DVT Prophylaxis in the Cancer Patient
advertisement

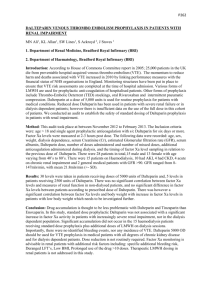
A Year 2009 Update for The Health System Pharmacist The Pharmacologic Foundations of DVT Prophylaxis in the Setting of Cancer Program Co-Chairs Samuel Z. Goldhaber, MD Edith Nutescu, PharmD, FCCP Clinical Associate Professor Pharmacy Practice Affiliate Faculty, Center for Pharmacoeconomic Research Director, Antithrombosis Center The University of Illinois at Chicago College of Pharmacy & Medical Center Chicago, IL Professor of Medicine Harvard Medical School Cardiovascular Division Director, Venous Thromboembolism Research Group Brigham and Women’s Hospital Boston, MA Welcome and Program Overview Jointly sponsored by the University of Florida College of Pharmacy and CMEducation Resources, LLC. Jointly sponsored by the University of Massachusetts Medical Center, office of CME and CMEducation Resources, LLC Commercial Support: Sponsored by an independent educational grant from Eisai, Inc. Mission statement: Improve patient care through evidence-based education, expert analysis, and case study-based management Processes: Strives for fair balance, clinical relevance, on-label indications for agents discussed, and emerging evidence and information from recent studies COI: Full faculty disclosures provided in syllabus and at the beginning of the program CEU Credit Designation Statement The University of Florida College of Pharmacy is accredited by the Accreditation Council for Pharmacy Education as a provider of continuing pharmacy education. The University of Florida College of Pharmacy will mail the Statements of Continuing Pharmacy Education Credit within 4 weeks after the course. To receive credit you must attend the sessions for which you want credit and complete an evaluation form. The College of Pharmacy will award 2 (two) continuing pharmacy education credits (2.0 CEU’s) upon completion of this program. Program Educational Objectives As a result of this session, attendees will be able to: ► List the recent trials, research, and expert analysis of issues focused on thrombosis and cancer. ► Outline specific strategies for risk-directed prophylaxis against DVT in at-risk patients with cancer. ► Describe dose anticoagulation therapy for patients requiring prophylaxis in special patient populations. ► Outline steps for avoiding medication errors using anticoagulation in cancer patients at risk for DVT. ► List the guidelines for DVT prophylaxis in cancer issued by the National Comprehensive Cancer Network (NCCN), the American College of Chest Physicians (ACCP), and the Surgeon General’s Report. Program Faculty Program Co-Chairs Edith Nutescu, PharmD, FCCP Distinguished Experts and Presenters John Fanikos, RPh, MBA Clinical Associate Professor, Pharmacy Practice Affiliate Faculty, Center for Pharmacoeconomic Research Director, Antithrombosis Center The University of Illinois at Chicago College of Pharmacy & Medical Center Chicago, IL Assistant Director of Pharmacy Brigham and Women’s Hospital Assistant Clinical Professor of Pharmacy Northeastern University Massachusetts College of Pharmacy Boston, MA Karen Fiumara, PharmD Samuel Z. Goldhaber, MD Professor of Medicine Harvard Medical School Cardiovascular Division Director, Venous Thromboembolism Research Group Brigham and Women’s Hospital Boston, MA Medication Safety Officer Brigham and Women’s Hospital Adjunct Assistant Professor of Pharmacy Practice Massachusetts College of Pharmacy and Allied Health Sciences Adjunct Assistant Professor of Pharmacy Practice Bouve’ College of Health Sciences Northeastern University Boston, MA Faculty COI Financial Disclosures Samuel Z. Goldhaber, MD Grant/Research Support: AstraZeneca; Boehringer-Ingelheim; Eisai; GSK; sanofi-aventis; Consultant: Boehringer-Ingelheim; BMS; Eisai; Merck; Pfizer; sanofi-aventis Edith Nutescu, PharmD Speakers Bureau: Eisai Inc., GlaxoSmithKline, sanofi-aventis U.S. Advisory Committees or Review Panels, Board Membership, etc.: Boehringer Ingelheim Pharmaceuticals, Inc., Scios Inc. Karen Fiumara, PharmD Nothing to disclose John Fanikos, RPh, MBA Speakers Bureau and Consulting: Abbott Laboratories, Astra-Zeneca, Eisai Pharmaceuticals, Genentech, GlaxoSmithKline, sanofi-aventis, The Medicines Company A Year 2009 Update for The Health System Pharmacist Cancer and Prevention of VTE Landmark Advances and New Paradigms of Care for the Health System Pharmacist Program Co-Chair Samuel Z. Goldhaber, MD Professor of Medicine Harvard Medical School Cardiovascular Division Director, Venous Thromboembolism Research Group Brigham and Women’s Hospital Boston, MA VTE and Cancer—A Looming National Healthcare Crisis MISSION AND CHALLENGES Recognizing cancer patients at risk for DVT and identifying appropriate candidates for long-term prophylaxis and/or treatment with approved and indicated therapies are among the most important challenges encountered in contemporary pharmacy and clinical practice. Comorbidity Connection COMORBIDITY CONNECTION SUBSPECIALIST STAKEHOLDERS CAP UTI Cancer Heart Failure ABE/COPD Respiratory Failure Myeloproliferative Disorder Thrombophilia Surgery History of DVT Other Infectious diseases Oncology PHARMACISTS Cardiology Pulmonary medicine Hematology Oncology/hematology Interventional Radiology Hospitalist Surgeons EM PCP Epidemiology of First-Time VTE Variable Finding Seasonal Variation Possibly more common in winter and less common in summer Risk Factors 25% to 50% “idiopathic” 15%-25% associated with cancer 20% following surgery (3 months) Recurrent VTE 6-month incidence, 7%; Higher rate in patients with cancer Recurrent PE more likely after PE than after DVT Death After Treated VTE 30-day incidence 6% after incident DVT 30-day incidence 12% after PE Death strongly associated with cancer, age, and cardiovascular disease White R. Circulation. 2003;107:I-4 –I-8.) Epidemiology of VTE ► One major risk factor for VTE is ethnicity, with a significantly higher incidence among Caucasians and African Americans than among Hispanic persons and Asian-Pacific Islanders. ► Overall, about 25% to 50% of patient with first-time VTE have an idiopathic condition, without a readily identifiable risk factor. ► Early mortality after VTE is strongly associated with presentation as PE, advanced age, cancer, and underlying cardiovascular disease. White R. Circulation. 2003;107:I-4 –I-8.) Comorbidity Connection Overview Comorbidity Connection Acute Medical Illness and VTE Multivariate Logistic Regression Model for Definite Venous Thromboembolism (VTE) Risk Factor Odds Ratio (95% CI) X2 Age > 75 years Cancer Previous VTE 1.03 (1.00-1.06) 1.62 (0.93-2.75) 2.06 (1.10-3.69) 0.0001 0.08 0.02 Acute infectious disease 1.74 (1.12-2.75) 0.02 Alikhan R, Cohen A, et al. Arch Intern Med. 2004;164:963-968 Comorbid Condition and DVT Risk ► Hospitalization for surgery (24%) and for medical illness (22%) accounted for a similar proportion of the cases, while nursing home residence accounted for 13%. ► The individual attributable risk estimates for malignant neoplasm, trauma, congestive heart failure, central venous catheter or pacemaker placement, neurological disease with extremity paresis, and superficial vein thrombosis were 18%, 12%, 10%, 9%, 7%, and 5%, respectively. ► Together, the 8 risk factors accounted for 74% of disease occurrence Heit JA, O'Fallon WM, Petterson TM, Lohse CM, Silverstein MD, Mohr DN, Melton LJ 3rd. Arch Intern Med. 2002 Jun 10;162(11):1245-8. Relative impact of risk factors for deep vein thrombosis and pulmonary embolism: a population-based study VTE Recurrence Predictors of First Overall VTE Recurrence Baseline Characteristic Hazard Ratio (95% CI) Age 1.17 (1.11-1.24) Body Mass Index 1.24 (1.04-1.7) Neurologic disease with extremity paresis 1.87 (1.28-2.73) Malignant neoplasm With chemotherapy Without chemotherapy Heit J, Mohr D, et al. Arch Intern Med. 2000;160:761-768 4.24 (2.58-6.95) 2.21 (1.60-3.06) ICOPER Cumulative Mortality 25 17.5% Mortality (%) 20 15 10 5 0 7 14 30 60 Days From Diagnosis Lancet 1999;353:1386-1389 90 Stages of Chronic Venous Insufficiency 1. Varicose veins 2. Ankle/ leg edema 3. Stasis dermatitis 4. Lipodermatosclerosis 5. Venous stasis ulcer Progression of Chronic Venous Insufficiency From UpToDate 2006 Rising VTE Incidence in Hospitalized Patients Stein PD et al. Am J Cardiol 2005; 95: 1525-1526 DVT Registry (N=5,451): Top 5 Medical Comorbidities 1. Hypertension 2. Immobility 3. Cancer 4. Obesity (BMI > 30) 5. Cigarette Smoking Am J Cardiol 2004; 93: 259-262 Implementation Implementation of VTE prophylaxis continues to be problematic, despite detailed North American and European Consensus guidelines. SURGEON GENERAL: CALL TO ACTION TO PREVENT DVT AND PE September 15, 2008 Surgeon General’s Call to Action 42-Page Document ► Issued September 15, 2008 ► Endorsed by Secretary, HHS ► Endorsed by Director, NHLBI ► Foreword by Acting Surgeon General, Steven K. Galson, MD, MPH (RADM, U.S. Public Health Service) Call to Action for VTE Foreword ► Dr. Galson’s 1st Call To Action ► > 350,000-600,000 Americans suffer VTE annually ► > 100,000 U.S. deaths per year ► Negative impact on QOL of survivors ► “Must disseminate info widely” to “address gap” because we’re not applying knowledge systematically Call to Action for VTE I. Major Public Health Problem II. Reducing VTE Risk III. Gaps in Application, Awareness of Evidence IV. Public Health Response V. Catalyst for Action Symposium Themes 1. Cancer rates are increasing as heart disease Rx improves and as cancer Rx improves. 