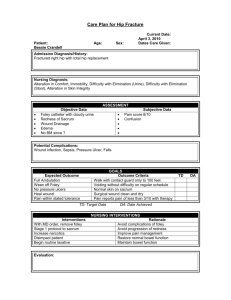
Stork test
advertisement

Valeria Pelvis Course Day 1 Student’s issues with the pelvis: 1. Effective TTT 2. Pelvic floor assessment 3. Interpretation of findings – lack of basics & incomplete diagnosis. 4. Anatomy – SIJ movement? Pelvis: Components – posture/force. Focus on lack of movement. Use the skin as a way in – not digging in. Interpretation – rule in and rule out certain relations. Relate qualities of the TLF Case study: 61 yoa M. B pelvic inflair. Structural assessment: will change each session 1. +ve findings 2. Reject –ve findings 3. Open minded 4. Be curious 5. Use “impression” of the structures on the patient’s skin. Standing pelvic assessment: 1. Kneel on floor. Use MCP of index finger – come from above B and keep soft onto skin above iliac crest. Feel for different density of tissue. Listening station – feel, possibly for anterior or posterior, do not interpret what it means. 2. Go with skin anterior on one side and then posterior. Then recheck the other side anterior and posterior. Do not interpret – go for side of +ve finding of ↓ ROM. 3. Change hand position to thumbs now inferior B PSIS. Now ask patient to forward bend. This allows for findings of groin involvement +ve to one side – on forward bending you will feel avoidance in patient on that side – possible involvement of hips/lower abdominal/groin/pubis > more ideas for assessment. Feel how skin is pulling through the iliolumbar ligaments and TLF. Should B PSIS move at same time. One PSIS may come before the other. The one not opening is the +ve finding. Feel for restriction in groin/hip when bending forward – the patient will avoid that side on flexion after 50°. L5/S1fixation usually the sacrum hooks up on flexion of LSp and can be differentiate with the SIJ > differentiation of the Lumbars from the sacrum. 4. Stork test: squat down and kneel. Applicators under PSIS and on S2 on ipsilateral side. Get patient to ipsilateral hip flex and hold with opposite hand. The PSIS thumb should roll posterior and inferior. +ve test is that the PSIS (innominate) does not move inf and post on ipsilateral hip flexion. Test contralateral hip flexion with palpation of sacrum using contralateral innominate. If the sacroiliac ligaments are good the sacrum should follow the movement and should go down (counternutate). If these ligaments have an issue will feel that there will be a struggle in the sacral ligamentous tissue. This will differentiate the SIJ on one side and the sacrum from the innominate. However this does give you a diagnois just yet. 5. Trendelenberg test: Patient lifts hip flexion. Have hands into the waist. A true +ve trendelenberg is a true ipsilateral drop on ipsilateral hip flexion. This shows a true muscular weakness of the gluteal medius on the EXT hip side (contralateral side). It is not a true weakness if there is a slight dip – the GMed may not be functioning so well. There should be a normal dip in contralateral gluteus medius on ipsilateral hip flexion. Muscle Att Function Antagonist Gluteal maximus Iliac crest, sacral EXT of hip and Psoas border laterally, trunk and EXT coccyx ITB, gluteal ROT of hip. tuberosity, saxcrotuberous ligament Gluteal Medius Between ABD and INT intermediate and ROT inferior gluteal line, Stabilises the greater trochanter pelvis Adductors 6. Gossip test: Hips EXT ROT and then bend one knee and then the other. Test Results Expected result Standing palpation L or R innominate Restriction = +ve Anterior/Posterior finding PSIS with Flexion L or R PSIS restriction PSIS should open +ve is restriction Stork test Test for PSIS with PSIS should move ipislateral hip flexion posterior and inferior Test ipsilateral S2 Sacrum should move (sacrum) with inferiorly (counter- contralateral hip nutate) flexion Sitting pelvic assessment: 1. For +ve stork test. Patient is seated with feet on floor. Pelvic floor is off stretch when seated; sacrum, ischium and innominate is taken out of the equation. With forward flexion and there is a much better response in the SIJ > there is an issue in the pelvis rather than the LSp. Supine pelvic assessement: 1. Check ASIS, put your body projected over the pelvis. Is the same pattern there? 2. Check pelvic floor from feet. Is the diamond shape more oblique or flat on one side. What is the shape of the diamond by Lifting patient’s legs at heels. Hold and feel for connection to pelvis. Light/heavy isn’t a diagnostic tool. Feel for the pelvic floor at feet and assess for shape. No diagnosis of gynae, Hip, LSp, innominate/sacrum – these are findings. 