Physical Assessment Class 3

Physical Assessment Class 3
Daily Tasks
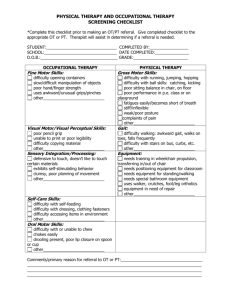
**Spot Test and assessment 1 (Class materials from1-2)**
Goals:
• Understand significant features of a neurological history
• Know the complete sequence of cranial nerve examinations , adding CN VII-XII in addition to last weeks material
• Understand the organizing principles of the neurologic examination: symmetry versus asymmetry and localization of findings to the central nervous system versus peripheral nervous system.
• Learn about examination of the motor system, including bulk, strength, tone and cerebellar function; rapid alternating movements; finger to nose (F-->N); Heel to Shin (H-->S) and features of various gait types.
• Wrap up general assessment of the Central Nervous system and
Cranial Nerves
CN VII: What it innervates
Testing CN VII
*CN VII Testing
Sensory: anterior 2/3 of tongue taste buds
Motor: facial expression muscles (smile showing teeth, raise eyebrows, scowl)
Parasymp: sublingual and submandibular salivary glands, lacrimal, nasal mucosa
CN VIII
*CN VIII Function
Cochlear Branch: hearing
1. Rub fingers on either side of head with patient’s eyes closed. Get a general feel of where and when the sound is heard
2. Rinne’s Test
3. Weber’s Test
Vestibular Branch: equilibrium testing
*CN VIII Testing
*CN VIII Testing
• Vestibular component is difficult to independently test, but can be tested using cold water flushing in ear canal
• Overall history and assessment of sensory system, cognitive function, cerebellar function can help lead to a diagnosis of vestibular pathology
CN IX: glossopharyngeal nerve
*CN IX
Sensory: posterior 1/3 of tongue; pharynx
Motor: pharyngeal muscles (swallowing), check with swallow and gag reflex (afferent component)
Parasymp: parotid salivary gland
CN IX and X
*CN X: Vagus Nerve
Sensory: from thoracic & abdominal viscera
(heart, lungs, GI tract)
Motor: pharynx (check gag reflex: motor component) & larynx (listen to speech)
Parasymp: HT, LU, abd organs
CN IX and X: Testing
*CN XI: Spinal Accessory/Accessory
Nerve
CN XI supplies motor and sensory control to the
Sternocleidomastoid & Trapezius muscles: Test muscle strength with active and resisted motions
CN XI: Spinal Accessory/Accessory
Nerve
CN XI
• tongue muscles
*CN XII:
CN XII: Hypoglossal Nerve
CN XII
*CN XII
• Test by having patient stick out tongue. Look for deviation to one side (side of weakness), fasciculations, atrophy
Spot test and Practice!
• Test each other on cranial nerves I-XII
• Perform task at Spot Test when I come around to you and your partner
*Review: CN VII-XII
CN VII: Check smile, frown, scowl, wink. Ask about lacrimation, salivation, taste
CN VIII: test hearing with finger rub, Rinne’s, and
Weber’s test. Ask about equilibrium
CN IX & X: Gag reflex, have patient swallow, ask about taste, listen to voice and look at soft palate deviation with “AH” sound
CN XI: Test SCM and Trapezius muscle strength
CN XII: Have patient protrude tongue and look for deviation
Understanding Upper and Lower
Motor Neuron Lesion Signs
• Injury to a neuron can be seen on physical exam with various signs which depend upon where the injury is located. If the injured neuron is an upper motor neuron it often has certain signs, just like a lower motor neuron injury has distinct characteristics.
• Review what an upper and lower motor neuron are…
*Understanding Upper and Lower
Motor Neuron Lesion Signs
• An upper motor neuron connects the primary motor cortex of the precentral gyrus of a cerebral hemisphere with a synaptic junction to a lower motor neuron cell body (often located )in the ventral horn of the spinal cord
• A lower motor neuron travel then from the ventral horn of the spinal cord, out the ventral root through the spinal nerve (to either ventral or dorsal rami) and then to a named nerve (ex: musculocutaneous nerve) to a specific group of now innervated muscles
(the musc. cutaneous nerve supplies the biceps brachii muscle))
*More about UMNL and LMNL
*Upper Motor Neuron Lesion (UMNL)
Signs
• Loss of distal extremity strength (ex: weakness in hands)
• Loss of distal extremity dexterity (poor hand control, dropping objects, etc.)
