Welcome to the Jungle - Targeted Therapies,
Immunomodulatory Approaches, and the New
Drugs in HNSCC
Ezra E. W. Cohen
Moores Cancer Center
University of California San Diego
“Welcome to the jungle
We've got fun 'n' games
We got everything you want...”
GNR
Incidence
• 2014, US:
– ~50000 new cases
– ~8000 deaths
• Worldwide:
– 500000 new cases
– 6th leading cause of death
• M:F = 3:1
Ten Leading Cancer Types, United
States, 2012
CA Cancer J Clin 2012 Jan-Feb;62(1):10-29.
Risk Factors
•
•
•
•
Age (majority of patients >50 years old)
Tobacco
Alcohol
Viral
– Epstein-Barr virus (NPC)
– HPV (oropharynx)
• Hereditary (rare):
– Family history increases risk (3.5X)
– Rare genetic syndromes, e.g. Fanconi’s Anemia
HPV
Cancers with Increasing Incidence
Trends in the US
•CA Cancer J Clin. 2012 Jan 4.
Three-dose HPV vaccination
coverage among girls (13 to 17
years), by state, 2010.
New (HPV)–associated cancers
overall, and by sex, in the United
States, 2009
Sexual Behaviors and HNC
Diagnosis of
HPV-SCCHN
(case-case)
Risk of
HPV-SCCH
(case-control)
Number of sexual partners
+
+
History of oral-genital sex
+
+
History of anal cancer
+
+
Spouse with tonsil cancer
+
+
Assoc
Assoc
Behavior
Cervical CIS or cancer
HNC HPV
• Strong association with oropharynx,
especially tonsil, cancers
• Non-smokers, non-drinkers
• Younger age
• M:F = 3:1
• 90% of HNC cases with HPV are sub-type
16
Prognostic effect of HPV
•Langer CJ. Exploring biomarkers in head and neck cancer. Cancer. 2012 Aug 15;118(16):3882-92. 13
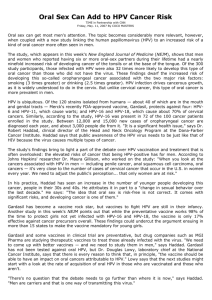
Human Papillomavirus and
Overall Survival After
Progression of
Oropharyngeal Squamous
Cell Carcinoma
C Fakhry et al
Overall survival after disease
progression
100
Survival (%)
75
p16-positive
54.6%
50
p<0.001
p16-negative
25
27.6%
0
0
No. at Risk
p16-positive 105
p16-negative 76
1
Years after Progression
61
27
2
51
19
15
DE-INTENSIFICATION
…as an approach to address
HPV related disease and good
prognosis
E1308
Induction followed by IMRT/Cetuximab
INDUCTION
(3 cycles)
ELIGIBILITY
Stage
III/IVa,b
Resectable
HPV+
Oropharynx
S
I
M
U
L
A
T
I
O
N
CONCURRENT
Paclitaxel 90
mg/m2 q 7d
CDDP
75mg/m2 q21d
IMRT 54Gy/30 fxs
CR*
Cetuximab
250mg/m2
qwk
Cetuximab 250mg/m2
qwk
CONCURRENT
<CR
IMRT 69.3Gy/33fxs
Cetuximab 250mg/m2 qwk
Cetuximab loading dose = 400mg/m2 on Day1 of Cycle1 with Induction
* CR indicates clinical CR and in patients with near CR will undergo biopsies
of primary site to confirm pathological CR
Phase II Randomized Trial of Transoral Surgical
Resection followed by Low-dose or Standard-dose
IMRT in Resectable p16+ Locally Advanced
Oropharynx Cancer (E3311)
p16+, Stage III/IV (cT1-2N1-N2b) OPSCC
Credentialing of surgeon required as part of site
participation in the trial
Stratify by stage and smoking status
Trial Schema
Risk-Stratified IMRT
Arm 1
TORS
Nmax = 54
T1-4a, N1-3
HPV+ OPSCC
Amenable to TORS
B
I
O
P
S
Y
Induction Chemotherapy
3 cycles
pCR or
pT1-2 N0-1
(-) margin, no ECE
Observe
Arm 2
Cisplatin 75 mg/m2/q3wk
TORS,
SLND
Paclitaxel 90 mg/m2/week
BYL719 daily
Close margin,
≥pN2, or PNI/LVI
60 Gy
IMRT
9 weeks
Arm 3
*
*FDG/PET-CT scan
*
(+) margin, ECE
66 Gy
IMRT
+
Weekly
Cisplatin
Treatment Overview
• Early stage (I, II): single modality – RT or
surgery
