2-6 - Europace
advertisement

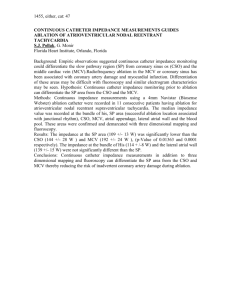
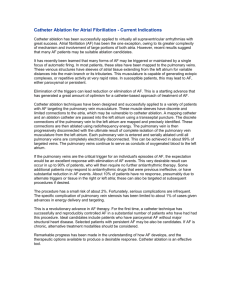
Appendix- Cost-effectiveness of radiofrequency catheter ablation as first-line treatment APPENDIX The cost-effectiveness of radiofrequency catheter ablation as firstline treatment for paroxysmal atrial fibrillation: results from a MANTRA-PAF substudy Brief title: Cost-effectiveness of radiofrequency catheter ablation as first-line treatment Mattias Aronsson, Håkan Walfridsson, Magnus Janzon, Ulla Walfridsson, Jens Cosedis Nielsen, Peter Steen Hansen, Arne Johannessen, Pekka Raatikainen, Gerhard Hindricks, Ole Kongstad, Steen Pehrson, Anders Englund, Juha Hartikainen, Leif Spange Mortensen, Lars-Åke Levin. 1. Information about appendix Most relevant model assumptions are presented in section 2. Assumptions about reversion rate, crossover rate and CHADS2-score are described in section 3 and 4. Supplementary data about model parameters are presented in section 5. Standard deviations presented in the table were used for probabilistic sensitivity analyses. The range of parameter values presented in the table was used when alternative scenarios were tested deterministically. All costs and prices are in Swedish krona (SEK). 8.7 SEK ≈ 1 Euro. A procedural model is presented in section 6. The importance of the time horizon is shown in section 7. 2. Assumptions The clinical benefit of catheter ablation is mainly driven by a reduced risk of ischemic stroke and events related to the use of oral anti-coagulation treatment. Patients not successfully treated with AAD will over time do crossovers to catheter ablation (see section 3). Crossover patients (from AAD to RFA) are expected to hold the same risk of events as patients randomized to RFA. Patients with known AF are expected to be treated with warfarin. Additional ablations were allowed in 50 % of the patients with AF recurrence >24 months after first ablations procedure. All assumptions were rigorously tested in sensitivity analyses. 3. Reversion and crossover The recurrence of AF during the first 24 months was obtained from the MANTRA-PAF trial for both the AAD- and RFA-treated patients. The crossover rate for first 24 months was obtained from MANTRA-PAF study data. 1 Appendix- Cost-effectiveness of radiofrequency catheter ablation as first-line treatment Recurrence of AF after first 24 months in patients treated with AAD was obtained from Pappone et al (1). A non-linear model was used as the reversion rate to AF declined with time. The long-term effectiveness of RFA is currently not well established due to a continuous development of the RFA-technique. The effectiveness of RFA may be better than in the MANTRA-PAF study and the other studies used for the reversion rate calculation (2-6). The parameter was rigorously tested in sensitivity analyses. No relevant data regarding crossover rate in patients treated with RFA were identified during the literature search. We made the assumption that patients with PAF not successfully treated with AAD will do crossovers to RFA, as second-line RFA are recommended in guidelines and been proven both clinical efficient and cost-effective. Three scenarios with different readiness of offering RFA to AADpatients with PAF are shown in the manuscript. 4. CHADS2-Score CHADS2-score were used to predict the stroke risk because CHA2DS2-VASc were not widely used when the MANTRA-PAF study were initiated. The hypothetic population in the model was expected to have the same distribution between the CHADS2 states as the MANTRA-PAF study population (7). The CHADS2 –score increased thru the model as patients become older than 75 year and experienced strokes. 