10 Hserv 482 Canada
Learning Objectives
Describe plausible reasons for Canada's good standing
in the Health Olympics
List factors that may be involved in the decline in
standings over the last decade
My Background
born in Toronto, lived there for the first 23 years of my life,
went to U of Toronto
lived a year in Montreal in 1970s as an intern at McGill
University
lived and worked as a doctor in BC in the 1970s
worked for University of Calgary in 1980s
cared for my father in Toronto nursing home, and BC nursing
home
own land in BC
continue to spend much time there
–Vancouver, Lower Fraser Valley, Toronto, Montreal, Edmonton
–in the mountains (Yukon, Rockies, Selkirks, Coast Ranges)
Canada comparisons with the US
Canada a British Colony from 1700s
strong ties with England continued to recent times
social welfare contract:
–baby bonus checks
–publicly supported education system with no private
schools at university level and very few below that
more progressive taxation system
Universal coverage health care since 1960s
1974 Lalonde Report (New Perspective on the Health
of Canadians)
LaGuardia and Toronto airports 2002
US
Canada
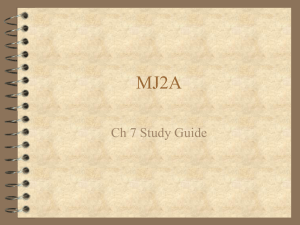
76.9
79.2
7
6
4187
1783
9.8
3.4
29,605
23,852
Smoking Prevalence Male
27.6
27
Smoking Prevalence Female
22.1
23
Gini
40.1
31.5
World Bank 2000
CEO-Boss/ Average Worker pay
ratio
531:1
21:1
New York Times Jan
25, 2004
Highest
53/1000
15/30
16/1000
SCF 2004 report
Educational Disadvantage
7th worst
4th best
UNICEF Innocenti
Research Group
Child Injury Deaths
4th worst
9th worst
Child Poverty
2nd worst
7th worst
Child Abuse Deaths
2nd worst
7th worst
Life Expectancy
IMR
Health Care Costs/capita (USD)
Maternal Mortality Ratio
GDP/capita (USD)
Teen Births
Source
UNDP 2003
UNICEF 2000
WHO 2000
OECD
UNDP 2000
American Cancer
Society
United Nations Human Development Report 2007
BETTER HEALTH
MORE EQUALITY
Kaplan 1996 BMJ
BETTER HEALTH
Ross et. al. BMJ 2000
MORE EQUALITY
Lowest Life Expectancy
And disability free years
Highest Life Expectancy
And disability free years
Life expectancy disparity
is 16 years
Metropolitan Income Inequality
and Mortality in North America
Siddiqi & Hertzman SSM 2007
81
80
Life Expectancy
79
78
Idaho
Washington
77
British Columbia
76
75
74
1980
1985
1990
1995
2000
Williams-Derry 2002
Cascadia
2002
NW Env Wa
Seattle Magazine August 2007
Infant Mortality: US vs Canada, 1996
Canada
US
Poorest 20%
Second
Third
Fourth
Richest 20%
6.5/1000
5.2
5.1
4.7
3.9
-----------
Overall
5.2
7.8
Infant Mortality Rates, Status Indians
and Other Residents, B.C., 1991-2001
Rate Per 1,000 Live Births
14
Status Indians
Other Residents
12
10
8
6
4
2
0
1991-96
1997
1998
1999
2000
2001
1997-2001
Year
Sources:
BC Vital Statistics Agency, 1997
BC Ministry of Health Planning, 2003
LESS EQUALITY
VIOLENCE AND INEQUALITY Daly 2001
LESS EQUALITY
VIOLENCE AND INEQUALITY Daly 2001
More PRISONERS
Prisoners
MORE EQUALITY
Wilkinson et. al. SSM 2007
More TRUST
TRUST
MORE EQUALITY
Uslaner 02
After Willms 1999
Better SCHOOL Performance
Math and Literacy Scores
MORE EQUALITY
Wilkinson et. al. SSM 2007
UNICEF League Table Educational Well-Being
Household Poverty Rates
(Household Head Aged 25-64)
(A)
Market
Income
Canada
