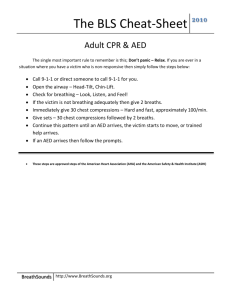
Worksheet Title - Heart Volunteer
advertisement

Dallas 2015 AED training methods TFQO: EVREVs: Taskforce: Robert Greif Jan Breckwoldt, Henrik Fischer Education Implementation and Training (EIT) COI Disclosure Dallas 2015 (specific to this systematic review) Commercial/industry None to declare Potential intellectual conflicts RG: # 344 HF: # 84 JB: # 30 2010 Consensus of Science Dallas 2015 1 study (LOE 2) demonstrated that training delivered by laypeople is as effective as training by by HCPs. 1 study (LOE 1) reported that instruction by nurses, as compared with physicians, resulted in better skill acquisition [for nurses]. 4 studies (LOE 2; LOE 4) reported that the use of computer-based AED training improved skill acquisition and retention, particularly when combined with manikin practice. 1 study (LOE 1) supported the use of video-self instruction when compared with instructor-led training. 3 studies (LOE 1) showed that the use of video self instruction was less effective for some elements when compared with instructor-led training. 1 study (LOE 1) supported the use of a training poster and manikin for learning AED skills. 3 studies (LOE 2; LOE 4) reported that laypeople and HCPs could use an AED without training. 3 studies (LOE 2) reported that untrained individuals could deliver a shock with an AED. However, even minimal training (15-min lecture, 1-h lecture with manikin practice, or reading instructions) improved performance (e.g., time to shock delivery, correct pad placement, safety). 2010 Treatment Recommendation Dallas 2015 AED use should not be restricted to trained personnel. Allowing use of AEDs by individuals without prior formal training can be beneficial and may be lifesaving. Since even brief training improves performance (e.g., speed of use, correct pad placement), it is recommended that training in the use of AEDs be provided. Laypeople can be used as AED instructors. Short video/computer self-instruction (with minimal or no instructor coaching) that includes synchronous hands-on practice in AED use (practice-whileyou-watch) may be considered as an effective alternative to instructor-led AED courses. C2015 PICO Dallas 2015 Among Population: students who are taking AED courses in an educational setting (P), Intervention: does any specific training intervention (I), Comparison: compared with traditional lecture/practice sessions (C), Outcomes: change clinical outcome, skill performance in actual resuscitations, skill performance at 1 year, skill performance at course conclusion, cognitive knowledge, use of AEDs (O)? Inclusion/Exclusion & Articles Found Dallas 2015 Inclusions/Exclusions Include: studies describing the effect of training interventions on AED skill acquisition, retention or performance. Also alternative approaches as non-istructor led training, self-training (kits); also for pediatric AED use; Not only health care providers also first responders, lay people, police, fire brigade, first aid providers, swimming pool attendants Exclude: purely descriptive studies of courses with no evaluation of training; studies comparing different course duration, studies addressing refresher training, non-RCT studies; animal and non-human studies; studies not available except in abstract format 1331 articles from primary search, 40 articles evaluated as full texts, 7 articles finally included for PICO question Dallas 2015 Draft Treatment Recommendations For lay persons we can give a weak suggestion to combine self-instruction teaching methods of shorter durations with practical hands-on training. No recommendation can be given for isolated selfinstruction without involvement of a trainer. For HCPs we suggest shorter duration of trainings and/or self-directed teaching methods. All these suggestions are based on low evidence studies, due to outcomes with low clinical relevance. We did not identify any evidence to address the critical outcome of “neurologically intact survival”. Risk of Bias in studies Dallas 2015 Dallas 2015 Evidence profile table(s) Self instruction without instructor-led practice for lays subquestion -1- Dallas 2015 Evidence profile table(s) Self instruction without instructor-led practice for HCPs subquestion -2- Dallas 2015 Evidence profile table(s) subquestion -3- Self instruction combined with instructor-led practice for lays Dallas 2015 Evidence profile table(s) Self instruction combined with instructor-led practice for HCPs subquestion -4- Proposed Consensus on Science statements Dallas 2015 Studies related to this PICO question do not describe outcomes on levels of clinical performance, or patient outcome. All studies for this PICO are manikin-based and participants were all adults. Manikin studies are the standard method for AED training and assessment. Substantial heterogeneity was found for interventions and controls, and for time points of assessment. Except for one study, none investigated AED alone. All other studies address the whole sequence of BLS with primary outcomes on chest compression quality. Proposed Consensus on Science statements Dallas 2015 We specified 4 sub-questions to account for the nature of training alternatives. 