2 Appendix- Cost-effectiveness of radiofrequency catheter ablation as first-line treatment 5. Supplementary tables with important parameters Determ inistic Standar d error Sensitivity test range Distribution Alfa Beta Reference/Comment Monthly drug cost Beta blockers 31 (15 – 60) Deterministic ACE-inhibitors 156 (50 – 300) Deterministic Monthly warfarin cost >24 months Drugs and monitoring visits 517 (250 – 750) Deterministic (8) Discounting Discount costs 3% (0 – 10) Deterministic Guidelines from Swedish authority TLV. Discount effects 3% (0 – 10) Deterministic Guidelines from Swedish authority TLV. QALY-decreases QALY-loss from Ischemic stroke (yearly) QALY-loss from Hemorrhagic stroke (yearly) QALY-loss from MI (first year) QALY-loss from symptomatic AF QALY-loss from RFAprocedure www.FASS.se/, Unpublished MANTRAPAF-data www.FASS.se/, Unpublished MANTRAPAF-data 0.15 0.012 (0 – 0.3) Beta 132.3 750 (9) Expected to include the effects disability 0.3 0.041 (0 – 0.45) Beta 36.8 85.87 (9) Expected to include the effects disability (0 – 0.3) 0.19 (10) 0.13 0.025 (0 – 0.2) Normal Unpublished MANTRA-PAF-data 0 0 (0 – 0) Normal Only for sensitivity analyses QALY overall population 3 Appendix- Cost-effectiveness of radiofrequency catheter ablation as first-line treatment 40–49 0.863 0.009 Normal 50–59 0.839 0.010 Normal 60–69 0.808 0.011 Normal 70–79 0.794 0.015 Normal 80–88 0.733 0.028 Normal Operation-modeltransitions Procedure mortality Tamponade Stroke Stenosis Hemothorax Femoral pseudo aneurysm Transient ischemic attack Artero venous fistulae 0.046 % 1.22 % 0.28 % 0.74 % 0.16 % 0.54 % 0. 66 % 0.42 % Relative risk Relative risk NSR 0.625 0.3036 ADR Fatal ADR per year (year >2) 0.32% 0.05% Crossover and reversion rate per months Crossover rate >24 months Reversion rate AAD 1.1 % 1.9 % Beta Beta Beta Beta Beta Beta Beta Beta 0.3 (11) Used for adjusting MANTRA-PAF data for age in the model (11) Used for adjusting MANTRA-PAF data for age in the model (11) Used for adjusting MANTRA-PAF data for age in the model (11) Used for adjusting MANTRA-PAF data for age in the model (11) Used for adjusting MANTRA-PAF data for age in the model 4 107 20 53 14 47 47 37 8741 8638 7134 7101 8731 8698 7107 8708 (12) Used >24 months (12) Used >24 months (12) Used >24 months (12) Used >24 months (12) Used >24 months (12) Used >24 months (12) Used >24 months (12) Used >24 months Lognormal (13) (0 – 0.5) Beta Meta-analysis in (14). Standard deviation used in the probabilistic sensitivity analyses was estimated. (0 – 2) Beta Calculated from the reversion (0 – 4) Beta Calculation based on (15). Standard 4 Appendix- Cost-effectiveness of radiofrequency catheter ablation as first-line treatment >24 months Reversion rate RFA >24 months deviation estimated. Meta-analysis of (2-6) (0 – 2) Beta 0.178 (0.1 – 0.5) Beta 3319 18 601 (16) 0.269 (0.1 – 0.5) Beta 4716 12 796 (16) 0.367 (0.1 – 0.5) Beta 7810 21 298 (16) Intervention/ investigation cost MR 9968 (5000 – 15 000) Deterministic Percutaneous intervention 17542 (10 000 – 30 000) Deterministic Symptomatic AF Proportion symptomatic 55 % (30 – 80) Deterministic Unpublished MANTRA-PAF-data (15 000 – 45 000) (0 -700) Deterministic+ Range Deterministic Deterministic+ Range Deterministic (17) Range 10 000 – 40 000 tested in sensitivity analyses (18) (17) Range 0 – 1500 tested in sensitivity analyses (10) Standard deviation estimated. Normal (19) Risk of Death Stroke Risk of death, acute. CHADS= 0-1 Risk of death, acute. CHADS= 2 Risk of death, acute. CHADS= 3-4 0.8 % 0.1 Cost for the Department of Cardiology, Linköping University Hospital Cost for the Department of Cardiology, Linköping University Hospital AF Cost events Cost severe bleeding 26 339 Cost GI-bleeding Cost minor bleeding 31 377 350 Cost MI 184 115 10 000 Stroke cost Hospitalization stroke 84 999 1 088 (50 000 – 300 000) 5 Appendix- Cost-effectiveness of radiofrequency catheter ablation as first-line treatment (acute) Social service (Year 1) Health care (Year 1) Primary care (Year >1) Social service (Year >1) 50 746 36 760 22 400 40 856 81 Normal (19) (19) (19) (19) Procedure consumption and cost Mean SD Cost ECG