- University of Portsmouth
advertisement

MICRO-MECHANICAL DAMAGE OF TRABECULAR BONE-CEMENT
INTERFACE UNDER SELECTED LOADING CONDITIONS: A FINITE
ELEMENT STUDY
Qing-Hang Zhang, Gianluca Tozzi, Jie Tong
Mechanical Behaviour of Materials Laboratory
School of Engineering
University of Portsmouth, UK
For correspondence:
Prof. Jie Tong, Ph.D.
Mechanical Behaviour of Materials Laboratory
School of Engineering
University of Portsmouth
Anglesea Road
Portsmouth PO1 3DJ
UK
Tel: 0044-9284-2326
Fax: 0044-9284-2351
Email: jie.tong@port.ac.uk
ABSTRACT
In this study, two micro finite element (FE) models of trabecular bone-cement
interface developed from high resolution computed tomography (CT) images were
loaded under compression and validated using the in situ experimental data. The
models were then used under tension and shear to examine the load transfer
between the bone and cement and the micro damage development at the bonecement interface. In addition, one of the models was further modified to investigate
the effect of cement penetration on the bone-cement interfacial behaviour. The
simulated results show that the load transfer at the bone-cement interface occurred
mainly in the bone cement partially integrdigitated region, while the fully interdigitated
region seemed to contribute little to the mechanical response. Consequently cement
penetration beyond a certain value would seem to be ineffective in improving the
mechanical strength of trabecular bone-cement interface. Under tension and shear
loading conditions, more cement failures were found in denser bones, whilst the
cement damage are generally low under compression.
Keywords: trabecular bone-cement interface, finite element analysis, micromechanical behaviour, cement penetration depth, loading modes.
2
1. Introduction
Cemented joint fixation relies on mechanical interlocking between the bone
and the cement. The mechanical interlocking, or interdigitation, is achieved by
frictional contact of the mating morphologies as the cement has no adhesive
properties (Skripitz and Aspenberg, 1999; Lucksanasombool et al., 2003). The bonecement interdigitation could be affected by a number of factors including cement
viscosity (Stone et al., 1996; Race et al., 2006), bone preparation technique
(Majkowski et al.,1993; Berry, 2004) and degree of cement pressurization (Oates et
al., 1995; Flivik et al., 2005). However, the role of cement penetration in improving
the bone-cement strength is still unclear so far. The results from Mann et al. (1997,
2001) showed some moderate correlation between the interdigitation and the
apparent strength under tension and shear. In the studies of Krause et al (1982) and
Majkowski et al. (1994), however, cement penetration depth was shown to have low
effect on the apparent strength under tension and shear, respectively.
Recently, micro-mechanical experimental studies together with digital image
correlation techniques have been conducted to investigate the failure behaviour of
bone-cement interfaces under various loading conditions (Mann et al., 2008, 2009).
The results showed that the main deformation in the specimens occurred at the
bone-cement interface, where more micro-crack damage was found in the cement
and the damage was localised within the interdigitated region. In the study of Mann
et al. (2008), the compliance values of specimens with and without an interdigitated
region were compared, although the contribution of the contact interface and the fully
interdigitated bulk composite region to the load transfer was not assessed, largely
due to the lack of latter in their bone type taken from the medullary cavity of the
femur with only limited trabecular bone.
Complementary to experimental studies, FE models of detailed bone-cement
interface developed from high resolution CT images were also used to reveal the
local stress-displacement response of bone and cement which cannot be otherwise
obtained from testing (Janssen et al., 2008, 2009; Waanders et al., 2009, 2010). The
first micro FE model of bone-cement composite was developed by Janssen et al.
(2008), in which the effect of parametric variations of frictional, morphological and
material properties on the mechanical response of the bone-cement interface was
3
analysed. Further analyses using these models also showed that high interdigitation
and large contact area can strongly increase the apparent strength, although more
cracks occurred in the cement than in the bone irrespective of the average
interdigitation depth (Janssen et al., 2009; Waanders et al., 2010). In the above
mentioned FE studies, the bone-cement interface specimens were prepared using
bones from the medullary cavity of the femur which has mostly cortical bone with
limited trabecular bone, hence the range of the cement penetration depth is also
limited (<2.2mm). The load transfer and damage development at the bone-cement
interface is still unclear when increased cement penetration is attempted, such as in
the case of acetabular or knee replacements.
