Cultural Diversity and Behavioral Research
advertisement

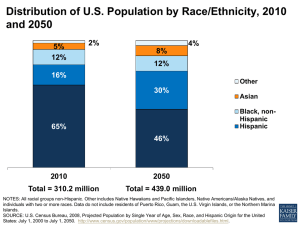
Nelda Mier, Ph.D. Assistant Professor School of Rural Public Health Social and Behavioral Health Department South Texas Center The U.S. Census Bureau uses 5 race categories: American Indian and Alaska Native Asian Black or African American White Native Hawaiian and Other Pacific Islander Race and Hispanic origin are separate and distinct concepts. Hispanic" or "Latino" are those who classify themselves as: Mexican Puerto Rican Cuban “Other Spanish, Hispanic, or Latino." U.S. Bureau Census: Origin can be considered as the heritage, nationality group, lineage, or country of birth of the person or the person’s parents or ancestors before their arrival in the United States. People who identify their origin as "Spanish," "Hispanic," or "Latino" may be of any race. In 2000, the total population: 281,421,906. 98% of the population reported only one race, with a majority reporting to be White. BY 2050…. White 69% 50% 81% 72% Black Asian 24% 3% 15% 13% 4% 13% 8% 5% U.S. Bureau Census Hispanic or Latino All other races White alone, not Hispanic More than 1 in 8 people are Hispanic 2 in 5 Hispanics are foreign born The Hispanic population became the largest minority group by increasing 67% --22.4 million in 1990 to 37.4 million in 2002, excluding Puerto Rico and other islands U.S. Bureau Census 2000 U.S. Bureau Census 2000; Total population: 11 million % of the Population that are White alone (2006) % of the Population that are Black alone (2006) % of the Population that are Asian alone (2006) % of the Population that are American Indian and Alaska Native alone (2006) % of the Population that are Native Hawaiian and other Pacific Islander alone (2006) HOW MUCH DIVERSITY TO YOU SEE AROUND? Minorities experience a disproportionate burden of preventable disease, death, and disability compared with non-Hispanic Whites Williams DR, Collins C. U.S. socioeconomic and racial differences in health. In: LaVeist TA, editor. A public health reader. Race, ethnicity, and health. San Francisco, CA: Jossey-Bass; 2002. p. 391-431. Asthma mortality Rate (per million; northeast U.S. 1993-1995) Hispanics/Latinos whites 34 15.1 HIV/AIDS mortality rate per 100,000 (1999) Puerto Ricans living on the U.S. mainland 32.7 non-Hispanic whites 2.4 national average 5.4 Adult immunization, 65+ years (2002) Influenza vaccination Hispanics/Latinos 46.7% whites 70.2% Millard AV, Graham MA, Mier N, Flores I, Carrillo-Zuniga G, & Sánchez ER. Addressing Health Disparities: The Hispanic Perspective. In S. Kosoko-Lasaki, R.L. O'Brien & C.T. Cook [Eds.]. Promoting Cultural Proficiency in Eliminating Health Disparities. Boston: Jones & Bartlett Publishers. (In Press.) Cancer of the cervix (2000) Hispanic incidence higher than that of nonHispanic whites by: Cancer of the stomach (2000) Males: Hispanic incidence higher by: Females: Hispanic incidence higher by: 152% 63% 150% Overweight among Hispanics 20 to 74 years of age Males: Hispanic incidence higher than in nonHispanic whites by: Females: Hispanic incidence higher by: Obesity, 20 to 74 years of age Males: Hispanic incidence higher by: Females: Hispanic incidence higher by: 11% 26% 7% 32% Millard AV, Graham MA, Mier N, Flores I, Carrillo-Zuniga G, & Sánchez ER. Addressing Health Disparities: The Hispanic Perspective. In S. Kosoko-Lasaki, R.L. O'Brien & C.T. Cook [Eds.]. Promoting Cultural Proficiency in Eliminating Health Disparities. Boston: Jones & Bartlett Publishers. (In Press.) CDC, 2005 168% 128% 41% Diabetes 62% 28% Stroke Chronic liver disease HIV Homicide Millard AV, Graham MA, Mier N, Flores I, Carrillo-Zuniga G, & Sánchez ER. Addressing Health Disparities: The Hispanic Perspective. In S. Kosoko-Lasaki, R.L. O'Brien & C.T. Cook [Eds.]. Promoting Cultural Proficiency in Eliminating Health Disparities. Boston: Jones & Bartlett Publishers. (In Press.) Hispanics whites Those under the age of 65 years with health insurance 66% 87% Those with a regular source of ongoing health care 77% 90% 73% 78% Vaccinations Children aged 19-35 months who are fully vaccinated (2002) Millard AV, Graham MA, Mier N, Flores I, Carrillo-Zuniga G, & Sánchez ER. Addressing Health Disparities: The Hispanic Perspective. In S. Kosoko-Lasaki, R.L. O'Brien & C.T. Cook [Eds.]