4053X1 1999 Nov25
advertisement

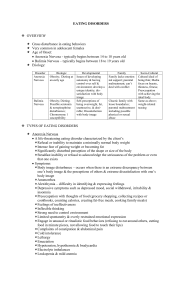
Child Psychopathology Normal eating behavior Eating disorders Reading: Chapter 13 Normal eating development Troublesome eating habits and limited food preferences are common in early childhood among boys and girls Family rituals surround eating, e.g., getting children to eat new foods Societal norms and expectations affect girls more than boys, particularly at adolescence Continuity in eating behavior and later problems Pica Bulemia Picky eating, Digestive problems Anorexia Other risk factors: Early pubertal maturation, high body fat, concurrent psychological problems, poor body image Diagnostic criteria for pica and rumination disorder Table 13.1 & 13.2 of the text What is wrong with this billboard? 1. Glamorizes anorexia, a deadly physical and mental illness, as "cute" 2. Sends the message that starving oneself leads to beauty and approval 3. Insults eating disorders sufferers, their loved ones and women everywhere who are tormenting themselves to meet an unattainable beauty ideal Anorexia nervosa Refusal to maintain weight, intense fear of gaining weight, disturbance in perception of body size Denial of thinness Menstrual cycle stops due to low body fat Restricting type: Diet, fasting or excericise Binge-eating/Purging type Bulimia nervosa Binge eating follows change in mood, stress, or hunger Purging involves selfinduced vomiting, diuretics, laxative abuse, or by other compensation (e.g., exercise) Weight is usually average or slightly above average Diagnostic criteria in Tables 13.4 and 13.5 Prevalence 1-2% of population, more common than 30 years ago More common in females than males (approximately 10:1 ratio); Purgative behaviors may differ Usually strikes between age 14 18, but exists in adulthood and even late childhood 50% show complete recovery, others may continue irregular eating and body dissatisfaction Etiology Neurobiology and genetic contributions – addiction models have looked at endogenous opiods released when hungry Sociocultural factors – belief that self-worth, happiness, and success are determined by appearance – dieting/ nondieting cycle – prevalence of social models (e.g., 90120) Family interaction patterns – Enmeshment, alliances, conflicts, victimisation, parental pressure Psychological factors Autonomy, competence, and control are themes Phobic avoidance of normal adult body weight or sexual maturity in anorexia Binge/Purge cycle becomes addictive Unattainable standards of perfectionism Bulimia related to poor impulse control , sexual acting out, borderline or histrionic personality disorders Treatment is difficult: Anorexia Bulimia Hospitalisation, i.v. feeding at “set point” may be necessary Contracting for weight gain to earn privileges (e.g., access to family) & avoid food battles Family therapy to deal with autonomy and control Individual counselling Dietary education Hospitalisation may be necessary if electrolytes are “out of whack” (siezures) or purging must be monitored Cognitive Behavioral approaches to address self control Antidepressants have been helpful Dietary education