACS)
Document intended diagnosis such as
intermediate/insufficiency syndrome, unstable angina,
coronary slow flow syndrome, myocardial infarction
Cardiac history
Document specific diagnoses such as CAD, angina, old
MI (document date when MI occurred)
Atrial fibrillation
Specify type (e.g., paroxysmal, permanent, persistent,
chronic)
Atrial flutter
Specify type such as typical (type I) or atypical (type II)
BP 70/40, ordered norepinephrine or dopamine
for support
Shock (specify type such as cardiogenic septic,
hypovolemic)
A code may not be assigned based on abnormal laboratory results or diagnostic report findings alone. The physician
must document the corresponding diagnosis in the body of the medical record.
E&M DRG Assurance
Physician
The Key Elements :
Chief Complaint
History
Examination
Medical Decision Making
Chief Complaint:
Symptom, problem, condition,
diagnosis ( reason for the
encounter)
Code diagnoses to the highest
level of specificity known (i.e.
symptoms)
Inpatient
Definitive diagnosis unknown,
document conditions evaluated
treated up:
“Probable”
“Possible”
“Suspected”
Coded as if condition exists until
condition has been excluded
Facility Principal Diagnosis:
Condition established after
careful study to be chiefly
responsible for occasioning
admission to the hospital
Two Midnight Rule
Signs Symptoms Expectation of 2 Midnight
Risk of Adverse Event
Physician and Advanced Practitioners Role
Focus remains on patient care
Respond to query and document in the EMR
Do not need to learn coding
Minimal impact on day-to-day routine
Clinical Documentation Specialists – a resource
to the physician
3M 360 : Natural Language Processing (NLP)
Impact of Responding to Query
Query: “The magnesium level is 1.6 and the patient is
receiving magnesium sulfate” “Please provide a corresponding
diagnosis ”
Physician documents: “hypomagnesimia”
Cranial Procedure
Impact w/o Response to Query
• RW = 2.9797
• GLOS = 8.98
• SOI = 2 Moderate
• ROM = 2 Moderate
Impact w/ Response to Query
• RW = 2.9797
• GLOS = 8.98
• SOI = 3 Major
• ROM = 2 Moderate
Provider Documentation
Provider Documentation
Principal & Secondary Diagnoses
Principal & Secondary Procedures
ICD-9-CM Codes
ICD-10-CM Codes
ICD-10-PS Codes
DRG Assignment
Severity & Risk of Mortality
Classification
Profiling/Reimbursement
(Providers/Hospitals)
19
© 3M 2008. All rights reserved.
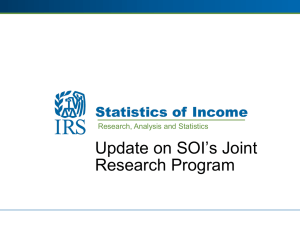
APR-DRG
Y
3M™
Subdivide into subclasses
Severity of Illness Subclasses
Risk of Mortality Subclasses
1. Minor
1. Minor
2. Moderate
2. Moderate
3. Major
3. Major
4. Extreme
4. Extreme
Mortality at < 4
Quality
Coding
Documentation
Principal Diagnosis "XYZ"
Impact of Secondary Diagnosis
21
1
2
3
4
Severity of Illness
Minor
Moderate
Major
Extreme
1
2
3
4
Risk of Mortality
Minor
Moderate
Major
Extreme
Secondary Diagnosis-Diabetes Mellitus
Uncomplicated Diabetes
Diabetes w Neuropathy
Diabetes w Ketoacidosis
Diabetes w Hyperosmolar Coma
Secondary Diagnosis-Cardiac Dysrhythmias
Premature Beats
Sinoatrial Node Dysfunction
Paroxysmal Ventricular Tachycardia
Ventricular Fibrillation
Underlying Principle of 3M™ APR DRGs
High SOI and ROM are characterized by:
(a) multiple
(b) serious diseases and
(c) the interaction among those diseases.
22
Severity Summary Analysis by Service Lines
Advocate Good Shepherd Hospital
Medical Specialty
Behavioral
Cardiology
CT Surgery
Medicine
Neurology
Neurosurgery
Ophthalmology
Orthopedics
Pulmonary
Renal
Surgery
Transplant
Vascular
Women's Health
Total
23
Hospital
Volume
14
568
105
1,265
224
31
9
626
539
273
263
0
53
18
3,988
% of Total
Cases
0.4%
14.2%
2.6%
31.7%
5.6%
0.8%
0.2%
15.7%
13.5%
6.8%
6.6%
0.0%
1.3%
0.5%
100%
Average
State
Severity
Weight
0.3868
1.1554
4.5666
0.9560
1.0281
2.5799
0.7526
1.5914
1.2115
1.1599
2.3734
10.2349
2.5322
0.9498
1.3093
Hospital
Average
Severity
Weight
% Difference
0.6156
59.2%
1.1032
-4.5%
4.1170
-9.8%
1.0474
9.6%
1.0372
0.9%
2.1726
-15.8%
0.6814
-9.5%
1.7530
10.2%
1.3092
8.1%
1.0339
-10.9%
2.3339
-1.7%
0.0000
-100.0%
2.3451
-7.4%
0.8326
-12.3%
1.3883
6.0%
Risk-Adjusted Mortality Analysis
Advocate Good Shepherd Hospital
Medical Specialty
Behavioral
Cardiology
CT Surgery
Medicine
Neurology
Neurosurgery
Ophthalmology
Orthopedics
Pulmonary
Renal
Surgery
Transplant
Vascular
Women's Health
Total
Medicare
Volume
14
568
105
1,265
224
31
9
626
539
273
263
0
53
18
3,988
Actual
Deaths
0
15
3
51
7
1
0
3
28
1
9
0
0
0
118
Actual
Death
Rate
0.00%
2.64%
2.86%
4.03%
3.13%
3.23%
0.00%
0.48%
5.19%
0.37%
3.42%
0.00%
0.00%
0.00%
2.96%
Expected
Deaths
0.0
17.3
2.4
50.4
10.5
0.1
0.0
7.2
31.6
3.5
9.8
0.0
1.2
0.1
134.1
Expected Variance,
Variance,
Death
In
As A %
Rate
Deaths
Of Expected
0.00%
0.0
0.0%
3.05%
-2.3
-13.3%
2.29%
0.6
25.0%
3.98%
0.6
1.2%
4.69%
-3.5
-33.3%
0.32%
0.9
900.0%
0.00%
0.0
0.0%
1.15%
-4.2
-58.3%
5.86%
-3.6
-11.4%
1.28%
-2.5
-71.4%
3.73%
-0.8
-8.2%
0.00%
0.0
0.0%
2.26%
-1.2
-100.0%
0.56%
-0.1
-100.0%
3.36%
-16.1
-12.0%
Data based on all cases using selection criteria. No inference is made or conclusion can be drawn about the significance of
actual to expected mortality variance without further study.
24
3M APR DRG Classification System
Risk-Adjusted Mortality Example
APR-DRG 194, HEART FAILURE
Illinois Average
APR DRG
Subclass
1
2
3
4
Total
Advocate Good Shepherd Hosp.
Actual
Cases Deaths Mortality Rate
1,549
5
0.3%
9,812
46
0.5%
10,792
239
2.2%
2,856
390
13.7%
25,009
680
2.7%
Actual
Cases
9
89
90
34
222
Actual
Expected Actual Mortality
Deaths Deaths Rate
0.0
0
0.0%
0.4
2
2.2%
2.0
1
1.1%
4.6
4
11.8%
7.0
7
3.2%
Data Source: 3M APR DRG Classification System utilizing MEDPAR 2013
Data based on all cases using selection criteria. No inference is made or conclusion can be drawn about the significance of
actual to expected mortality variance without further study.
25
Heart Failure
Common
•
Acuity
Type
Etiology
•
Impacts all specialties
Core Measure
Driver of SOI ROM
Quality (PPR)
Acute, chronic, acute on chronic/exacerbation
Systolic and/or diastolic heart failure
If known or suspected:
– Ischemia
– Anemia
– Kidney failure
– Hypertension
– Myocarditis
– Structural heart disease
– Supraventricular tachycardia
– Cardiomyopathy : Alcoholic congenital, congestive, constrictive, dilated, endomyocardial,
idiopathic hypertrophic sub aortic stenosis ,nonobstructive hypertrophic, obstructive
hypertrophic, restrictive
Collaboration and clinically effective: Core measure ;Potential Preventable Readmission
(PPR);continuum
Acute Kidney Failure Documentation
Impact of Appropriate Documentation on SOI and ROM and Physician Scorecard
– Acute renal “insufficiency”
– Acute kidney injury (AKI)
– Acute kidney failure
SOI 1; ROM 1
SOI 3; ROM 3
SOI 3; ROM 3
Versus
– Acute kidney failure “ due to”
• Acute tubular necrosis
• Cortical necrosis
• Medullary (papillary) necrosis
SOI 4; ROM 4
SOI 4; ROM 3
SOI 4; ROM 3
Chronic Kidney Disease
• Specify the stage of chronic kidney disease:
– Stages 1-5
– ESRD
• Do not document CKD stage as a range.
