Delirium Prevention, Assessment and Management
advertisement

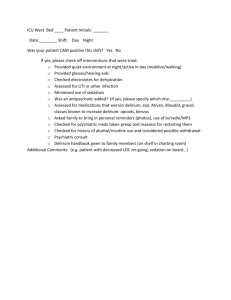
Delirium Prevention, Assessment and Management Susan Schumacher, MS, G-CNS Objectives • Identify 3 differences in clinical presentation of delirium versus underlying dementia. • Explain how to perform the Confusion Assessment Method (CAM). • Identify at least 3 factors contributing to the development of delirium. • Identify appropriate interventions to prevent or shorten the course of delirium. • Describe pharmacological treatment of delirium. What is Delirium? A transient state of cognitive impairment manifested by simultaneous disturbance of behaviors that develop abruptly and fluctuate diurnally (daily) Changes Observed in Delirium • • • • • • • Level of consciousness Attention Perception Memory Thinking Orientation Psychomotor behavior Perceptions from Patients • “I thought there were some photographers and things around taking advantage of people.” • Felt like “someone had pulled a curtain.” • Felt like “hospital staff were plotting against me.” – McCurren, Cronen (2003) How Common is Delirium? • Incidence within hospital 4-53.3% • Complicates hospital stay for more than 2.3 million older persons annually • Occurs in 5-61% of orthopedic patients, especially those with hip fractures • Between 22-89% of patients with delirium have underlying dementia. • Prevalence in patients receiving mechanical ventilation is as high as 83%. Differentiating Delirium and Dementia Delirium Dementia Onset Acute, abrupt Insidious Duration Hours to days, may last months Months to years Course Fluctuating course which tends to be worse at night Steady decline; can be stepwise decline with vascular dementia. Attention Inattention present No change Differentiating Delirium and Dementia Delirium Dementia Consciousness Changes- vigilant to lethargic No change until late in the illness Hallucinations/Delusions Visual and auditory hallucinations and delusions Delusions Visual hallucinations with Lewy body dementia Sleep/wake cycle Impaired, sleep schedule Fragmented; may can become reversed awaken frequently Mood/Affect Rapid swings; paranoid Apathetic, depressed Psychomotor behavior Hypoactive, hyperactive or mixed No change Outcomes Related to Delirium • • • • Length of stay Higher level of care at discharge Increased mortality after discharge Increased risk of adverse events Investigating the factors leading to Delirium (Multi-factorial) • Underlying risk factors: Factors that cannot be changed which impact delirium. • Precipitating factors: Factors that contribute to development of delirium which can be changed. Underlying Risk Factors • • • • • • • Dementia Substance abuse Parkinson’s disease Sensory deficits Age Traumatic brain injury Chronic kidney disease Precipitating Factors • • • • • • • • Hypoxia Infections Electrolyte imbalances Anemia Medications Uncontrolled pain Constipation Tethers (catheters) What is Confusion Assessment Method(CAM)? • Diagnostic assessment tool for delirium developed by Sharon Inouye (Yale) • Assesses 4 features of delirium: – Acute onset and fluctuating course – Inattention – Disorganized thinking – Altered level of consciousness Completion of CAM • On admission for all patients greater than 70 years • Every 8 hours for patients greater than 70 years • Supportive information: – Hours of sleep – Agitation score – Behaviors – Nursing interventions CAM Assessment on Admission • Completed and documented within 4 hours of admission – Baseline Cognitive Status Impairment (dementia, traumatic brain injury, other neurologic diseases impacting cognition) – Admission Cognitive Status – CAM completed by Surgery Center RN for surgical patients (documented in PICIS) Criteria for Patients Unable to Complete the CAM • Language Barrier (unable to speak english) • Receptive/Expressive Aphasia • Unconscious or sedated (Use CAM-ICU) • Severe stage of dementia or brain injury What makes a positive CAM? Feature I: Acute Onset of mental status changes AND Feature II: Inattention AND Feature III: Disorganized Thinking AND/ OR Feature IV: Altered Level of Consciousness ONE abnormal finding for each feature = a positive result for that feature Confusion Assessment Method (CAM) • Criteria 1 (Acute onset and Fluctuating Course)- Has patient changed from their baseline cognitive status? Does the behavior fluctuate during the day, such as worse in the evening or night? Case Study- Criteria 1 • An 88 yr old woman who is admitted with an intracranial bleed and has underlying mild cognitive impairment. She has been alert and oriented to person, place and time. She is cooperative with cares, but has a difficult time remembering to use the call light. At 3am she wakes up and cries out for help, pulls out her IV line, tries to push nursing staff away and is paranoid about what the staff are trying to do with her. Case Study- Criteria 1 • A 79 yr old man admitted for total hip is POD #3. He has underlying dementia (mild), CAD, Type II diabetes, and osteoarthritis. Patient’s bed alarm is going off 2-3 times/ shift, as he tries to get out of bed to use bathroom and he forgets to use the call light. He is alert and oriented to person and place, slept well during the night and cooperates with nursing cares. He asks the staff about calling his wife several times every shift. Confusion Assessment Method (CAM) Criteria 2-Inattention • Does the patient have difficulty focusing attention, for example, being easily distractible, or having difficulty keeping track of what was being said? Case Study- Criteria 2 • Talking with a patient about his hospital stay, patient gives eye contact to the nurse initially, but when an x-ray machine moves past his door, his focus shifts to the hallway. Also, patient unable to follow the directions that nurse has provided about using call light when needing assistance. Confusion Assessment Method (CAM) • Criteria 3(Disorganized Thinking) Is the patient’s speech disorganized or incoherent, such as rambling or irrelevant