In our previous study, bovine trabecular bone were used to interdigitate with
bone cement to obtain trabecular bone-cement interface specimens with relatively
high average cement penetration (3.60±1.50 mm) (Tozzi et al., 2012). A novel
custom-made micromechanical loading stage and time-lapsed µCT imaging were
used to assess the real-time local deformation and damage development in the
bone-cement specimens under selected levels of uniaxial compression. A FE bonecement interface model was also developed to investigate the possible load transfer
path between the bone and the cement. It was found that, under compression, the
load transfer in bone-cement interface occurred mainly in the bone-cement partially
interdigitated region and thus a higher penetration depth had no effect on the
mechanical response. The purpose of the current study is to examine the effect of
cement penetration on the mechanical response under tensile and shear as well as
compressive loading conditions. FE models were built base on CT images of two
trabecular bone-cement interface specimens, and validated using the experimental
data obtained from the compressive tests.
The load transfer and damage
development in the bone-cement interface were examined in tensile and shear
loading cases, and compared with those under compression.
2. Material and Methods
Two lab prepared bovine trabecular bone-cement interface specimens (BC01,
BC02) tested in a previous study (Tozzi et al, 2012) were selected for the current FE
modelling and parametric analyses. The µCT images of the two specimens with
4
resolution of 20µm were imported into Avizo 6.3 (Visualization Sciences Group,
Mérignac, France) for three-dimensional reconstruction and FE mesh generation.
The bone and the cement structures were segmented mainly based on the threshold
values, while editing and Boolean operations were further performed to separate the
two materials and remove isolated artefacts. The generated bone and cement
volumes were meshed individually using four-nodded tetrahedral elements, in which
the cement volume was shrunk by one voxel (20µm) to ensure the absence of initial
penetration between the two constituents. The element size for the bone mesh was
controlled to be about 40µm to ensure numerical accuracy (Niebur et al., 1999),
while the element size of the cement mesh was set to be 60 - 100µm to limit the total
number of elements. In addition, the remote part of the cement was removed to
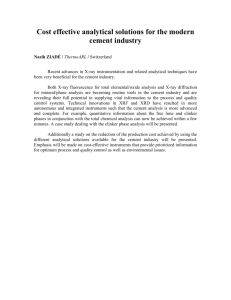
further reduce the total mesh size. The created bone-cement interface models, with
a dimension of 9mm×8mm×4.4mm, consist of 2,506,235 and 3,726,972 elements
and 571,756 and 820,277 nodes for BC01 and BC02, respectively (Figure 1). The
detailed morphological parameters for these two models are listed in Table 1, where
the methods of calculation of volume fraction (BV/TV) and cement penetration
followed Tozzi et al. (2012).
The trabecular bone tissue was modelled as a bi-linear elastic-plastic
𝑦𝑡
𝑦𝑐
material, with an asymmetric yield strain of 0.6% (𝜀𝑏 ) in tension and 1% (𝜀𝑏 )in
compression (Niebur et al., 2000). The elastic modulus (𝐸𝑏 ), Poisson's ratio and
post-yield modulus (𝐸𝑏′ ) were assumed to be 15GPa, 0.3 and 750MPa, respectively.
A similar but symmetrical bi-linear elastic-plastic constitutive law was used for the
cement material, of which the elastic modulus (𝐸𝑐 ), Poisson's ratio, yield stress (𝜎𝑐 )
and post yield modulus (𝐸𝑐′ ) were assumed to be 3GPa, 0.33, 40MPa, and 1MPa,
respectively (Harper & Bonfield, 2000; Lewis, 1997). The detailed constitutive laws
used were as follows. For bone tissue:
𝑦𝑐
𝑦𝑐
{𝜀𝑏𝑦𝑐 ≤ 𝜀 ≤ 𝜀𝑏𝑦𝑡
𝑦𝑡
𝜀𝑏
𝑦𝑐
𝜎 = 𝐸𝑏 𝜀𝑏 + (𝜀 − 𝜀𝑏 )𝐸𝑏′
𝜀 < 𝜀𝑏
𝜎 = 𝐸𝑏 𝜀
<𝜀
𝜎=
𝑦𝑡
𝐸𝑏 𝜀𝑏
+ (𝜀 −
,
(1)
𝑦𝑡
𝜀𝑏 )𝐸𝑏′
for cement:
𝑦
{
𝜎 ≤ 𝜎𝑐
𝑦
𝜎𝑐 < 𝜎
𝜎 = 𝐸𝑐 𝜀
𝑦
𝜎 = 𝜎𝑐 + 𝐸𝑐′ (𝜀 −
𝑦
𝜎𝑐
𝐸𝑐
.