(1994)
Sweden
(1992)
US
(1994)
(B)
(C)
(D)
(E)
Col A +
Col B + Col C – Col D +
Percent
Change
Private Universal Taxes
Social
Income
and
Assistance Columns
A to E
Transfers
Social
Transfers
Transfers
23.9
21.1
15.4
16.6
14.5
-39.3
20.7
20.1
5.0
8.5
3.8
-81.6
23.2
21.0
18.4
20.5
18.9
-18.5
Solo Poverty
% of children living below the poverty line, 1990-1992
Sweden
Denmark
Finland
Belgium
Italy
Norway
Netherlands
Canada
Australia
United States
Source: Canada Social Trends,
1996
• Children in
two• parent
families
2.2
2.5
1.9
3.2
9.5
1.9
3.1
7.4
7.7
11.1
Children in
solo
mother family
5.2
7.3
7.5
10.0
13.9
18.4
39.5
50.2
56.2
59.5
Social Expenditure on Family Benefits as a
% of GDP
Rank
• Sweden
• France
• Norway
• Finland
• Australia
• Canada
• USA
2.23
2.13
1.91
1.90
1.36
0.51
0.22
Source: OECD Social Expenditure Database (1998)
1
2
3
4
5
6
7
Q5/Q1 Mortality Ratios
Canada
3.50
3.25
1971-M
3.00
2.75
1986-M
2.50
1991-M
2.25
1996M
2.00
1971-F
1.75
1986-F
1.50
1991-F
1.25
1996-F
1.00
0.75
<1
1-14
15-24
25-34
35-44
45-54
55-64
65-74
Mortality by Neighbourhood Income in Urban Canada,
Wilkins R, Berthelot JM, Ng E,PPA March 2001
75-84
85+
Age (yrs)
Canada beats USA But Loses Gold to Sweden
0.4
International comparisons of intergenerational social mobility
Higher columns show that people’s social position is more strongly
determined by their parents’ position
0.3
0.2
0.1
Source: Blanden J, Gregg P, Machin S. Intergenerational mobility in Europe and N.
America. Centre for Economic Performance, London School of Economics. 2005
Norway
Sweden
Denmark
Canada
Finland
W
Germany
Britain
USA
0
Father's and Son's Incomes
More financial mobility
If poor in US, stay poor
MORE EQUALITY
Wilkinson et. al. SSM 2007
16 nations, 169,776 people
Lowest Life Expectancy
And disability free years
Highest Life Expectancy
And disability free years
Life expectancy disparity
is 16 years
BC/Washington Comparisons
BC
WA
PUBLIC/ PRIVATE
spending, Taxes
Taxes
$1700 more
Retail sales tax, property tax and
misc. taxes
Income, property and sales tax
Public Programs
$1000 less per
person
Student tuition
$1700 more in
public universities
Utilities
$540 more per
family
Life insurance,
pensions,
$2300 more per
family
BC/Washington Comparisons
BC
WA
Inequality
Social Assistance
More generous
Only adults caring for
dependent child eligible for
5 years over lifetime
People without
health insurance
0
900,000 (16% of
population in 1998)
Income inequality
(Q5/Q1)
IMR (1989)
6.2 (1998)
5.2 (1989)
4.03
9.2 (1998)
7.0 (1989)
7.0
Minimum wage
$7.60
$8 (Can at ppp)
BC/Washington Comparisons
BC
WA
Working Conditions
Worker's paid
statutory holidays
Maternity Leave
9 days + 2 weeks
annual vacation
then 3 weeks after 5
yrs
55% up to
$413/week for 50
weeks (15 weeks
maternity + 35
weeks parental
leave shared with
father)
compassionate care leave
while caring for a dying
0
12 weeks only if
working in public
sector or for private
companies with >50
employees (amounts to
55% of workforce)
2009 WA up to 5
weeks at $250/wk
BC/Washington Comparisons
BC
WA
Working Conditions
Unionization
30.4%
18.2%
Getting fired,
(termination)
"Just cause" or 2
"At will"
weeks notice after a
year of work or 2
weeks pay
Income vs. Income Inequality?