before 1 231 ECG after 1 231 Physicians** minutes 279 Range Reference 50 000 – 150 000 Cost for the Department of Cardiology, Linköping University Hospital Cost for the Department of Cardiology, Linköping University Hospital Unpublished MANTRA-PAF-data/ Cost for the Department of Cardiology, Linköping University Hospital Unpublished MANTRA-PAF-data/ Cost for the Department of Cardiology, Linköping University Hospital Unpublished MANTRA-PAF-data/ Cost for the Department of Cardiology, Linköping University Hospital Unpublished MANTRA-PAF-data/ Cost for the Department of Cardiology, Linköping University Hospital Unpublished MANTRA-PAF-data/ Unit cost from Linkoping University hospital Cost for the Department of Cardiology, Linköping University Hospital Cost southeast health care region of Sweden Cost southeast health care region of Sweden 127.30 5588 Anesthetist (phy) minutes 5.65 9.68 134 Anesthetist (nur) minutes 148 108.92 1778 Other ass per minutes 446 202.02 4459 Hospital care 2.28 1.43 Ablation materials 1 43 314 Other costs Total cost 1 24050 90294 10 185 6 Appendix- Cost-effectiveness of radiofrequency catheter ablation as first-line treatment Monthly risk of events in AF-patients Warfarin Ischemic stroke Low risk CHADS: 0-1 Moderate risk CHADS: 2 High risk: CHADS: 3-6 0.053% 0.094% 0.158% Bleeding stroke Low risk CHADS: 0-1 Moderate risk CHADS: 2 High risk: CHADS: 3-6 0.07% 0.07% 0.07% Other events Severe bleeding GI-bleeding Minor bleeding Myocardial infarction 0.13% 0.09% 1.48% 0.04% 7 Appendix- Cost-effectiveness of radiofrequency catheter ablation as first-line treatment Life tables Swedish population 2011 Age 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 57 58 59 60 61 62 63 64 65 66 67 68 69 70 71 72 73 74 75 76 77 78 79 80 81 82 83 84 85 86 87 88 89 90 91 92 93 94 95 96 97 98 99 100 101 102 103 104 105 106 107 108 109 110 111 112 Monthly mortality 0,007% 0,008% 0,009% 0,011% 0,012% 0,012% 0,014% 0,013% 0,016% 0,020% 0,022% 0,026% 0,024% 0,031% 0,031% 0,033% 0,036% 0,043% 0,048% 0,048% 0,057% 0,059% 0,069% 0,075% 0,089% 0,092% 0,102% 0,106% 0,129% 0,139% 0,147% 0,162% 0,185% 0,197% 0,240% 0,257% 0,274% 0,328% 0,368% 0,403% 0,467% 0,564% 0,605% 0,689% 0,771% 0,877% 1,015% 1,148% 1,302% 1,450% 1,616% 8 1,850% 2,022% 2,204% 2,398% 2,605% 2,824% 3,056% 3,302% 3,563% 3,840% 4,134% 4,449% 4,784% 5,144% 5,531% 5,950% 6,403% 6,896% 7,434% 8,022% 8,667% 9,377% Appendix- Cost-effectiveness of radiofrequency catheter ablation as first-line treatment Baseline patients (≤50 year) Baseline N Age (mean) Age (median) Female (%) Systolic BP Diastolic BP Height Weight NYHA class 1 CCS class 1 Underlying disease Floppy mitral valve Coronary artery disease AP Prior MI Prior PCI Prior CABG CAG with > 50% stenosis Other structural disease Valvular heart disease History of valve intervention. Left ventricular. hypertrophy Congenital heart disease Hypertension Previous rate control Beta blocker Calcium antagonist Digoxin His-ablation Previous rhythm control Beta blocker RA isthmus block Other RA ablation Pacemaker with PES Previous SVT Atrial tachycardia Other SVT AVNRT WPW Focal atrial tachycardia Atrial fibrillation (R) Atrial flutter Ischemic stroke RFA AAD 33 43 42.85 45 21 132.63 79.50 179.81 90.88 1.00 1.00 0.30 0.00 0.03 0.00 0.03 0.03 0.00 0.00 0.12 0.00 0.00 0.03 0.00 0.15 0.55 0.42 0.12 0.09 0.00 0.64 0.64 0.03 0.00 0.00 0.03 0.03 0.00 0.00 0.00 0.00 0.03 0.03 0.00 42.14 43.5 12 130.27 79.98 181.58 85.53 0.98 1.00 0.19 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.02 0.00 0.00 0.02 0.00 0.19 0.42 0.35 0.07 0.07 0.00 0.51 0.51 0.02 0.00 0.00 0.05 0.02 0.00 0.02 0.02 0.00 0.00 0.05 0.00 9 p-value 0.63 0.262 0.523 0.82 0.341 0.09 0.385* 0.24 0.256 0.256 0.256 0.09 0.852 0.697 0.278 0.509 0.449 0.739 0.283 0.283 0.852 0.723 0.667 0.385 0.385 0.256 0.723 - Appendix- Cost-effectiveness of radiofrequency catheter ablation as first-line treatment Transient