– 80-90% long-term survival
• Advanced stage (III, IVA, IVB): multi-modality
therapy – surgery/RT/chemotherapy
– 50% long term survival
• Recurrent/Metastasis
– 15% can be salvaged (surgery, re-RT)
– Palliative systemic therapy
EGFR Directed Therapy
Cetuximab Phase III Study
Stratify by
Karnofsky score:
90-100 vs. 60-80
Regional Nodes:
Negative vs. Positive
Tumor stage:
AJCC T1-3 vs. T4
RT fractionation:
Concomitant boost
vs. Once daily
vs. Twice daily
R
A
N
D
O
I
M
I
Z
E
Arm 1
Radiation therapy
Arm 2
Radiation therapy
Cetuximab, weekly
Phase III: Cetuximab Plus RT for
SCCHN: Results
Locoregional Control
47% vs 34% at 3 years
P<0.01 at 3 years
OS
55% vs 45% at 3 years
P=0.05 at 3 years
Bonner. N Engl J Med. 2006;354:567. Copyright © [2006] Massachusetts Medical Society. All
rights reserved.; Posner. N Engl J Med. 2006;354:634.
EXTREME - Study design
Randomized
Group A
Cetuximab 400 mg/m2 initial dose
then 250 mg/m2 weekly +
EITHER carboplatin (AUC 5, d1)
OR cisplatin (100 mg/m2 IV, d1)
+ 5-FU (1000 mg/m2 IV, d1-4):
3-week cycles
Group B
EITHER carboplatin (AUC 5, d1)
OR cisplatin (100 mg/m2 IV, d1)
+ 5-FU (1000 mg/m2 IV, d1-4):
3-week cycles
6 chemotherapy cycles maximum
Cetuximab
No treatment
Progressive disease or unacceptable toxicity
Overall Survival
1.0
|
0.9
| ||
|
|
CTX only
CET + CTX
|
|
|
Survival Probability
0.8
||
HR (95%CI): 0.797 (0.644, 0.986)
Strat. log-rank test: 0.0362
|
0.7
|
0.6
0.5
10.1
mo
|
7.4 mo
0.4
|
0.3
0.2
|
| |
| |||| | | |
|
| |
|
|| |||
| ||
||
|| | |
||
||
| |||
|
|||
|||
| | | | ||
|
|||| | | |
|| | |
| | | || ||
0.1
0.0
0
Patients at Risk
CTX only 220
CET + CTX 222
3
6
9
12
15
18
21
24
Survival Time [Months]
173
184
127
153
83
118
65
82
47
57
19
30
8
15
1
3
Afatinib versus methotrexate as second-line
treatment for patients with R/M HNSCC who
progressed after platinum-based therapy:
primary efficacy results of
LUX-Head & Neck 1, a Phase III trial
J-P. H. Machiels, R. I. Haddad, J. Fayette, L. F. Licitra, M. Tahara,
J. B. Vermorken, P. M. Clement, T. Gauler, D. Cupissol, J. J. Grau,
J. Guigay, F. Caponigro, G. de Castro Jr, L. de Souza Viana,
U. Keilholz, J. M. del Campo, X. Cong, L. Svensson, E. Ehrnrooth,
and E. E. W. Cohen on behalf of the LUX-H&N 1 investigators
LUX-Head & Neck 1: study design
Patients with incurable R/M HNSCC
progressing on/after first-line
platinum-based therapy (N=474)
Randomisation (2:1)
Stratified by: ECOG PS (0 vs 1) and
prior use of EGFR mAb therapy (Yes/No)
Afatinib
40 mg orally once daily
(n=316)
Methotrexate
40 mg/m2 IV weekly
(n=158)
Primary endpoint: PFS
Key secondary endpoint: OS
Secondary endpoints: ORR, patient-reported outcomes, safety
Primary endpoint: PFS independent review
Estimated PFS probability
1.0
Afatinib
MTX
(n=322)
(n=161)
275 (85.4)
135 (83.9)
2.6
1.7
0.80 (0.65–0.98)
0.030
PFS event, n (%)
Median PFS (months)
HR (95% CI)
Log-rank test p-value
0.8
0.6
42.8%
0.4
30.5%
0.2
0
0
No. of patients
Afatinib
322
MTX
161
3
6
9
Time (months)
12
15
18
93
28
26
6
9
2
3
0
1
0
0
0
CI, confidence interval; MTX, methotrexate
Overall tumour response
Percentage of patients
60
60
50
50
†
Afatinib
Methotrexate
49.1
38.5
40
40
30
30
20
20
10
10
*
10.2
5.6
00
ORR
afatinib
*Odds
DCR‡
mtx
ratio: 1.9 (0.88–4.14); p-value = 0.101