)
(2)
5
The interaction between the contact surfaces of the bone and the cement was
modelled as surface to surface finite sliding contact, with a friction coefficient of 0.4
(Jin, 2006).
All the simulations were performed on the FE solver ABAQUS 6.9 (Dassault
Systèmes, RI, USA), using large deformation to account for geometrical nonlinearity.
The bottom surface of the cement was fully constrained in all degrees of freedom
while a uniaxial static displacement, in compression, tension and shear, was applied
incrementally to the top surface of bone up to 0.3mm. The predicted apparent stressdisplacement curves of the two subject-specific models under compression were
then compared against their experimental results (Tozzi et al., 2012). In addition, the
predicted local strain distributions were compared with the recorded local
deformation in a sub-volume reconstructed from the CT images at the maximum
displacements.
To facilitate the analyses, regions of interest were defined in the FE models
as: Bone; bone and cement partially interdigitated (BC-PI); bone and cement fully
interdigitated (BC-FI) and cement region, as shown in Figure 1. The BC-FI region
was absent for sample BC02 due to its relatively low cement penetration. The
principal strains of each bone element were examined at every increment, in which
any element with either maximum principal strain higher than 0.6% or minimum
principal strain lower than -1.0% was defined as “damaged”. For the cement, any
element with a von Mises stress higher than the yield stress was deemed as
"damaged". The damaged bone and cement elements in these regions as a function
of the applied displacement were recorded.
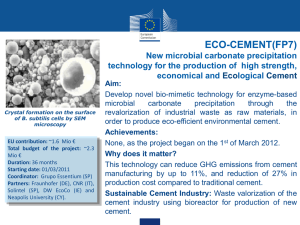
To investigate the effects of cement penetration on bone-cement interface
behaviour, two additional models (BC01a, BC01b) were created from BC01 by
converting some of the trabecular bones into cement to manually reduce the cement
penetration (Figure 2). As the reduction of cement penetration mainly occurred in the
BC-FI region, the comparison of the predicted results from the three models may
help to identify the role of cement penetration as well as the contribution of the BC-FI
region on the apparent strength of the bone-cement interface, whilst the influence of
bone morphology was removed.
6
3. Results
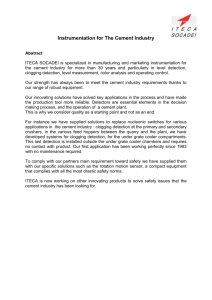
Figure 3 shows the predicted stress-displacement curves of the two models
and the experimental responses of the subject-specific specimens. Generally
speaking the comparison seems reasonable. The predicted stiffness of BC01 and
BC02 are about 50% and 30% higher than the experimental values, respectively;
while the predicted peak stresses are slightly lower. Although the FE model could not
reproduce the large deformation, such as buckling of the trabeculae, the predicted
strain concentrations in the subject-specific models seem to correlate well with the
eventual deformation observed from the experiment of the same sub-volume (Figure
4). It was found that the predominant deformation initiate in the Bone region,
whereas the Cement region appeared to be unaffected even towards the final stage,
which was consistent with the predicted overall strain distributions of the two models.
Trabecular bone seems to sustain most of the damage under tension and
shear loading conditions. Under tensile displacement of 0.3mm, the damaged bone
volumes in BC01 and BC02 are 13.9% and 12.0%, respectively; while the damaged
cement volumes are only 0.1% and 2.3%, respectively. The predicted peak stress
under compression is higher than that under tension and shear due to the
asymmetric yield strains assigned for the trabecular bone tissue. In addition, the
predicted stiffness and peak stresses of BC02 are higher than those of BC01 under
the same loading conditions due to its higher bone volume fraction (Figure 5a).