1. lay persons: self-instruction without (or with minimal) instructor involvement vs. traditional instructor led course 2. HCPs: self-instruction without (or with minimal) instructor involvement vs. traditional instructor led course 3. lay persons: self-instruction combined with instructor led vs. traditional course. 4. HCPs: self-instruction combined with instructor led vs. traditional course. Proposed Consensus on Science statements Dallas 2015 For 1. “self-instruction without (or with minimal) instructor involvement vs. traditional instructor led course for lay persons” we identified important outcomes with low quality of evidence with the following studies: De Vries 2010, 1004: For two of the investigated DVD-based teaching methods, the relative risk to pass the overall test was only 0.36, and 0.35. Reder 2006, 443 found a small non-significant inferiority for a computerlearning-only course after two months. Roppolo 2007, 276: described no significant difference of AED performance (time to first shock and AED placement) for a video-self learning intervention of 30 min. Meischke 2001, 216, investigating training for senior citizens (video-selftraining of 11 min + 45 min manikin training + minimal instructor) found no significant difference compared to the control group. This study also suggests a saving of resources by the alternative training method. Proposed Consensus on Science statements Dallas 2015 For 2. “self-instruction without (or with minimal) instructor involvement vs. traditional instructor led courses in HCPs” we identified important outcomes with very low quality of evidence with the following studies: Ropollo 2011, 319, showed that a pure self-instructed training was as efficient as traditional training but testing was limited to the end of the course. De Vries 2008, 76, did not find differences between groups, but reported significant time (and financial) savings. However, sample size was very low. Miotto 2010, 328, found worse results with a theory-only training, but was flawed due to an inadequate control group. Proposed Consensus on Science statements Dallas 2015 For 3. “self-instruction combined with instructor led vs. traditional courses for lay persons” important outcomes were identified, but the quality of evidence was low for the following studies: Reder 2006, 443, showed that interactive computer session of 45 min + 45 min instructor based practice led to comparable results as a traditional course of the same duration. Interestingly, AED skills remained rather stable over 2 months, while CPR skills deteriorated significantly. De Vries 2010, 1004, showed, that a 9 min DVD + manikin training + scenario training was inferior to traditional training, with a relative risk to pass the overall test of 0.55, which - notably - increased to 0.84 after two months. This may indicate a potential learning effect of the short post-course test Proposed Consensus on Science statements Dallas 2015 For 4. “self-instruction combined with instructor led vs. traditional courses in HCPs” we identified important outcome with low quality of evidence. A benefit could be shown in terms of reducing training time, while performance was slightly reduced. Ropollo 2011, 319 demonstrated that 40 min skills lab + instructor led to correct AED use, but a higher rate of mistakes in AED operations. De Vries 2008, 76, did not find differences between groups, but reported significant time (and financial) savings. However, sample size was very low. Dallas 2015 Draft Treatment Recommendations For lay persons we can give a weak suggestion to combine self-instruction teaching methods of shorter durations with practical hands-on training. No recommendation can be given for isolated selfinstruction without involvement of a trainer. For HCPs we suggest shorter duration of trainings and/or self-directed teaching methods. All these suggestions are based on low evidence studies, due to outcomes with low clinical relevance. We did not identify any evidence to address the critical outcome of “neurologically intact survival”. Knowledge Gaps (AED training methods) Dallas 2015 If isolated questions of AED trainings are to be answered, studies are needed where the primary objective is AED performance. Study designs should include adequate sample sizes and participants. The duration of effective AED training still is unclear. The effect and proper time point of brief refresher trainings should be evaluated. Most suitable methods to train children are not known yet. Overall, clinical outcomes (ROSC, discharge from hospital, intact neurological outcome) which may be related to AED training should be aimed at. However, this might not be feasible given the low probability of an individual to witness cardiac arrest. Next Steps Dallas 2015 This slide will be completed during Task Force Discussion (not EvRev) and should include: Consideration of interim statement Person responsible Due date