2. Cancer increases VTE risk. 3. VTE is preventable (immunize!) 4. VTE prophylaxis may slow cancer 5. Increased emphasis on prophylaxis: OSG, NCCN, ASCO, ACCP, NATF 6. Facilitate prophylaxis with alerts. A Year 2009 Update for The Health System Pharmacist Cancer and Prevention of VTE Landmark Advances and New Paradigms of Care for the Health System Pharmacist Edith Nutescu, PharmD, FCCP Clinical Associate Professor Pharmacy Practice Affiliate Faculty, Center for Pharmacoeconomic Research Director, Antithrombosis Center The University of Illinois at Chicago College of Pharmacy & Medical Center Chicago, IL Peculiar Relationship Between Cancer and Thrombosis Hypercoagulation/ thrombosis may indicate Occult Cancer may cause Cancer Hypercoagulation/ thrombosis Thromboembolism in Malignancy 1. 2. 3. 4. ► 15% of cancer patients develop venous or arterial thrombosis1 ► Annual incidence of VTE in all patients: 117 in 100,0002 ► Cancer increases risk of thrombosis 4.1-fold3 ► Chemotherapy increases risk of thrombosis 6.5-fold3 ► Annual incidence of VTE in patients with cancer: 1 in 2004 Green KB, Silverstein RL. Hematol Oncol Clin North Am. 1996;10:499-530. Silverstein MD et al. Arch Intern Med. 1998;158:585-593 Heit JA et al. Arch Intern Med. 2000;160:809-815 Lee AYY, Levine MN. Circulation. 2003;107(23 Suppl 1):I17-21. Factors That May Affect Risk for Cancer-Associated VTE Patient-related factors Treatment-related factors ► Older age ► Recent surgery ► Comorbidities ► Hospitalization ► Chemotherapy ► Hormonal therapy Cancer-related factors ► Antiangiogenic agents ► Site of cancer ► Advanced stage ► Initial period after diagnosis ► Erythropoiesis-stimulating agents Biological factors (biomarkers) ► Elevated pre-chemotherapy platelet count ► D-dimer ► Tissue factor expression by tumor cells Rao MV, et al., In Khorana AA, Francis CW, eds. 2007 Risk of Inpatient VTE by Type of Cancer Rate of VTE, % 14 n=3550 n=68 n=326 n=43 n=51 n=55 n=127 n=95 12.10 12 9.50 10 8 6 n=53 8.96 7.00 7.41 6.75 7.64 5.37 4 2 0 In hospitalized neutropenic cancer patients Khorana AA et al. J Clin Oncol. 2006;24:484-490. 6.50 Risk of Inpatient VTE by Type of Cancer 7 Rate of VTE, % 6 N=3550 n=641 n=79 n=262 n=204 5.79 5.37 5 n=650 5.01 4.39 3.87 4 3.93 3 2 1 0 All Leukemia NHL Hodgkin’s Myeloma In hospitalized neutropenic cancer patients Khorana AA et al. J Clin Oncol. 2006;24:484-490. Breast Patients With Cancer Represent About 20% of All DVT and PE Patients with cancer: approximately 19.8% All DVT and PE Heit JA. et al. Arch Intern Med 2002;162:1245-1248. VTE, Cancer, and Survival N = 1,211,944 Medicare admissions with cancer vs 8,177,634 without cancer 1.00 Probability of Death DVT/PE and Malignant Disease 0.80 0.60 Malignant Disease 0.40 DVT/PE Only 0.20 Nonmalignant Disease 0.00 0 20 Levitan N, et al. Medicine 1999;78:285 40 60 80 100 120 Number of Days 140 160 180 VTE and Inpatient Mortality Mortality, % No Venous Thromboembolism 20 18 16 14 12 10 8 6 4 2 0 Venous Thromboembolism 16.13 14.85 10.59 7.98 All (n=66,016) Nonmetastatic Cancer (n=20,591) Khorana AA et al. J Clin Oncol. 2006;24:484-490. 16.41 8.67 Metastatic Cancer (n=17,360) Prophylaxis Rates in Hospitalized Patients Amin A et al. J Thromb Haemost. 2007; 5:1610-6. Patients Receiving Appropriate DVT Prophylaxis, % Thromboprophylaxis Is Underutilized in Non-surgical Patients With Cancer Premiere Perspective™ database: 72,391 discharges from 225 hospitals between January 2002 and September 2005 Amin AN et al. J Clin Oncol. 2007;25 (suppl):Abstract 9047. Clots and Cancer—A Looming National Healthcare Crisis MISSION AND CHALLENGES Recognizing cancer patients at risk for DVT and identifying patients who are appropriate candidates for long-term prophylaxis and/or treatment with approved and indicated therapies are among the most important and difficult challenges encountered in contemporary pharmacy and clinical practice. Clotting, Cancer, and Controversies A Systematic Analysis of VTE Prophylaxis in the Setting of Cancer Linking Science and Evidence to Clinical Practice—What Do Trials Teach the Health System Pharmacist? Program Co-Chairman Samuel Z. Goldhaber, MD Professor of Medicine Harvard Medical School Cardiovascular Division Director, Venous Thromboembolism Research Group Brigham and Women’s Hospital Boston, MA VTE and Cancer: Epidemiology ► Of all cases of VTE: ● ● ► Of all cancer patients: ● ● ► About 20% occur in cancer patients Annual incidence of VTE in cancer patients ≈ 1/250 15% will have symptomatic VTE As many as 50% have VTE at autopsy Compared to patients without cancer: ● ● ● Higher risk of first and recurrent VTE Higher risk of bleeding on anticoagulants Higher risk of dying Lee AY, Levine MN. Circulation. 2003;107:23 Suppl 1:I17-I21 DVT and PE in Cancer Facts, Findings, and Natural History ► VTE is the second leading cause of death in hospitalized cancer patients1,2 ► The risk of VTE in cancer patients undergoing surgery is 3to 5-fold higher than those without cancer2 ► Up to 50% of cancer patients may have evidence of asymptomatic DVT/PE3 ► Cancer patients with symptomatic DVT exhibit a high risk for recurrent DVT/PE that persists for many years4 1. Ambrus JL et al. J Med. 1975;6:61-64 2. Donati MB. Haemostasis. 1994;24:128-131 3. Johnson MJ et al. Clin Lab Haem. 1999;21:51-54 4. Prandoni P et al. Ann Intern Med. 1996;125:1-7 Clinical Features of VTE in Cancer ► VTE has significant negative impact on quality of life ► VTE may be the presenting sign of occult malignancy • • • 10% with idiopathic VTE develop cancer within 2 years 20% have recurrent idiopathic VTE 25% have bilateral DVT Bura et. al., J Thromb Haemost 2004;2:445-51 Thrombosis and Survival Likelihood of Death After Hospitalization 1.00 Probability of Death DVT/PE and Malignant Disease 0.80 0.60 Malignant Disease 0.40 DVT/PE Only 0.20 Nonmalignant Disease 0.00 0 20 40 60 80 100 120140 160 180 Number of Days Levitan N, et al. Medicine 1999;78:285 Mortality (%) Hospital Mortality With or Without VTE N=66,016 Khorana, JCO, 2006 N=20,591 N=17,360 Rate of VTE (%) Trends in VTE in Hospitalized Cancer Patients 7.0 6.5 6.0 5.5 5.0 4.5 4.0 3.5 3.0 2.5 2.0 1.5 1.0 0.5 0.0 P<0.0001 1995 1996 1997 VTE- patients on chemotherapy Khorana AA et al. Cancer. 2007. 1998 1999 2000 2001 VTE-all patients PE-all patients 2002 2003 DVT-all patients Thrombosis Risk In Cancer Primary Prophylaxis ► Medical Inpatients ► Surgery ► Radiotherapy ► Central Venous Catheters Risk Factors for Cancer-Associated VTE ► Cancer ● Type • Men: prostate, colon, brain, lung • Women: breast, ovary, lung ● ► Stage Treatments ● Surgery • 10-20% proximal DVT • 4-10% clinically evident PE • 0.2-5% fatal PE ● ● Chemotherapy Central venous catheters (~4% generate clinically relevant VTE) ► Patient ● ● ● Prior VTE Comorbidities Genetic background VTE Risk And Cancer Type “Solid And Liquid Malignancies” Relative Risk of VTE Ranged From 1.02 to 4.34 Relative Risk of VTE in Cancer Patients 4.5 4 3.5 3 2.5 2 1.5 1 Stein PD, et al. Am J Med 2006; 119: 60-68 Bladder Cervix Breast Leukemia Liver Ovary Colon Kidney Rectal Prostate Esophagus Lung Uterus Lymphoma Stomach Myeloprol Brain Pancreas 0.5 Cancer and Thrombosis Medical Inpatients Thromboembolism in Hospitalized Neutropenic Cancer Patients ►Retrospective cohort study of discharges using the University Health System Consortium ►66,106 adult neutropenic cancer patients between 1995 and 2002 at 115 centers Khorana, JCO, 2006 Neutropenic Patients: Results ►8% had thrombosis ►5.4% venous and 1.5% arterial in 1st hospitalization ►Predictors of thrombosis ● ● ● Age over 55 Site (lung, GI, gynecologic, brain) Comorbidities (infection, pulmonary and renal disease, obesity) Khorana, JCO, 2006 Predictors of VTE in Hospitalized Cancer Patients Characteristic OR P Value Site of Cancer Lung Stomach Pancreas Endometrium/cervix Brain 1.3 1.6 2.8 2 2.2 <0.001 0.0035 <0.001 <0.001 <0.001 Age 65 y 1.1 0.005 Arterial thromboembolism 1.4 0.008 Comorbidities (lung/renal disease, infection, obesity) 1.3-1.6 <0.001 Khorana AA et al. J Clin Oncol. 