In Canada, income inequality health relationship is not as strong as in the
US because of other supports that mitigate adverse effects of income
inequality
–McLeod 2003: prospective cohort study, SAH 94,96, 98 found low
hh income associated with poor SAH, but not inc. ineq. (measured in
91 from census in 53 metro. areas)
–Sanmartin 2003 Labour market income inequality in NA
metropolitan areas: more effect in US than in Canada
–Laporte (2003) provincial time-series modeling from 1980 to 1997
look at income and mortality don't find income or income inequality
significant but health spending and unemployment predicts mortality
better
–Daly (2001) find homicide and inc. ineq. related in Canada as in US,
with differences in inc. ineq. Explaining lower rates in Canada when
lump states & provinces
Saez 2005
USA Canada Economic Comparisons
After-Tax Income Gap is Bigger than Ever for
Families Raising Children in Canada (ratio of aftertax income in deciles 10 and 1, 1976-2004)
10.0
Earnings
9.5
9.0
8.5
8.0
7.5
7.0
1976
1978
1980
1982
1984
1986
1988
1990
1992
1994
1996
1998
2000
2002
2004
Yalnizyan, 2007
Yalnizyan 2007
Yalnizyan 2007
United Nations Human Development Report 2007
United States
USA economic pie shares
Share of nation's net worth 2004
Top 1%
Next 9%
34.7%
35.4%
Bottom 90%
29.9%
US Wealth Distribution 2004
29.9%
34.7%
35.4%
Top 1%
Next 9%
Bottom 90%
from 1992 to 2004 the wealth share of the
least wealthy
half of the population fell significantly
to 2.5 percent of total wealth
Source Federal Reserve Board Survey
Of Consumer Finances and Forbes
Pizzigati, Too Much
http://www.cipa-apex.org/toomuch/articlenew2006/April24a.html
Harvey 2005
Health in Canada
Very good in comparison to US
The result of a historical social contract and
redistribution that is not income-based
Not because of health care system
Sin (2003) looking at children of very poor vs poor & nonpoor families in Alberta had higher rates of asthma ER
visits despite universal access (all births 850401 to 880331)
followed for ten years
Munnell 2004
Medical Care Act, 1966
Passed House of Commons
Insurance rather than national system
By 1971, all provinces ratified
Doctors accepted limitations on their practice
–Penticton Hospital Swan Ganz Catheter
Medical care less intervention-based (comparative
studies with US on doing less and having better
outcomes) current cardiac work-up examples
Influence of Great Depression
“if medical care is a contingency left to
each individual to secure as best he can,
it becomes a function of the distribution
of wealth”
Marsh, Grant, Blackler Health and
Unemployment: Some Studies of Their Relationships
(1938)
Extra Billing/Two-Tiered System
"Any free country that talks about
the democratic process and allows
extra billing to become the general
rule is denying the basic principles
of the democratic process"
– Tommy Douglas 1982, introduced Medical Care Act in
Saskatchewan in 1962, the first single-payer in Canada
% GNP x 100
Universal Health Care/Population Health
Manitoba 10 year study: who uses how much care
how this differs by health & ses
Is health care an effective policy tool for reducing
inequalities in health?
Examine 1986 health care use in Winnipeg, and ten
years later
Health characteristics (life expectancy, prevalence of
chronic disease, rates of avoidable hospitalization) in
1986 and 1996
Effect of downsizing hospital system (24% bed
closure over that period)
Roos 2006
Roos 2006
“To conclude, a universal health
care system is definitely the right
policy tool for delivering care to
those in need, and for this it
must be respected and
supported. However,
investments in health care
should never be confused with,
or sold as, policies whose
primary intent is to improve
population health or to reduce
inequalities in health. Claims to
that effect are misleading at
best, dangerous and highly
wasteful at worst.”