– Alternatively note if there is a progression of the stage of
CKD during the stay
• Document the etiology of the CKD, when known,
for example:
– Diabetic CKD
– Hypertensive CKD
• Document dependence on chronic dialysis, if
appropriate
Heart Failure
Training objective:
Sample Physician: SOI less than Peers
Respond to query
Target for Training/guidance
Document the drivers of SOI
Treat underlying cause: clinical effectiveness
Top 10 secondary diagnoses from National Norms driving SOI subclass 3 and 4
194 - Heart Failure
SOI
Subclass
1
2
3
4
Overall
Cases
Actual Days
1
10
3
0
14
1
40
19
0
60
ALOS
1.0
4.0
6.3
0.0
4.29
Peer Comparison
Sample Physician
Peer Group 1 - Cardiology
Peer Group 2 - Physician Practice Group
Peer Group 3 -National
Distribution
7%
71%
21%
0%
100%
Actual
Weight
0.4868
Total
Weight
0.4868
0.6127
0.9591
2.0096
6.1270
2.8773
0.0000
9.4911
Severity
Index
0.6779
Variance
0.7311
0.7982
0.8695
--7.3%
-15.1%
-22.0%
Lower SOI
Subclass 3
Subclass 4
Dx Code
Description
Dx Code
Description
5849
486
42833
42823
4271
5119
42831
42821
2639
51883
Acute Kidney Failure Nos
Pneumonia, Organism Nos
Ac On Chr Diast Hrt Fail
Ac On Chr Syst Hrt Fail
Parox Ventric Tachycard
Pleural Effusion Nos
Ac Diastolic Hrt Failure
Ac Systolic Hrt Failure
Protein-cal Malnutr Nos
Chronic Respiratory Fail
51881
41071
5070
51884
5845
4275
78551
262
99592
570
Acute Respiratry Failure
Subendo Infarct, Initial
Food/vomit Pneumonitis
Acute & Chronc Resp Fail
Ac Kidny Fail, Tubr Necr
Cardiac Arrest
Cardiogenic Shock
Oth Severe Malnutrition
Severe Sepsis
Acute Necrosis Of Liver
Physician Performance following physician training
by service line
Period 1 - 09/01/2011 - 08/31/2012
Percent of
Service Line
Med. /
Surg.
Cases
Total Case Average Case
Rank
CMI
Total Cases
Weight
Weight
within Contribution
within
within
within
Service
within
Line
Service Line
Service Line Service Line Service Line
Period 2 - 09/01/2012 - 08/31/2013
Percent of
Cases
Total Case Average Case Rank
CMI
% Change of
Total Cases
Weight
Weight
within Contribution Average Case Contribution
within
within
within
Service
within
weights
Line
Service Line
(high to Low)
Service Line Service Line Service Line
Difference
Cardiology
M
19
8.92%
17.4141
0.9165
39
0.0818
37
11.67%
37.8740
1.0236
3
0.1195
-10.5%
-0.0377
Cardiology
S
19
8.92%
17.4141
0.9165
39
0.0818
10
10.00%
28.2568
2.8257
3
0.2826
-67.6%
-0.2008
Medicine
M
8
1.05%
5.9252
0.7407
96
0.0078
14
1.15%
9.9959
0.7140
22
0.0082
3.7%
-0.0004
Orthopedics
M
1
1.56%
0.8467
0.8467
55
0.0132
1
0.91%
0.8467
0.8467
58
0.0077
0.0%
0.0055
Pulmonary
M
0
0.00%
0
0.0000
0
0.0000
3
0.81%
2.9510
0.9837
26
0.0080
-100.0%
-0.0080
Renal
M
0
0.00%
0
0.0000
0
0.0000
3
2.50%
4.0457
1.3486
22
0.0337
-100.0%
-0.0337
Surgery
S
0
0.00%
0
0.0000
0
0.0000
1
0.31%
2.8504
2.8504
57
0.0088
-100.0%
-0.0088
Vascular
S
1
1.43%
3.1477
3.1477
23
0.0450
1
0.95%
5.0962
5.0962
29
0.0485
-38.2%
-0.0036
Average length of stay by APR subclass:
efficiency opportunities
Severity Adjusted LOS
20.0
17.7
18.0
16.0
14.0
12.0
11.5
12.0
10.0
8.8
7.1
8.0
5.3 5.0
6.0
4.0
2.2 2.3
3.0
2.1
2.9 3.1
4.0
5.6
5.2
3.5 3.7
3.1
2.0
0.0
SOI 1 - Minor
Physician
31
2 - Moderate
Cardiology
3 - Major
4 - Extreme
Physician Practice Group
National Norm
Overall
4.0
Severity adjusted LOS
Severity
4.96
Minor
7.44
Dr B
3.33
7.45
Moderate
10.41
4.22
Dr A
11.24
Major
15.86
6.10
24.34
Extreme
Benchmark
18.26
10.53
0
5
10
15
20
25
Identify Specific Departmental Costs
Heart Failure & Shock by Level of Severity
Med/ Surg
Minor
ICU/CCU
Moderate
Pharmacy
Radiology
Major
Laboratory
Extreme
Other
$0
$5,000
$10,000
$15,000
$20,000
$25,000
Probable, Possible, Suspected Diagnosis Uncertain
Diagnosis
Inpatient application only:
• These conditions may be coded as though they exist
• Applies to hospital setting only
• If condition is ruled out, it may not be coded
Outpatient application:
Must code signs/symptoms, not the suspected condition
Supports appropriate E&M professional component
34
Possible/Probable Cause of Chest Pain
Anxiety
MS-DRG 880
RW = 0.6191
Biliary Colic
MS-DRGs
444/445/446
RW = 1.5055
Cardiac Cath
MS-DRGs
286/287
RW = 1.9634
GERD Gastritis
MS-DRGs 391/392
RW = 1.0958
Anterior CP
Pleuritic CP
Chest Wall Pain
MS-DRG 204
RW = 0.6472
Psychogenic
Angina Pericarditis
MS-DRGs
314/315/316
RW = 1.7589
Chest Pain
MS-DRG 313
RW = 0.5404
Pleurisy
MS-DRGs
193/194/195
RW = 1.4378
Psychogenic
Chest Pain
MS-DRG 882
RW = 0.6676
35
Costochondritis
Tietze’s Disease
MS-DRGs 205/206
RW = 1.2566
Pulmonary
Embolism
MS-DRGs 175/176
RW = 1.6121
Shingles
MS-DRGs
595/596
RW = 1.7691
CAD
MS-DRGs
302/303
RW = 0.9999
Angina
MS-DRG 311
RW = 0.5128
Cardiac
Arrhythmia
MS-DRGs
308/309/310
RW = 1.2188
Documentation for Pulmonary Embolism
•
Document acuity:
Acute
Chronic
– Healed/old
–
–
•
Specify meaning of “history of PE”
Chronic PE continuing to be treated, is
being prophylactically treated
– or patient no longer has the condition
– “chronic pulmonary embolism” vs.
