Lambert Eaton: An Elusive Diagnosis
advertisement

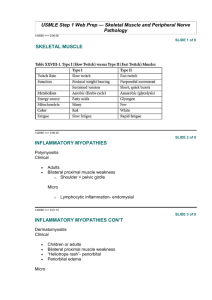
Lambert Eaton: An Elusive Diagnosis Julie Silverman, MD Internal Medicine R3 University of Washington November 4, 2011 Lambert-Eaton Myasthenic Syndrome (LEMS) Lambert-Eaton Myasthenic Syndrome (LEMS) Disorder of the neuromuscular junction in which antibodies are made against presynaptic voltagegated calcium channels Lambert-Eaton Myasthenic Syndrome (LEMS) Disorder of the neuromuscular junction in which antibodies are made against presynaptic voltagegated calcium channels Symptoms include proximal muscle weakness, fatigue and autonomic dysfunction Lambert-Eaton Myasthenic Syndrome (LEMS) Disorder of the neuromuscular junction in which antibodies are made against presynaptic voltagegated calcium channels Symptoms include proximal muscle weakness, fatigue and autonomic dysfunction Annual Incidence = 0.48 per million population Lambert-Eaton Myasthenic Syndrome (LEMS) Disorder of the neuromuscular junction in which antibodies are made against presynaptic voltagegated calcium channels Symptoms include proximal muscle weakness, fatigue and autonomic dysfunction Annual Incidence = 0.48 per million population There is a high association with malignancy Initial Presentation Ms. S: 70-year-old, previously healthy JapaneseAmerican woman presented to her primary care physician with concerns of dyspnea, orthopnea and peripheral edema. Review of systems further revealed nausea, muscle weakness, joint and back pain, and excessive thirst. History PMHx HTN HLD DJD Mild mitral insufficiency PSHx Unilateral oophorectomy (s/p MVA) Appendectomy (s/p MVA) Hysterectomy (for benign reasons) L knee arthroscopy L knee arthroplasty Social Hx Married Retired from Kent school district Lifelong non-smoker Rare EtOH Family Hx Mother died from asthma in 40s Medications Losartan Atenolol Triamterene-HCTZ Simvastatin Omeprazole Pyridoxine Cyanocobalamin Vitamin C Flax seed oil Diagnostics Diagnostics Diagnostics Diagnostics Diagnostics Diagnostics Diagnostics Diagnostics NO DIAGNOSIS Continued Symptoms Ms. S returned to PCP with worsening dry mouth, anorexia and unintentional 20 pound weight loss. More Diagnostics More Diagnostics More Diagnostics More Diagnostics More Diagnostics More Diagnostics DIAGNOSIS: Depression? Hospitalized again and again and again… Hospitalization # 3 Hospitalization # 4 Hospitalization # 5 CC: “nausea and fatigue” CC: “difficulty swallowing” CC: “slumped on floor” Hospitalized again and again and again… Hospitalization # 3 Hospitalization # 4 Hospitalization # 5 CC: “nausea and fatigue” CC: “difficulty swallowing” CC: “slumped on floor” Workup: barium swallow, esophageal manometry, videoflouroscopy, laryngoscopy, CT neck, CT head Consults: GI, neurology, ENT, rehab medicine, speech therapy Diagnoses: Medication-related? Deconditioning? Poor nutrition? Neurology Consults “I do not find evidence of any dysfunction of central or peripheral nervous system including any evidence of peripheral myopathy or neuromuscular junction disease.” “At this point I would be reassured on clinical grounds that there is no significant neurological explanation and I do not recommend or see specific need to proceed with any specific neurological diagnosis… She does have a dry mouth which raises the question of a Lambert-Eaton syndrome and that unlikely possibility can be further probed with an anti-calcium channel antibody test and with neurophysiologic studies.” Finally… Finally… Reason for admission: Na 112 (previously low 130s) Finally… Reason for admission: Na 112 (previously low 130s) Physical exam: No fatiguability or diplopia elicited with sustained upgaze x 1 min Normal muscle mass and tone Strength 4-5 in all muscle groups; poor effort with give way weakness Declined gait assessment Lambert’s sign absent DTRs 1+ B biceps; 0 in brachioradialis, patella, Achilles Finally… Reason for admission: Na 112 (previously low 130s) Physical exam: No fatiguability or diplopia elicited with sustained upgaze x 1 min Normal muscle mass and tone Strength 4-5 in all muscle groups; poor effort with