2006;24:484-490. Antithrombotic Therapy: Choices Nonpharmacologic (Prophylaxis) Intermittent Pneumatic Compression Elastic Stockings Inferior Vena Cava Filter Pharmacologic (Prophylaxis & Treatment) Unfractionated Heparin (UH) Low Molecular Weight Heparin (LMWH) Oral Anticoagulants New Agents: e.g. Fondaparinux, Direct anti-Xa inhibitors, Direct anti-IIa, etc.? Rate of VTE (%) Prophylaxis Studies in Medical Patients Relative risk reduction 63% Relative risk reduction 44% Placebo Enoxaparin Placebo Dalteparin MEDENOX Trial Francis, NEJM, 2007 PREVENT Relative risk reduction 47% Placebo Fondaparinux ARTEMIS ASCO Guidelines 1. SHOULD HOSPITALIZED PATIENTS WITH CANCER RECEIVE ANTICOAGULATION FOR VTE PROPHYLAXIS? Recommendation. Hospitalized patients with cancer should be considered candidates for VTE prophylaxis with anticoagulants in the absence of bleeding or other contraindications to anticoagulation. Lyman GH et al. J Clin Oncol (25) 2007; 34: 5490-5505. Cancer and Thrombosis Surgical Patients Incidence of VTE in Surgical Patients ► Cancer patients have 2-fold risk of post-operative DVT/PE and >3-fold risk of fatal PE despite prophylaxis: No Cancer Cancer N=16,954 N=6124 Post-op VTE 0.61% 1.26% <0.0001 Non-fatal PE 0.27% 0.54% <0.0003 Autopsy PE 0.11% 0.41% <0.0001 Death 0.71% 3.14% <0.0001 Kakkar AK, et al. Thromb Haemost 2001; 86 (suppl 1): OC1732 P-value Natural History of VTE in Cancer Surgery: The @RISTOS Registry ► Web-Based Registry of Cancer Surgery Tracked 30-day incidence of VTE in 2373 patients Type of surgery • 52% General • 29% Urological • 19% Gynecologic 82% received in-hospital thromboprophylaxis 31% received post-discharge thromboprophylaxis Findings ► 2.1% incidence of clinically overt VTE (0.8% fatal) ► Most events occur after hospital discharge ► Most common cause of 30-day post-op death Agnelli, Ann Surg 2006; 243: 89-95 Prophylaxis in Surgical Patients LMWH vs. UFH ► Abdominal or pelvic surgery for cancer (mostly colorectal) ► LMWH once daily vs. UFH tid for 7–10 days post-op ► DVT on venography at day 7–10 and symptomatic VTE Study N Design Regimens ENOXACAN 1 631 double-blind enoxaparin vs. UFH Canadian Colorectal DVT Prophylaxis 2 475 double-blind enoxaparin vs. UFH 1. ENOXACAN Study Group. Br J Surg 1997;84:1099–103 2. McLeod R, et al. Ann Surg 2001;233:438-444 Prophylaxis in Surgical Patients Incidence of Outcome Event 16.9% P=0.052 13.9% Canadian Colorectal DVT Prophylaxis Trial N=234 N=241 1.5% 2.7% VTE (Cancer) McLeod R, et al. Ann Surg 2001;233:438-444 Major Bleeding (All) Incidence of Outcome Event Extended Prophylaxis in Surgical Patients 12.0% ENOXACAN II P=0.02 N=167 5.1% 4.8% N=165 3.6% 1.8% 0.6% VTE Prox DVT 0% 0.4% NNT = 14 Any Major Bleeding Bleeding Bergqvist D, et al. (for the ENOXACAN II investigators) N Engl J Med 2002;346:975-980 Major Abdominal Surgery: FAME Investigators—Dalteparin Extended ► A multicenter, prospective, assessor-blinded, open-label, randomized trial: Dalteparin administered for 28 days after major abdominal surgery compared to 7 days of treatment ► RESULTS: Cumulative incidence of VTE was reduced from 16.3% with short-term thromboprophylaxis (29/178 patients) to 7.3% after prolonged thromboprophylaxis (12/165) (relative risk reduction 55%; 95% confidence interval 15-76; P=0.012). ► CONCLUSIONS: 4-week administration of dalteparin, 5000 IU once daily, after major abdominal surgery significantly reduces the rate of VTE, without increasing the risk of bleeding, compared with 1 week of thromboprophylaxis. Rasmussen, J Thromb Haemost. 2006 Nov;4(11):2384-90. Epub 2006 Aug 1. ASCO Guidelines: VTE Prophylaxis ► All patients undergoing major surgical intervention for malignant disease should be considered for prophylaxis. ► Patients undergoing laparotomy, laparoscopy, or thoracotomy lasting > 30 min should receive pharmacologic prophylaxis. ► Prophylaxis should be continued at least 7 – 10 days post-op. Prolonged prophylaxis for up to 4 weeks may be considered in patients undergoing major surgery for cancer with high-risk features. Lyman GH et al. J Clin Oncol (25) 2007; 34: 5490-5505. Central Venous Catheters Thrombosis is a potential complication of central venous catheters, including these events: –Fibrin sheath formation –Superficial phlebitis –Ball-valve clot –Deep vein thrombosis (DVT) Geerts W, et al. Chest Jun 2008: 381S–453S Prophylaxis for Venous Catheters Placebo-Controlled Trials Study Regimen N CRT (%) Reichardt* 2002 Dalteparin 5000 U daily placebo 285 140 11 (3.7) 5 (3.4) Couban* 2002 Warfarin 1mg daily placebo 130 125 6 (4.6) 5 (4.0) ETHICS† 2004 Enoxaparin 40 mg daily placebo 155 155 22 (14.2) 28 (18.1) *symptomatic outcomes; †routine venography at 6 weeks Reichardt P, et al. Proc ASCO 2002;21:369a; Couban S, et al, Blood 2002;100:703a; Agnelli G, et al. Proc ASCO 2004;23:730 Central Venous Catheters: Warfarin Tolerability of Low-Dose Warfarin ► 95 cancer patients receiving FU-based infusion chemotherapy and 1 mg warfarin daily ► INR measured at baseline and four time points ► 10% of all recorded INRs >1.5 ► Patients with elevated INR 2.0–2.9 6% 3.0–4.9 19% >5.0 7% Masci et al. J Clin Oncol. 2003;21:736-739 Prophylaxis for Central Venous Access Devices Summary ► Recent studies demonstrate a low incidence of symptomatic catheter-related thrombosis (~4%) ► Routine prophylaxis is not warranted to prevent catheter-related thrombosis, but catheter patency rates/infections have not been studied ► Low-dose LMWH and fixed-dose warfarin have not been shown to be effective for preventing symptomatic and asymptomatic thrombosis 8th ACCP Consensus Guidelines No routine prophylaxis to prevent thrombosis secondary to central venous catheters, including LMWH (2B) and fixed-dose warfarin (1B) Chest Jun 2008: 454S–545S Primary Prophylaxis in Cancer Radiotherapy The Ambulatory Patient ► No recommendations from ACCP ► No data from randomized trials (RCTs) ► Weak data from observational studies in high risk tumors (e.g. brain tumors; mucinsecreting adenocarcinomas: Colorectal, pancreatic, lung, renal cell, ovarian) ► Recommendations extrapolated from other groups of patients if additional risk factors present (e.g., hemiparesis in brain tumors, etc.) Cancer and Thrombosis Ambulatory Chemotherapy Patients Risk Factors for VTE in Medical Oncology Patients ► Tumor ● Ovary, brain, pancreas, lung, colon ► Stage, ● ► grade, and extent of cancer Metastatic disease, venous stasis due to bulky disease Type of antineoplastic treatment ● ► type Multiagent regimens, hormones, anti-VEGF, radiation Miscellaneous VTE risk factors ● Previous VTE, hospitalization, immobility, infection, thrombophilia Independent Risk Factors for DVT/PE Risk Factor/Characteristic O.R. Recent surgery with institutionalization 21.72 Trauma 12.69 Institutionalization without recent surgery 7.98 Malignancy with chemotherapy 6.53 Prior CVAD or pacemaker 5.55 Prior superficial vein thrombosis 4.32 Malignancy without chemotherapy 4.05 Neurologic disease w/ extremity paresis 3.04 Serious liver disease 0.10 Heit JA et al. Thromb Haemost. 2001;86:452-463 VTE Incidence In Various Tumors Oncology Setting VTE Incidence Breast cancer (Stage I & II) w/o further treatment 0.2% Breast cancer (Stage I & II) w/ chemo 2% Breast cancer (Stage IV) w/ chemo 8% Non-Hodgkin’s lymphomas w/ chemo 3% Hodgkin’s disease w/ chemo 6% Advanced cancer (1-year survival=12%) 9% High-grade glioma 26% Multiple myeloma (thalidomide + chemo) 28% Renal cell carcinoma 43% Solid tumors (anti-VEGF + chemo) 47% Wilms tumor (cavoatrial extension) 4% Otten, et al. Haemostasis 2000;30:72. Lee & Levine. Circulation 2003;107:I17 Primary VTE Prophylaxis ►Recommended for hospitalized cancer patients ►Not recommended or generally used for outpatients ● ● Very little data Heterogeneous Need for risk stratification Ambulatory Cancer plus Chemotherapy Study Methods ► Prospective observational study of ambulatory cancer patients initiating a new chemotherapy regimen, and followed for a maximum of 4 cycles ► 115 U.S. centers participated ► Patients enrolled between March, 2002 and August, 2004 who had completed at least one cycle of chemotherapy were included in this analysis Khorana, Cancer, 2005 Ambulatory Cancer plus Chemotherapy Study Methods ► VTE events were recorded during mid-cycle or new-cycle visits ► Symptomatic VTE was a clinical diagnosis made by the treating clinician ► Statistical analysis ● ● Odds ratios to estimate relative risk Multivariate logistic regression to adjust for other risk factors Khorana, Cancer, 2005 Incidence of VTE Rate of VTE (%) 3.0% 2.5% 2.0% 1.5% 1.0% 0.5% 0.0% Baseline Cycle 1 Cycle 2 Cycle 3 VTE / 2.4 months VTE/month VTE /cycle Cumulative rate (95% CI) 1.93% 0.8% 0.7% 2.2% (1.7-2.8) Khorana, Cancer, 2005 VTE (%) / 2.4 months Risk Factors: Site of Cancer 12 10 8 6 4 2 0 Site of Cancer Khorana, Cancer, 2005 Incidence of Venous Thromboembolism By Quartiles of Pre-chemotherapy Platelet Count Incidence Of VTE Over 2.4 Months(%) 5.0% p for trend=0.005 4.5% 4.0% 3.5% 3.0% 2.5% 2.0% 1.5% 1.0% 0.5% 0.0% <217 217-270 270-337 Pre-chemotherapy Platelet Count/mm Khorana, Cancer, 2005 >337 3 (x1000) Risk Factors: Multivariate Analysis Characteristic OR Site of Cancer P value 0.03 Upper GI 3.88 0.0076 Lung 1.86 0.05 Lymphoma Pre-chemotherapy platelet count > 350,000/mm3 Hgb < 10g/dL or use of red cell growth factor Use of white cell growth factor in highrisk sites 1.5 0.32 2.81 0.0002 1.83 0.03 2.09 0.008 Khorana, Cancer, 2005 Predictive Model Patient Characteristic Score Site of Cancer Very high risk (stomach, pancreas) 2 High risk (lung, lymphoma, gynecologic, GU excluding prostate) 1 Platelet count > 350,000/mm3 1 Hgb < 10g/dL or use of ESA 1 Leukocyte count > 11,000/mm3 1 BMI > 35 1 Khorana AA et al. JTH Suppl Abs O-T-002 Incidence of VTE Over 2.4 Months Predictive Model Actual Incidence Estimated Incidence 95 % Confidence Limits 18% 16% 14% 12% 10% 8% 6% 4% 2% 0% 0 1 2 3 4 Risk Score 0 1 2 3 4 N 1,352 974 476 160 33 VTE(%) /2.4 mos. 0.8 1.8 2.7 6.3 13.2 Predictive Model Validation Rate of VTE over 2.5 mos (%) 8% 7.1% 7% Development cohort 6% Validation cohort 6.7% 5% 4% 3% 1.8% 2.0% 2% 1% 0.8% 0.3% 0% n=734 n=374 Risk Low (0) Khorana AA et al. JTH Suppl Abs O-T-002 n=1627 n=842 Intermediate(1-2) n=340 n=149 High(>3) Oral Anticoagulant Therapy in Cancer Patients: Problematic ► Warfarin ● ● ● ● ► therapy is complicated by: Difficulty maintaining tight therapeutic control, due to anorexia, vomiting, drug interactions, etc. Frequent interruptions for thrombocytopenia and procedures Difficulty in venous access for monitoring Increased risk of both recurrence and bleeding Is it reasonable to substitute long-term LMWH for warfarin ? When? How? Why? CLOT: Landmark Cancer/VTE Trial Dalteparin Dalteparin CANCER PATIENTS WITH Randomization ACUTE DVT or PE [N = 677] ► ► Dalteparin Oral Anticoagulant Primary Endpoints: Recurrent VTE and Bleeding Secondary Endpoint: Survival Lee, Levine, Kakkar, Rickles et.al. N Engl J Med, 2003;349:146 Landmark CLOT Cancer Trial Probability of Recurrent VTE, % Reduction in Recurrent VTE 25 Recurrent VTE Risk reduction = 52% p-value = 0.0017 20 OAC 15 10 Dalteparin 5 0 0 Lee, Levine, Kakkar, Rickles et.al. N Engl J Med, 2003;349:146 30 60 90 120 150 Days Post Randomization 180 210 Bleeding Events in CLOT Dalteparin OAC N=338 N=335 Major bleed 19 ( 5.6%) 12 ( 3.6%) 0.27 Any bleed 46 (13.6%) 62 (18.5%) 0.093 * Fisher’s exact test Lee, Levine, Kakkar, Rickles et.al. N Engl J Med, 2003;349:146 P-value* Treatment of Cancer-Associated VTE Study Design Length of Therapy (Months) N Recurrent Major Death VTE Bleeding (%) (%) (%) 6 4 NS 39 NS 41 0.09 7 16 0.09 11 0.03 23 0.03 6 8 NS 23 NS 22 CLOT Trial (Lee 2003) Dalteparin OAC 6 336 336 9 17 0.002 CANTHENOX (Meyer 2002) Enoxaparin OAC 3 67 71 11 21 LITE (Hull ISTH 2003) Tinzaparin OAC 3 80 87 6 11 ONCENOX (Deitcher ISTH 2003) Enox (Low) Enox (High) OAC 6 32 36 34 3.4 3.1 6.7 NS NS NR Treatment and 2° Prevention of VTE in Cancer – Bottom Line New Development ► New standard of care is LMWH at therapeutic doses for a minimum of 3-6 months (Grade 1A recommendation—ACCP) ► NOTE: Dalteparin is only LMWH approved (May, 2007) for both the treatment and secondary prevention of VTE in cancer ► Oral anticoagulant therapy to follow for as long as cancer is active (Grade 1C recommendation—ACCP) Chest Jun 2008: 454S–545S CLOT 12-month Mortality All Patients Probability of Survival, % 100 90 80 70 Dalteparin 60 OAC 50 40 30 20 10 0 HR 0.94 P-value = 0.40 0 30 60 90 120 180 240 300 Days Post Randomization Lee AY et al. J Clin Oncol. 2005; 23:2123-9. 360 Anti-Tumor Effects of LMWH CLOT 12-month Mortality Patients Without Metastases (N=150) Probability of Survival, % 100 Dalteparin 90 80 70 OAC 60 50 40 30 20 10 HR = 0.50 P-value = 0.03 0 0 30 60 90 120 150 180 240 300 Days Post Randomization Lee AY et al. J Clin Oncol. 2005; 23:2123-9. 360 LMWH for Small Cell Lung Cancer Turkish Study ► 84 patients randomized: Chemo +/- LMWH (18 weeks) ► Patients balanced for age, gender, stage, smoking history, ECOG performance status Chemotherapy plus Dalteparin Chemo alone P-value 1-y overall survival, % 51.3 29.5 0.01 2-y overall survival, % 17.2 0.0 0.01 Median survival, m 13.0 8.0 0.01 CEV = cyclophosphamide, epirubicin, vincristine; LMWH = Dalteparin, 5000 units daily Altinbas et al. J Thromb Haemost 2004;2:1266. Rate of Appropriate Prophylaxis, % VTE Prophylaxis Is Underused in Patients With Cancer Cancer: FRONTLINE Survey1— 3891 Clinician Respondents Cancer: Surgical Major Surgery2 Major Abdominothoracic Surgery (Elderly)3 Medical Inpatients4 Confirmed DVT (Inpatients)5 Cancer: Medical 1. Kakkar AK et al. Oncologist. 2003;8:381-388 4. Rahim SA et al. Thromb Res. 2003;111:215-219 2. Stratton MA et al. Arch Intern Med. 2000;160:334-340 3. Bratzler DW et al. Arch Intern Med. 1998;158:1909-1912 5. Goldhaber SZ et al. Am J Cardiol. 2004;93:259-262 Conclusions and Summary ► Risk factors for VTE in the setting of cancer have been well characterized: solid tumors, chemotherapy, surgery, thrombocytopenia ► Long-term secondary prevention with LMWH has been shown to produce better outcomes than warfarin ► Guidelines and landmark trials support administration of LMWH in at risk patients ► Cancer patients are under-prophylaxed for VTE ► Health system pharmacists can play a pivotal role in improving clinical outcomes in this patient population Clotting, Cancer, and Clinical Strategies Venous Thromboembolism (VTE) Prophylaxis in the Cancer Patient and Beyond Guidelines and Implications for Clinical Practice John Fanikos, RPh, MBA Assistant Director of Pharmacy Brigham and Women’s Hospital Assistant Clinical Professor of Pharmacy Northeastern University Massachusetts College of Pharmacy Boston, MA Outline of Presentation ► Guidelines for VTE prevention ► Performance to date ► Opportunities for improvement ► Guidelines for VTE Treatment ► Performance to date Prophylaxis Rates in Hospitalized Patients Amin A et al. J Thromb Haemost. 2007; 5:1610-6. VTE, Cancer, and Survival N = 1,211,944 Medicare admissions with cancer vs 8,177,634 without cancer 1.00 Probability of Death DVT/PE and Malignant Disease 0.80 0.60 Malignant Disease 0.40 DVT/PE Only 0.20 Nonmalignant Disease 0.00 0 20 Levitan N, et al. Medicine 1999;78:285 40 60 80 100 120 Number of Days 140 160 180 Time Distribution of VTE Events Following Cancer Surgery @RISTOS Registry: prospective cohort N=2373 12 10 VTE Events 8 6 4 2 0 1-5 d Agnelli G et al. Ann Surg 2006; 243:89-95. 6-10 d 11-15 d 16-20 d 21-25 d 26-30 d > 30 d • www.nccn.org • NCCN Clinical Practice Guidelines in Oncology™ • “…The panel of experts includes medical and surgical oncologists, hematologists, cardiologists, internists, radiologists. And a pharmacist.” • www.asco.org •Recommendations for VTE Prophylaxis & Treatment in Patients with Cancer 2004 ACCP Recommendations Cancer patients undergoing surgical procedures receive prophylaxis that is appropriate for their current risk state (Grade 1A) ● General, Gynecologic, Urologic Surgery • Low Dose Unfractionated Heparin 5,000 units TID • LMWH > 3,400 units Daily – Dalteparin 5,000 units – Enoxaparin 40 mg – Tinzaparin 4,500 units • GCS and/or IPC Cancer patients with an acute medical illness receive prophylaxis that is appropriate for their current risk state (Grade 1A) • Low Dose Unfractionated Heparin • LMWH Contraindication to anticoagulant prophylaxis (Grade 1C+) • GCS or IPC 1A is the highest possible grade Indicates that benefits outweigh risks, burdens, and costs, with consistent RCT level of evidence Geerts WH et al. Chest. 2004;126(suppl):338S-400S NCCN Practice Guidelines in VTE Disease At Risk Population ► ► ► ► ► ► ► ► ► ► ► ► ► ► Adult patient Diagnosis or clinical suspicion of cancer Inpatient Relative contraindication to anticoagulation treatment RISK FACTOR ASSESSMENT Age Prior VTE Familial thrombophilia Active cancer Trauma Major surgical procedures Acute or chronic medical illness requiring hospitalization or prolonged bed rest Central venous catheter/IV catheter Congestive heart failure Pregnancy Regional bulky lymphadenopathy with extrinsic vascular compression http://www.nccn.org/professionals/physician_gls/PDF/vte.pdf Initial Prophylaxis Continue Prophylaxis After Modifiable risk factors: Lifestyle, Discharge ? smoking, tobacco, obesity, Prophylactic anticoagulation therapy (category 1) + sequential compression device (SCD) Mechanical prophylaxis (options) - SCD - Graduated compression stockings activity level/exercise ► ► ► AGENTS ASSOCIATED WITH INCREASED RISK Chemotherapy Exogenous estrogen compounds - HRT - Oral contraceptives - Tamoxifen/Raloxifene - Diethystilbestrol Thalidomide/lenalidomide NCCN Practice Guidelines in VTE Disease Inpatient Prophylactic Anticoagulation Therapy ► LMWH - Dalteparin 5,000 units subcutaneous daily - Enoxaparin 40 mg subcutaneous daily - Tinzaparin 4,500 units (fixed dose) subcutaneous daily or 75 units/kg subcutaneous daily ► Pentasaccharide - Fondaparinux 2.5 mg subcutaneous daily ► Unfractionated heparin 5,000 units subcutaneous 3 times daily http://www.nccn.org/professionals/physician_gls/PDF/vte.pdf NCCN Practice Guidelines in VTE Disease Relative Contraindications to Prophylactic or Therapeutic Anticoagulation ► ► ► ► ► ► ► ► ► Recent CNS bleed, intracranial or spinal lesion at high risk for bleeding Active bleeding (major): more than 2 units transfused in 24 hours Chronic, clinically significant measurable bleeding > 48 hours Thrombocytopenia (platelets < 50,000/mcL) Severe platelet dysfunction (uremia, medications, dysplastic