ratio: 1.5 (1.03–2.26); p-value = 0.035
‡Disease control rate (DCR): includes objective response and stable disease
†Odds
Overall survival
Estimated OS probability
1.0
Afatinib
MTX
(n=322)
(n=161)
OS event, n (%)
237 (73.6) 121 (75.2)
Median OS (months)
6.8
6.0
HR (95% CI)
0.96 (0.77–1.19)
Log-rank test p-value
0.700
0.8
0.6
0.4
0.2
0
0
No. of patients
Afatinib
322
MTX
161
3
6
9
255
115
172
76
89
48
12
15
Time (months)
53
29
28
16
18
21
24
27
14
9
6
7
1
3
0
0
Time to deterioration of pre-specified
patient-reported outcomes*
Global health status
Estimated probability
1.0
0.74 (0.56–0.97);
0.027
HR (95% CI); p-value†
0.8
0.6
Afatinib
Methotrexate
0.4
0.2
0
0
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
1.0
Pain
0.8
HR (95% CI); p-value†
Swallowing
1.0
0.73 (0.55–0.96);
0.022
0.6
0.4
0.2
0
Estimated probability
Estimated probability
Time (months)
HR (95% CI); p-value†
0.8
0.67 (0.50–0.89);
0.004
0.6
0.4
0.2
0
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21
Time (months)
0
1
2
3
4
5
6
7
8
9 10 11 12 13 14 15 16 17 18
Time (months)
*Assessed using European Organization for Research and Treatment of Cancer (EORTC) questionnaire QLQ-C30 and Head and Neck
cancer-specific module (QLQ-H&N35) for pain (composite of items 31–34) and swallowing (composite of items 35–38).
†Based
on log-rank test.
Molecular
Phenotyping
COMPREHENSIVE
GENOMIC
CHARACTERIZATION OF
SQUAMOUS CELL
CARCINOMA OF THE
HEAD AND NECK
Neil Hayes, MD, MPH
UNC Chapel Hill
Lineberger Comprehensive
Cancer Center
ASCO
6/3/2013
Significantly mutated genes in HNSCC by
whole exome sequencing
Analysis – Juok Cho, Peter Hammerman, Carrie Sougnez
COSMIC
CDKN2A
17%
FAT1
na
TP53
44%
CASP8
na
JUB
na
PIK3CA
6%
NOTCH1
14%
MLL2
7%
NSD1
6%
HLA-A
na
TGFBR2
na
HRAS
8%
EPHA2
na
RB1
na
NFE2L2
5%
KEAP1
na
B2M
na
RAC1
na
40
Deregulation of signalling pathways and transcription factors.
MS Lawrence et al. Nature 517, 576-582 (2015) doi:10.1038/nature14129
Cancer Immunotherapy
Immunotherapy
Harnessing the body’s
own immune system to
fight cancer
Surgery
Radiotherapy
Chemotherapy
Removal of the
tumor
Energy delivery to specific
anatomical site
Drugs designed to exploit
cancer mutations
Pursuing Immunotherapy in
Head and Neck Cancer
KEYNOTE-012 – Study Design
• Multi-center, non-randomized Phase Ib HNSCC expansion
cohort
• Multi-cohort trial* HNSCC cohort
Recurrent or metastatic
Head and Neck Cancer
- PD-L1 positive
- Investigator assessed
HPV status
HPV(-)
cohort
Pembrolizumab
HPV(+)
cohort
Pembrolizumab
10mg/kg Q2 weeks
10mg/kg Q2 weeks
*Additional cohorts included: Bladder Cancer, Triple Negative Breast Cancer, Gastric Cancer
•Presented by: Tanguy Seiwert
Treat
until
PD*
Efficacy: Waterfall Plot*
100
HPV (-)
HPV (+)
Change From Baseline, %
80
60
40
20
0
–20
–40
–60
51% (26/51) of patients had decreased tumor burden
–80
–100
Subjects
Best percent change from baseline in target lesions (site assessment) delineated by HPV status
*as of May 23, 2014; Includes only patients with RECIST measurable lesions at baseline and at least 1 follow-up scan
(n=51)
•Presented by: Tanguy Seiwert
Best Overall Response*
56 pts evaluable for
Total Head/neck
HPV (+)
HPV (-)
N=56†
N=20
N=36§
Response
n (%)
1 (1.8)
95% CI†
(0.0, 9.6)
n (%)
95% CI†
n (%)
95% CI†
1 (5.0)