give way weakness Declined gait assessment Lambert’s sign absent DTRs 1+ B biceps; 0 in brachioradialis, patella, Achilles Labs: ESR 82, CRP 216 CK normal ANA 1:80 with negative reflexive panel Finally… Reason for admission: Na 112 (previously low 130s) Physical exam: No fatiguability or diplopia elicited with sustained upgaze x 1 min Normal muscle mass and tone Strength 4-5 in all muscle groups; poor effort with give way weakness Declined gait assessment Lambert’s sign absent DTRs 1+ B biceps; 0 in brachioradialis, patella, Achilles Labs: ESR 82, CRP 216 CK normal ANA 1:80 with negative reflexive panel Rheumatology and Neurology consults Electrodiagnostic Evaluation with Repetitive Nerve Stimulation: “moderately severe disorder of presynaptic neurotransmission with findings supportive of an endplate myopathy” Electrodiagnostic Evaluation with Repetitive Nerve Stimulation: “moderately severe disorder of presynaptic neurotransmission with findings supportive of an endplate myopathy” Compound Muscle Action Potentials (CMAP) Post-Exercise Facilitation Exercise testing in LEMS with median nerve stimulation and abductor pollicis brevis muscle recorded Baseline Immediately after 10 seconds of maximal voluntary exercise Malignancy Workup Tumor markers (CA19-9, CA27.29, CEA) within normal limits CT chest/abdomen/pelvis no evidence of malignancy PET scan no evidence of occult malignancy Bronchoscopy not performed Treatment Initially started on pyridostigmine (anticholinesterase inhibitor) 3,4-DAP (K channel blocker) added Once PET results returned, prednisone added At one month follow-up, patient’s strength had returned. She was able to perform ADLs and IADLs. Conclusions LEMS can be difficult to diagnose. At time of diagnosis, Ms. S had been hospitalized 6 times at 5 different hospitals seen by at least 12 specialists undergone at least 9 CT scans, ultrasounds, EGD, colonoscopy, laryngoscopy, blood work While the prevalence is low, recognition of LEMS is critical because treatment can be effective in reducing symptoms up to 70% of patients have an underlying malignancy Signs and Symptoms Symptoms Signs Proximal limb weakness Legs > arms Fatigue or fluctuating sx Difficulty rising from sitting; climbing stairs Metallic taste in mouth Autonomic dysfunction Dry mouth Constipation Blurred vision Impaired sweating Proximal limb weakness Legs > arms Weakness on exam is less demonstrable than pt’s level of disability Hypoactive or absent muscle stretch reflexes Lambert’s sign (grip becomes more powerful over several seconds) Sluggish pupillary reflexes Thanks Drs. Susan Merel, Eric Kraus, Ken Steinberg Questions? Extra Slides Mechanism of Action SEMINARS IN NEUROLOGY/VOLUME 24, NUMBER 2 2004 Treatment for LEMS Treat underlying malignancy Pyridostigmine 3,4-DAP Cochrane Review 2011 “limited but moderate to high quality evidence” showing 3,4-DAP improved muscle strength scores and CMAP amplitudes Other possible treatments (plasma exchange, steroids and immunosuppressive agents) have not been tested in randomized controlled trials. Treatment for LEMS Myastenia Gravis vs. LEMS Both are acquired autoimmune disorders characterized by defective neuromuscular transmission LEMS MG Antibodies against voltage-gated Ca channels Antibodies about acetylcholine receptors Usually starts at extremities and moves up Usually starts at eyes and moves down Autonomic dysfunction present No autonomic dysfunction Diplopia and dysphagia uncommon Diplopia and dysphagia common Weakness improves with activity Weakness worsens with activity Associated with SCLC Associated with thymoma LEMS and Malignancy The overwhelming majority of cancers associated with LEMS are SCLC. Other malignancies include non-SCLC neuroendocrine carcinomas lymphosarcoma malignant thymoma Breast CA Stomach CA Colon and Rectal CA Prostate CA Bladder CA Kidney CA Gallbladder CA Basal cell carcinoma Leukemia Laboratory Workup Antibodies to voltage-gated calcium channels (VGCCs) have been reported in 75-100% of LEMS patients who have small cell lung cancer (SCLC) and in 50-90% of LEMS patients who do not have underlying cancer.