hematopoiesis) Recent major operation at high risk for bleeding Underlying coagulopathy Clotting factor abnormalities - Elevated PT or aPTT (excluding lupus inhibitors) - Spinal anesthesia/lumbar puncture High risk for falls http://www.nccn.org/professionals/physician_gls/PDF/vte.pdf ► Should hospitalized patients with cancer receive anticoagulation for VTE prophylaxis ? ● “Hospitalized patients with cancer should be considered candidates for VTE prophylaxis in the absence of bleeding or other contraindications to anticoagulation” Lyman GH et al. J Clin Oncol (25) 2007; 34: 5490-5505. Incidence and Relative Risk of High-Grade VTE with Bevacizumab Tumor Type No. Studies Overall 13 Bevacizumab Control Incidence RR 235/3795 134/3167 6.3 1.38 Colo-rectal 4 96/1315 50/1128 7.3 1.56 NSCLC 4 78/1228 41/862 6.6 1.24 Breast Cancer Renal Cell 2 20/594 13/561 3.9 1.47 1 7/337 2/304 2.0 2.86 Mesothelioma 1 9/53 5/55 17.0 1.89 Pancreatic Cancer 1 24/268 23/257 9.0 1.00 SR Nalluri et al. JAMA 2008;300(19):2277-2285 ► Should ambulatory patients with cancer receive anticoagulation for VTE prophylaxis during systemic chemotherapy? ● “Routine prophylaxis is not recommended.” ● “Patients receiving thalidomide or lenalidomide with chemotherapy or dexamethasone are at high risk for thrombosis and warrant prophylaxis.” Lyman GH et al. J Clin Oncol (25) 2007; 34: 5490-5505. ► Should hospitalized patients with cancer undergoing surgery receive perioperative VTE prophylaxis ? ● All patients should be considered for thromboprophylaxis. Procedures greater than 30 minutes should receive pharmacologic prophylaxis. Mechanical methods should not be used as monotherapy. Prophylaxis should continue for at least 7-10 days post-op. Prolonged prophylaxis may be considered for cancer with high risk features. ● ● ● Lyman GH et al. J Clin Oncol (25) 2007; 34: 5490-5505. Compliance With ACCP VTE Prophylaxis Guidelines Is Poor Compliance With VTE Prophylaxis Guidelines in Hospitals by Patient Group 62,012 70,000 At risk for DVT/PE 35,124 Received compliant care Number of patients 10,000 9175 5,000 2324 1388 52.4% 15.3% 12.7% Orthopedic Surgery At-risk Medical Conditions General Surgery 9.9% 6.7% 0 Urologic Surgery Gynecologic Surgery Data collected January 2001 to March 2005; 123,340 hospital admissions. Compliance assessment was based on the 6th American College of Chest Physicians (ACCP) guidelines. HT Yu et al. Am J Health-Syst Pharm 2007; 64:69-76 Reasons for Inadequate Duration of VTE Prophylaxis At-Risk Medical (n=5,994) Abdominal Surgery (n=3,240) Urologic surgery (n=158) Gynecologic surgery (n=163) Neurosurgery (n=250) Started Late Started late & Ended Early Ended Early 1,347 (22.5) 2,961 (49.4) 1,686 (28.1) 824 (25.4) 1,764 (54.4) 652 (20.1) 18 (11.4) 73 (46.2) 67 (42.4) 13 (8.0) 43 (26.4) 107 (65.6) 66 (26.4) 125 (50.0) 59 (23.6) HT Yu et al. Am J Health-Syst Pharm 2007; 64:69-76 Predictors of the Use of Thromboprophylaxis Effect Odds Ratio (95% CI) Malignancy 0.40 Others 0.58 Infection 0.83 Bleeding Risk 0.91 Gender Hospital Size 0.92 0.93 Age 1.00 LOS 1.05 Cardiovascular Disease 1.06 Internal Medicine 1.33 Respiratory 1.35 AMC Duration of Immobility VTE Risk Factors 1.46 1.60 1.78 0.0 0.5 1.0 Kahn SR et Al. Thromb Res 2007; 119:145-155 1.5 2.0 2.5 Odds Ratio 3.0 3.5 4.0 Unfractionated Heparin Prophylaxis: BID vs TID—What Works, What Doesn’t? Meta-analysis: 12 RCTs ► DVT, PE, all VTE events, Bleeding ► Proximal ● ● DVT plus PE BID VTE event rate: 2.34 events per 1,000 patient days TID event rate: 0.86 events per 1,000 patient days P=0.05 ► NNT ● ● 676 hospital prophylaxis days with UFH TID to prevent 1 major bleed with 1,649 hospital prophylaxis days of TID dosing King CS et al. CHEST 2007;131:507-516 Heparin, Low Molecular Weight Heparin Prophylaxis ► Meta-analysis LMWH vs UFH ► 36 DVT randomized controlled trials Risk Study Reduction (95% CI) Weight % hospitalized medical patients ► UFH 5,000 units TID is more effective in preventing DVT than UFH BID Harenberg et al, 1990 0.70 (0.16-3.03) 3.4 Turpie et al, 1992 0.29 (0.10-0.81) 11.4 Dumas et al, 1994 0.74 (0.38-1.43) 14.4 Bergmann & Neuhart 0.94 (0.39-2.26) 8.1 Lechler et al, 1996 0.25 (0.03-2.23) 3.3 ► Low Hillbom et al, 2002 0.55 (0.31-0.98) 20.5 Kleber, et al 2003 0.77 (0.43-1.38) 19.4 Diener et al, 2006 0.76 (0.42-1.38) 18.9 Overall (95% CI) 0.68 (0.52-0.88) ► 23,000 molecular weight heparin is 33% more effective than unfractionated heparin in preventing DVT ● RR for DVT 0.68 et al, 1996 Harenberg et al, 1996 (p=0.004) 2.89 (0.30-27.71) 0.1 1.0 Risk Ratio LMWH Better Wein L et al. Arch Intern Med. 2007;167:1476-86. 10 LMWH Worse 0.8 BWH/DFCI Partners Cancer Care Experience • Consecutive patients, < 60 days • 2 Nursing units • LOS ranged from 3 days to 31 days • Number of days where doses were omitted ranged from 1 to 6 days VTE Incidence: More Common in the Outpatient Setting ► Medical records of residents (n=477,800) ► 587 VTE events (104 per 100,000 population) ► 30 Day recurrence 4.8 % Patients receiving prophylaxis during high risk periods VTE Event Location Spencer FA, et al. Jour Gen Int Med 2006; 21 (7):722-777 Thrombosis in Malignancy 7TH ACCP Consensus Conference Recommendations Initial Phase Chronic Phase 5-7 days Dalteparin 200/kg q24h (GRADE 1A) Continue anticoagulation (warfarin or LMWH) long-term or until malignancy resolves (GRADE 1C) 5 - 7 days 3 - 6 mos 6 mos - indefinite Subacute Phase 3 - 6 months Dalteparin* 150 units/kg q24h (GRADE 1A) * Dalteparin Approved for Extended Treatment to Reduce the Recurrence of Blood Clots in Patients with Cancer Buller HR, et al. Chest 2004; 126 (suppl 3): 401s-428s Warfarin vs. Dalteparin for VTE Treatment in Malignancy Recurrent Thrombosis Dalteparin: 200 units/kg/day x 1 mo, then 150 units/kg/day Warfarin dosed to INR 2-3 Thromboembolism (%) Dalteparin: 9.0% of 336 Warfarin: 17% of 336 Probability of Recurrent Venous 25 P=0.002 20 Oral anticoagulant 15 10 Dalteparin 5 0 Duration: 6 months 0 30 60 90 120 150 180 210 Days after Randomization No. at Risk Lee AY et al. New Engl J Med 2003; 349:146-53. Dalteparin 336 301 264 235 227 210 164 Oral anticoagulant 336 280 242 221 200 194 154 Subgroup Analysis 12-month Cumulative Mortality Rate Dalteparin Warfarin P Value Metastatic Disease (n=452) 72% 69% P = 0.46 Non-metastatic Disease (n=150) 20% 36% P=0.03 Lee AY et al. J Clin Oncol. 2005; 23:2123-9. Dalteparin Cost Effectiveness in Recurrent VTE Cost Parameter Dalteparin (n=338) Warfarin (n=338) Drug 2852 269 Laboratory 303 437 Diagnostic Tests 253 267 Unscheduled Visits 286 300 Transfusions 143 208 Major bleeding 97.5 92.3 VTE Recurrence 228 429 Mean Cost Per Patient 4162 2003 Dranitsaris G. Pharmacoeconomics 2006; 24(6):5093-607 NCCN Practice Guidelines—Venous Thromboembolic Disease Therapeutic Anticoagulation Treatment for DVT, PE, and Catheter-Associated Thrombosis Immediate ► LMWH - Dalteparin (200 units/kg subcutaneous daily) - Enoxaparin (1 mg/kg subcutaneous every 12 hrs) - Tinzaparin (175 units/kg subcutaneous daily) ► Pentasaccharide - Fondaparinux (5.0 mg [<50 kg]; 7.5 mg [50-100 lg]; 10 mg [>100 kg] subcutaneous daily ► Unfractionated heparin (IV) (80 units/kg load, then 18 units kg/hour, target aPTT to 2.0-2.9 x control) http://www.nccn.org/professionals/physician_gls/PDF/vte.pdf NCCN Practice Guidelines—Venous Thromboembolic Disease Therapeutic Anticoagulation Treatment for DVT, PE, and Catheter-Associated Thrombosis Long Term ► ► LMWH is preferred as monotherapy without warfarin in patients with proximal DVT or PE and prevention of recurrent VTE in patients with advanced or metastatic cancer Warfarin (2.5-5 mg every day initially, subsequent dosing based on INR value; target INR 2.0-3.0) Duration of Long Term Therapy ► ► ► Minimum time of 3-6 mo for DVT and 6-12 mo for PE Consider indefinite anticoaugulation if active cancer or persistent risk factors For catheter associated thrombosis, anticoagulate as long as catheter is in place and for 1-3 mo after catheter removal http://www.nccn.org/professionals/physician_gls/PDF/vte.pdf ► What is the best treatment for patients with cancer with established VTE to prevent recurrent VTE ? ● LMWH is the preferred approach for the initial 5-10 days. LMWH, given for at least 6 months, is the preferred for long-term anticoagulant therapy. After 6 months, anticoagulation therapy should be considered for select patients. For CNS malignancies, elderly patients anticoagulation is recommended with careful monitoring and dose adjustment. ● ● ● Lyman GH et al. J Clin Oncol (25) 2007; 34: 5490-5505. ► Should patients with cancer receive anticoagulants in the absence of established VTE to improve survival? ● “Anticoagulants are not recommended to improve survival in patients with cancer without VTE.” Lyman GH et al. J Clin Oncol (25) 2007; 34: 5490-5505. Antithrombotic Therapy Practices in U.S. Hospitals ►Survey of 38 U.S. Hospitals ►n=939 DVT or PE ►50% patients reached INR >2 for 2 consecutive days Therapy n (%) LMWH 527 (56.1%) UFH 562 (59.8%) UFH SC 78 (8.3%) DTI 6 (0.6%) Tapson V et al. Arch