The fully interdigitated (BC-FI) region seems to have little influence on the
bone-cement interfacial behaviour. As shown in Figure 5b, there is virtually no
difference between the peak stress from model BC01 and BC01a. Even when the
entire BC-FI region was removed (BC01b), the reduction in the peak stress (in
tension) is still less than 10%. The load transferred through the BC-PI region of
BC01 under the three simulated loading conditions are presented in Figure 6, wich
may help to further explain the contribution of the two regions on the bone-cement
interface load transfer. In addition, the predicted distributions of the damaged
elements of the two models under the three loading directions are shown in Figure 7.
Generally speaking, for a bone-cement interface specimen containing both BC-PI
and BC-FI region (BC01), the damage of bone occurred mainly in the Bone and the
BC-PI region, whilst cement failed mainly in the BC-PI region due to the load shared
7
in different regions. At a displacement of 0.3mm, the percentage of damaged bone
volume from the BC-PI region against the whole interdigitated region (BC-PI+BC-FI)
is 96.7%, 94.5% and 98.3% under compression, tension and shear, respectively;
whilst the values for the cement are 97.4%, 95.5% and 84.8%, respectively. It was
obvious that the major load transfer between the bone and the cement occurred in
the BC-PI region, and any further increase in cement penetration may not be
effective in improving the apparent strength.
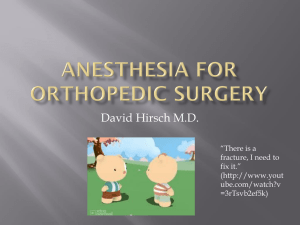
Figure 8 showed quantitatively the damage evolution of the bone and the
cement in the interdigitated region (BC-PI+BC-FI) for the two models. It seems that
bone density affects both the damage in the bone and in the cement. The bone
damage in sample BC02 is lower than that of BC01; while the reverse is true for the
damage in the cement due to the higher BV/TV of trabecular bone in sample BC02.
When the bone and the cement damages from the same model are compared, the
bone damage of both models is higher than that of cement under compression.
Under tension and shear, however, the cement damage is higher than that of bone in
sample BC02 but reverse is true for sample BC01. For sample BC02, the tensile
loading resulted in the highest cement damage, followed by shear and compression.
For BC01, the maximum cement damage is found under shear while minimum under
tension. Comparatively, the cement damage under compression from both models is
very low (<0.6%). It seems that the interfacial failure behaviour of bone-cement
interface may be affected by both bone morphology and loading mode.
4. Discussion
In our previous study, pure bovine trabecular bones were used to interdigitate
with bone cement to obtain trabecular bone-cement interface samples, which were
tested in step-wise compression using a custom-made loading stage within the µCT
chamber (Tozzi et al., 2012). In the current study, finite element models of two of
those specimens, one with a relatively high (BC02) and another (BC01) relatively low
bone volume fraction, were built and validated using the experimental results. The
models were then used to further explore the micro-mechanical behaviour of the
bone-cement interface under tensile and shear loading conditions. The results from
both experimental observation and numerical prediction showed that the bone
sustained most of the deformation in the bone-cement composite. Thus the
8
mechanical responses of such specimens are mainly determined by the properties of
the trabecular bone (Figure 5a). The bone BV/TV has a significant influence also on
the damage development pattern (Figure 8), particularly for tensile and shear loading
cases.
Higher apparent strengths were achieved when the bone with a higher
BV/TV was used to interface with the cement. Moreover, more cement damage
occurred in the interface generated using a bone with high BV/TV under tension and
shear load cases (Figure 8b, c).The same conclusion could also be drawn when the
absolute damaged volume were used for comparison. These results are consistent
with Waanders et al (2010) who observed predominant failure in the cement when
the interface samples were built from bones from the medullary cavity of proximal
femurs, where a mixture of cortical bone and trabecular bone is present. The cement
interdigitation in these cases would be admittedly limited. This might also be the
main reason for the discrepancy between the results from the current study and
those of Waanders et al. (2010) regarding the apparent model response under
tension and shear. In the current study, both the apparent stiffness and peak stress
under shear are lower than those under tension since the response of the trabecular
bone dictates the response. In the study of Waanders et al. (2010), the interface
models are stronger under shear but stiffer under tension because the responses of
their model are from the intedigitated region with the contribution from both bone and
cement.
