Reactive
advertisement

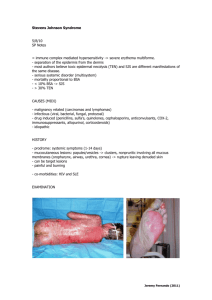
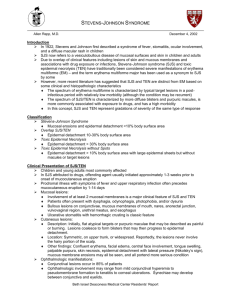
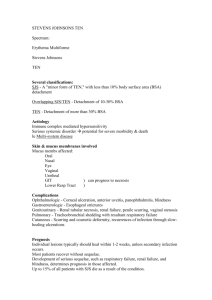
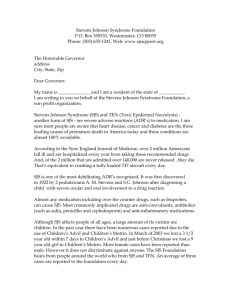
“Reactive” and Idiopathic Skin Diseases Rich Callahan MSPA, PA-C Fletcher Allen Dermatology Burlington, Vermont ICM I – Summer 2009 Overview • Erythema Multiforme (EM) • Erythema Nodosum (EN) • Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis (TEN) • Urticaria/Angioedema • Lichen Simplex Chronicus/Prurigo Nodularis • Lichen Planus EM – What is it? • An acute, common skin rash associated with a number of causative factors, although 50% of the time a precipitating cause is not found. • Classified as a reactive, inflammatory process of the skin, or “Hypersensitivity syndrome.” • Reactive change in dermal vasculature with overlying epidermal changes EM – Epidemiology/Causative Factors • Can be caused by drugs, infections (Herpes,) pregnancy, internal malignancy, acute URI, atypical pneumonia • ~50% idiopathic • Mostly see in younger patients, most common age range is 20-40 years • I have seen several patients who develop EM after HSV outbreaks (cold sores) EM – Clinical Presentation • Characteristic erythematous, target-shaped, urticarial papules, vesicles and bullae • Affects trunk, extremities, mucous membranes, palms/soles. • Lesions appear quickly in a symmetric pattern, usually first on dorsal hands/feet, then migrating along extensor extremities, then to trunk in severe cases. • Can be asymptomatic, pruritic or painful. • Occassionally, will manifest only as oral bullae and ulcerations. EM – Clinical Presentation • Eruption evolves over several days, may be preceded by prodromal symptoms including malaise, fever or burning/itching at sites where EM will later develop. • Presentation can be entirely non-diagnostic at first, then later dx’ed as EM when classic “target lesions” develop. • Entire course of disease usually 1 month or less. • Rarely life-threatening with extensive mucous membrane involvement, patches of vesiculation, etc EM - Diagnosis • EM is a clinical diagnosis based on patient history and disease presentation. • Skin biopsy seldom helpful in my experience as histologic findings can be non-specific at early stages of disease, which is when it tends to get biopsied. • Biopsy of target lesions generally diagnostic, but seldom biopsied as is an easy clinical diagnosis by that point! EM - Treatment • Mild cases do not require treatment. • Moderate cases respond well to a 1-3 week course of oral steroids (prednisone.) • Severe cases treated with IV steroids. • In recurrent cases with positive HSV association, I have used prophylactic therapy with oral antiviral meds (Valtrex) with good success. Erythema Nodosum – EN – What is it? • An acute panniculitis of the lower extremities with diverse causes • Considered a delayed hypersensitivity reaction to a number of possible antigens, I.e., it is a reaction to a concurrent disease or condition. • Most common cause today is streptococcal infection. • Can be precipitated by drugs, infections, sarcoidosis, misc. inflammatory disorders EN - Causes • • • • • • Infections Bacterial Fungal Viral GI parasites Drugs (esp. OCP’s) • • • • • • Cancer Concomitant Disease Sarcoidosis IBD Ulcerative Colitis Crohn’s Disease EN - Epidemiology • • • • Women >> men. Female: Male ratio is 5:1 Peak ages of incidence are 18 – 35 years. Extremely rare in the elderly. Historically, much less common in the modern area with advent of antibiotic drugs. EN – Clinical Presentation • Presents as development of painful red nodules, patches and plaques, usually on lower legs, over a period of 1-2 weeks. • Often preceded by prodromal symptoms of fever, malaise, arthritis and arthralgias. • Individual lesions begin as reddish, swollen papules on shins bilaterally, then grow into violaceous, indurated, tender patches and plaques which resolve in 1-2 weeks. • Eruption can recur in crops for months to years. EN - Treatment • Usually resolves spontaneously w/o treatment. • Symptomatic relief with rest and/or NSAID’s. • SSKI (supersaturated potassium iodide.) • Prednisone • ID and treatment of precipitating cause if possible. Stevens-Johnson Syndrome/Toxic Epidermal Necrolysis – What is it? • Both names