“healed PE” or “old PE”
–
•
•
Specify if related to any other
condition such as:
–
Atrial fibrillation
–
DVT (specify site and laterality)
–
Hypercoagulable state
–
Malignancy/Orthopedic
surgery/Sepsis/Trauma
–
Not POA and after an operative
episode is considered a patient
safety indicator (PSI 12)
–
A hospital acquired condition
(HAC) when following certain
orthopedic procedures
Document presence of
cor pulmonale (acute
/chronic)
Specify type:
–
–
–
Saddle
Septic
Postprocedural or due to a vascular
device
Myocardial Infarction
ICD-10-CM documentation for myocardial
infarction will need to include:
Type of infarction (STEMI or NSTEMI)
Specific site of myocardium involved (
anterior wall, inferior wall)
Coronary artery involved (LAD, RCA,
LMCA, LCx)
New MI within 4 weeks of a previous
MI
Specify date of onset)
ICD-10
37
Syncope Alternatives”: “possible” “probable”
Heart Failure
MS-DRGs
291/292/293
RW = 1.4609
Alcohol Abuse
MS-DRGs
896/897
RW = 1.4155
Hypotension
MS-DRGs
314/315/316
RW = 1.7589
38
Arrhythmia
MS-DRGs
308/309/310
RW = 1.2188
Syncope
MS-DRG 312
RW = .7215
Anemia
MS-DRGs 811/812
RW = 1.2431
Dig Poisoning
MS-DRGs
917/918
RW = 1.4449
Dehydration
MS-DRGs 640/641
RW = 1.0896
Stroke or CVA
MS-DRGs 64/65/66
RW = 1.8258
Transient Ischemic Attack
• “TIA” = unspecified code
• If known or suspected, document more specific
diagnosis:
–
–
–
–
–
–
–
Amaurosis fugax
Carotid artery stenosis
Carotid artery syndrome
Precerebral artery syndrome
Transient global amnesia
Vertebro-basilar artery syndrome
Other cerebral ischemic attacks and syndromes
Cerebral Infarction
• Specify etiology or cause of the infarct:
– Thrombosis
– Embolism
– Occlusion or stenosis
• Document specific artery involved and laterality:
– Precerebral arteries which include:
• Carotid artery
• Basilar artery
• Vertebral artery
– Cerebral arteries which include:
40
•
•
•
•
Anterior cerebral artery
Cerebellar artery
Middle cerebral artery
Posterior cerebral artery
Cerebral Infarction Following Cardiac Surgery
• Document etiology of cerebral
infarction:
–
–
–
–
Embolism
Thrombosis
Occlusion
Stenosis
• Specify artery involved:
–
–
–
–
–
–
–
Anterior cerebral artery
Basilar artery
Carotid artery
Cerebellar artery
Middle cerebral artery
Posterior cerebral artery
Vertebral artery
• Document the link between the
occluded vessel and the CVA, if
appropriate
• Requires laterality distinction (left
vs. right)
• Intraoperative or postprocedural
cerebral infarction occurring during
cardiac or other type of surgery
Respiratory Failure
• Acute/chronic/acute on chronic
• Cause or etiology (pneumonia, COPD,drug,trauma; if following
surgery was it POA ( a PSI) or due to underlying pulmonary
condition, failure to wean
• Signs :RR> 26, accessory muscles use, altered mental status
• Arterial blood gas and pH:
– pH of <7.30 or >7.50
– pCO2 of >50
– pO2 of <60 (impacted by hemoglobin level)
• Type I Hypoxemic: pO2 60 mm Hg normal or low pCO2
• Type II Hypercapnic: pH < 7.30 and increased
bicarbonate;pCO2 >50
• Chronic : As above and low flow 02 at home; polycythemia;
cor pulmonale; heart failure
• Document in Progress Notes and Discharge Summary:
“improved”
42
Ventilator Support
• Document time of intubation, ventilator start/end times including weaning
times
• Mechanical vent > than 96 hours and may impact the MS-DRG and APR-DRG risk
of mortality (ROM)
• Mechanical ventilation support includes:
– Endotracheal respiratory assistance
– Intermittent mandatory ventilation (IMV)
– Positive end expiratory pressure (PEEP)
– Pressure support ventilation (PSV)
• Mechanical ventilation does not include non-ventilated respiratory treatments
such as:
– CPAP, Bi-PAP or IPPB
43
3M APR DRG Classification System
Risk-Adjusted Mortality Example
APR-DRG 720,
SEPTICEMIA & DISSEMINATED INFECTIONS
Illinois Average
APR DRG
Subclass
1
2
3
4
Total
Advocate Good Shepherd Hosp.
Actual
Cases Deaths Mortality Rate
880
1
0.1%
3,680
50
1.4%
10,539
518
4.9%
11,594 3,067
26.5%
26,693 3,636
13.6%
Actual
Cases
9
26
72
120
227
Actual
Expected Actual Mortality
Deaths Deaths Rate
0.0
0
0.0%
0.4
0
0.0%
3.5
4
5.6%
31.7
28
23.3%
35.6
32
14.1%
Data Source: 3M APR DRG Classification System utilizing MEDPAR 2013
Data based on all cases using selection criteria. No inference is made or conclusion can be drawn about the significance of
actual to expected mortality variance without further study.
44
Sepsis
• Urosepsis imprecise
• No IDD-10 a code for urosepsis
• Sepsis is classified by the
bacteria causing the infection
– Streptococcal sepsis (group A,
group B, Streptococcus
pneumoniae, other
streptococcal) or
– Other sepsis (e.g., MRSA,
pseudomonas)
• Severe sepsis is associated
with organ dysfunction/failure
– Document the specific associated
organ dysfunction (not MOD) and
– Document presence of septic
shock
Diabetes
• Document
– Type Type 1 Type 2 Drug or chemical induced
– Cause :Cushing's syndrome Cystic fibrosis malignant neoplasm malnutrition
or Pancreatitis
– Other specified diabetes mellitus :Genetic defects of beta-cell function
Genetic defects in insulin action or postpancreatectomy diabetes mellitus
postprocedural diabetes mellitus
Manifestations
Cause and effect link between the diabetes and the condition
– “Chronic osteomyelitis of the left ankle due to type 2 diabetes”
– “Type 1 moderate nonproliferative diabetic retinopathy with macular
edema”
Control status:
• “Diabetes with hyperglycemia”
• “Diabetes out of control”
Obesity
• New
– New code for obesity documented as nutritional
or due to excess calories
– Single combination code for morbid obesity with
alveolar hypoventilation
• Stays the Same
• Due to drugs, also specify drug
• Other
– Endogenous, familial
– Endocrine, glandular
» Due to thyroid or pituitary disorder
Body Mass Index
• No changes
• BMI value:
– Predict likelihood of
joint replacement
– Predict how well
patient will do after
surgery
Nutritional Anemias
ICD-10 :more specificity
Specific codes for the different types:
Iron deficiency
“secondary to blood loss, sideropenic, inadequate dietary iron intake
Vitamin B12
“due to intrinsic factor deficiency, vitamin B12 malabsorption”
Folate
“dietary, drug induced “
Other nutritional
“protein deficiency”
Bronchitis
• What’s New
– Combination codes
for acute bronchitis
due to specific
organisms
• If chronic, specify:
– Simple
– Mucopurulent
– Mixed (both simple
and mucopurulent)
Asthma
• Document type
• Document acuity
– With acute
– Mild intermittent
exacerbation
– Mild, moderate, or severe persistent
– With status
asthmaticus
Depression
•
“Depression” is classified in ICD-10 as:
–
•
F32.9 Major depression disorder, single
episode, unspecified
Additional specificity, if known or
suspected, will change the code reported,
for example:
Adjustment disorders with depression
and/or anxiety (grief reaction)
Anxiety depressive disorders
Bipolar disorder with depression
Depressive neurosis, neurotic depression,
or dysthymic disorder
Major depression, single or recurrent
episode
–
–
–
–
–
•
•
•
•
•
Mild
Moderate,
Severe
Severe with/without psychotic features
Or in partial/full remission
Tobacco Dependence and Abuse/Use
– Separate codes for:
• Tobacco abuse/use
• Tobacco dependence
– Type of tobacco
product
• Cigarettes
• Chewing tobacco
• Other, such as cigars
– Ability to differentiate
• Personal history of
tobacco use versus
current use
• For dependence:
– Currently in remission
– With withdrawal
– With nicotine-induced disorder
– Exposure to second hand
smoke
Drug Underdosing
• Identifies intentionally or unintentionally
taking less of a medication than prescribed
• Document intentional versus unintentional
or accidental
– Intentional
• For example, due to financial hardship
– Unintentional or accidental
• For example, due to age related disability
– Age-related dementia
– Rheumatoid arthritis of hands
Coma
Glasgow Coma Scale (GCS)
• Based on 3 categories of responsiveness: eye opening, best
motor response, and best verbal response.
• Lower the GCS, the deeper the level of unconsciousness.
– 90% with a score < or equal to 8 are in a coma
– 50% with score < than or equal to 8 at six hours die
• Head injury classification:
– Severe – GCS 8 or less
– Moderate – GCS 9 to 12
– Mild – GCS 13 to 15
55
Documentation of Pancreatitis
History: 66 year old male admitted with nausea, vomiting, and abdominal
pain; history of elevated triglycerides and daily alcohol use.
Lab: Elevated lipase and amylase
Treatment: IVF, NPO, pain control, electrolyte correction.
Current Documentation
Improved Documentation
Final Diagnosis: Pancreatitis,
alcohol abuse
Final Diagnosis: Acute pancreatitis
due to alcohol dependence
Ulcerative Colitis
• Document anatomical
site:
– Pancolitis
– Proctitis
– Rectosigmoiditis
• Document any
associated complications
such as:
– Abscess
– Fistula
– Intestinal obstruction
– Rectal bleeding
• Avoid documenting
“inflammatory
bowel disease”
when the intended
diagnosis is
ulcerative colitis
– Inflammatory bowel
disease is classified
as noninfective
gastroenteritis
Viral Hepatitis
• Document type
– A, B, C, E, Non-A or Non-B
• For hepatitis B, document any findings of
delta agent
• Specify acuity
– Acute, chronic
• Document presence of hepatic coma,
encephalopathy or hepatic failure
Neoplasms
•
59
•
Document specific site and laterality for example:“Malignant neoplasm of
central portion of left female breast” or “Benign neoplasm of right ovary sites”
Document primary and all secondary neoplasms
•
Specify if the primary site is still present
•
Document the reason or multiple reasons for admission:
– Chemotherapy/immunotherapy/radiotherapy
– Treatment of symptoms associated with the malignancy (e.g., headache,
weakness, Intractable pain requiring pain control/management
– Staging to determine the extent of the malignancy
– Treatment of conditions associated with malignancy (e.g., anemia [specify
type], ascites, dehydration, malnutrition)
– Treatment directly towards primary or secondary malignancy
Anemia in Chronic Disease
• Document the link between the chronic
disease and the anemia
– Chronic kidney disease
– Neoplastic disease
• Examples
– Anemia due to CKD stage 3
– Anemia associated with lung cancer
• Distinguish if the anemia is due to the
malignancy or the chemotherapy
Blood Loss Anemia
• Blood loss anemia may be due to trauma,
gastrointestinal conditions, obstetrical delivery or
surgery or other causes
• Document:
– Anemia due to acute blood loss
– Anemia due to chronic blood loss
– Postoperative anemia due to blood loss
• Link anemia to the blood loss, when appropriate
• Anemia following surgery with an expected amount
of blood loss may be documented as acute blood loss
anemia.