Model BC01 was further modified to study the effects of varying cement
penetration depth on the apparent strength under compression, tension and shear
loading conditions. No effect of cement penetration depth on the apparent strength
was found for all three loading conditions. This is significant as, although this
observation is made from the numerical results only, the influence of morphological
parameters is nevertheless removed in the present cases, unlike in experimental
studies where such an influence invariably presents. The underline reason for this is
because the primary load transfer between the bone and the cement occurs at the
BC-PI region or at the immediate contact region between the bone and the cement,
whereas further penetration in the BC-FI region had little effect on the apparent
response of the bone-cement composite (Figures 7, 8). As a result, no further gains
in apparent strength may be obtained beyond a certain depth of cement penetration.
This may help to explain some of the discrepancies in the results reported in the
9
literature. In the study of Majkowski et al. (1994), the shear strength of the bonecement interface had no correlation with the cement penetration depth for specimens
with a mean penetration from 2.9 to 9.2 mm; while Waanders et al. (2010) found a
strong correlation between the apparent strength and the cement penetration depth.
In the latter case, however, the cement penetration depth was no more than 2.2mm,
and virtually no BC-FI region due to the type of bones used in their models. In
Majkowski et al. (1994), however, only cancellous bones, as in the current study,
were utilised thus a significant BC-FI region would be present due to the high cement
penetration achieved, although ultimately ineffective.
A main limitation of the current study is that, although the FE models are
validated from in situ experimental data under compression, there are no
experimental data for tension and shear load cases, hence only numerical results
are presented. Secondly, simple elastic-plastic material constitutive models were
used for the bone and the cement, which cannot account for failures such as
cracking in the cement or buckling in the bone. These treatments are necessarily
approximate due to the lack of a multiaxial constitutive law for trabecular tissue, and
micro-mechanics consideration for the cement. Nevertheless only relatively low
displacement (0.3mm) was applied so the failure modes associated with large
deformation may be insignificant. For example, the peak percentages of the volumes
that sustained more plastic energy than elastic energy are relatively small (<4% for
bone; <1% for cement), suggesting that the overall deformation is reasonably well
defined by the constitutive laws. Finally, the study was only applicable for assessing
the initial state of cemented fixation without any bone remodeling.
5. Conclusions
FE models of two trabecular bone-cement composite specimens were
constructed and analysed to investigate the micro-mechanical behaviour of bonecement interface under tension, compression and shear loading conditions. It was
found that the load transfer in bone-cement interface occurred mainly in the partially
integrdigitated region, while the fully interdigitated region contributed little to the
apparent mechanical response of the trabecular bone-cement composite. The bone
and the cement damages were affected by both bone morphology and loading
10
directions. More cement failure was observed in the bone-cement composite when
the bone density was high under tension and shear loading conditions. Under
compression, the cement damage was generally low, irrespective of the bone
density.
Conflict of interest statement
There is no conflict of interest to declare.
Acknowledgements
The authors gratefully acknowledge the provision of the friction coefficient
between the bovine cancellous bone and the bone cement by Professor Z-M Jin of
University of Leeds. The bone cement was donated by Stryker, UK.
Numerical
computations were performed on the Sciama High Performance Compute (HPC)
cluster which is supported by the ICG, SEPNet and the University of Portsmouth.
REFERENCES
Berry, D.J., 2004. Cemented femoral stems: what matters most. J. Arthroplasty 19,
83–84.
Flivik, G., Sanfridsson, J., Onnerfalt, R., Kesteris, U., Ryd, L., 2005. Migration of the
acetabular component: Effect of cement pressurization and significance of early
radio-lucency.
A
randomized
5-year
study
using
radiostereometry.
Acta
Orthopaedica. 76(2), 159-68.
Harper, E.J., Bonfield, W., 2000. Tensile characteristics of ten commercial acrylic
bone cements. Journal of Biomedical Materials Research. 53(5), 605-616.
Janssen, D., Mann, K.A., Verdonschot, N., 2008. Micro-mechanical modeling of the
cement-bone interface: the effect of friction, morphology and material properties on
the micromechanical response. Journal of Biomechanics. 41(15), 3158-63.
Janssen, D., Mann, K.A., Verdonschot, N., 2009. Finite element simulation of
cement-bone interface micromechanics: a comparison to experimental results. J
Orthop Res. 27(10), 1312-8.
11
Jin, Z-M, 2006, private communication.
Krause, W.R., Krug, W., Miller, J., 1982. Strength of the cement-bone interface. Clin.
Orthop. Rel. Res. 163, 290-299.