• A Babinski sign
• Increased muscle tone, either
– Spasticity (clasp knife-like weakness)
– Rigidity (feels like bending hard plastic…constant resistance through range of motion)
• Hyperreflexia( increased reflex muscle jerk reactions)
• “Clasp-knife phenomena”: giveaway weakness at the end range of a muscle test (like closing a swiss army knife)
Babinski Reflex
*Lower Motor Neuron Lesion (UMNL)
Signs
• Loss of muscle strength and tone
• Loss of reflexes due to denervation
• Muscle wasting and atrophy
• Denervation hypersensitivity noted by fasciculations (tiny, ongoing contractions of fascicles within a muscle)
*Other Motor System Exams
• Cerebrocerebellar Tests: These test cerebellar coordination with cerebrum
1) Finger-to-nose: have patient close their eyes and try to touch their index finger to their nose
2) Heel-to-shin: have patient with their eyes closed run their heel down their skin (superior to inferior)
3) Rapidly alternating movements: have patient flip both hands from supination to pronation and back again many times in rapid succession
*Other Motor System Exams
• Common abnormal Gaits
1) Neuropathic Gait Demonstration
2) Myopathic Gait Demonstration
3) Parkinsonian Gait Demonstration
• Neuropathic Gait Demonstration
This type of gait is most often seen in peripheral nerve disease where the distal lower extremity is most affected. Because the foot dorsiflexors are weak, the patient has a high stepping gait in an attempt to avoid dragging the toe on the ground.
• Myopathic Gait Demonstration
With muscular diseases, the proximal pelvic girdle muscles are usually the most weak.
Because of this the patient will not be able to stabilize the pelvis as they lift their leg to step forward, so the pelvis will tilt toward the nonweight bearing leg which results in a waddle type of gait.
• Parkinsonian Gait Demonstration
This type of gait is seen with rigidity and hypokinesia from basal ganglia disease. The patient's posture is stooped forward. Gait initiation is slow and steps are small and shuffling; turning is en bloc like a statue.
*Muscle Strength Nerve Root Levels
Biceps – C5-6
Brachioradialis – C5-6
Triceps – C7
Finger Flexors – C8
Finger abduction and thumb opposition-T1
L2 – Hip flexion
L3 – Knee extension
L4 – Knee flexion
L5 – Ankle dorsiflexon
S1 – Ankle plantar flexion
• The next slide is an interesting and helpful chart to help understand and examine a patient with weakness
Putting it together
• A patient that has a larger distribution of pain or neurological symptoms will have a more centralized lesion (closer to the spinal cord, in the spinal cord, or other CNS location). Also metabolic disorders can result in symmetrical loss/change in reflexes (ex: diabetes)
• Ex: compare a patient with numbness along the T1 dermatome verses a patient that has arm and leg numbness
Putting it together
• Similarly, if a patient has unilateral
(asymetrically) altered reflexes in the C5 & C6 levels, how is that different from a patient that has bilateral (symetrically) altered reflexes in the C5 & C6 levels?
• What if all reflexes are diminished?
• Muscle testing of all muscle levels will be reviewed in a later class
Epilepsy and other causes of convulsive activity
• Non-epileptic causes of seizure:
– Fever
– Drug reaction
– Hypoxia
– Hypoglycemia
Epilepsy and other causes of convulsive activity
• Know causes of epilepsy:
– Vascular (AV malformation, aneurysm)
– Tumor (glioblastoma)
– Head trauma (subdural hematoma)
– Metabolic (diabetes)
Review:
• Make sure that you understand the concepts of CN I-
XII and how to test these
• Understand the differences between UMNL and
LMNL, and be able to write or describe their associated findings
• Be able to test cerebrocerebellar function
• Recognize common gait abnormalities and their significance
• Understand common causes of seizure disorders
• Start to learn muscle testing nerve root levels