Adult Malnutrition
• Classification of adult malnutrition is based on the
documented known or suspected etiology:
– Starvation-related
– Chronic disease-related
– Acute disease or injury-related
• Two or more of the following six characteristics required:*
–
–
–
–
–
Insufficient energy intake
Weight loss
Loss of muscle mass
Loss of subcutaneous fat
Localized or generalized fluid accumulation that may mask weight
loss
– Diminished functional status as measured by hand grip strength
*May 2012, the Academy of Nutrition and Dietetics (Academy) and the American Society for Parenteral and Enteral Nutrition (ASPEN)
“Postoperative” Diagnosis: Two Definitions
Clinical Definition
“A condition occurring in the postoperative
period”.
Coder Definition
“A diagnosis related to the surgical
procedure”
Complication-900 code
“Coder cannot make the determination if it is a
complication or an expected outcome”
(Coding Clinic 4/27/2011)
63
Examples
Complication
Non-Complication
• Postop ileus (997.4 + 560.1)
• Ileus
• Ileus secondary to surgery
• Prolonged ileus
(997.4 + 560.1)
• Post op atelectasis (997.39 + 518.0)
• Expected ileus
• Post op anemia
• Incidental atelectasis
(998.11 + 285.1)
• Atelectasis
• Acute blood loss anemia
64
Complications of Surgery
• ICD-10-CM codes provide specificity to report
– Timeframe of when complication occurred
• Intraoperative or postoperative
– Body system of organ related to complication
– Body system on which the procedure was performed
– Example of infection following a procedure
•
Notice in this example,
it does not matter what
body system on which the
procedure was performed
3M APR DRG Classification System
Risk-Adjusted Mortality Example
APR-DRG 308, HIP & FEMUR PROCEDURES FOR TRAUMA EXCEPT JOINT
REPLACEMENT
Illinois Average
APR DRG
Subclass
1
2
3
4
Total
Cases
1,500
2,587
1,401
296
5,784
Advocate Christ Med Ctr.
Actual
Deaths Mortality Rate
3
0.2%
9
0.3%
28
2.0%
61
20.6%
101
1.7%
Actual
Cases
30
38
21
8
97
Actual
Expected Actual Mortality
Deaths Deaths Rate
0.1
0
0.0%
0.1
1
2.6%
0.4
1
4.8%
1.6
4
50.0%
2.2
6
6.2%
Mortality
Rate %
Variance
-100%
900%
150%
150%
173%
Data Source: 3M APR DRG Classification System utilizing MEDPAR 2013
Data based on all cases using selection criteria. No inference is made or conclusion can be drawn about the significance of
actual to expected mortality variance without further study.
66
Documentation Requirements for Fractures
Physician documentation requirements
• Encounter: initial, subsequent, sequale
• Open
• Closed (Gustilo Open Fracture Classification )
• Salter-Harris Classification for growth plate fractures
• Displaced or nondisplaced
• Name of bone and specific part of the bone that is fractured
• Laterality – right or left
• Orientation of fractures of the shaft of the bone such as:
• Comminuted/Oblique/Segmental/Spiral/Torus/Transverse
67
ICD-10 Diagnosis Code
Code Example Fracture Femur
S
Fracture of
the femur
68
7
Head &
Neck
2
0
Base of
Neck
4
2
Displaced
fracture left
K
Subsequent encounter
for closed fx with
nonunion
Documentation Examples
• Documentation example today:
– Patient seen for follow up of hip fracture
• 820.8 Fracture of hip, unspecified part of neck of femur, closed
• V54.13 Aftercare for healing, traumatic fracture of hip
• Documentation needed for ICD-10:
– Subsequent encounter for nonunion displaced fracture base
of the femur neck left hip
• S72.042K Displaced fracture of base of neck left femur, subsequent
encounter, closed fracture, non-union
69
Fracture Treatment
• Reduction: open vs. closed
• Fixation: internal vs. external vs. no fixation device
• Reduction = “reposition” in ICD-10-PCS
– Example “Closed reduction with percutaneous internal fixation of
right femoral neck fracture”
ICD-10 Documentation Requirements for Procedures
71
Laterality of site
―
Left
―
Right
―
Bilateral
Specificity of approach
•
Open
•
Percutaneous
•
Percutaneous endoscopic
•
Via natural or artificial opening
•
Via natural or artificial opening- endoscopic
•
Open with percutaneous endoscopic assistance
•
External
Documentation of Root Operation
• The root operation depends on the intent
of the procedure
– If the intent of the procedure is vague or
unknown, the physician may need to be
queried for clarification
– Example: Revision of hip replacement
• Operative report needs to be descriptive as to how
the hip joint was revised so that the appropriate
root operation can be identified (e.g., revision,
replacement, removal, supplement)
72
Documentation of Root Operation
• The physician is not expected to document in
“ICD-10-PCS terms”
– It is the coder’s responsibility to determine what the
documentation in the medical record equates to in
the ICD-10-PCS definitions
– Example: Arthroscopy
• It is understood that the root operation for a arthroscopy is
inspection – even without physician documentation of
“inspection”
– Physician documentation needs to be complete
enough to describe the entire procedure performed
73
Total Joint Replacement
• Specify joint and laterality
• Document device inserted:
• Autologous tissue substitute
• Nonautologous tissue substitute
• Synthetic substitute
• If synthetic substitute, specify:
•
•
•
•
Metal
Metal on polyethylene
Ceramic
Ceramic on polyethylene
• Also specify the following for synthetic substitute:
• Cemented
• Uncemented
Documentation of a procedure:
Example stent ICD-10-PCS
Section
Body
System
Root
Operation
0
2
7
Med/Surg
Body
Part
B 3
Dilatation
Heart & Great
Vessels
Approach
Device
Qualifier
4
Z
Percutaneous
Coronary
Artery
None
Transluminal
Device, Drug
Eluting
Coronary Angioplasty
• Root operation: Dilation (expanding an orifice or the lumen of a tubular body
part)
• Body part: Coronary artery [specify number of coronary artery sites receiving
treatment]
• Approach: Open, percutaneous or percutaneous endoscopic
• Device: Drug-eluting intraluminal device, intraluminal device, radioactive
intraluminal device, no device
• Qualifier: Bifurcation or no qualifier
• Document body part, approach, device and qualifier [if any]
Insertion of PICC Line
ICD-10-PCS code assigned
02HV33Z
Lumbar Puncture
• Root operation: Drainage (taking or letting out fluids and/or gases
from a body part)
• Body part: Spinal canal
• Approach: Percutaneous
• Document if procedure was therapeutic or diagnostic
Section
0
Med & Surg
Body System
0
Central Nervous System
Root Operation
9
Drainage
Body System
U
Spinal Canal
Lumbar Puncture
009U3ZX
Approach
3
Percutaneous
Device
Z
No Device
Qualifier
X
Diagnostic
Impact of Documentation
MS-DRG 330
2.4981
MS-DRG 329
5.1396
MS-DRG 329
5.1396
Bowel Procedure
with MCC
Bowel Procedure
with CC
Bowel Procedure
with MCC
PDx: Colon cancer
PDx: Colon cancer
SDx:
SDx:
SDx:
Dehydration
Acute Renal Failure – ATN
Acute Renal Failure – ATN
Post-op ileus
(codes to 997.4 + 560.1)
Expected ileus
(560.1)
Expected ileus
(560.1)
“Ulcer/Wound” noted by RN
Pressure Ulcer, site unspecific
Pressure Ulcer Stage IV
on Sacrum
PPx: Left hemicolectomy
PPx: Left hemicolectomy
PPx: Left hemicolectomy
APR DRG:
SOI Level:
APR Weight:
ROM Level:
Peer Group
79
221
2
1.7681
1
0.0%
APR DRG:
SOI Level:
APR Weight:
ROM Level:
Peer Group
Highest MSDRG payment
221
3
2.9531
3
2.5%
PDx: Colon cancer
APR DRG:
SOI Level:
APR Weight:
ROM Level:
Peer Group
221
4
6.3732
4
24.2%
Clinical Informatics/Clinical
Documentation Improvement
(CDI)/Coding
How can we help you?
January 29th & 30th, 2015
Clinical Informatics
Clinical Informatics
Who we are:
Informatics experts, leaders, and change
agents utilizing innovation, evidence-based
practice, quality, and collaboration, to create
the safest environment resulting in the best
health outcomes for our patients.
82
Clinical Informatics bridges….
