Housekeeping/Intro/Overview - University of Michigan School of

Are We Heading For a Train Wreck?:
The US Health Care System in 2007
Richard Lichtenstein Ph.D, MPH
Department of Health Management and Policy
School of Public Health
University of Michigan
“The problem of providing satisfactory medical care to all the people of the
United States at costs which they can meet is a pressing one. At the present time, many persons do not receive service which is adequate either in quantity or quality, and the costs of service are inequitably distributed.
The result is a tremendous amount of preventable physical pain and mental waste. Furthermore, these conditions are…largely unnecessary. The United
States has the economic resources, the organizing ability and the technical experience to solve this problem.”
Source: Committee on the Costs of
Medical Care. Medical Care for the
American People: The Final Report of the Committee on the Costs of Medical
Care.
Chicago: The University of
Chicago Press. October 31, 1932
The nation’s health care system is a “tangled, highly fragmented web that often wastes resources by providing unnecessary services and duplicating efforts, leaving unaccountable gaps in care and failing to build on the strength of all health professionals.”
The Institute of Medicine, Crossing the Quality Chasm. 2001
World Health Organization (WHO)
Definition of Health
“Health is a state of complete physical, mental, and social well-being and not merely the absence of disease or infirmity.”
The Traditional Health Care
System in the US Has Had
Several “Fatal” Flaws
• System of Financing Care
(Fee-for-service system; fragmented payments)
• Organization of Services
“A Paradox of Excess and Deprivation”*
• Insurance Coverage of the Population
Health coverage is not a right in America
*
Enthoven and Kronick , NEJM 320:29-37. 1989
PROBLEMS WE FACE AS A
RESULT:
• COSTS
• ACCESS TO COVERAGE AND CARE
• QUALITY AND ACCOUNTABILITY
• RACIAL AND ECONOMIC
DISPARITIES in HEALTH AND CARE
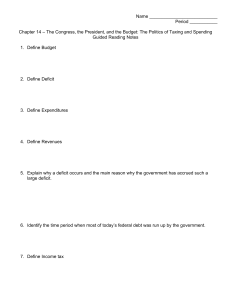
Health Care Costs: Magnitude of Growth
Both total and per capita spending on health have skyrocketed.
$2,500
$2,000
$1,500
$1,000
$500
$0
U.S. Total and Per Capita Expenditures on
Health Care, 1965-2005
$1.988 Trillion
$6,697
$172
$8,000
$7,000
$6,000
$5,000
$4,000
$3,000
$2,000
$1,000
$-
$35 Billion 1965 1975 1985 1994 1996 1998 2000 2002 2004
Total (billions) Per Capita
9
Source: Health, United States, 2001, Table 114; Health Affairs, National Health Spending in 2005, Jan-Feb. 2007.
!/28/07
General Motors
Health Care Costs
• $5.4 billion in health spending in ’05
– $1.4 billion in 2002 for prescription drugs
(31% of healthcare costs)
– $1,500 per vehicle
• 3.1 retirees/active worker, compared to Toyota with .02 retirees/active worker
Source: Detroit News February 10, 2005 and March 11, 2004 and NYTimes.com May 19, 2006
General Motors
Health Care Costs
• In October, 2005, GM and the UAW negotiated to increase costs of care to retirees. Active workers now contribute
$1/hour for retiree health care.
• Unfunded liability of $85 billion (in 2006 dollars) for future health care costs for workers and retirees.
Source: Detroit News February 10, 2005 and March 11, 2004 and NYTimes.com May 19, 2006
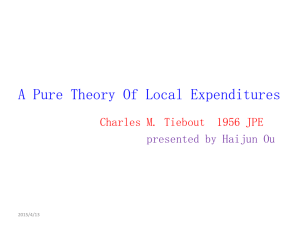
Health Care Costs: Impact on the Public Sector
Health care is consuming an increasing percentage of public budgets.
30%
25%
20%
15%
10%
5%
0%
Government Health Expenditures as a Percent of Total
Government Expenditures: Selected Years, 1960-2004
Michigan spent 25% of its budget on health in 2003
New York
State spent over 45% of its budget on
Medicaid in 2004-
2005.