conversation, unclear or illogical flow of ideas, or unpredictable switching from subject to subject? Confusion Assessment Method (CAM) Criteria 4 Levels of Consciousness • Overall, how would you rate this patient’s level of consciousness? • Alert (normal) • Vigilant (hyperalert) • Lethargic (drowsy, easily aroused) • Stupor (difficult to arouse) • Coma (unarousable) Richmond Agitation Sedation Scale (RASS) Scor e Term Description +4 Combative Overtly combative, violent, immediate danger to staff +3 Very agitated Pulls or removes tubes or catheters, aggressive +2 Agitated Frequent non-purposeful movement, fight ventilator +1 Restless Anxious but movements not aggressive, vigorous 0 Alert and calm -1 Drowsy Not fully alert, but has sustained awakening (eye opening/eye contact) to voice (> 10 seconds) -2 Light Sedation Briefly awakens with eye contact to voice (< 10 seconds) -3 Moderate Sedation Movement or eye opening to voice (but no eye contact) -4 Deep Sedation No response to voice, but movement or eye opening to physical stimulation What makes a positive CAM? Feature I: Acute Onset of mental status changes AND Feature II: Inattention AND Feature III: Disorganized Thinking AND/ OR Feature IV: Altered Level of Consciousness ONE abnormal finding for each feature = a positive result for that feature Let’s Practice! E-paging a new Positive CAM Delirium is an urgent medical condition. A positive CAM test should be reported immediately so the patient can be evaluated for delirium quickly. Have this information ready when you page: • BGM • Last void/is patient retaining urine • Oxygen saturation • Last BM If no response • Pain status within 10 mins, • Temperature & Blood Pressure call an RET • I & O balance • Latest labs if available (serum K, Na, Mg, Cr, etc) • Agitation Score Confirm your CAM POSITIVE result with the Charge Nurse before paging. Interventions to Prevent and Manage Delirium • Delirium Prevention Trial (Inouye) – Patients in the highest adherence group demonstrated an 89% reduction in delirium risk compared with patients in the lowest group. – Protocols for orientation, therapeutic activities and mobility make a significant difference when implemented consistently! Intervention Protocols Protocols: • Orientation • Therapeutic activities • Mobility Interventions for Delirium • Medication management – Review for culprit medications – Pharmacy consult – Administer medications for delirium per order set – Pain Management Interventions for Preventing and Resolving Delirium • A2 Evidence – Promotion of nutrition – Removal of urinary catheter and other tethers – Early mobilization – Glasses and hearing aides – Pain management – Bowel and bladder needs – Fluids and electrolyte balance – Adequate 02 Patient and Family Education • Brochure/Booklet – What is Delirium? – Why is it occurring ? – What can be done to treat and resolve it? – What can family members do to help? Comfort Measures and patients with Dementia • Temperature (hot or cold?) • Hungry or thirsty • Over or under- stimulated • Bowel or bladder needs • Provide reassurance • Personal items such as family pictures Hospital Elder Life Program (HELP) • A comprehensive program of care for hospitalized older patients, designed to PREVENT delirium and functional decline. • Target patient =>70 years old with a LOS > 2 days. HELP® Goals • • • • Maintain physical and cognitive functioning throughout hospitalization (through daily interventions) Maximize independence at discharge Assist with the appropriate transition from hospital to home or stepdown setting Improve geriatric skills of staff throughout the general medicine units. Hospital Elder Life Program (HELP) Trained program volunteers: 100 Patient visits per month: 400!! Hospital Elder Life Program (HELP) Key interventions of the program • Daily visitor program with structured cognitive orientation • Therapeutic activities program • Early mobilization • Non-pharmacologic sleep protocol • Hearing and vision protocol • Feeding and fluid assistance • Geriatric patient care education for unit nursing staff How to order a HELP consult Delirium Order set- Medications • IV Haloperidol (Haldol) (Severe, Moderate Hyperactive Delirium and Hypoactive Delirium) – Scheduled doses of Haldol based on RASS score – PRN doses to reduce agitation to 0 on RASS scale or until 8mg given (moderate) 12mg (severe) – Contact provider if Haldol every 30 minutes for 2hours is not decreasing agitation. – Weaning off Haldol (once pt goes 24 hours without prn dose) – Try to avoid in patients with Parkinson’s disease – Risk of prolongation of the QT/QTc interval (baseline and daily EKG) Why the daily EKG? Prolongation of QT/QTc interval may occur with any antipsychotic medication (Haldol) and increases risk for Torsades de Pointes. Delirium Order set- Medications • QUEtiapine (Seroquel) – Used for patients with Parkinson’s disease – May give Haldol and Ativan additionally for RASS score of +3. (Combative patient) – Watch of orthostatic hypotension • LORazepam (Ativan) – Given with IV Haldol for very agitated patients ONLY Prevention of Delirium is Key! References • • • • Inouye,S., Baker, D., Fugal, P. & Bradley, E. (2006). Dissemination of the hospital elder life program: Implementation, adaptation, and successes. Journal of Gerontological Society, 54:1492-1499. Inouye,S., Bogardus,S., Williams,C. & Leo-Summers,L. (2003). The role of adherence on the effectiveness of nonpharmacologic interventions. Archives of Internal Medicine, 163: 958-964. Robinson,S., Rich, C., Weitzel,T., Vollmer, C. & Eden,B. (2008). Delirium prevention for cognitive, sensory, and mobility impairments. Research and Theory for Nursing practice: An International Journal, 22(2): 103-113. Sendelbach, S.& Finch Guthrie,P. (2009). Acute Confusion/Delirium. In M.G. Titler (Series Ed.), Series on Evidence-Based Practice for Older Adults, Iowa City, IA: The University of Iowa College of Nursing Interventions Research Center, Research Translation and Dissemination Core.