ischemic attack Systemic peripheral embolism Intracranial hemorrhage Sinus bradycardia/SSD Sinoatrial exit block Tachycardia-bradycardia AV-block Most advanced degree Pacemaker insertion ICD insertion Diabetes mellitus Chronic lung disease Thyroid disease 0.00 0.00 0.00 0.03 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.06 0.09 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.00 0.07 0.00 0.00 0.256 0.24 0.105 0.044 * Mann-Whitney U- Test, All other: independent sample t-test Baseline patients >50 year Baseline N Age (mean) Age (median) Female Systolic BP Diastolic BP Height Weight NYHA class 1 CCS class 1 Coronary artery disease AP Prior MI Prior PCI Prior CABG CAG with > 50% stenosis Other structural disease Valvular heart disease History of valve intervention. Left ventricular. hypertrophy Congenital heart disease Hypertension Previous rate control Beta blocker Calcium antagonist Digoxin His-ablation Previous rhythm control RFA AAD p-value 108 60.29 60 0.34 139.34 82.16 177.66 84.58 0.86 0.96 103 59.79 59 0.36 136.75 82.03 175.96 83.96 0.83 0.96 0.80 0.33 0.93 0.19 0.76 0.41* 0.94* 0.05 0.01 0.01 0.00 0.03 0.01 0.11 0.06 0.01 0.07 0.00 0.34 0.74 0.61 0.12 0.16 0.00 0.07 0.02 0.00 0.02 0.01 0.00 0.01 0.11 0.15 0.01 0.12 0.02 0.44 0.65 0.57 0.07 0.12 0.00 0.07 0.18 0.07 0.12 0.07 0.12 0.10 0.31 0.30 0.10 0.29 0.10 0.49 0.46 0.49 0.29 0.35 0.26 10 0.47 Appendix- Cost-effectiveness of radiofrequency catheter ablation as first-line treatment Beta blocker RA isthmus block Other RA ablation Pacemaker with PES Previous cardioversion Previous SVT Atrial tachycardia Other SVT AVNRT WPW Focal atrial tachycardia Atrial fibrillation (R) Atrial flutter Ischemic stroke Transient ischemic attack Systemic peripheral embolism Intracranial hemorrhage Sinus bradycardia/SSD Sinoatrial exit block Tachycardia-bradycardia AV-block Most advanced degree Pacemaker insertion ICD insertion Diabetes mellitus Chronic lung disease Thyroid disease 0.45 0.45 0.03 0.00 0.00 0.06 0.02 0.00 0.01 0.04 0.00 0.01 0.02 0.00 0.04 0.02 0.04 0.02 0.01 0.09 0.06 0.05 0.03 0.06 0.01 0.06 0.06 0.44 0.44 0.00 0.00 0.00 0.02 0.01 0.00 0 0.01 0.00 0 0 0.00 0.01 0.04 0.01 0.00 0.00 0.08 0.06 0.03 0.02 0.05 0.03 0.09 0.06 0.50 0.50 0.12 0.20 0.12 0.07 0.15 0.07 0.10 0.15 0.17 0.15 0.10 0.07 0.28 0.23 0.19 0.15 0.23 0.14 0.31 0.23 * Mann-Whitney U- Test, All other: independent sample t-test 6. Structure procedural model Every RFA-intervention could be repeated up to three times and complication could occur after every procedure. Complications include risk for local hematomas, pseudoaneurysm, vasovagal reaction, infection, chest pain or discomfort, arrhythmias, pericardial effusion, transient ischemic attack, cerebrovascular accident, cardiac tamponade, pericarditis and death. 7. Time horizon 11 Appendix- Cost-effectiveness of radiofrequency catheter ablation as first-line treatment As shown below, the result is dependent of the time horizon in the model. The effect of an additional year on the ICER declined after approximately 20 years. 8. Sensitivity analyses of the overall population Parameter Value Cost RFA-procedure Cost RFA-procedure RFA proc. mortality QALY weight (both groups) QALY decrement isch.stroke QALY decrement isch.stroke RR NSR RR NSR €/QALY €5 000 €15 000 0.5% 0.8 0.1 0.2 0.75 0.5 9. PROBABILISTIC SENITIVITY ANALYSES 12 20 146 76 716 66 924 59 559 50 070 51 080 53 457 47 903 Appendix- Cost-effectiveness of radiofrequency catheter ablation as first-line treatment REFERENCES: 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. 