. Promoting Cultural Proficiency in Eliminating Health Disparities. Boston: Jones & Bartlett Publishers. (In Press.) Why is important to understand cultural diversity and eliminate health disparities? For health professionals, there is an ethical and moral dilemma that must be addressed. Their ethical standards demand fairness and compassion. Healthcare is a resource that is associated to social justice, opportunity, and quality of life. Health status is linked to productivity. Institute of Medicine, 2002 From the perspective of public health, racial and ethnic disparities threaten efforts to improve the nation’s health. Racial and ethnic disparities in healthcare pose a significant dilemma to a society that is still dealing with a legacy of racial discrimination. Institute of Medicine, 2002 Studies examining disparities Studies implementing culturally sensitive interventions Race, ethnicity, and cultural are consistently used interchangeably in health promotion research, even though they are not synonymous terms. Integrated patterns of human behavior that include: language, thoughts, communications, actions, customs, beliefs, values and institutions of racial, ethnic, religious or social groups” (16) Unique shared values, beliefs, and practices that are: - Directly associated with a health-related behavior - Indirectly associated with that behavior - Influencing acceptance and adoption of the health education message or activity. (15) 15.Pasick RJ DOC, Otero-Sabogal, R. Similarities and differences Across Cultures: Questions to Inform a Third Generation for Health Promotion Research. Health Education Quarterly 1996;23(Suppl):S142-S161. 16.Assuring cultural competence in health care: Recommendations for national standards and outcomes-focused research agenda. In: Health USDoHaHSOoM, editor.: Washington, DC: U.S. Government Printing Office; 2000. Race, ethnicity, language, nationality, and even geographic location are most commonly used as proxies for culture. African Americans have a perception that “eating healthy” means giving up part of their cultural heritage and trying to conform to the dominant culture Compared with White women, African American women are more satisfied with their weight and, if overweight, are more likely to feel attractive .(18) .(19) 18. James DC. Factors influencing food choices, dietary intake, and nutrition-related attitudes among African Americans: application of a culturally sensitive model. Ethnicity & health 2004;9(4):349-67. 19. Eyler AA, Matson-Koffman D, Vest JR, Evenson KR, Sanderson B, Thompson JL, et al. Environmental, policy, and cultural factors related to physical activity in a diverse sample of women: The Women's Cardiovascular Health Network Project--summary and discussion. Women & health 2002;36(2):123-34. Another study found that Latina women believe that sports are for men and that family and children come before personal needs (such as being physically active). Other studies found that Hispanics believe that diabetes is caused by emotional trauma (20) .(21) 20. Evenson KR, Sarmiento OL, Macon ML, Tawney KW, Ammerman AS. Environmental, policy, and cultural factors related to physical activity among Latina immigrants. Women & health 2002;36(2):43-57. 21. Arcury TA, Skelly AH, Gesler WM, Dougherty MC. Diabetes meanings among those without diabetes: explanatory models of immigrant Latinos in rural North Carolina. Soc Sci Med 2004;59(11):2183-93. Studies examining disparities Studies implementing culturally sensitive interventions The extent to which ethnic or cultural characteristics, experiences, norms, values, behavior patterns, and beliefs of a target population, and relevant historical, environmental, and social forces are incorporated in the design, delivery, and evaluation of targeted health interventions. Resnicow K, Braithwaite RL, Dilorio C, Glanz K. Applying theory to culturally diverse and unique populations. In: Glanz K, Rimer BK, Lewis FM, editors. Health behavior and health education: theory, research, and practice. 