Web of Influence
Chapter 5, Universal Medical Care and Health Inequalities: right
objectives, insufficient tools. Roos, Brownell, Menec (2006). Oxford
University Press.
Guyatt, G. H., P. J. Devereaux, et al. (2007). "A
systematic review of studies comparing health
outcomes in Canada and the United States." Open
Medicine 1(1): e27-36.
High Quality
Studies
Low Quality
Studies
Resulting favoring
United States
2
3
Results favoring
Canada
5
9
Mixed or equivocal
results
3
16
stay < 24 h, obstetrics, transfer, cardiac arrest o
n arrival and subsequent death, rehab, psychiatric
Baker et al CMAJ 2004 Figure 1
Baker et al Adverse Events Results
7.5% of patients had ≥1 Adverse Event (AE)
–51% surgery, 45% medicine
–Errors of omission and commission
–16% of AE's resulted in death
36% highly preventable (score >4)
AEs resulted in longer stays, temporary disability
–5% resulted in permanent disability
9250 to 23750 deaths from AEs were preventable
–~ 64% not preventable total deaths 34900 to 98700
Death associated with AE in 1.6% of patients with similar hospitalizations in Canada Adjusting
for sampling strategy
Baker et al CMAJ 2004
Baker et al CMAJ 2004
*Weighted to account for the total number of charts per hospital
and the total number of hospitals per type per province.
†Adjusted for 8 comorbidities plus age and sex
Baker et al CMAJ 2004
Baker et al Adverse Events Results
Higher AEs in teaching hospitals
1. ? Higher patient acuity
2. Teaching hospitals receive patients at different
points in care (small or large community hospitals
may not be able to provide care)
3. Complexity of care in teaching hospitals--usu.
Several providers, with risk of miscommunication,
coordination
4. Patient records may vary across hospital types
5. Lower quality of care
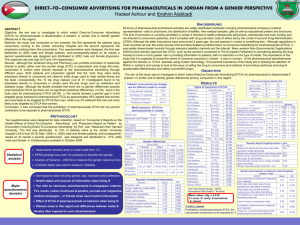
DIRECT TO
CONSUMER
ADVERTISING
Direct to Consumer Advertising
DTCA: 3 types
Disease-awareness advertisements
–Prompts consumers to talk to providers about treatment
without expressing brand preferences
Reminder advertisements
–States name of product, strength, dosage, form and price
but may not mention production's indication or make
claims about effectiveness
Product-claim advertisements
–Includes indication and effectiveness
–Allows manufacturers to associate claims with particular
brands
Direct to Consumer Advertising
DTCA: PRODUCT CLAIM type
Product-claim advertisements
–Begun in US in 1982 in Readers Digest and required
product labeling information to be presented as in medical
journals
•Moratorium from 1983 to 1985 as FDA consulted
–Began again in Sept. 1985 and by 1987 spending $35
million annually on DTCA
–Required major side effects and contraindications
Broadcast advertisements began late 1980s
Spending $380 million in 1995, $790 million in 1996
US growth in DTCA
1997: required major statement about risk 4 sources
–
–
–
–
Toll-free telephone service
Concurrently running print advertisements or brochures
Consumer's health care provider
Web site
2005 spending of $4.24 billion (11 times that of 1995)
1996-2004: DTCA grew from 9% to 16% of total
expenditures on drug promotion (including retail
value of professional samples)
– Excluding samples: 19% to 27% by 2005
DTCA spending to exceed doctor advertising by 2011
DTCA vs drug marketing to doctors
1996-2004:
DTCA Expenditures increased 408%
"On the basis of an analysis of 49
brands that were the subject of
DTCA between 1998 and 2003,
IMS Management Consulting
concluded that the return on
investment from DTCA is "nearly
unprecedented in terms of the
positive sales response
generated."