Federal Health Expenditures State and Local Health Expenditures
13
Source: Health, United States, 2006, Table 120
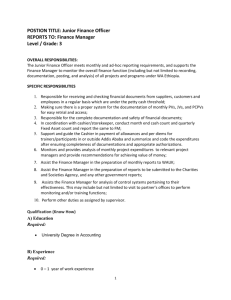
Medicare Expenditures and Non-Interest Income by Source as a Percent of GDP -2007
Source: Status of the Social Security and Medicare Programs. A SUMMARY OF THE 2007 ANNUAL REPORTS http://www.ssa.gov/OACT/TRSUM/trsummary.html
), 2007
Spending on Medicare Drug Benefit
• Between 2006-2015 expenditures for the
Medicare Drug Benefit estimated $724 bill.
• One-time increased expenditures 2005-2006 of 27.8% due to addition of benefit
• Projected growth in Medicare expenditures on drugs of 7.3% annually between 2006-
2014
Source: Kaiser Family Foundation Fact Sheet, April 2005 using data from CMS/Office of the Actuary
ACCESS TO CARE: The Uninsured
19.0%
18.0%
17.0%
16.0%
15.0%
14.0%
13.0%
12.0%
Percent of Non-Elderly Population Without Health
Insurance Coverage, 1987-2005 Americans without health insurance increased by 1.4 million in 2003.
*2005: 44.8 million Americans were uninsured
Source: US Census Bureau, Historical Health Insurance Tables, http://www.census.gov/ (accessed May, 14, 2007)
In 2007, the US Census Bureau revised downwards the figures for 2004-05 (methodological issue) . 2003 data not revised.
The wording of CPS questions implies that these estimates represent the number uninsured for the entire calendar year. However, estimates. Some of the dip observed in 1999 and later years reflects the addition of a verification question that reduced the number uninsured for calendars years 1999 and later.
Quality is Uneven
Americans Received
Recommended health care only 54.9% of the time!
McGlynn, EA, Asch, SM, Adams,J, et al. (2003) ”The Quality of health care delivered to adults in the United States.” NEJM 348:2635-45
How good is American health care?
Based on an extensive literature review performed at RAND in 1998:
• Only 50% of Americans receive recommended preventive care
• Patients with acute illness:
70% received recommended treatments
30% received contraindicated treatments
• Patients with chronic illness:
60% received recommended treatments
20% received contraindicated treatments
Schuster MA, McGlynn EA, Brook RH. How good is the quality of healthcare in the United
States? Milbank Quarterly 1998; 76(4):517-63 (Dec).
Hospital Safety and Medical Errors
Leapfrog Group Hospital Safety Measures
• Evidence-Based Hospital Referral (EHR)
• Computer Physician Order Entry (CPOE)
• ICU Physician Staffing (IPS) “Intensivists”
Leapfrog has added over 20 other safety measures since beginning with these
Racial and Economic Disparities
30
20
10
0
40
Infant Mortality Rates by Race*
United States, 1970-2003
All races White Black
Source: Health, United States, 2006, Table 22
*Race of mother
Years of Potential Life Lost due to Diabetes Mellitus, by race and Hispanic Origin, 2003
White Black
Am. Indian or Alaskan Asian/Pacific Islander
Hispanic
400
300
200
100
0
Source: Health, United States, 2006, Table 30
* Age-adjusted years lost before age
75 per 100,000 population under 75 years of age.
What would be the characteristics of a well-designed system?
(At least, this was what we thought for several years!)
IOM Aims for the 21st Century
Health Care System
• Safe
• Effective
• Patient-centered
• Timely
• Efficient
• Equitable
Source: IOM, Crossing the Quality Chasm, 2001, p. 5-6
1. Coverage
• We need universal coverage to make the system work.
– “There will be no universal coverage unless it is mandated by the Government.” (Lichtenstein)
– “You can’t have universal coverage without a police state” (Newt Gingrich)
2. Financing
• Link the population to providers and hold the providers accountable for costs and quality.
• Rely primarily on prepaid, capitated payments.
• Single payment integrates physician and
“facilities.”
3. Services
• Match level and type of services to needs of the populationEpidemiologically-based planning.