represent a spectrum of disease with SJS being the less severe end. • A life-threatening condition characterized by large scale and widespread necrosis and detachment of epidermis, affecting both skin and mucosal surfaces of eyes (conjunctivae,) nares, mouth, anorectal/genital areas. • One of the few truly acute medical emergencies in Dermatology. SJS/TEN • Pathophysiology not entirely understood, but thought to be reaction in keratinocytes where cells accumulate foreign antigen and are stimulated to apoptosis (cell death) by T-cells. • Large areas of epidermis become necrotic and slough off in sheets • Results in massive transcutaneous water loss and usually secondary bacterial infection SJS/TEN - Causes • Most often caused by drugs, then infections, then rarely by a malignancy. • Drugs include: Sulfonamides, Bactrim/Septra, Quinolones, Cephalosporins, acetaminophen, phenobarbital, NSAID’s, cocaine, ginseng, allopurinol, fluconazole, many others. • Infections include influenza, HSV, Epstein-Barr virus, Cat-Scratch disease, histoplasmosis • Malignancies include carcinomas and lymphomas SJS/TEN Spectrum of Disease • Grade I - SJS: Less than 10% of Body Surface Area (BSA) affected. • Grade II - SJS/TEN Overlap: Between 10% and 30% BSA affected. • Grade III – TEN: Greater than 30% BSA affected. SJS/TEN Epidemiology/Morbidity/Mortality • Usually seen in Caucasians, male:female ration is 2:1. • Average patient is 20-40 years old, although occasionally seen in infants/elderly. • If BSA involvement 10% or less, mortality is 15% of cases. 30% or higher BSA involvement has mortality rate between 25% and 35% • Overall mortality for entire SJS/TEN spectrum of disease is 15% SJS/TEN – Clinical Presentation • Clinically manifests as erythematous and purpuric macules and target lesions, distributed over trunk, palms, soles and mucosal areas. Blister formation and sloughing/necrosis of skin follow. • Nikolsky Sign: Pushing down on blisters causes them to spread laterally with little resistance • Skin rash preceded by cough/URI symptoms. • Patients have fever, electrolyte imbalances, eye/mucous membrane involvement, pain, occassional lung involvement. SJS/TEN – Clinical Presentation • Mucosal lesions lead to widespread epidermal sloughing and crust formation. • Extensive disease can lead to scarring, stricture formation and partial loss of funcion of organ system involved. • Eye involvement includes corneal ulcerations and conjunctival injury which can lead to scarring and blindness. SJS/TEN - Treatment • Most often a reaction to drugs, so look for offending cause in all cases: Usually the newest drug on a patient’s list, within 1 to 4 weeks of starting it • Treatments are supportive, although oral prednisone is often used in an attempt to shorten duration of illness. • Other treatments include oral antihistamines, lidocaine gargles, liquid/soft diet, Burrow’s compresses, topical steroids to non-eroded areas, ophthalmology consult, antibacterial therapy for secondary infections. Urticaria/Angioedema • Urticaria presents as groups of itchy, pink/flesh-colored wheals • Caused by edema, or fluid accumulation in epidermis/superficial dermis • Papillary vascular plexus • Angioedema presents as broad, poorlydefined areas of swelling • Caused by edema of dermis and subcutis • Deep vascular plexus Urticaria/Angioedema • Wide Variety of • Physical Urticaria – Causes: Angioedema • 50-60% of cases • Infections idiopathic • Treatment usually • Allergies with antihistamines • Drugs and/or prednisone • Contact urticaria • Autoimmune and immunologic mediated LSC/Prurigo Nodularis • Lichenification of skin in direct reaction to repeated rubbing and scratching of skin • Skin becomes thickened with accentuation of skin markings • Scratching becomes pleasurable to patient • Dome-shaped, hyperpigmented papules and nodules in areas of lichenification • Often deeply excoriated • Hyperplasia of cutaneous nerves leads to enhanced sensitivity and pruritis Lichen Planus (LP) • Idiopathic eruption defined by the 4 P’s: • Pruritic, purple, polygonal papules • Tends to affect wrists, flexor extremities, lumbar areas, genitals, mucosa • Tends to last 6 months to one year • Leaves behind deep, long-lasting hyperpigmentation • Presence of Wickham’s striae diagnostic