Intern Med 2005 Self-Managed Long Term LMWH Therapy 2212 patients with proximal vein thrombosis assessed for eligibility 737 Randomized 369 assigned to LMWH 1475 excluded for anticoagulant violations or inability to give written consent 369 assigned to usual care with heparin and warfarin 3 lost to follow-up 3 lost to follow-up 1 withdrew consent 5 withdrew consent 369 included in analysis Hull R. Am Jour Med 2007; 120:72-82 369 included in analysis Self-Managed Long Term LMWH Therapy Tinzaparin Usual Care Absolute Difference (n=369) (n=368) (95% CI) New VTE at 3 Mos 18 (4.9) 21 (5.7) -0.8 (-4.2-2.4) NS New VTE at 12 Mos 33 (8.9) 36 (9.8) -0.8 (-5.5-3.5) NS All Bleeding 48 (13.0) 73 (19.8) -6.8 (-12.4--1.5) p=.011 Major Bleeding 12 (3.3) 17 (4.6) -1.4 (-4.3-1.4) NS Minor Bleeding 36 (9.8) 56 (15.2) -5.5 (-10.4--0.6) p=.022 Stratified BleedingHigh Risk 31/144 (21.5) 39/146 (26.7) -5.2 (-15%-4.6%) NS Stratified Bleeding-Low Risk 17/225 (7.6) 34/222 (15.3) -7.8 (-13.6--1.9%) p=.01 Thrombocytopenia (<150) 21 (5.7) 9 (2.4) 1.6 (-3.6-0.3) NS Bone Fracture 4 (1.1) 7 (1.9) -0.8 (-0.9-2.6) NS Outcomes Hull R. Am Jour Med 2007; 120:72-82 p-value LMWHs and Bleeding in Patients with Renal Dysfunction Dosage adjustments for renal dysfunction Lim W et al. Ann Intern Med 2006; 144:673-84 Barriers to Long-term Use of LMWH for Treatment of Cancer-associated VTE Initial treatment LMWH for 3-6 months UFH/LMWH for 5-7 days followed by warfarin 19% 81% Reasons LMWH not used long-term Not covered by medical insurance Physician preference Patient refused long-term injections History of HIT Severe renal insufficiency Wittkowsky AK. J Thromb Haemost. 2006; 4:2090-1. 49.4% 32.0% 13.6% 2.5% 2.5% Conclusions Examine your current practices of VTE prophylaxis and treatment ► Review available guidelines as a benchmark ► Consider the use of a pharmacologic or mechanical intervention ► Evaluate use of Reminder or Risk Scoring Systems ► Utilize the regimen providing the best efficacy in reducing events and offering best compliance ► Follow-up with patients to monitor and avoid adverse events and to ensure optimal outcomes A Year 2009 Update for The Health System Pharmacist Pharmacologic Prophylaxis of DVT in Special Populations Edith Nutescu, PharmD, FCCP Clinical Associate Professor Pharmacy Practice Affiliate Faculty, Center for Pharmacoeconomic Research Director, Antithrombosis Center The University of Illinois at Chicago College of Pharmacy & Medical Center Chicago, IL Objectives 1. Differentiate data with various LMWHs in special populations 2. Review appropriate dosing and monitoring of LMWHs in patients with obesity and renal failure 3. Discuss cautions of using emerging agents in special populations Risk of Inadequate Therapy in High Risk Patients ► 524 VTE Patients ● Active Cancer in 26% • Only 1/3rd on LMWH monotherapy ● Weight > 100Kg in 15% • Under-dosing of LMWH by > 10% – 36% of > pts 100Kg – 8% of pts < 100Kg (p < 0.001) ● CrCL < 30mL/min in 5% • LMWH tx in 67% Cook LM, et.al. J Thromb Hemost 2007;5;937-41. 8th ACCP Conference on Antithrombotic Therapy Obese Patients “In obese patients given LMWH prophylaxis or treatment, we suggest weight-based dosing (Grade 2C).” ► What is this weight-based dosing and how does it differ from typical dosing? ► At what weight do we move away from standard dosing and move to weight-based dosing? Hirsh J et al. Chest. 2008;133(suppl):141S-159S. Pharmacokinetic Characteristics of Low Molecular Weight Heparins Lipid solubility LOW Plasma protein binding HIGH Tissue binding LOW Volume of Distribution 5-7 L Logical conclusion: IBW may be a better predictor of LMWH dosing than TBW LMWH: Maximum Weights Studied Kinetic Studies Clinical Trials Dalteparin 190 kg 128 kg* Enoxaparin 144 kg 194 kg Tinzaparin 165 kg 88 kg Fondaparinux * max dose 18,000 - 20,000 IU/day Duplaga BA et al. Pharmacotherapy 2001; 21:218-34. Synergy Trial: Data on File Davidson, et al. J Thromb Haem 2007;5:1191-4 175.5 kg LMWH Pharmacokinetics in Obesity Actual body weight correlates best with anticoagulant response to LMWHs as measured by anti-factor Xa levels Clin Pharmacol Ther 2002;72:308-18. Thromb Haemost 2002;87:817-23. Dalteparin Pharmacokinetics in Obesity Dose: 200 U/kg qd Duration: routine Obese (BMI > 30) Normal (BMI < 30) 10 10 TBW (mean +/- SD) 106.4 +/- 22.1 69.7 +/- 9.3 LBW (mean +/- SD) 64.1 +/- 12.3 66.1 +/- 8.7 Mean Vd (l) 12.39 8.36 Mean CI (l/hr) 1.30 1.11 N Yee JYV, Duffull SB. Eur J Clin Pharmacol 2000; 56:293-7. Dalteparin Pharmacokinetics In Obesity Correlation Coefficient Between Vd and: LBW 0.05 ABW 0.52 TBW 0.55 Correlation Coefficient Between Cl and: LBW 0.01 ABW 0.32 TBW 0.39 Conclusion: TBW may be a better predictor of LMWH dose than IBW Yee JYV et al. Eur J Clin Pharmacol 2000; 56:293-7. Dalteparin Pharmacokinetics In Obesity Dose: 200 U/kg qd Duration: 5 Days <20% of IBW 20-40% of IBW > 40% of IBW N 13 14 10 Mean Dose (U) 14,030 17,646 23,565 Day 3 Peak 1.01 0.97 1.12 NS Day 3 Trough 0.12 0.11 0.11 NS Max TBW: 190kg Ant-Xa Activity (u/ml) Conclusion: Body mass does not appear to have an important effect on the response to LMWH up to a weight of 190kg in patients with normal renal function. Wilson SJ et al. Hemostasis 2001; 31:42-8. LMWH Safety and Effectiveness Using TBW Enoxaparin In ACS (ESSENCE/TIMI IIb) P=0.39 16.1% 14.3% P=0.13 1.6% 0.4% Obese: BMI > 30mg/m2 Enox max weight 158 kg Spinler SA et al. Am Heart J 2003; 146:33-41 Safety Of TBW-based Dosing of Dalteparin for Treatment of Acute VTE in Obese Patients N = 193 patients > 90 kg 3 month outcomes: major bleeding = 1.0% (n=2) recurrent VTE = 1.6% (n=3) WEIGHT (kg) N Mean Dose Full dose +/- 5% QD Dosing BID Dosing 90-99 40 19,300 39 24 16 100-109 52 20,850 49 25 17 110-119 41 21,470 21 26 15 120-129 25 24,300 22 16 9 130-139 16 25,250 8 10 6 140-149 9 26,920 6 5 4 > 150 10 28,280 6 6 4 Al-Yaseen E et al. J Thromb Haemost 2004; 3:100-2. Fondaparinux In Obesity Results From the Matisse Trials Fondaparinux: < 50kg: 5mg qd 50-100kg: 7.5mg qd > 100kg: 10mg qd Enoxaparin: (Matisse DVT) 1mg/kg q12h Heparin: (Matisse PE) Adjusted per aPTT Davidson BL et al. J Thrombosis Haemost 2007; 5:1191-4. No weight-dependent difference in efficacy or safety Body Weight and Anti-Xa Activity for Prophylactic Doses of LMWH Area under the curve for 10 h N = 17 patients and 2 volunteers Enoxaparin 40mg SQ x1 dose AntiXa levels hourly x10 hours Regression line 95% CI for line 95% CI for data points 200 150 100 50 0 40 60 80 100 120 Body Weight (kg) Frederiksen SG et al. Br J Surgery 2003; 90:547-8 140 160 Dalteparin: Fixed Dosing For VTE Prevention Subgroup analysis of PREVENT TRIAL (dalteparin vs placebo in medically ill) BMI (kg/m2) Patients % < 25 37.5 25-29.9 33.1 30-34.9 18.9 35-39.9 7.1 > 40 3.3 Favors Dalteparin Favor Placebo Overall Prevent Trial 0.01 0.1 0.55 1.0 Relative Risk 10.0 Dalteparin 5,000 units daily was similarly effective in obese and non-obese patients (except pts with BMI>40) with no observed difference in mortality or major bleeding Kucher N et al. Arch Int Med 2005;165:341-5. Enoxaparin VTE Prophylaxis in TKA/THA/Trauma 31.8% p<0.001 16.7% N: 807 Dose: 40 mg qd Samama MM et al. Thromb Haemost 1995; 73:977. Obese : BMI>32kg/m2 Enoxaparin: VTE Prophylaxis in Bariatric Surgery 5.4% p<0.01 0.6% 30mg bid: n=92 BMI 51.7kg/m2 Scholten Obes Surg 2002; 12:19-24. 40mg bid: n=389 BMI 50.3kg/m2 Dalteparin in Morbid Obesity: Bariatric Surgery N=135 Bariatric Surgery Mean Weight: 148.8Kg Body Weight (kg) 200 Mean BMI: 53.7 Dalteparin: 7,500 IU daily Anti-factor Xa level P=0.031 180 P=0.052 P=0.444 160 140 120 0 Under target value Target value Over target value <>0.5 IU/mL <0.2 IU/mL <0.2-0.5 IU/mL n=13 n-=41 n-=81 Number of patient (%) Body weight (kg) Below target value (<0.2 UI/ml) 41 (30.4%) 159.4 ± 35.8 Target value (0.2–0.5 UI/ml) 81 (60.0%) 145.7 ± 28.4 Above target value (>0.5 UI/ml) 13 (9.6%) 134.6 ± 24.2 p value Simonneau MD, et.al. Obes Surg. 2008; [Epub ahead of print] 0.0152 LMWH in Obesity: Summary ► Treatment: in controlled trials, LMWH dosing has been based on TBW (max 160-190 kg) ● Dalteparin • Dose based on TBW • PI recommends dose capping • Recent clinical data supports TBW dosing – QD or BID dosing ● Enoxaparin • Dose based on TBW • Dose capping NOT recommended • BID dosing preferred ● Tinzaparin • Dose based on TBW, NO dose adjustment or capping ● ► Anti-Xa monitoring not necessary for TBW < 190kg Prophylaxis: a 25-30% dose increase (or 50IU/kg in high risk patients) Nutescu E, et.al. Ann Pharmacother; 2009; in press. 