• Promotes
understanding,
integration, and
application of
technology in the
healthcare setting
• Supports
interdisciplinary
approach across the
continuum of care
Clinical Science
Clinical Informatics
Computer
Science
83
Information
Science
Clinical Informatics role with
ICD-10
• Ensure EMR documentation supports new
requirements – partnering with CDI
• New documentation changes in EMR need to
reflect physician workflows and evidence
based practice
• Educate and support physicians with new
documentation practices.
• Enhance voice recognition capabilities to
reflect ICD-10 changes and best practice
84
CDI-ICD-10 Physician
Education
Stephen Crouch, MD
Medical Director, Care Management
stephen.crouch@advocatehealth.com
Kelly Tarpey RN, MSN, CPHQ
System Director, Clinical Documentation
Improvement
kelly.tarpey@advocatehealth.com
86
Plan: Standardizing CDI
Practice
People
Process
Tools
Accurate
picture of
the patients
we care for
Case Mix Index
IMPACT:
• Improvement from baseline at 8 of 10 facilities in
November
89
•
•
Medicare only
Reported 15 days post month end close
Advocate Care Connection Query Process
Do not type your reply hereSee step 2 below
90
Sherman CDI Query Process
91
How You Can Help
• Promptly reply to CDI staff query
o Agreement is not required
o If you do not agree, please provide a brief rationale
• Spread the word among your colleagues
• Interact with CDI staff / ask questions
o Learning process for physicians and CDI staff
o Will be able to track frequent questions and help CDI
staff direct physician education
• More robust physician clinical documentation will
smooth the transition to ICD-10
92
93
Documentation
for Coding
Lou Ann Schraffenberger, Downers Grove Support Center
Dawn Monegato, Advocate Lutheran General Hospital
Principal Diagnosis
• Definition
• The reason for admission after study that is
chiefly responsible for occasioning the
admission of the patient for care
• After all is said and done…
– Why did the patient have to be in the hospital?
– Why couldn’t the patient been taken care of at
home or in an outpatient status?
95
Patient’s Medical Record
• Medical Record is the “Storybook”
–
–
–
–
–
–
–
Describes the patient’s illness and care
What’s the patient’s story?
Diagnoses are carried throughout the record
Not just a diagnosis listed on a Problem List
Not something only mentioned once
Diagnoses: What’s been ruled-out?
Diagnosis written by a consultant that the attending
physician never mentions
– Timeliness and completeness of discharge summary
96
Diagnoses and Procedures
• All of these determine the MS-DRG
– Determines payment
– Determines severity of illness and risk of mortality
• Principal diagnosis
• Principal procedure
• Secondary diagnoses
– Condition evaluated, treated, had a diagnostic
procedure, affected the length of stay or the
amount of nursing care
97
Top 10 List of Questions to Doctors
• The top 10 diagnoses
that coders contact a
physician for diagnosis
clarification
–
–
–
–
–
Heart failure
Debridement procedures
Malnutrition
Sepsis, SIRS, bacteremia
Acute vs chronic blood
loss anemia
– Catheter associated
urinary tract infection
– Altered mental status vs.
encephalopathy
– AKI, ARF
– Respiratory failure,
insufficiency, distress
– Pathology diagnoses not
included in attending
physician’s
documentation
98
#1 Heart Failure
•
•
•
•
•
•
•
99
Systolic heart failure
Diastolic heart failure
Combined systolic and diastolic
Acute
Chronic
Acute on chronic
Congestive heart failure is considered less
specific
#2 Debridement
• Excisional
– Must be stated
– Coder cannot assume
everything doctor does
is surgical
– Coded to deepest depth
•
•
•
•
Skin or subcutaneous
Fascia
Muscle
Bone
– “Sharp” is not enough
• Non-Excisional
– Default code if excisional
is not stated
– Not considered a surgical
procedure
– Ultrasonic
– Versajet
– Pulsed lavage
– Dermabrader
– Wet-to-dry dressings
100
#3 Malnutrition
• Type and severity
• First-second-third degree
– Mild, Moderate, Severe
• Protein “calorie”
– Mild, Moderate, Severe
• “Protein” malnutrition codes to Kwashiorkor
– Rare severe protein deficiency
– Not seen in the USA
101
#4 Sepsis
• Sepsis, a systemic infection
– Bacterial organism, if known
– Is it viral instead of bacterial
• Is SIRS present?
• Is septic shock present?
• Is there an underlying infection?
– such as pneumonia, urinary tract infection,
infected decubitus ulcer, peritonitis?
• Is it Bacteremia instead?
102
#5 Blood Loss Anemia
• Acute
– Anemia due to acute blood loss
– Cause?
– Intraoperative, postoperative, or posthemorrhagic
• Chronic
– Anemia due to chronic blood loss
– Cause?
– Normocytic anemia due to blood loss?
103
#6 CAUTI
• Catheter associated urinary tract infection
• Patient had a Foley catheter and a urinary
tract infection
– Is the UTI due to the urinary catheter?
– Was it present on admission?
– Was it hospital acquired?
104
#7 AMS/Encephalopathy
• Altered mental status
– Cause?
– It will be coded to a
“symptom” which
means doctor could
not identify the cause
– If the patient has AMS
due to known
condition, important
to document
– Is it the same as
encephalopathy?
105
• Encephalopathy-type?
- Alcoholic
- Arteriosclerotic
- Hepatic
- Hypertensive
- Hypoglycemic
- Metabolic
- Posttraumatic
- Septic
- Toxic
#8 Acute Kidney……
• AKI – acute kidney injury
– Do you mean the same as acute renal failure?
– It doesn’t mean acute kidney “insufficiency” –
right?
– Anymore descriptions available?
• Tubular necrosis
• Acute cortical necrosis
• Medullary necrosis
106
#9 Respiratory Failure
• Find the mixing of the phrases in record
–
–
–
–
–
Respiratory failure
Acute respiratory failure
Respiratory insufficiency
Respiratory distress
Chronic respiratory failure-insufficiency-distress
• Underlying cause?
• Postoperative status?
107
#10 Pathology Findings
• Pathology diagnoses not documented by the
attending physician or surgeon
• Coder cannot code from the pathologist’s
report without the attending physician or
surgeon documenting as a diagnosis
• Acceptable to be written after discharge if the
pathologist report was not available when the
patient went home
108
Sorry, there are more!
• CVA versus TIA
– Which is it?
• Pneumonia
– What type is it?
• BMI is calculated
– “obesity,” “overweight,” or “underweight,” must be
written
• Syncope
– Was a cause established?
• Fall and Motor Vehicle Accident are not “diagnoses”
• Fracture
– Traumatic versus pathologic with its cause
109
Appreciate Your Attention….
• Coder’s questions
• Clinical documentation specialist’s questions
– Your “responses” have to be written in the record
in a progress note or discharge summary
• More insurance company audits occurring
– Not just Medicare and Medicaid
– Coding is being challenged every week
• Coding is telling the patient’s story… we want
it to be accurate
110
Thank You!
•
•
•
•
Questions?
Comments?
Requests?
Remarks?
• Contact your hospital’s HIM
Department Director or Coding
Leader if we can help
•
•
•
•
•
•
•
•
•
•
•
•
Diane.cronin@advocatehealth.com (ACMC)
Susan.bittner@advocatehealth.com (COND)
Kathryn.anthony@advocatehealth.com (GSAM)
Kim.ferris@advocatehealth.com (GSHP)
Latarsha.atkins@advocatehealth.com (IMMC)
Dawn.monegato@advocatehealth.com (LGH)
Julie.mueller@advocatehealth.com (SHERM)
Felicia.evans@advocatehealth.com (SSUB)
Patricia.warren@advocatehealth.com (TRIN)
Heather.segerstrom@advocatehealth.com
(BROMENN)
Lynnette.haller@advocatehealth.com (EUREKA)
Louann.schraffenberger@advocatehealth.com
111
Break
15 Minutes
Using CareConnection to
Improve Documentation
Anupam Goel
(anupam.goel@advocatehealth.com)
Why document in the
electronic medical record?
• Identify issues that need additional attention before
moving the patient out of the hospital
• Let other team members know what you are doing
• Protect yourself in a lawsuit
• Justify payment
114
Why document in the
electronic medical record?