(0.1, 24.9)
0 (0.0)
(0.0, 9.7)
Partial Response
10 (17.9)
(8.9, 30.4)
3 (15.0)
(3.2, 37.9)
7 (19.4)
(8.2, 36.0)
Best Overall Response
(Complete + Partial)‡
11 (19.6)
(10.2, 32.4)
4 (20.0)
(5.7, 43.7)
7 (19.4)
(8.2, 36.0)
Stable Disease
16 (28.6)
(17.3, 42.2)
8 (40.0)
(19.1, 63.9)
8 (22.2)
(10.1, 39.2)
Progressive Disease
25 (44.6)
(31.3, 58.5)
7 (35.0)
(15.4, 59.2)
18 (50.0)
(32.9, 67.1)
4 (7.1)
(2.0, 17.3)
1 (5.0)
(0.1, 24.9)
3 (8.3)
(1.8, 22.5)
Response Evaluation
Complete Response
No Assessment
Based on RECIST 1.1 Per site assessment; includes confirmed and unconfirmed responses
†61 patients eligible for treatment; 60 patients dosed; 56 patients eligible for pre-defined full analysis set.
‡A
single patient with PD followed by PR on treatment was classified as PR.
§Includes
† Based
2 patients for whom HPV data unavailable.
on binomial exact confidence interval method.
• PD-L1 expression correlates with Response
• Using a Youden-Index derived, preliminary PD-L1 cut point:
Above cutpoint: 45.5% (5/11) RR
Below cutpoint: 11.4% (5/44) RR
*as of May 23, 2014
•Presented by: Tanguy Seiwert
Subjects
Time on treatment and disposition*
Complete Response
Partial Response
Treatment Ongoing
0
4
8
12
16
20
24
28
32
36
40
44
48
Treatment Exposure, weeks
Swimmer plot of all patients who experienced CR or PR.
8 additional patients had SD >6 months, of which 7/8 remain on treatment.
*as of May 23, 2014
•Presented by: Tanguy Seiwert
Toll-like Receptor 8 (TLR8) Pathway is Important
in Human Immune Responses
• Activation induces potent Th1 immune response
• Expressed on myeloid dendritic cells (CD11c+), monocytes
(CD14+), and natural killer cells (CD56+) in humans
• Induces significant IL-12 production in humans
• Can be activated by small molecule agonists
•58
A Randomized, Double-Blind, Placebo-Controlled
Study of Chemotherapy Plus Cetuximab in
Combination with VTX-2337 in Patients with
Recurrent or Metastatic Squamous Cell Carcinoma
of the Head and Neck
Active8
Study Schema
175 patients with locally advanced or metastatic head/neck cancer
Primary endpoint: progression-free survival
Mutation frequency among cancers of different histotypes
Mutational screen of 305 HNSCC exome sequences deposited in TCGA
HNSCC tumors express missense mutations
Mutational screen of 305 HNSCC exome sequences deposited in TCGA
HNSCC tumors express missense mutations
Project: Exome-guided neoantigen discovery in HNSCC
HNSCC pt
In office/clinic
1) Tumor: FNA, core, or excision biopsy
2) <1 ml PBL
salvage surgery
Immune monitoring of
checkpoint blockade trials
gDNA & mRNA
Whole Exome Sequencing
expand TIL with
‘antigenic mutanome’ peptides
Establish PDX model
& perform ACT with ‘improved” TIL
“antigenic
mutanome”
Test peptides for recognition
by autologous T cells w ELISPOT
(use prediction algorithm as needed)
Bioinformatics:
Reassembly, alignment, QC
mutation calling
Confirm SNVs in expressed
genes (RNAseq)
CONCLUSIONS
• EGFR inhibitors still the only proven
“targeted therapy” in HNSCC
• HPV is a recognized prognostic marker
– Other stratification factors needed
• Immunotherapy extremely promising
– Phase 3 trials underway in R/M disease likely
to complete accrual this year
– PDL1 being explored as predictive biomarker