3rd ed. San Francisco, CA: Joseey-Bass; 2002. p. 485-509. Cultural Competence Multicultural Culturally appropriate, relevant, congruent, specific. Targeting denotes a process of identifying a population subgroup for the purpose of insuring exposure to the intervention by that group. E.g. targeting an ethnic group. Tailoring implies adapting the intervention to best fit the needs and characteristics of a target population. Cultural tailoring is the development of interventions, strategies, messages, and materials to conform with specific cultural characteristics (15) .(15) Innovate? Adopt an evidencebased program? Literature review of RCTs testing nutrition and exercise interventions tailored for Hispanics Principles and components of these interventions. Mier N, Ory MG, Medina AA. Anatomy of Culturally Sensitive Interventions Promoting Nutrition and Exercise in Hispanics: A Critical Examination of Existing Literature Submitted to Health Promotion Practice. In review. (1) described an intervention that was tailored for Hispanics; (2) the intervention aimed at modifying knowledge, beliefs, or behavior related to nutrition or exercise; (3) the intervention was tailored for Hispanics of any age group; (4) the study was based on the randomized controlled trial research design; (5) the study was published in a peer review journal, (6) the study was conducted in the United States; and (7) the study was published between 1990 and 2006. 71% 29% Yes No 45% 40% 35% 30% 25% 20% 15% 10% 5% 0% 25% 20% 15% 10% 5% 0% 59% 41% 6% Yes No Measured effects 53% 47% Yes No Other, 7% Mexican American, 29% Latino, 35% Hispanic, 29% Group-settings 24% Community health workers 24% Ethnic foods 29% Back-translation technique 31% Bilingual materials and delivery agents 77% Family-based 29% 47% 29% 35% Literacy Social support Hispanic values Not much detail Settings: Community agencies Churches Schools Media Theory-driven, yes. But… 1st Determine a specific health issue for which an intervention is needed 2nd Identify the theories from a socioecological perspective and select the most appropriate one for understanding causal factors and processes of specific health-behaviors 3rd Determine potential points of interventions suggested by the selected theory or framework 4th Consider the collective wisdom on what interventions work with what populations under what conditions PRECEED-PROCEED model http://www.lgreen.net/precede.htm Influenced by the health belief model, theory of reasoned action, and PRECEEDPROCEED model Culture is the core of health promotion and disease prevention programs Used to assess cultural eating patterns and to develop AIDS prevention programs .(18) (Airhihenbuwa 1995); 18. James DC. Factors influencing food choices, dietary intake, and nutrition-related attitudes among African Americans: application of a culturally sensitive model. Ethnicity & health 2004;9(4):349-67. PEN-3 MODEL RELATIONSHIPS & EXPECTATIONS CULTURAL EMPOWERMENT Positive Existential Negative Perceptions Enablers Nurturers Person Extended Family Neighborhood CULTURAL IDENTITY Acknowledges the role of social and cultural influences in health behavior Emphasizes the transactions between individual and the environment at different levels: individual, family, community, environment. It uses a consumer orientation, audience analysis and segmentation, and aspects of exchange theory. Reaim.org It emphasizes the idea that communities themselves can achieve social and behavioral outcomes and that social forces influence behaviors. Formative research plays an important role in the design and implementation of an intervention for Hispanics. Health assessments, focus group discussions, literature searches, and interviews are tools for tailoring an intervention by identifying attitudes, beliefs, language use, and other opinions of the priority population in relation to specific health issues or behaviors The diversity of the Hispanic population must be acknowledged in intervention design Consider