• Identify issues that need additional attention before
moving the patient out of the hospital
• Let other team members know what you are doing
• Protect yourself in a lawsuit
• Justify payment
• Determine
– Illness severity and risk of mortality
– Health of a population for value-based purchasing (to be done
annually)
– Public physician quality scorecards
115
Documenting for multiple
purposes
• Enter all relevant diagnoses
– Prefer discrete data entry, but free-text is acceptable
– Be as specific as possible about the patient’s condition or
diagnosis
– IMO search field can help suggest specific diagnoses
• Use the free-text section after each diagnosis to
– Include all of the relevant information that you use to make a
clinical decision justifying the diagnosis or treatment step you
chose
• Update documentation as new information becomes
available
116
Nuances to Advocate’s
CareConnection system
• Currently, inpatient billing is performed in an outside
system
– No ICD-10 code selected in CareConnection directly goes onto a
patient’s bill
– CDI and coding teams need enough information to support
specific diagnoses in your documentation for the relevant ICD-10
codes to be selected in the billing system
• Outside of ICD-10 or physician documentation, there are
efforts to get patients information about their condition
– Encounter diagnoses (this hospitalization)
– Problem list (ongoing issues)
117
On admission
• Diagnoses: use symptoms rather than “rule out”
“Chest pain,” not “rule out MI”
• Free-text section: consider adding these
descriptors
•
•
•
•
•
•
118
Where (site and laterality)
Specificity
Timing (acute or chronic)
Manifestations
Stage
Status (new, unchanged, improving, resolving)
Daily progress notes
• Update diagnoses after reviewing test results
and seeing the patient
• Use the “..dx” term to pull in all diagnoses
with “_” to enter free-text information
• Copy-and-paste is strongly discouraged
If you must, be sure to update every diagnosis
based on new patient information
119
On discharge
• Include
– All diagnoses addressed over the course of the
hospitalization
– Conditions that have been evaluated, but a
definitive diagnosis is not yet known (chest pain,
non-cardiac)
• Describe next steps for each ongoing
condition in the discharge summary
• Update the patient’s problem list based on
the hospital events
120
Case Examples Discussion
3M DRG Assurance Program
122
The 3M DRG ASSURANCE™ Program
Case Studies Advocate
Physician
Presentation
Thomas C Kravis MD
January 29 2015
Case Study Sepsis
• Patient admitted with dysuria, fever, altered mental status.
• “Urosepsis” documented in progress notes.
• Lab reports showed serum creatinine and BUN levels of 4.5 &
50, respectively. Low urinary output
• Physician ordered 1L of IV NS wide open with maintenance IV
fluids of 150 cc/hr to follow.
• Serial creatinine and BUN levels declined over the next 3 days
to 1.2 & 24, respectively.
Advocate Case Sepsis
Before
After
MS-DRG: 690 (without MCC)
Relative weight: 0.7693
MS-DRG: 871 (with MCC)
Relative weight: 1.8527
PDx: Urinary tract infection
PDx: Sepsis
SDx: AML
Coronary artery dz
Hypertension
Hyperlipidemia
SDx: Add:
Acute renal failure
with acute tubular
necrosis
Query for corresponding
diagnosis
Procedures:
APR DRG:
SOI Level:
APR Weight:
ROM Level:
Exp. Mort Rate:
Procedures:
463
2
0.5233
2
0.3%
APR DRG:
SOI Level:
APR Weight:
ROM Level:
Exp. Mort Rate:
720
4
2.8127
3
6.3%
This report includes data produced by 3M’s
proprietary APR-DRG Software. All copyrights in and
to APR-DRG Classification System and all APR-DRG
Code Assignments are owned by 3M. All rights
reserved.
Altered Mental Status Alternatives
Alzheimer’s
Disease
Parkinson’s
Disease
Drug-Induced and
Alcoholic Delirium
and Dementia
MS-DRGs 056/557
RW = 1.7368
MS-DRGs 896/897
RW = 1.5146
CVA
MS-DRGs
064/065/066
RW = 1.7417
TIA
MS-DRG 069
RW = 0.6948
Dementia and
Vascular Dementia
Encephalopathy and
Metabolic
Encephalopathy
MS-DRG 884
RW = 1.0060
Acute
Confusional State
Altered Mental
Status
MS-DRGs 880
RW = 0.6388
MS-DRGs 947/948
RW = 1.1324
MS-DRGs 070/071/072
RW = 1.6593
Hypertensive
Encephalopathy
MS-DRGs
077/078/079
RW = 1.6290
UTI
MS-DRGs 689/690
RW = 1.1300
Coma
Diabetic
Ketoacidosis
MS-DRGs
637/638/639
RW = 1.3888
MS-DRGs 080/081
RW = 1.2252
Hepatic
Encephalopathy
MS-DRGs
441/442/443
RW = 1.8534
Seizures
Toxic and Anoxic
Encephalopathy
MS-DRGs 100/101
RW = 1.5185
MS-DRGs 091/092/093
RW = 1.5851
CMS
Definitions
• Bacteremia – nonspecific laboratory finding of bacteria in
the blood with no signs of illness.
• Septicemia – “systemic disease associated with the
presence of pathogenic microorganisms in the blood.”
(positive blood culture and fever)
• Sepsis – “SIRS due to an infection.” An infection-induced
syndrome in the presence of two or more manifestations of
SIRS without organ dysfunction. Septicemia that has
advanced to involve two or more manifestations of SIRS.
• Severe sepsis – Sepsis with associated acute organ
dysfunction.
• Septic shock – severe sepsis in which the cardiovascular
system begins to fail, blood pressure drops, and vital organs
are deprived of adequate blood supply
Continuum of Illness Due to
Infection
Bacteremia
Document the clinical “theme”
in the medical record through
to the discharge summary.
Septicemia
Sepsis
Severe Sepsis
Septic Shock
Documentation of Acute Tubular Necrosis (ATN)
• Document signs, symptoms, findings
and treatments for ATN
• Acute tubular necrosis (ATN)
– Document hypoperfusion to the renal
cell caused by surgery, hypovolemia,
hypotension or infection
– Document causative medications such
as antibiotics, ACE inhibitors, ARBs,
chemotherapy agents , IV contrast
– Document other conditions such as
rhabdomyolysis and sepsis
Signs and Symptoms
― ↓decrease urine output, fluid
retention
― Increase in serum creatinine
― Electrolyte abnormalities
(hyperkalemia, hyponatremia,
metabolic acidosis, altered mental
status, nausea and vomiting)
Diagnostic testing
― UA for renal tubular casts, renal
ultrasound, biopsy
Treatment
― Treating underlying cause,
optimization of CV function and
intravascular volume, diuretics or
dialysis
Specificity of Secondary Diagnosis: Impact on SOI and ROM
Diagnosis
Severe malnutrition
Malnutrition of moderate degree
Severity of Illness Impact
Extreme
High
Low
Extreme
High
X
Medium
Low
X
X
X
X
Malnutrition of mild degree
Malnutrition, unspecified
Medium
Risk of Mortality Impact
X
X
X
X
Cachexia (wasting disease)
X
X
Anemia, unspecified
X
Acute blood loss anemia
X
X
Chronic blood loss anemia
X
X
X
Dehydration
X
Hyponatremia
Hypernatremia
130
X
© 3M 2015. All Rights Reserved.
X
X
X
Case Study Neuro/Trauma
• Patient admitted with traumatic subdural hemorrhage.
• H&P s “significant amount of midline shift over 1 cm…largely
symptomatic from her right sided subdural hematoma.”
• SEPS drain was placed in ICU without successful drainage.
• CT of head “left-to-right midline shift of 11mm…there may be
early herniation as well.”
• Patient expired.
Sample Case Neuro
Before
After
MS-DRG: 087 (without
CC/MCC)
CMI: 0.7345
LOS: Traumatic
2.2
PDx:
subdural
MS-DRG: 085 (with MCC)
CMI: 1.9733
LOS: 4.9
PDx: Same
hemorrhage, no LOC
SDx: Alzheimer’s dementia
Unspecified fall
Palliative care
APR DRG:
SOI Level:
APR Weight:
ROM Level:
Exp. Mort Rate:
055
1
0.6365
2
2.9%
SDx: Add:
Herniation of brain
APR DRG:
SOI Level:
APR Weight:
ROM Level:
Exp. Mort Rate:
055
3
1.3717
3
7.5%
This report includes data produced by 3M’s
proprietary APR-DRG Software. All copyrights in and
to APR-DRG Classification System and all APR-DRG
Code Assignments are owned by 3M. All rights
reserved.
Head Injury
• Nonspecific:
– Closed head injury (CHI)
– Traumatic brain injury (TBI) - diffuse or focal
– Intracranial injury
• Document the specific type of injury:
–
–
–
–
–
–
–
Brain herniation
Cerebral edema
Compression of brain
Concussion
Contusion of brain
Hemorrhage of brain
Laceration of brain
• Specify if any loss of consciousness and the time duration
• Encounter
Traumatic Brain Hemorrhage
• Specify site
– Left or right
cerebrum
– Cerebellum
– Brainstem
– Epidural
– Subdural
– Subarachnoid
• Specify if with LOC
and for how long in
order to accurately
report time.