• Focus on primary care and prevention.
• Create a hierarchy of services.
• Concentrate high cost/low incidence procedures in regional centers.
4. Cost Containment
• Reduce unnecessary care --hospital days, procedures, lab tests, etc.
• Less duplication of costly technology.
• More reliance on primary care providers; less on sub-specialists.
• Cost-effective prevention.
• Lower administrative costs.
5. Quality and Accountability
Systems should be held Accountable for Quality and Cost, They should:
• Promote clinical effectiveness research.
• Only use effective procedures, therapies, tests, etc.
(Evidence-Based Medicine)
• Use clinical “guidelines,” “clinical pathways,” etc.
• Reduce errors
• Increase Patient Centeredness
• Follow ideals of TQM, CQI, Six Sigma, LEAN
Reporting Systems such as
HEDIS Can Be Used to Evaluate
Hospitals and Health Plans
• Patient Satisfaction
• Quality of Care
• Costs
• Access
• Population Health Status
From the late 1980s through the early 1990s, a “Revolution” in the
Organization of the Delivery System
Occurred --
But it happened through market mechanisms , not government intervention (i.e. The Clinton Health
Plan)
Physicians
There Was a Shift in the
Health Care Paradigm
Solo Practice
Group Practice or
Employed
Hospitals
Free-standing, community
Networks & Integrated
Delivery Systems
Insurance
Indemnity Managed Care
Purchasers
Passive
Source: J. Billi, MD, U of M
“Prudent Purchaser” as Proactive Partner
Change in Physician Roles
Traditional:
• Self-employed
• Solo practice
• Single specialty groups
• Fee-for-service reimbursement for care of individual patients
• No “gate keeping”
• Autonomy
Managed Care Era:
• Employed
• Group practice
• Multi-specialty groups
• Capitated for care of a population
• Primary care physician gatekeeper
• Accountability
Source: J. Billi, M.D., U of M
The Paradigm Shift was Closely
Associated with the Movement to
Managed Care and Integrated
Delivery Systems
*BUT,* Since the late 1990s, the paradigm has shifted again!--Away from tightly managed care and toward a modified fee-for-service system.
.
ACCESS TO CARE: Enrollment in Various Types of
Employment-Based Health Insurance
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
(1)
1988 1993 1996 1999 2002 2005
Conventional
PPO
HMO
POS
Source: American Hospitals Association, TrendWatch ChartBook, 2006 ( http://www.aha.org/aha/research-and-
36 trends/health-and-hospital-trends/2006.html
, accessed May 28, 2007)
The Decline of the Hospital
The Hospital is no Longer the
“Center of the Health Care
Universe.”
It is Now Becoming One of the
Pieces of an Integrated Delivery
System.
Since 1981, there has been an incredible decrease in the use of inpatient care
• Decline of 80 million patient days per year
– Financial Incentives (e.g. managed care)
– New Technology (e.g. Laparoscopy, new Rxs)
– Early Ambulation
• More hospital-based surgery is performed on an outpatient basis than inpatient
Major Trends in the Hospital
Sector during the late 80’s and
90’s:
Mergers
Acquisitions
Downsizing
Re-engineering
Integration
System Formation
Managed Care
Many of these trends have stopped or even reversed!
• System “divorces” (Stanford and UCSF)
• Virtual Integration
• Physician Practice Management Groups have collapsed
Trends in Private Sector Health
Care Financing
• Shift of cost of care to employees
– Higher share of premiums
– Premiums for dependents
– Higher Co-pays and Deductibles (e.g. for hospital)
• Consumer–Directed Health Plans
– Health Savings Accounts,
– Defined Contribution Plans
• Avoidance of Employee Coverage (Walmart)
– Contractors
– Part-time employees
OTHER MAJOR ISSUES
• The Future of Medicare
– Unsustainable Growth in Costs
• Medicaid, SCHIP and the Uninsured
– Will we ever cover the whole population?
• Physician Workforce Issues
– Will we have a physician surplus or a shortage?
• Nursing Shortage
–
How can we train more American Nurses?
• **How will we afford the costs of new technology?**
The solutions to these problems are complex:
Beware of anyone who says they know a simple solution to our health care dilemma!