Osteoarthritis OA
advertisement

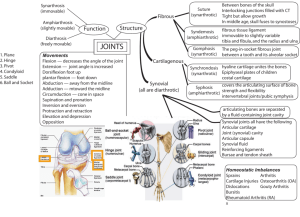
OSTEOARTHRITIS OSTEOARTHROSIS DEGENERATIVE JOINT DISEASE Prof. Dr. Ülkü Akarırmak DEFINITION Osteoarthritis OA is a degenerative disease of diarthrodial (synovial) joints, characterized by Breakdown of articular cartilage and proliferative changes of surrounding bones EPIDEMIOLOGY Osteoarthritis(OA) is the most common joint disease OA of the knee joint is found in 70% of the population over 60 years of age Radiological evidence of OA can be found in over 90 % of the population LIMITED FUNCTION OA may cause functional loss Activites of daily living Most important cause of disability in old age Major indication for joint replacement surgery CHARACTERISTICS OF OA OA is a chronic disease of the musculoskeletal system, without systemic involvement OA is mainly a noninflammatory disease of synovial joints No joint ankylosis is observed in the course of the disease CLASSIFICATION OF OA Primary OA Etiology is unknown Secondary OA Etiology is known AGE Primary OA > 40 years Direct correlation Aging process RISK FACTORS FOR PRIMARY OA Age Sex Obesity Genetics Trauma (daily) SECONDARY OSTOARTHRITIS Trauma Previous joint disorders; Congenital hip dislocation Infection: Septic arthritis, Brucella, Tb Inflammatory: RA, AS Metabolic: Gout Hematologic: Hemophilia Endocrine: DM ETIOLOGY OF OA Cartilage properties Biomechanical problem Morphology of Primary OA Primary Generalized OA STRUCTURE OF JOINT CARTILAGE Collagen (Type 2) Proteoglycan - Hyaluronic acid - Glycoseaminoglycan Water Condrocyte Regeneration and Degeneration PATHOLOGY OF OA Fibrillation Eburnation Osteophytes Subcondral cysts LABORATORY FINDINGS OF OA There are no pathognomonic laboratory findings for OA Laboratory analysis is performed for differential diagnosis RADIOLOGIC FINDINGS OF OA Narrowing of joint space (due to loss of cartilage) Osteophytes Subchondral (paraarticular) sclerosis Bone cysts RADIOLOGIC GRADE OF OA G1 G2 G3 G4 Normal Mild Moderate Severe Kellgren Lawrence Classification DIAGNOSIS OF OA CLINICAL FINDINGS Joint pain + RADIOLOGIC FINDINGS Osteophytes CLINIC OF OA SIGNS AND SYMPTOMS Joint pain - degenerative Stiffness following inactivity – 30 min Limitation of ROM – later stages Deformity – restricition of ADL OA OF KNEE JOINT (GONARTHROSIS) More common in obese females over 50 years of age Joint stiffness (<30 minutes) Mechanical pain Physical examination findings: Crepitus Pain on pressure Painful ROM and functional limitation Limitation of ROM in later stages of OA (first extension) Laboratory analysis within normal limits GENU VALGUM - ORTHOSIS RADIOLOGIC FINDINGS? GRADE 1 - 4? OA OF HIP JOINT More common in males over 40 years of age Joint stiffness Pain of hip, gluteal and groin areas radiating to the knee (N obturatorius) Mechanical pain Limited walking function COXARTHROSIS Physical examination: Antalgic limping Limitation of ROM (first internal rotation) Painful ROM Trendelenburg test positivity Leg length discrepancy Laboratory analysis within normal limits BIOMECHANICS X-RAY OF HIP OA Peripheral Joints Hands Feet ETIOPATHOGENESIS OF OA Age,gender Local Genetic biochemical Other factors OA effects ETIOPATHOGENESIS OF OA Dysfunction of joint cartilage Condrocyte function: 1- Degredative enzymes (metalloproteases) 2- Inhibitors Degeneration and regeneration functions are balanced IL-1 , degredative enzymes + synovial inflammation results: Breakdown of cartilage PATHOGENESIS OF OA Cytokines IL-1, IL-6, TNF- Cell destruction Membrane phospholipids Arachidonic acid Cox-1, Cox-2 IL-1 and metalloproteases have been found to play an important role in cartilage destruction. Local growth factors, especially transforming growth factor (TGF) are involved in the formation of osteophytes TREATMENT OF OA Symptomatic treatment Structure modifying treatment Surgical treatment STRUCTURE MODIFYING TREATMENT Hyaluronic acid injection (HA) Glycose amino glycans (GAG) PRIMARY PREVENTION OF OA ?? Regular exercises Weight control Prevention of trauma AIMS OF OA TREATMENT Pain relief Preservation and restoration of joint function Education Non-Pharmacologic Treatment of OA Patient education Weight loss (if overweight) Aerobic exercise programs Physical therapy Range-of-motion exercises Muscle-strengthening exercises Assistive devices for ambulation Patellar taping Appropriate footwear Lateral-wedged insoles (for genu varum) Bracing Occupational therapy Joint protection and energy conservation PHARMACOLOGIC TREATMENT OF OA Oral Systemic Medical Agents - Analgesics (acetaminophen) - NSAIDs - Opioid analgesics Intraarticular agents: Hyaluronan Glucocorticoids (effusion) Topical agents HAND OA - RESTING SPLINT SYMPTOMATIC TREATMENT OF OA Decrease of joint loading - Weight control - Splinting - Walking sticks Exercises - Swimming - Walking - Strengthening Patient education INDICATIONS OF SURGICAL INTERVENTION Severe joint pain, resistant to conservative treatment methods Limitation of daily living activities Deformity, angular deviations, instability INVASIVE METHODS Joint lavage Arthroscopy Cartilage grefting- genetic engineering Surgery Osteotomy Joint replacement QUESTIONS?