Subarachnoid, Intracerebral and Intracranial Hemorrhage
•
•
Clarify if subarachnoid, intracranial and intracerebral hemorrhages are traumatic or
non-traumatic
Subarachnoid hemorrhage: document the specific artery where hemorrhage occurred
and the laterality :
–
–
–
–
–
•
Intracerebral hemorrhage: document the specific location:
–
–
–
–
–
•
•
Carotid siphon and bifurcation
Middle cerebral artery
Anterior communicating artery
Posterior communicating artery
Basilar artery
Subcortical hemisphere
Cortical hemisphere
Brain stem
Cerebellum
Intraventricular
Intracranial hemorrhage: document as extradural/epidural hemorrhage or subdural
hemorrhage
Subdural or extradural hemorrhage: document as acute, subacute or chronic
Cardiac Arrest
• Document the underlying cause or etiology if known or
suspected
• Indicate a linkage to the known or suspected etiology
by selecting words such as “due to” or “secondary to”
End of Life/Palliative Care Documentation
• When further treatment is deemed futile or in which patient/family has declined further
treatment, the patient’s chart may have typical documentation that includes:
– “Comfort measures”
– “Supportive care”
– “Condition grave”
• Even though no aggressive treatment will be rendered, it is critical that documentation
of the patient’s status and subsequent conditions are documented to accurately reflect
patient’s extreme severity of illness and risk of mortality. Examples include:
–
–
–
–
Coma
Agonal respirations
Respiratory failure
Renal failure
• Also remember to fully document the underlying terminal diagnosis (cancer, end-stage
heart failure or renal failure)
MacNews Tuesday October 11, 2011
“Steve Jobs Dies of Respiratory Failure
. Steve Jobs' death certificate lists respiratory
failure caused by the spread of a metastatic
pancreas neuroendocrine tumor.”
Case Study Pulmonary
• Patient admitted through ED with obtundation, labored
breathing, and fever. Diagnosed with pneumonia.
• Temp 102.9, BP 97/57; O2 sat 84% on R/A. WBCs 20,000 with
left shift. BUN/Creatinine = 49/2.1. ABGs: pH 7.33; pCO2 60;
pO2 55. Changed to 100% NRB mask.
• BP started to drop: 85/57, 97/46, 90/60. Placed on Levophed
infusion @ 90cc/hr. BP cont’d to drop. Dopamine.added.
Received IV Rocephin and IV Flagyl.
• Patient became unresponsive to tactile and verbal stimuli.
Cardiac arrest occurred.
• Patient was subsequently intubated and expired.
Sample Case: Pulmonary Medicine
Before
After
MS-DRG: 194 (with CC)
Relative weight: 0.9771
MS-DRG: 871 (with MCC)
Relative weight: 1.8527
PDx: Pneumonia
SDx: Atrial fibrillation Left
heart failure
Atelectasis
Hypotension
Cystic kidney disease
Edema
Renal insufficiency
History of colon CA
PDx: Sepsis
Procedures: Mech vent &
intub
APR DRG:
SOI Level:
APR Weight:
ROM Level:
Exp. Mort Rate:
139
3
1.0089
3
4.5%
SDx: Add:
Septic shock
Acute renal failure
Acute respiratory
failure
Coma
Query for corresponding
diagnoses and for principal
diagnosis
APR DRG:
SOI
Level:
Procedures:
APR Weight:
intubation
ROM
Level:
Exp. Mort Rate:
Mech vent
720
&4
3.0499
4
29.8%
This report includes data produced by 3M’s
proprietary APR-DRG Software. All copyrights in and
to APR-DRG Classification System and all APR-DRG
Code Assignments are owned by 3M. All rights
reserved.
Case Study Orthopedics
• 80 y/o female admitted with fractured ankle after a fall at
home.
• To surgery for repair.
• Admission orders indicated “continue home meds” including
Lisinopril 20 mg daily
• Nurses’ notes indicate heart failure and the presence of a dual
chamber permanent cardiac pacemaker.
Case study Orthopedics
Before
After
.
MS-DRG: 493 (with CC)
Relative weight: 1.9971
MS-DRG: 494 (without
CC/MCC)
Relative weight: 1.5073
PDx: Fracture of ankle
PDx: Same
SDx: None
SDx: Add:
Left heart failure
S/P cardiac pacemaker
Query for corresponding
diagnoses
Procedures: ORIF of ankle
Procedures: Same
APR DRG:
SOI Level:
APR Weight:
ROM Level:
Exp. Mort Rate:
313
1
1.0420
1
0.0%
APR DRG:
SOI Level:
APR Weight:
ROM Level:
Exp. Mort Rate:
313
2
1.5059
2
0.1%
This report includes data produced by 3M’s
proprietary APR-DRG Software. All copyrights in and
to APR-DRG Classification System and all APR-DRG
Code Assignments are owned by 3M. All rights
reserved.
Documentation Requirements for Fractures
Gustilo Open Fracture Classification
The following is required for open fractures of the forearm, femur,
lower leg or ankle:
– Type I: clean wound less than 1 cm with minimal soft tissue injury. Bone
fracture is simple with minimal comminution.
– Type II: moderately contaminated wound greater than 1 cm with
moderate soft tissue injury. Fracture contains moderate comminution.
– Type III: extensive skin damage involving muscle or nerves. Type III is
further subdivided as follows:
• Type III A: extensive laceration of soft tissues with bone fragments
from severe comminution or segmental fractures
• Type III B: extensive lesion of soft tissues with periosteal stripping
and contamination which usually requires a flap to cover the
exposed bone
• Type III C: exposed fracture with major vascular injury requiring
repair for limb salvage
Documentation of Root Operation
• The physician is not expected to document
in “ICD-10-PCS terms”
– It is the coder’s responsibility to determine
what the documentation in the medical record
equates to in the ICD-10-PCS definitions
– Example: Arthroscopy
• It is understood that the root operation for a
arthroscopy is inspection – even without physician
documentation of “inspection”
– However, the physician documentation needs
to be complete enough to describe the entire
procedure performed
ICD-10 Documentation Requirements for Procedures
•
Laterality of site
–
–
–
•
Left
Right
Bilateral
Specificity of approach
•
•
•
•
•
•
•
Open
Percutaneous
Percutaneous endoscopic
Via natural or artificial opening
Via natural or artificial opening- endoscopic
Open with percutaneous endoscopic assistance
External
Fracture Treatment
• Reduction: open vs. closed
• Fixation: internal vs. external vs. no fixation device
• Reduction = “reposition” in ICD-10-PCS
– Example “Closed reduction with percutaneous internal fixation of
right femoral neck fracture”
ICD-9 vs. ICD-10
Structural Changes
• ICD-9 (Diagnoses)
#
#
#
#
#
3-5 characters
Category
etiology, site,
manifestation
ICD-10 (Diagnoses)
a
#
a/#
a/#
a/#
a/#
a/#
3-7 characters
Category
etiology, site,
manifestation
extension
Case Study Advocate Surgery
• Patient presented with active GI bleeding secondary to
diverticular disease and AVM.
• Admission H&H = 12.7/36.5. Progress note on 2nd hospital day
states “Hct 35 down to 33%. Continues to have slow bleed.”
GI note on 4th hospital day states “actively bleeding AVM.”
Lowest serial H&H is 11.3/32.7.
• Transfused with PRBCs. On the 5th hospital day, patient is given
250cc bolus of IV fluids and placed on strict I&Os with
continued IV fluids. Cardiology consult note also indicates
“pulmonary hypertension.”
