PHYSICAL THERAPY AND OCCUPATIONAL THERAPY
advertisement

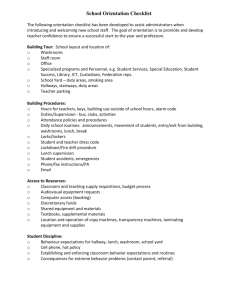
PHYSICAL THERAPY AND OCCUPATIONAL THERAPY SCREENING CHECKLIST *Complete this checklist prior to making an OT/PT referral. Give completed checklist to the appropriate OT or PT. Therapist will assist in determining if a referral is needed. STUDENT:_______________________________ COMPLETED BY:_________________ SCHOOL:________________________________ DATE COMPLETED:_______________ D.O.B.:__________________________________ GRADE:________________________ OCCUPATIONAL THERAPY PHYSICAL THERAPY Fine Motor Skills: Gross Motor Skills: Visual Motor/Visual Perceptual Skills: Gait: difficulty opening containers slow/difficult manipulation of objects poor hand/finger strength uses awkward/unusual grips/pinches other___________________________ poor pencil grip unable to print or poor legibility difficulty copying material other___________________________ Sensory Integration/Processing: defensive to touch, doesn’t like to touch certain materials exhibits self-stimulating behavior clumsy, poor planning of movement other___________________________ Self-Care Skills: difficulty with running, jumping, hopping difficulty with ball skills: catching, kicking poor sitting balance in chair, on floor poor performance in p.e. class or on playground fatigues easily/becomes short of breath stiff/inflexible weak/poor posture complaints of pain other___________________________ difficulty walking: awkward gait, walks on toes, falls frequently difficulty with stairs on bus, curbs, etc. other___________________________ Equipment: needs training in wheelchair propulsion, transferring in/out of chair needs positioning equipment for classroom needs equipment for standing/walking needs special bathroom equipment uses walker, crutches, foot/leg orthotics equipment in need of repair other___________________________ difficulty with self-feeding difficulty with dressing, clothing fasteners difficulty accessing items in environment other___________________________ Oral Motor Skills: difficulty with or unable to chew chokes easily drooling present, poor lip closure on spoon or cup other___________________________ Comments/primary reason for referral to OT or PT:____________________________________ _____________________________________________________________________________ _____________________________________________________________________________ _____________________________________________________________________________