Genetics Overview - Alport Syndrome Foundation

Alport Syndrome
Genetics and Diagnosis
Martin Gregory, MD, PhD
Professor of Medicine
University of Utah
Nothing to disclose
Modes of Inheritance
• X-linked (XLAS)
– COL4A5 on chromosome Xq22 85% of cases
• Autosomal
– COL4A3 or COL4A4 on chromosome 2q36-37
– Recessive (ARAS) 10-15% of cases
– Autosomal Dominant (ADAS) 1-5% of cases
• Diseases mimicking AS
– MYH9 disorders: Epstein and Fechtner syndromes
Giant Platelets in Fechtner Syndrome
Autosomal Dominant AS
• Rare, mild
• Vertical pattern of inheritance
• Male to male transmission
• Mutation in
COL4A3 or
COL4A4
Autosomal Recessive AS
• Uncommon
• Horizontal pattern of inheritance
• Consanguinity
• Mutations in
COL4A3 or
COL4A4
• Parents are
“carriers”: they have TBMN
• Most common
• Vertical pattern of inheritance
• NO male to male transmission
• Mutations in
COL4A5
X-linked AS
Implications of Inheritance Patterns
• Need to be as sure as possible of mode of inheritance before drawing conclusions or advising families.
• Prediction is treacherous, and genetic counseling subtle.
• Both the chance that children will inherit the disorder and the likely severity of the syndrome vary with the type of AS
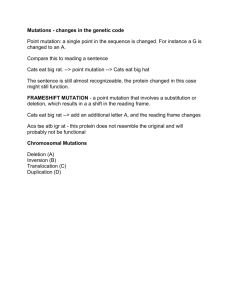
Time to onset of ESRD associates with COL4A5 mutation type
From the left of figure, Light weight solid line: large deletion, Dots: splice site mutation, Dash-Dot: small deletion, Heavy solid line: truncating mutation, Dash: missense mutation. Bekheirnia, M. R. et al. J Am Soc Nephrol 2010;21:876-883
Copyright ©2010 American Society of Nephrology
Relevance of Specific Mutations in XLAS
• Large deletions and truncations cause the most severe phenotype.
• Splice-site mutations: intermediate severity
• Missense mutations: relatively mild disease.
• In US, but not Europe, mutations in the
NC1 domain are more benign than those in the triple helical domain
Genetic Tests Available – COL4A5
• Sequencing and deletion analysis
– Expensive. Sensitivity > 80% for XLAS
• Targeted mutation analysis (Carrier detection)
– Cheap. Use this once family’s mutation is known.
• Test for 3 common “ Adult types ”
– Cheap. Use if family has one of these 3 mutations.
– ?use for screening certain groups
• Adults with dysmorphic hematuria and CKD.
• Alport syndrome with late-onset renal failure
“ Adult-type ” Mutations in the USA – Known gene carriers
COL4A5 mutation
L1649R
C1564S
R1677Q
G1170S c.2476delC
44
G1234X 42
16 others
Total
32
50
38
ESRD age in males
39
Male Female Total % of total
150
52
19
13
222
81
38
11
372
133
57
24
48.6
17.4
7.5
3.1
11
7
12
16
23
23
3.0
3.0
70 63 133 17.4
322 443 765 100
Pont-Kingdon G et al. BMC Nephrology 2009; 10:38
Genetic Tests Available – COL4A3/4
• COL4A3 and COL4A4 sequencing and deletion analysis
– Expensive. Sensitivity >80%
• Use after COL4A5 mutation excluded or if inheritance suggests autosomal transmission
• Can use to diagnose ~40% of cases of TBMN
Before Genetic Testing
•Gather a complete family history, patient history, u/a.
•Make your best guess for mode of inheritance
•Is a mutation known in the family?
•Is genetic testing appropriate?
•Families making reproductive decisions
•To avoid kidney biopsy, or if diagnostic certainly is desired
Choice of an Appropriate Genetic Test
•Targeted analysis or Adult-type 3 mutation test if the mutation is known in the family
•If no mutation is known, usually start with sequencing, including deletion analysis in females
•May start with Adult-type 3 mutation test in families with renal failure in middle age
•COL4A3/4 sequencing if autosomal disease likely or if COL4A5 testing was negative
Now you Tell me …
A lab test has 90% sensitivity and
99% specificity. The disease it tests for occurs in 1 in 50,000 people. A person in the population has a positive test. What is the likelihood that he has the disease tested for?
99%
90%
50%
10%
<1%
Now you Tell me …
Of people with the
A lab test has 90% sensitivity and
99% specificity. The disease it tests for occurs in 1 in 50,000 people. A person in the population has a positive test. What is the likelihood that he has the disease tested for?
disease 90% will have a positive test
Of people without the disease, 1% will have a positive test
99%
90%
50%
10%
<1%
Now you Tell me …
A lab test has 90% sensitivity and
99% specificity. The disease it tests for occurs in 1 in 50,000 people. A person in the population has a positive test. What is the likelihood that he has the disease tested for?
Test 100,000 people
1.8 true positives
99%
90%
50%
10%
<1%
Now you Tell me …
A lab test has 90% sensitivity and
99% specificity. The disease it tests for occurs in 1 in 50,000 people. A person in the population has a positive test. What is the likelihood that he has the disease tested for?
Test 100,000 people
1.8 true positives
1,000 false positives
Probability of disease
2/1002 = 0.2%
99%
90%
50%
10%
<1%
Now you Tell me …
A lab test has 90% sensitivity and
99% specificity. The disease it tests for occurs in 1 in 50,000 people. A person in the population has a positive test. What is the likelihood that he has the disease tested for?
Test 100,000 people
1.8 true positives
1,000 false positives
Probability of disease
2/1002 =
0.2%
99%
90%
50%
10%
<1%
A priori probability A posteriori
Now you Tell me …
A lab test has 90% sensitivity and
99% specificity. The disease it tests for occurs in 1 in 50,000 people. A person in the population has a positive test. What is the likelihood that he has the disease tested for?
Test 100,000 people
1.8 true positives
1,000 false positives
Probability of disease
2/1002 = 0.2%
99%
90%
50%
10%
<1%
A priori probability A posteriori if test is
+
0.002%
50%
98%
0.2%
98%
99.998%
Conclusions about Genetic Testing
•If a family has several males with ESRD, genetic testing will likely not improve prognostic accuracy.
•If the family is very small, the phenotype is likely severe.
•Before giving advice that may affect reproductive decisions, consider getting a genetic diagnosis for the prospective parent(s) involved (not just a diagnosis in the family).
•Only get a genetic diagnosis if it can change what you will do.
•Even very good tests may be misleading if misapplied