Advocate Sample Case: Surgery
Before
MS DRG:
After
331 (w/o CC/MCC)
Relative Wt:
1.6267
MS DRG:
Relative Wt:
331 (w/o CC/MCC)
1.6267
PDx:
Diverticulosis of Colon
With Hemorrhage
PDx:
Same
SDx:
Angiodysplasia/AVM
Type 2 Diabetes Mellitus
Coronary Artery Disease
Hemorrhoids
Hypertension
S/P Cardiac Pacemaker
SDx:
Same
Total Colectomy
Colonoscopy
EGD with Closed Biopsy
PRBC Transfusion
Endoscopic Destruction of
Lesion of Large Intestine
Procedures:
Procedures:
3M APR DRG:
SOI Level
APR Weight
ROM Level
Exp. Mort Rate
221
2
1.7686
2
0.90%
ADD:
Chronic Blood Loss Anemia
Hypovolemia
Pulmonary Hypertension
Same
Query for Chronic Blood Loss Anemia
and Hypovolemia
3M APR DRG:
SOI Level
APR Weight
ROM Level
Exp. Mort Rate
Change:
221
3
3.0683
2
0.90%
0.00%
This report includes data produced by
3M’s proprietary APR-DRG Software. All
copyrights in and to APR-DRG
Classification System and all APR-DRG
Code Assignments are owned by 3M. All
rights reserved
Drivers of Severity and ROM ( partial list)
• Common Severity/Mortality Drivers
• Acute blood loss anemia
• Acute renal failure (indicate underlying cause)
• Electrolyte imbalances (hypo/hypernatremia, hypo/hyperkalemia, hypo/hypermagnesemia,
hypo/hypercalcemia)
• Encephalopathy (specify type, acuity and cause)
• End stage renal disease (specify underlying cause)
• Gastrointestinal hemorrhage (document acuity and link to site of bleed)
• Heart failure (specify acuity and type)
• Hemiparesis (specify cause and laterality)
• Hypotension (specify cause)
• Ileus
• Malnutrition (specify severity)
• Metastases to bone, brain, liver, lung, lymph nodes
• Sepsis
• Urinary tract infection (specify site of infection such as bladder, kidney, or urethra)
Gastrointestinal Hemorrhage
• Document underlying cause:
–
–
–
–
–
–
Angiodysplasia
Diverticulitis
Diverticulosis
Duodenitis
Gastritis
Ulcer (duodenal, esophageal, gastric, gastrojejunal, peptic)
• Document etiology and show cause and effect
Example:
– Acute GI bleed due to bleeding esophageal varices
• If no active bleeding during endoscopic exam, clarify if
a condition (e.g., ulcer) is the likely cause of the bleed
• If multiple causes of GI hemorrhage, document all
causes
Gastrointestinal Ulcer
• Document all sites
–
–
–
–
–
Duodenal
Esophageal
Gastric
Gastrojejunal
Peptic
• Document associated complications, if appropriate:
– Hemorrhage
– Perforation
• Document acuity
– Acute
– Chronic
Barrett’s Esophagus & Barrett’s
Ulcer
• Barrett’s esophagus,
disease, syndrome
• Barrett’s ulcer
– Document presence of
bleeding
– Document presence of
dysplasia
• High grade dysplasia
• Low grade dysplasia
ICD-10
K22.10
Barrett’s ulcer without bleeding
K22.11
Barrett’s ulcer with bleeding
K22.70
Barrett’s esophagus without dysplasia
K22.710
Barrett’s esophagus with low grade
dysplasia
K22.711
Barrett’s esophagus with high grade
dysplasia
K22.719
Barrett’s esophagus with dysplasia,
unspecified
Hemorrhoids
• Document the degree/grade/stage of hemorrhoids:
• First degree
o Hemorrhoids (bleeding) without prolapse outside of anal canal
• Second degree
o Hemorrhoids (bleeding) that prolapse with straining, but retract
spontaneously
• Third degree
o Hemorrhoids (bleeding) that prolapse with straining and require manual
replacement back inside anal canal
• Fourth degree
o Hemorrhoids (bleeding) with prolapsed tissue that cannot be manually
replaced
• Document presence of any associated complications:
•
•
•
•
Prolapsed
Strangulated
Thrombosed
Ulcerated
Removal of Intestine
• Root operation:
• Excision (cutting out or off, without replacement, a portion of a body part)
• Resection (cutting out or off, without replacement, all of a body part)
• Body part: The anatomic site or body part removed (see next
slide)
• Approach: Open, percutaneous endoscopic, via natural or
artificial opening, via natural or artificial opening endoscopic
• Document body part, approach and if all the body part was
character 1
character 2
character 3
character 4
character 5
character 6
character 7
removed
Section
Body System
Root Operation
Body System
Approach
Device
Qualifier
0
Med & Surg
D
Gastrointestinal
System
T
K
0
Z
Z
Resection
Ascending Colon
Open
No Device
No Qualifier
Open Resection of Ascending Colon
0DTK0ZZ
Document specific gastrointestinal
body parts
•
•
•
•
•
•
•
•
•
•
•
•
•
Esophagus, upper
Esophagus, middle
Esophagus, lower
Esophagogastric junction
Esophagus
Stomach
Stomach, pylorus
Small intestine
Duodenum
Jejunum
Ileum
Ileocecal valve
Large intestine
•
•
•
•
•
•
•
•
•
•
•
•
•
Large intestine, right
Large intestine, left
Cecum
Appendix
Ascending colon
Transverse colon
Descending colon
Sigmoid colon
Rectum
Anus
Anal sphincter
Greater omentum
Lesser omentum
Case Study Pediatrics
• Newborn H&P: Premature infant born at 36 weeks 2 days at
2550 grams.
• Fever to 101;Possible sepsis.
• Receiving IV Gent & Ampicillin.
• Discharge summary: “At risk for sepsis”
Sample Case: Newborn
Before
After
:.
MS-DRG: 790
Relative weight: 5.0315
MS-DRG: 790
Relative weight: 5.0315
PDx: Single liveborn
PDx: Single liveborn
SDx: Prematurity
RDS
35-36 Gestation
NB feeding
problem
SDx:
Add:
Sepsis of newborn
Query for clarification
Procedure:
Procedure:
APR DRG:
SOI Level:
APR Weight:
ROM Level:
Exp. Mort Rate:
634
1
0.5761
1
0.3%
APR DRG:
SOI Level:
APR Weight:
ROM Level:
Exp. Mort Rate:
634
2
1.1003
2
3.2%
This report includes data produced by 3M’s
proprietary APR-DRG Software. All copyrights in and
to APR-DRG Classification System and all APR-DRG
Code Assignments are owned by 3M. All rights
reserved.
Fever Alternatives
Benign Lymphoreticulosis,
Cat Scratch Fever & Lyme
Disease
APR-DRG 724
0.5823
Bacterial
Meningitis
APR-DRG 049
0.9364
Viral Meningitis
APR-DRG 051
0.4921
Viral Diseases
Including Mumps,
Measles, & Viral
Syndrome
APR-DRG 723
0.3319
Chronic Leukemia
APR-DRG 691
0.9245
Febrile Seizure
APR-DRG 053
0.4741
Infections of Upper
Respiratory Tract Including
Croup, Otitis Media, Flu &
Tonsillitis
APR-DRG 113
0.2723
Organism
Specific/Complex
Pneumonia
APR-DRG 137
0.6469
FUO
APR-DRG 722
SOI = 0.3342
Acute
Leukemia
APR-DRG 690
1.0480
Neutropenic
Fever
APR-DRG 660
SOI = 0.6548
Bronchiolitis
APR-DRG 138
0.2932
UTI
APR-DRG 463
0.4007
Gastroenteritis
APR-DRG 249
0.3386
Lupus
APR-DRG 346
0.5823
Pneumonia
APR-DRG 139
0.3886
Newborn Documentation Issues
“R/O Sepsis”
Document if sepsis is either
• Confirmed
• Ruled out
• Treated and resolved
• Organism if known /suspected and link to sepsis
Newborn Documentation Issues
28 APR DRGs Related to Newborns
The following factors impact APR DRG assignment:
• Birthweight
– <500 grams
– 500-749 grams
– 750-999 grams
– 1000-1249 gram
– 1250-1499 grams
– 1500-1999 grams
– 2000-2499 grams
– >2499 grams
• Diagnoses:
– Congenital or perinatal
– Major cardiovascular
infection
procedure
– Major anomaly
– Major procedure
– Respiratory distress
syndrome
• Discharge Disposition:
– Other major
– Transfer to another
respiratory condition
acute care facility
– Other significant
condition
• Procedures:
– ECMO
Diagnoses that Impact Newborn APR DRGs
Major Respiratory Condition Examples:
• Aspiration of amniotic fluid, blood or
stomach contents with respiratory
symptoms
• Congenital pneumonia
• Meconium aspiration with respiratory
symptoms
• Persistent fetal circulation
• Pulmonary hypertension
• Respiratory distress syndrome
• Combination of certain respiratory
conditions with a different respiratory
condition or mechanical ventilation or
CPAP
Major Anomaly Examples:
• Congenital neutropenia
• Cystic fibrosis
• Diabetes insipidus
• DiGeorge syndrome
• Down’s syndrome
• Hemangioma
• Lung anomaly
• Macroglobulinemia
• Neurofibromatosis
• Panhypopituitarism
• Polycystic kidney disease
• Sickle cell
• Spina bifida
• Thrombocytopenia
• Valve disorders
• Wiskott-Aldrich syndrome
Diagnoses that DO NOT Impact Newborn APR DRGs
The presence or absence of the following diagnoses will not impact the
base APR DRG:
•
•
•
•
•
•
•
•
•
•
•
•
ABO/Rh incompatibilities
Atrial septal defect
Breast engorgement in newborn
Conjunctivitis and dacryocystitis
Facial nerve injury
Fetal alcohol syndrome
Fetal distress
Fractured clavicle
Hydrocele
Hyperthermia
Hypothermia
Petechiae
• Phrenic nerve paralysis
• Polycythemia
• Positive blood screen for drugs
without signs of withdrawal
• Respiratory distress in newborn
• Skull fracture
• Thrush
• Transient tachypnea of newborn
(TTN) (Type II RDS)
• Ventricular septal defect
Common Severity Drivers in Newborns
Newborn Conditions
• Apnea of newborn
• Atrial septal defect
• Congenital aortic stenosis
• Cyanosis of newborn
• Hyperbilirubinemia due to ABO
incompatibility
• Hypoglycemia
• Hypoxemia of newborn
• Jaundice in preterm infant
• Meconium staining
• Neonatal bradycardia
• Neonatal dehydration
• Patent foramen ovale
• Patent ductus arteriosus
• Respiratory distress in newborn
• Respiratory distress syndrome
• Transitory tachypnea of newborn
• Ventricular septal defect
Other Conditions Occurring in Newborns
• Hypoperfusion
• Heart failure
– Acute vs. chronic vs. unspecified
– Diastolic vs. systolic vs. combined
vs. unspecified
• Cardiomyopathy
– Dilated cardiomyopathy
– Hypertrophic cardiomyopathy, IHSS
– Restrictive cardiomyopathy
Parting Thoughts
• Thank you for your time
• Future opportunities
– Additional educational sessions
– Updating feedback loops for physicians
• Please email Anupam or Michelle with
comments, critiques or suggestions
165