Lucksanasombool P, Higgs WA, Ignat M, Higgs RJ, Swain MV., 2003. Comparison
of failure characteristics of a range of cancellous bone-bone cement composites. J
Biomed Mater Res A. 64(1), 93-104.
Lewis, G., 1997. Properties of acrylic bone cement: State of the art review. Journal of
Biomedical Materials Research. 38(2), 155-182.
Majkowski, R.S., Miles,A.W., Bannister,G.C., Perkins,J., Taylor,G.J., 1993. Bone
surface preparation in cemented joint replacement. J. Bone. Joint. Surg. Br. 75, 459–
463.
Majkowski RS, Bannister GC, Miles AW., 1994. The effect of bleeding on the
cement-bone interface. An experimental study. Clin. Orthop. Relat. Res. 299, 293297.
Mann, K.A., Ayers, D.C., Werner, F.W., Nicoletta, R.J., Fortino, M.D., 1997. Tensile
strength of the cement-bone interface depends on the amount of bone interdigitated
with PMMA cement. J. Biomech. 30, 339-346.
Mann, K.A., Mocarski, R., Damron, L.A., Allen, M.J., Ayers, D.C., 2001. Mixed-mode
failure response of the cement-bone interface. J. Orthop. Res. 19, 1153-1161.
Mann, K.A., Miller, M.A., Clearly, R., Janssen, D., Verdonschot, N., 2008.
Experimental micromechanics of the cement-bone interface. J. Orthop. Res. 26(6),
872-79.
Mann, K.A., Miller, M.A., Race, A., Verdonschot, N., 2009. Shear fatigue
micromechanics of the cement-bone interface: an in vitro study using digital image
correlation techniques. J. Orthop. Res. 27(3), 340-6.
Niebur, G.L., Feldstein, M.J., Yuen, J.C., Chen, T.J., Keaveny, T.M., 2000. Highresolution finite element models with tissue strength asymmetry accurately predict
failure of trabecular bone. Journal of Biomechanics. 33, 1575-1583.
12
Niebur, G.L., Yuen, J.C., Hsia, A.C., Keaveny, T.M., 1999. Convergence behavior of
high-resolution finite element models of trabecular bone. ASME, Journal of
Biomechanical Engineering 121(6), 629-35.
Oates, K.M., Barrera, D.L., Tucker, W.N., Chau, C.C.H., Bugbee, W.D., Convery,
F.R., 1995. In vivo effect of pressurisation of polymethylmethacrylate bone-cement.
Journal of Arthroplasty. 10(3), 373-81.
Race, A., Miller,M.A., Clarke,M.T., Mann,K.A., Higham,P.A., 2006. The effect of lowviscosity cement on mantle morphology and femoral stem micromotion: a cadaver
model with simulated blood flow. Acta Orthop. 77, 607–616.
Schmalzried TP, Kwong LM, Jasty M, Sedlacek RC, Haire TC, O'Connor DO,
Bragdon CR, Kabo JM, Malcolm AJ, Harris WH., 1992. The mechanism of loosening
of cemented acetabular components in total hip arthroplasty. Analysis of specimens
retrieved at autopsy. Clin Orthop Relat Res. 274, 60-78.
Skripitz R, Aspenberg P., 1999. Attachment of PMMA cement to bone: force
measurements in rats. Biomaterials. 20(4), 351-6.
Stone, J.J., Rand,J.A., Chiu,E.K., Grabowski,J.J., An,K.N., 1996. Cement viscosity
affects the bone–cement interface in total hip arthroplasty. J. Orthop. Res.14, 834–
837.
Tozzi, G., Zhang, Q.H., Tong, J., 2012. 3D real-time micromechanical compressive
behaviour of bone-cement interface: experimental and finite element studies. J
Biomech. J Biomech. 45(2):356-63.
Waanders, D., Janssen, D., Mann, K.A., Verdonschot, N., 2010. The mechanical
effects of different levels of cement penetration at the cement-bone interface. J
Biomech. 43(6):1167-75.
Waanders D, Janssen D, Miller MA, Mann KA, Verdonschot N., 2009. Fatigue creep
damage at the cement-bone interface: an experimental and a micro-mechanical finite
element study. J Biomech. 42(15):2513-9.