8th ACCP Conference on Antithrombotic Therapy Renal Impairment ► For each of the antithrombotic agents, we recommend that clinicians follow manufacturer-suggested dosing guidelines (Grade 1C) ► We recommend that renal function be considered when making decisions about the use of and/or dose of LMWH or fondaparinux (Grade 1A) ► Options for patients with renal impairment (Grade 1B) ● ● ● Avoid agents that renal accumulate Use a lower dose Monitor the drug level or anticoagulant effect Geerts WH. Chest 2008;133(suppl):381S-453S. LMWH in Renal Dysfunction Manufacturer Recommendations Dalteparin ● “should be used with caution in patients with severe kidney insufficiency.” • Monitor anti-Factor Xa for dose guiding with therapeutic doses Enoxaparin ● “adjustment of dose is recommended for patients with severe renal impairment (CrCL < 30 mL/min).” Tinzaparin ● “patients with severe renal impairment should be dosed with caution.” Fondaparinux - Contraindicated in CrCL < 30mL/min Recent Meta-Analysis of LMWHs and Bleeding In Patients With Severe Renal Dysfunction Patients w/ renal insuff. (n/n) Patients w/ no renal insuff. (n/n) Collet, et al; 2001 Paulas, et al; 2002 Siguret, et al; 2000 0/28 0/51 0/17 1/83 3/149 0/13 Chow, et al; 2003 0/5 0/13 Khazan, et al. (adj.); 2003 (Prophylactic) 2003 (Therapeutic) 2003 Spinler, et al; 2003 0/10 3/36 2/17 5/69 3/42 3/47 3/61 74/3,432 4.78 14.77 8.62 15.93 0.28 (0.01 – 5.16) 1.33 (0.25 – 7.05) 3.09 (0.35 – 27.31) 10.05 (2.02 – 49.98) Green, et al; 2005 1/18 0/20 2.66 8.26 (0.16 – 418.42) Kruse & Lee; 2004 0/50 1/120 2.22 0.24 (0.00 – 17.90) Macie, et al; 2004 2/7 6/201 2.68 977.78 (19.61 – 48,752.07) Peng, et al; 2004 0/7 0/43 Thorevska, et al; 2004 7/65 11/171 35.56 1.85 (0.63 – 5.40) Bazinet, et al; 2005 1/36 2/160 4.75 2.74 (0.15 – 51.73) 21/416 107/4,555 Study; year Total (95%, CI) Peto OR (95%, CI) Weight (%) 2.01 6.02 0.26 (0.00 – 23.94) 0.26 (0.02 – 3.50) Not estimable Not estimable Not estimable 100.00 0.01 0.1 1 Favors ↓’ed 10 100 Favors ↑’ed bleeding Lim W, et al. Ann Intern Med. 2006;144:673-684. Peto OR (95%, CI) 2.25 (1.19 – 4.27) Dosage adjustments for renal dysfunction Enoxaparin PK and PD in Renal Impairment Result: Tmax: 3-4 hours Amax: 10-35% higher in RI groups CI/F”linearly correlated with CrCl CL/F (L/h) Half-life (h) Normals 0.98 6.87 Mild RI 0.87 9.94 20% ↑ Moderate RI 0.76 11.3 21% ↑ Severe RI 0.58 15.9 65% ↑ Day 4 Sanderink GJCM. Thromb Res 2002;105:225-31. AUC (0-24) (h●IU/mL) LMWH Renal Dosing in NSTE ACS Patients ► 56 UA pts with CrCl <60 ml/min ► Enoxaparin dose empirically and anti-Xa level measured after 3rd dose • • • • Dose may be to 0.6mg/kg/ q12h if CrCL <30mL/min; or 0.8 mg/kg/q12h if CrCl 30-60 ml/min Anti-Xa monitoring Doses “appeared safe” Further prospective evaluation needed CrCl (ml/min) <30 (n = 28) >30 and <60 (n =28) Age 76+/-3 73+/-3 Enoxaparin (mg/kg/12h) 0.64 0.84 Anti-Xa (IU/ml) 0.95 0.95 Collet JP et al. International J Cardiol 2001;80:81-2. Clinical Use Of Recommended Enoxaparin Dosage in Renal Impairment N = 19 pts with Clcr < 30ml/min receiving enoxaparin 1mg/kg q24h 1.0. 6 0.9 TROUGH ANTI-Xa LEVELS 5 0.8 Number of Patients Antifactor X1 Level (U/mL) PEAK ANTI-Xa LEVELS 0.7 0.6 0.5 0.4 0.3 4 3 2 1 0.2 0.1 0 First dose Median Subsequent doses (second and third) 25-75% interquartile range Lachish T et al. Pharmacotherapy 2007; 27:1347-52. 0.05 0.10 0.15 0.20 0.25 0.30 0.35 0.40 0.45 0.50 0.55 Trough Antifactor Xa Level (U/mL) Tinzaparin 175 U/kg Peak Anti-Xa Levels According to Renal Function No correlation between peak anti-Xa activity and Clcr No accumulation of Anti-Xa activity after 10 days of therapy Siguret V et al. Thromb Haemost 2000;84:800-4. Pharmacokinetics of Prophylactic Enoxaparin vs Tinzaparin Enoxaparin 40mg qd or Tinazaparin 4500 IU qd N = 52 patients Mean age = 87.7 yrs Mean wt = 52.3kg Mean Clcr = 34.7ml/min Mahe I et al. Thromb Haemost 2007; 97:581-6. Dalteparin 100 U/kg q12h Peak Anti-Xa Levels According to Renal Function Clcr Mean peak anti-Xa level after 5-6 doses > 80 0.47 < 40 0.55 Antifactor Xa Level (U/mL) No difference in peak anti-Xa activity between normal patients and patients with renal impairement 1.5 1.0 0.5 x x 0 Subjects without Renal impairment N=11 Shprecher AR et al. Pharmacotherapy 2005; 25:817-22. Subjects with Renal impairment N=11 Pharmacokinetics of Prophylactic Doses of Dalteparin N = 115 elderly (age > 65) pts with acute medical illness and elevated SCr Tx: dalteparin 5000 U or 2500 U SQ qd (risk-based) for VTE prophylaxis Renal Failure Mild (n=12) Moderate (n=73) Severe (n=24) CrCL (ml/min) 60-89 30-59 <30 Day 6 peak anti-Xa 0.030 0.033 0.048 Minor Bleeding 0 3 0 Major Bleeding 0 0 0 P=0.72 ► No evidence of accumulation of anti-Xa activity ► No relationship between the degree of renal impairment and peak anti-Xa level on Day 6 ► No association between creatinine clearance and anti-Xa levels Tincani E et al. Haematologica 2006; 91:976-9. Dalteparin Thromboprophylaxis in Critically Ill Patients with Severe Renal Insufficiency: The Direct Study ● ● ● ● ● N=138 critically ill patients CrCl < 30 ml/min • Mean CrCL 18.9ml/min Dalteparin 5000 IU sc daily Serial anti Xa levels measured on days 3, 10, and 17 Bioaccumulation defined as trough anti-Xa level > 0.40 IU/mL Results: • • • The median duration of dalteparin exposure was 7 (4-12) days No patient had a trough anti Xa level > 0.4 IU/ml Based on serial measurements • peak anti-Xa levels were 0.29 to 0.34 IU/mL • trough levels were lower than 0.06 IU/mL Douketis, et al. Arch Intern Med. 2008 Sep 8;168(16):1805-12. Dosing of LMWHs In Renal Impairment Recommendations FOR CrCL < 30 ml/min ► Enoxaparin: ● ● ► Prophylaxis doses: 30 mg sq QD Treatment doses: 1mg/Kg sq QD Dalteparin and Tinzaparin: ● ● ● no specific dosing guidelines No or lower degree of accumulation expected Anti-Factor Xa activity monitoring FOR CrCL 30-50 mL/min ► No specific recommendations ► Concern with prolonged use > 10 days with enoxaparin (15-25% dose decrease ?) ► Monitoring anti-Xa ? Nutescu E, et.al. Ann Pharmacother; 2009; in press. Unresolved Issues in Renal Dosing of LMWHs CrCl (mL/min) < 30 < 20-15 Recommendations Dose of enoxaparin should be adjusted; dalteparin and tinzaparin no short term accumulation expected. LMWHs have not been adequately studied as repeated doses for prophylaxis and treatment indications; UFH is preferred in these patients. Issues with anti-factor Xa testing include: true therapeutic range, standardization, availability, recommendations for dose adjustment Anti-Xa Activity Level Monitoring Enoxaparin 1mg/kg SQ pharmacokinetic profile Peak (goal ~ 0.5-1 U/ml) at 3-4 hrs Trough (goal < 0.5 U/ml) at 11-12 hrs Laposata et al. Arch Pathol Lab Med. 1998;122:799-807. ANTI-Xa MONITORING: Recommendations Level 3 Evidence: (isolated anecdotal studies or the consensus of experts) ► Laboratory monitoring using an anti-Xa assay MAY be of value in certain clinical settings ► Use peak levels 4 hrs after SQ dose ► Through levels in renal impairment maybe preferred ► Use chromogenic, not clot-based assays ► Peak: • for BID dosing: • • for QD dosing: 1.0-2.0 U/ml Through: < 0.4 U/ml 0.5-1.1U/ml Laposata et al. Arch Pathol Lab Med. 1998;122:799-807. Nutescu E, et.al. Ann Pharmacother; 2009; in press. Fondaparinux Pharmacokinetics 100% bioavailable Pentasaccharide* concentration (µg/mL) 0.35 0.25 Cmax = 0.34 µg/mL (SD: 0.04) Tmax = 1.7 h (SD: 0.4) T1/2 = 17.2 h (SD: 3.2) 0.2 Elimination = RENAL 0.3 0.15 0.1 0.05 0 0 4 8 12 16 20 Time (h) Donat F, et al. Clin Pharmacokinetics 2002; 41 (suppl 2):1-9. 24 28 32 36 Fondaparinux Use in Patients with Impaired Renal Function ► Total clearance lower than in patients with normal renal function Fondaparinux: PI ● Mild impairment ~25% ● Moderate impairment ~40% ● Severe impairment ~55% Incidence (%) Full-dose Fondaparinux Risk Of Major Bleeding 4.8% 3.8% 1.6% 2.4% n=504 n=1288 n=1565 Clcr 80 mL/min Data on file, GlaxoSmithKline Clcr 50–80 mL/min Clcr 30–50 mL/min Clcr < 30 ml/min Influence of Renal Function Fondaparinux vs Enoxaparin in ACS OASIS-5: Fondaparinux 2.5mg qd vs enoxaparin 1mg/kg q12h for 2-8 days Fox KAA et al. Ann Intern Med 2007; 147:304-10. A Year 2009 Update for The Health System Pharmacist Electronic Alerts: Future Horizons Karen Fiumara, PharmD Medication Safety Officer Brigham and Women’s Hospital Adjunct Assistant Professor of Pharmacy Practice Massachusetts College of Pharmacy and Allied Health Sciences Adjunct Assistant Professor of Pharmacy Practice Bouve’ College of Health Sciences Northeastern University Boston, MA Background ► Past 10 years the prevention of medication errors has become a primary focus in healthcare ► In 1995 Bates et al. published landmark study indicating 28% of hospital admissions are attributed to preventable medication errors ► The IOM report “To Err is Human” have led to increased research and development of both medical informatics and computerized alerting systems Bates DW et al. JAMA 1995;274:1311-16 CPOE : Friend or Foe? ► Recently, institutions are beginning to critically assess electronic systems, such as CPOE ► VA Medical Center in Salt Lake City: ● ● ● ► 74% of medication errors occur during prescribing 11% during administration 0% during transcription Bates et al. study: ● ● ● 56% of medication errors - prescribing 24% of medication errors – administration 6% of medication errors – transcription Nebeker JR et al. Arch of Intern Med 2005;165:1111-16. CPOE : Friend or Foe? ► VA Medical Center attributed low error rates during the transcription and administration