Sample spending
increased 144%
Drug sales representative
contacts increased 224%
Morgan 2007
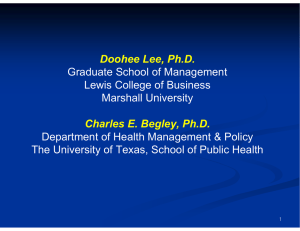
US spending on DTCA & US-Canada Difference in per-capita drug expenditures
US
DTCA $
US-Canada Drug $
Morgan 2007
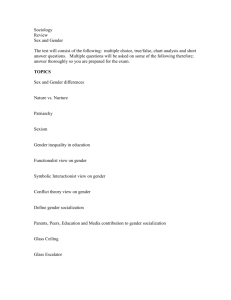
DTCA US/CANADA
COMPARISONS
DTCA Expenditures increased
408%
"On the basis of an analysis of
49 brands that were the
subject of DTCA between
1998 and 2003, IMS
Management Consulting
concluded that the return on
investment from DTCA is
"nearly unprecedented in
terms of the positive sales
response generated."
Sample spending
increased 144%
Drug sales representative
contacts increased 224%
Canada
Government
Writings
POPULATION HEALTH
Federal
Provincial
Local
Regional
Provincial
Determinants of Health
1 Income and social
status
2 Social support
networks
3 Education
4 Employment and
working conditions
5 Social environment
6 Physical
Environment
7 Biology and genetic
endowment
8 Personal healthy
practices and coping
skills
9 Healthy Child
Development
10 Health Services
11 Culture
12 Gender
Alberta Determinants of Health
1 Income and social status
8 Personal healthy practices and coping skills
"countries with the greatest differences between
the richest and poorest tend to have poorer
overall health status than societies which are both
prosperous and have an equitable distribution of
wealth"
"There is increasing understanding that personal
decisions are greatly influenced by the socioeconomic environments in which people live,
learn, work and play."
2 Social support networks
"Healthy child development is a powerful
determinant of health. How a child develops is
greatly influenced by their physical and social
environment."
"Caring and respect are derived from strong
social networks which improve one's sense of
well-being and appear to act as a buffer
protecting against health problems."
5 Social environment
"Goes beyond friends and family and extends to
the broader community in which a person lives
and works. It includes a sense of cohesiveness
within society from its values to its institutions to
informal giving."
9 Healthy Child Development
11 Culture
"particularly for those who are a part of a cultural
group that is not the dominant one in the area in
which they live and work."
12 Gender
"Gender refers to the societal roles placed on
the sexes that influence behaviors, personality,
attitudes, and power and influence on society
that may be on a differential basis."
CITY
Tides of Change Atlantic Canada
Tides of Change 7 Key messages
1. Health is conceptualized as physical, mental, and social well-being rather than as the
absence of disease. We then discuss the current tendency of chronic disease
prevention strategies to focus on changing individual risk behaviours, despite
evidence that changing to social and economic root causes could be more effective.
2. The scene in Atlantic Canada by reviewing statistics for the three categories of
chronic disease: noncommunicable, communicable, and mental health. We also
include main regions facing inequities within the provinces.
3. Theory and evidence that social and economic processes and the resulting poverty
create inequities and chronic disease in society.
4. Vulnerable populations who are affected by inequities: Aboriginal people and African
Canadians, single mothers and children living in poverty, seniors, and rural
populations.
5. Importance of place; neighbourhood, community, region, etc., in creating inequities
and points out that inequities in society affect the entire population, not just the poor.
We look briefly at cultural and social context, geographic areas, and income
distribution.
6. Ask how inequities can lead to chronic disease. Materialist, psychosocial, and
political/economic pathways are discussed in the Atlantic Canada context.
7. Recommend strategic directions that must be based on the root causes of inequities
in society.
Safe and affordable housing
Nutritious food
Safe and affordable housing
Nutritious food
 0
0