17. Pappone C, Rosanio S, Augello G et al. Mortality, morbidity, and quality of life after circumferential pulmonary vein ablation for atrial fibrillation: outcomes from a controlled nonrandomized long-term study. Journal of the American College of Cardiology 2003;42:185-97. Ouyang F, Tilz R, Chun J et al. Long-term results of catheter ablation in paroxysmal atrial fibrillation: lessons from a 5-year follow-up. Circulation 2010;122:2368-77. Shah AN, Mittal S, Sichrovsky TC et al. Long-term outcome following successful pulmonary vein isolation: pattern and prediction of very late recurrence. Journal of cardiovascular electrophysiology 2008;19:661-7. Tzou WS, Marchlinski FE, Zado ES et al. Long-term outcome after successful catheter ablation of atrial fibrillation. Circulation Arrhythmia and electrophysiology 2010;3:237-42. Bertaglia E, Tondo C, De Simone A et al. Does catheter ablation cure atrial fibrillation? Singleprocedure outcome of drug-refractory atrial fibrillation ablation: a 6-year multicentre experience. Europace : European pacing, arrhythmias, and cardiac electrophysiology : journal of the working groups on cardiac pacing, arrhythmias, and cardiac cellular electrophysiology of the European Society of Cardiology 2010;12:181-7. Sawhney N, Anousheh R, Chen WC, Narayan S, Feld GK. Five-year outcomes after segmental pulmonary vein isolation for paroxysmal atrial fibrillation. The American journal of cardiology 2009;104:366-72. Cosedis Nielsen J, Johannessen A, Raatikainen P et al. Radiofrequency ablation as initial therapy in paroxysmal atrial fibrillation. The New England journal of medicine 2012;367:1587-95. Davidson T, Husberg M, Janzon M, Levin L. The Cost of Thromboembolic Events and their Prevention among Patients with Atrial Fibrillation. Journal of Atrial Fibrillation 2011;2:1-11. Lee HY, Hwang JS, Jeng JS, Wang JD. Quality-adjusted life expectancy (QALE) and loss of QALE for patients with ischemic stroke and intracerebral hemorrhage: a 13-year follow-up. Stroke; a journal of cerebral circulation 2010;41:739-44. Janzon M. Treatment strategies in unstable coronary artery disease economic and quality of life evaluations. Linköping Medical Dissertation 2003;811. Burstrom K, Johannesson M, Diderichsen F. A comparison of individual and social time tradeoff values for health states in the general population. Health policy 2006;76:359-70. Cappato R, Calkins H, Chen SA et al. Worldwide survey on the methods, efficacy, and safety of catheter ablation for human atrial fibrillation. Circulation 2005;111:1100-5. Sherman DG, Kim SG, Boop BS et al. Occurrence and characteristics of stroke events in the Atrial Fibrillation Follow-up Investigation of Sinus Rhythm Management (AFFIRM) study. Archives of internal medicine 2005;165:1185-91. Reynolds MR, Zimetbaum P, Josephson ME, Ellis E, Danilov T, Cohen DJ. Cost-effectiveness of radiofrequency catheter ablation compared with antiarrhythmic drug therapy for paroxysmal atrial fibrillation. Circulation Arrhythmia and electrophysiology 2009;2:362-9. Pappone C, Vicedomini G, Augello G et al. Radiofrequency catheter ablation and antiarrhythmic drug therapy: a prospective, randomized, 4-year follow-up trial: the APAF study. Circulation Arrhythmia and electrophysiology 2011;4:808-14. Henriksson KM, Farahmand B, Johansson S, Asberg S, Terent A, Edvardsson N. Survival after stroke--the impact of CHADS2 score and atrial fibrillation. International journal of cardiology 2010;141:18-23. O'Brien CL, Gage BF. Costs and effectiveness of ximelagatran for stroke prophylaxis in chronic atrial fibrillation. JAMA : the journal of the American Medical Association 2005;293:699-706. 13 Appendix- Cost-effectiveness of radiofrequency catheter ablation as first-line treatment 18. 19. Cameron C, SV VANZ, Skedgel C, Flowerdew G, Moayyedi P, Sketris I. Cost-utility analysis of proton pump inhibitors and other gastro-protective agents for prevention of gastrointestinal complications in elderly patients taking nonselective nonsteroidal anti-inflammatory agents. Alimentary pharmacology & therapeutics 2010;31:1354-64. Ghatnekar O, Persson U, Glader EL, Terent A. Cost of stroke in Sweden: an incidence estimate. International journal of technology assessment in health care 2004;20:375-80. 14