13
Figure Captions
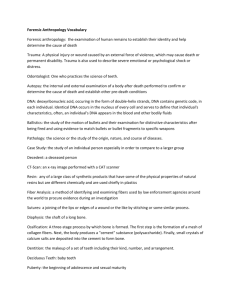
Figure 1. The finite element mesh of the trabecular bone-cement interface models generated
from (a) Sample1 (BC01) and (b) Sample 2 (BC02). The bone volume fractions (BV/TV) for
BC01 and BC02 are 0.152 and 0.230, respectively. Four regions of interest are identified:
Bone, bone-cement partially interdigitated (BC-PI), bone-cement fully interdigitated (BC-FI)
and Cement regions. The BC-FI region is absent in sample BC02. Red – bone; blue – cement.
Figure 2. The finite element mesh of BC01 (a) and two additional models (b, c) obtained by
artificially converting part of bone into cement to obtain variable depths of cement
penetration. ∆1=5.2; ∆2=4.1; ∆3=2.8.
Figure 3. The predicted apparent stress-displacement curves obtained from the two subjectspecific FE models compared with those obtained from the compressive testing of the
samples.
Figure 4. (a) CT images of a typical bone-cement interface sub-volume of BC01 (left) and
BC02 (right); (b) The FE predicted local minimum principal strain distributions of the subvolume and (c) CT images of the local deformation sustained in the sub-volume at the failure
state. The high local strain predicted may explain the local bulking damage observed
experimentally, as indicated by the arrows.
Figure 5. (a) The predicted apparent stresses of the two models at a 0.3mm displacement
under compression, tension and shear loading conditions; (b) The predicted apparent stresses
of the original BC01 and two modified models BC01a, BC01b at a 0.3mm displacement
under compression, tension and shear.
Figure 6. The contribution of load transferred in the BC-PI region of sample BC01 as a
function of the applied displacement. The percentage value was obtained by dividing the
14
contact force generated in the BC-PI region by the total contact force from carried by both the
BC-PI and the BC-FI regions.
Figure 7. The predicted distributions of yielded elements from (a) BC01 and (b) BC02 at a
displacement of 0.3mm under compression (left), tension (middle) and shear (right). The blue
represents yielded cement and red represents yielded bone.
Figure 8. The predicted percentage of yielded volumes accumulated for bone and cement in
the interdigitated region (BC-PI+BC-FI) from the two samples as a function of the applied
displacement under (a) compression; (b) tension and (c) shear. The percentage value was
obtained by dividing the yielded bone/cement volume by the corresponding whole
bone/cement volume in the same region.
15
Figures
(a)
(b)
16
Figure 1.
Δ1
(a)
Δ3
Δ2
(b)
(c)
Figure 2.
17
6
BC01-Exp
BC01-FE
BC02-Exp
BC02-FE
Stress (MPa)
4
2
0
0
0.2
0.4
0.6
Displacement Applied(mm)
Figure 3.
18
0.8
(a)
(b)
(c)
19
Figure 4.
20
6
BC01
BC02
Stress (MPa)
4
2
0
Compression
Tension
Shear
(a)
4
BC01
BC01a
BC01b
Stress (MPa)
3
2
1
0
Compression
Tension
(b)
Figure 5.
21
Shear
Percentage of Load transferred through
BC-PI region
100%
80%
60%
Compression
40%
Tension
Shear
20%
0%
0
0.1
0.2
Displacement (mm)
Figure 6.
(a)
(b)
22
0.3
Figure 7.
BC01-Bone
BC01-Cement
BC02-Bone
BC02-Cement
Normalized Yielded Cement Volume
6%
4%
2%
0%
0
0.1
0.2
Displacement (mm)
(a)
23
0.3
BC01-Bone
BC01-Cement
BC02-Bone
BC02-Cement
Normalized Yielded Cement Volume
12%
8%
4%
0%
0
0.1
0.2
0.3
0.2
0.3
Displacement (mm)
(b)
BC01-Bone
BC01-Cement
BC02-Bone
BC02-Cement
Normalized Yielded Cement Volume
6%
4%
2%
0%
0
0.1
Displacement (mm)
24
(c)
Figure 8
25
Table Captions
Table 1. The basic morphological parameters of the bone-cement models studied.
Table 1.
BC01
BC01a
BC01b
BC02
Bone BV/TV
0.152
0.152
0.152
0.230
Average
3.43
2.33
1.03
1.10
5.20
4.10
2.80
3.55
Penetration
(mm)
Maximum
Penetration
(mm)
26