3. Check each leg one at a time and by bending knees, then extending knees and lifting up leg more you go further up the leg into the pelvis, LSp and thorax. Prone sacral assessment: 1. Sacral assessment prone: Go onto inferior angle of sacrum. Hold onto B PSIS down to inferior angle B and make a shape with both hands (fingers at S4/S5 and thumbs at S2/PSIS). Sacrum recoil TTT: High on left and low on the right > pisiforms onto superior right (recoil downwards) and inferior angle (recoil upwards). For opposite presentation do the reverse. Gluteus max tech: thumb into sacral origin with reinforced elbow. Add Long Lever into compression and not stretch, with passive EXT ROT of hip and active leg into the midline with thumb on sacral border. Recheck the sacrotuberous ligament 2. Diagnosis of sacral levels and sides prone: Check sacrum with crab hands one reinforcing the other and compression from S2 down feeling for restricted side and level. For counter-nutation of sacrum > iliolumbar and Lsp is under tension . For nutated sacrum > sacrotuberous and sacrospinous ligament under tension. TTT for counter-nutated sacrum: pressure on S2 of opposite side to plinth with elbow over the gluteals at lateral sacrum with hand holding leg below the calf. The other hand under the knee you created passive innominate anterior rotation using knee flex and thigh ext by leaning back > you nutate sacrum. TTT for nutated sacrum: Have pressure of elbow below S2 (ie S4) on the sacral/ilium line. Press on the sacrum into counternutation and then get patient to Txx the leg down the plinth and you encourage the movement of lengthening Txx the sacrum. TTT for Sacrotuberous ligament and midline gluteals: sidelying with knee flexed. One hand onto midline gluteal attachment, knee into belly/hip of operator and have support under the thigh and link hand onto forearm. Create flexion active and/or passive to put gluteal fascia under tension and wait for some release. TTT to iliacus for L/S restriction: with a sacrum more posterior to L5. Release the iliacus, which tilts the pelvis posteriorly rotation as a major hip flexor, leading to sacral release and take pressure off the L/S. Thomas test for hipflexor/quad tension: supine and get patient to hip flex actively holding knee in their hand. +ve test for hip flexor tension is opposite hip into flexion and +ve quad tension is opposite knee flexed. Technique awareness: Key to TTT is biomechanics of operator finding specific vector of own posture and using the patient’s body to minimise overuse of operators posture and making a technique energy efficient. Rotated pelvis: analysis of muscle bulk in multifidus and into TLF and relation to the hypotone in the transversus abdominus. Look for tone and bulk. Check rib elevation in breathing. Look at posterior ribs, relation to serratus posterior inferior, connect tissue palpation, obs and findings. Link TES into gluteals and TLF via TTT – hand on TES and TLF, resist into gluteals with elbow and get them to actively INT ROT hip prone. Groin issue: use skin into tension in thigh. Get patient to EXT ROT and you hold in resistance. Direct stretch of fascia into a bind. Wait for change and release. Can use this resistance to create gapping at the hip joint. With lower LSp pain check the Pelvis: Check for skin drag at iliac crest Check PSIS versus LSp standing & seated – to differentiate lumbosacral or innominate issue Stork test – is it innominate or sacrum? Trendelenburg test – is gluteal medius involved. Abdominal facscia and TLF test with flat hands and breath on ribs Seated flexion of spine Supine and prone check Seated - if the SIJ opens smooth on seated means that the LSP is not involved and the sacrum is therefore in lesion. Pelvic floor direct Hands under ischial tuberosities > stretch lateral/ anterior and posterior. Pelvic floor indirect From heels bi hold the LEx and fascial listen into the pelvic floor Do hip exam passive > see if this affects the pelvic floor and how it relates to presentation. ASSESS pubic symphysis > shotgun technique Prone assessment of sacrum > nutation/counter nutation/SB/ ROT Psoas SL TECH: to get iliacus int rot at hip Modify with leg up and patient leg balancing so u don't have to carry all the weight Psoas supine one leg off the couch and other let straight or bent. Hook operator foot into knee flexion and hip ext and Twist skin int rot with rocking. Leg tug: release groin first int rot of skin with active ext Rot. She uses compression into the fascia. Tug: put other foot on thigh to stop patient moving. Int Rot opp leg in flex and add > 1st in to POE > focus and then tug. You can build tension in planes > tug at tibia.