to information system upgrades such as: ● ► Bar code technology during administration, EMAR and computerized drug-drug interaction and allergy screening Concluded that their systems are working as designed but lack decision support within CPOE leading to high error rates during prescribing Nebeker JR et al. Arch of Intern Med 2005;165:1111-16. CPOE Alerts ► Institutions that utilize decision support and computerized alerts during prescribing have reported high rates of physician override ► A study conducted at BIDMC reported that 94.2% of computerized alerts were overridden ► Reviewers concluded of the 189 rules studied, 36.5% of the rules were invalid and agreed with the physician’s decision 97.9% of the time Weingart SN et al. Arch of Intern Med 2003;163:2625-31. Saving CPOE from Extinction ► CPOE must evolve to keep up with the growing demand for effective medical informatics and technology solutions ► Next generation of CPOE will utilize algorithms that take into account patient specific factors and generate prescribing recommendations to providers ► One area in which CPOE has proven beneficial is VTE prophylaxis Medical Error Rates ► ► Two errors per day = 99% proficiency level If 99% was good enough: –Airline industry = 2 unsafe landings per day –Mail industry = 16,000 pieces of mail lost every hour –Banking industry = 32,000 checks deducted from the wrong account per hour ► How do we transform health care into a high reliability industry? Leape LL. JAMA. 1994;272:1851-7. Background ► At Brigham and Women’s Hospital, we have initiated a series of trials aimed at increasing prophylaxis by: ● ● Changing MD behavior and Improving the implementation of prophylaxis strategies Types of Interventions ► Electronic computer generated alerting systems ► Efficacy of these alerting systems have been studied in: ● ● RCT trial of a 1-screen alert Cohort study of a 3-screen alert First Generation Electronic Alerts ► BWH utilizes BICS (Brigham Integrated Computing System) for all order entry functions ● ► Admitting records, demographic information, lab results, medication orders, etc. VTE group utilized computer system to screen all patients admitted to the hospital for High Risk VTE status First Generation Alert: Development ► Aim: to increase rate of prophylaxis in patients at risk for DVT and PE ► Developed computer program to detect and identify which patients were at risk ► Alert the responsible physician of high risk patient (via e alert) and offer opportunity to order appropriate prophylaxis Study Schema All Adult Patients DVT Risk Score > 4 YES Presence of Prophylaxis NO Generate Alert Definition of “High Risk” VTE risk score ≥ 4 points: ► ► ► ► ► ► ► ► Cancer Prior VTE Hypercoagulability Major surgery Bed rest Advanced age Obesity HRT/OC 3 3 3 2 1 1 1 1 (ICD codes) (ICD codes) (Leiden, ACLA) (> 60 minutes) (“bed rest” order) (> 70 years) (BMI > 29 kg/m2) (order entry) Randomization VTE Risk Score > 4 No Prophylaxis N = 2506 Intervention Control Single Alert No Alert n = 1255 n = 1251 Kucher N, et al. NEJM 2005;352:969-977 Physician Notification of Alerts First Generation Computerized Alerts for VTE Prevention ► Utilization of computer generated alerts to house staff reduced the incidence of VTE by 41% ► VTE prophylaxis was prescribed in 33.5% of patients in the intervention group ► Following study conclusion a follow up cohort study was conducted Kucher N, et al. NEJM. 2005;352:969-977. Alerts Second Generation: Electronic Computer Generated Alerts BWH VTE Alerts: The Future ► Goals: ● Engage the house officer with an interactive alert to increase acceptance and gain feedback ● Update the DVT prophylaxis template to meet current practice guidelines ● Provide real-time knowledge links Interactive Techniques ► Provide objective data to the house officer that this alert positively impacts patient outcome ► Create opportunity to capture rationale for declining alert ● Hypothesized that many physicians fear a risk of bleeding with anticoagulation ► Provide a final opportunity to order mechanical prophylaxis ► Alert attending physician if alert is not acknowledged after 24 hours DVT Alert Screen Rule Logic – Alert Details Option A Option C or “Done” Escalation and Timing of Alerts ► Alerts should be set up to generate each day at 8:30 AM ► If an alert was not acknowledged after 24 hours the attending physician on record should be text paged. Quality Assurance ► Weekly reports are reviewed ► Allows core team to review all aspects of the alerts including: ● Type of action taken ● Rate of overrides ● Rational for declining the alerts ► Results coming soon Alerts Pharmacy/Physician Collaboration Human Alerts VTE Prophylaxis: hALERT ► Multicentered RCT of human alerts (hALERT). ► Objective: to recruit hospitals that differ from BWH re: IT, community vs. academic, urban vs. suburban/rural, location within USA. ► Can a human alert be more effective than an electronic alert? Methodology ► Patients admitted to the hospital are screen by human for increased VTE risk ► High risk patients are randomized to alert or no alert ► Physicians of patients in alert group receive page alerting them of high risk status ► Records are checked for prophylaxis order 48 hours after alert ► 90 day follow up for clinically significant VTE and clinically importing bleeding hALERT: Capturing New Prophylaxis Orders ► Enrolled patients must be reexamined in 24-48 hours to determine whether prophylaxis orders were written. ► Capturing prophylaxis orders after enrollment applies to both the Intervention Group and to the Control Group. Human Alert Trial 1. Human (often RN or pharmacist) issues the Alert, not a computer 2. The attending physician, not the intern, receives the Alert 3. Diversity of centers: community, suburban, throughout the USA 4. Will attendings pay more attention than house staff? Conclusions ► Changing behavior is challenging ► Multi-disciplinary team involvement is critical to successful implementation ► Need to engage providers and obtain feedback ► Designing “smart alerts” that include decision support functionality or “human alerts” that require face to face contact may be effective Alerts Electronic Alerts to Prevent Infusion Errors Patient Case—Infusion Pump Error Error Description ► 57 YOM endstage CMP ► 8:45 PM aPTT = 75.1 ► ► 1:13 AM Protamine 25mg ► 1:28 AM aPTT = >150 ► 3:13 AM aPTT = >150 ► 3:32 AM Protamine 26mg ► 2 Units PRBC ► 4:08 AM aPTT = >150 ► 8:21 AM aPTT = 44.4 ► ► ► ► EF = 10% Heart transplant candidate with BIVAD Receiving UFH 900 units per hour (9 mls/hr) New order to reduce Heparin 800 units per hour @ 10:22 PM Infusion pump set for 800 mls per hour Background National Data Rank Medications Causing Harm •Heparin has been identified both nationally and internally at BWH as a medication frequently associated with ADE 1. Insulin 2. Morphine •Removed access to different formulations 3. Heparin •Standardized UFH Concentration 4. Warfarin •Calculate infusion rates in OE 5. Potassium 6. Furosemide 7. Vancomycin 8. Hydromorphone 9. Meperidine 10. Diltiazem MEDMARXSM 2001. The United States Pharmacopoeia (USP)Convention Inc. UFH Error Analysis: BWH ► 1 event per 1,000 patients ● ● ● ► 52% - Administration related 31% - Equipment failure, rate or dosing error 23% - Infusion Pump 6% - Prolonged LOS or significant harm ***Patient Safety Initiative: Hospital invested 3 million dollars in state of the art infusion pumps*** Fanikos J et al. Medication Errors associated with anticoagulation therapy in the hospital. Am J Cardiol 2004;94:532-535 Objectives ► Evaluate impact of “smart” infusion technology on anticoagulation administration ► To determine if infusion technology equipped with drug libraries may reduce medication errors Features of the “Smart” Pumps ► “Smart” pumps share safety features of older pumps including dose calculation functions, freeflow protection and occlusion alerts ► “Smart” pumps also equipped with a drug library ● ● Provide dose and rate limits on commonly used medications Provide users with overdose and underdose alerts based on predetermined limits defined by the drug library Methods ► ► ► We programmed the drug library to alert for overdoses or underdoses Underdose Alert Overdose Alert Alerts where subsequently recorded in the device’s electronic memory, along with the user’s next action UFH <300 units/hour >2,800 units/hour Argatroban <0.5 mcg/kg/min >10 mcg/kg/min We retrospectively reviewed all anticoagulant alerts and the user’s next action for all devices from 10/2003 through 1/2005 Lepirudin <5 mg/hour >16.5 mg/hour Bivalirudin <0.2 mg/kg/hour >1.8 mg/kg/hour Medication Dosing Errors and their Magnitude Data Entry Errors Frequently Repeated with UFH 27.2 % entry errors User repeated the error Alerts by Time of Day Conclusions ► The drug library and its alerting system intercept programming errors ► Despite alerts, data entry errors are frequently repeated by the user ► The highest alert incidence occurs on weekdays between 2 PM and 4 PM, corresponding to Nursing Shift change