LIPOchip® experience
advertisement

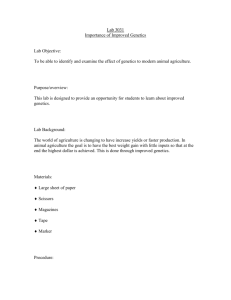
Bristol Genetics Laboratory Familial Hypercholesterolaemia: LIPOchip® experience Laura Yarram Bristol Genetics Laboratory Bristol Genetics Laboratory What is FH? Autosomal Dominant 1/500 heterozygotes in UK ○ (1/1,000,000 compound heterozygotes) Caused by LDLR, APOB & PCSK9 mutations Raised cholesterol, Xanthomas/Xanthelasma, Risk of CVD Simon Broome Criteria ‘definite’ or ‘possible’ ‘Normal’ life expectancy on statin treatment NICE guidelines Image 1. Achilles tendon xanthoma Definite Total cholesterol >7.5 mmol/L Tendon xanthomas Possible Total cholesterol >7.5 mmol/L Family history of myocardial Image 2. Xanthelasma (Image from Pietroleonardo st 2009) infarction <age 60 in 1& Ruzicka, degree relative Bristol Genetics Laboratory Why Perform Genetic Testing? Patient A, aged 8 LDLR mutation confirmed in family Equivocal cholesterol – 5.6mmol/L (FH >6.7mmol/L in children, ‘Normal’ <4.0mmol/L) Family history of extensive cardiovascular disease Great uncle – Myocardial infarction at aged 31 Patient A – mutation identified Will start statin treatment at ~ age 10 Early treatment gives the maximum health benefit More likely to adhere to treatment Bristol Genetics Laboratory Why Perform Genetic Testing? Patient B, aged 55 Pre-treatment cholesterol ~20mmol/L (FH >7.5mmol/L in adult) Unexpected compound heterozygote for two unclassified variants - c.[1766delA] + [932A>C] - p.[Asp589fs] + [Lys311Thr] Pedigree: Instigated further cardiology investigations p.[=] Exercise + [=] ECG positivep.[Asp589fs] + [Lys311Thr] Genetic diagnosis allows consideration of LDL apheresis p.[Asp589fs] + [=] Bristol Genetics Laboratory Current Testing Method +ve ARMS – 20 common mutations Mutation confirmation Sequencing Sequencing REPORT +ve REPORT CASCADE •Validated on known positive control samples• MLPA (MRC-Holland: -ve • Tested 104 samples date P062B)tovalidated using REPORT Offer 4 reported samples, sequencing/ obtained from a MLPA Norwegian lab -ve Proceed to MLPA • Primers designed for all 18 LDLR +ve -ve exons + promoter • Sequenced in 17 fragments REPORT • REPORT Validated using 4 known positives Bristol Genetics Laboratory Simon Broome Audit Data Simon Broome Criteria dFH pFH Unclassified No. Patients Tested 15 53 17 No. +ve Criteria not met 19 4 (21%) Total Diagnostic 104 48 (46%) Cascade 27 15 (56%) 15 (100%) 23 (43%) 6 (35%) Bristol Genetics Laboratory Results to Date 34 pathogenic variants detected to date + 2 variants ‘likely non-pathogenic’ - c.2390-16G>A and c.969C>T (p.[=]) cDNA Protein Diagnostic c.10580G>A p.Arg3527Gln (APOB) 9 (19%) c.1436T>C p.Leu479Pro 4 (8%) c.313+1G>A N/A 3 (6%) c.1640T>C p.Leu547Pro 2 (4%) c.662A>G p.Asp221Gly 2 (4%) c.1049G>C p.Arg350Pro 2 (4%) Commonly detected mutations in SW diagnostic patients (n=48) 28 of these variants required UV studies (Nb. Most were previously reported to database but with no functional/family studies) Bristol Genetics Laboratory Assay Sensitivity Assay Sensitivity (n=48) ARMS FH20 52% Bi-directional sequencing of LDLR (Promoter + 18 exons) 46% MLPA (P062B-C1) 2% Testing strategy not sustainable for disease frequency Bristol Genetics Laboratory LIPOchip® Background LIPOchip® has been in development since 2002 to detect the most prevalent Spanish mutations Current Version (8) includes ‘European’ specific mutations More than 100 hospitals are using LIPOchip® throughout Europe Copy number changes also detected Specific ‘BritChip’ due to be released June/July 2010 Validation – 40 samples used (36 previously tested, 4 new cases) Blind test All results concordant Bristol Genetics Laboratory LIPOchip® Processing 0 Extraction 1 Amplification PCR mixes 1, 2, 3 and 4 2 hours 2 hours 2 Fragmentation DNAse + Alkaline Phosphatase 3 Labelling TdT + Biotin-ddUTP 45 minutes 60 minutes 4 Hybridization Tecan 4800 HS Pro 3hours and 30 minutes OVERLAPPING PROCESSES DAY 1 DAY 2 5 Results analysis Bristol Genetics Laboratory Mutations Detected c.429C>A, p.Cys143X c.1432G>A, p.Gly478Arg Mutations not present in FH20 ARMS Bristol Genetics Laboratory c.2093G>A (p.Cys698Tyr) Patient has c.2093G>T (p.Cys698Phe) Slight displacement from the ‘Normal’ group Bristol Genetics Laboratory Del ex7-3’UTR Bristol Genetics Laboratory Duplication LDLR Exon 17 MLPA result LIPOchip result Long-range PCR confirmation Ex16_F 16 Ex18_R 17 3.5kb 18 ~5kb 3.5kb N dup 17 N Bristol Genetics Laboratory LIPOchip® Trial Results Point mutation analysis is robust Copy number detection results not always reportable ○ MLPA will still be required in a significant proportion of cases Assay Sensitivity (%) (n=48) Pick up (% of all diagnostic cases) (n=104) ARMS (20 common mutations) 52 24 Current LIPOchip (251 mutations) 58 27 British LIPOchip (Personal Communication) 77 36 Bristol Genetics Laboratory Proposed Method of Testing Initial screen using LIPOchip® platform Current European chip v.8 detects 251 mutations + copy number changes British LIPOchip predicted to detect 80% of UK mutations Followed by full bi-directional sequencing of LDLR (and MLPA where necessary) Negative patients meeting Simon Broome criteria Full PCSK9 screen by bi-directional sequencing (Validation near completion, 12 fragments) Sequencing of APOB hotspot regions (exon 26 and 29) Bristol Genetics Laboratory Conclusion Comprehensive testing service for FH implemented 131 cases tested overall, 48% mutation positive LIPOchip® evaluated – further work required to validate British version on release Network links with lipid and cardiac specialists have been established across the SW region Mechanism for robust funding is yet to be established Bristol Genetics Laboratory Acknowledgments Bristol Genetics Lab Maggie Williams Sarah Burton-Jones Thalia Antoniadi Genetic Technologists – Teresa Tovey, Jenny Coles, Gemma Dennis, William Cross and Matthew Garner Extraction Lab team and Array team Biochemistry Department, BRI Graham Bayly Mathangi Balasubramani Bath, Weston-super-Mare and Gloucester Biochemistry teams GOS Lab Alison Taylor Progenika Xabier Abad Maximilliano Crosetti Gen-probe (Tepnel diagnostics) MRC-Holland