immigration and contextual factors in intervention design Consider acculturation, but also understand that it is a complex phenomenon and more research is needed to better assess its impact on health outcomes. Level of immersion in the new culture or how far people have deviated from their cultural origins in adopting features of the new or dominant culture Conflicting evidence about the influence of acculturation on health behaviors (see table). Lara M, Gamoa C, Kahramanian MI, Morales LS, Hayes Bautista DE. (2005). Annu Rev Public Health, 26, 367-97. Millard AV, Graham MA, Mier N, Flores I, Carrillo-Zuniga G, & Sánchez ER. Addressing Health Disparities: The Hispanic Perspective. In S. Kosoko-Lasaki, R.L. O'Brien & C.T. Cook [Eds.]. Promoting Cultural Proficiency in Eliminating Health Disparities. Boston: Jones & Bartlett Publishers. (In Press.) Salient culturally sensitive intervention components are Bilingual and bicultural facilitators and materials Family-based activities Literacy-appropriate materials Social support. Having a clear understanding of Hispanic cultural values is also required. Evidence-based programs must use a program structure and curriculum that have been proven through prior research to be beneficial for participants. Incorporate measurable goals so that program managers can further evaluate and document their benefits in different settings and populations. Mary Altpeter, Ph.D., “Healthy Aging Briefing Series: The Basics of Evidence-Based Health Promotion Programming,” July 20, 2006. Pilot study A walking program for low-income women of Mexican origin living in areas known as “colonias” in the Texas-Mexico border region. Stages of Change Model Community-based Participatory Research 1.2 million people (U.S. Census 2006) Hidalgo and Cameron: 2 of the 10 poorest counties in the US 89.5% of the population: Hispanic (US Census Bureau, 2006) (Fronczek 2005) SOURCE: The Rio Grande Valley Partnership/Chamber of 22% 2001- 2006 8% 13% Valley El Paso Texas 6% 2006 US (US Census Bureau, 2006) EDUCATION LEVEL (< HS) % people 25 years and over 39% 21% Valley Texas 16% US (US Census Bureau, 2006) Speak a language other than English at home (% population > 5 yrs) 79% 34% 20% Valley Texas US (US Census Bureau, 2006) Unincorporated, impoverished settlements located along the U.S.-Mexico international boundary (Ward, 1999) Texas: 1,524 colonias (N=400,000) (Ward, 1999); 60% of these colonias are located in Hidalgo County . (Federal Reserve Bank of Dallas (FRBD), 1995; Housing Assistant Council, 2000; Ward, 1999) Average household income > $834 month 70% of residents have less than high school education High unemployment rates (20% - 60%, compared to 7% at the state level) and a lack of medical services . 50% of colonia residents are immigrants, mostly from Mexico (FRBD) (Dutton, Weldon, Shannon, Bowcock, Tackett-Gibson, Blakely et al., 2000). IDENTIFIED PHYSICAL ACTIVITY NEEDS ADMINISTERED A SURVEY COLONIA RESIDENTS ASKED FOR A PROGRAM Location Dates Residents and promotoras Recruitment Times Developed the Vamos a Caminar handbook -Included topics of diabetes and exercise - Addressed dogs problem - Social activities - Certificate - Children’s issue Be Active for Life Handbook Researchers and promotoras revised contents WALKING PROGRAM -Nonexpensive - Feasible activities The duration of the program was 12 weeks Program based on PA recommendations and encouraged participants to incorporate walking activities into their lifestyle. The groups met separately every week for 1hour The promotoras worked with participants using a problem-solving, self-management approach to discuss physical activity behavior change strategies. Addressed challenges Ninety-three percent of participants attended 88% of the sessions According to the program fidelity assessment we conducted, the promotoras delivered every lesson of the program as planned Acceptance of the program was assessed through feedback sessions with participants. Theory driven and use of the communitybased participatory research Feasibility issues: cost, setting, training, language. Acculturation? Evaluation issues