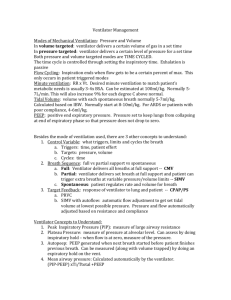
Modes of Ventilatory Support - Joshua Smith, RTT (Registered
advertisement

Modes of Ventilatory Support Lecture Hours: Lab Hours: Online Study Hours: Credit Hours: Reading assigned: Fundamentals of Respiratory Care, chapters 42, 44 Suggested reading: Course Description The student will learn the various modes of ventilation available when placing patients on mechanical ventilation. In addition, the student will learn the criteria used to determine the proper mode for a given patient. Educational Objectives At the end of the course, the student will be able to: 1. Define the terms sensitivity, trigger, cycle, and limit. 2. List the common modes of ventilatory support and describe the function and mode of action or initiation of each. Lesson Plan I. II. Terminology. A. Sensitivity – the measure of the amount of effort required by a patient to initiate the inspiratory phase of a ventilator. B. Trigger – the change in pressure or flow that the patient must produce to initiate a breath. C. Cycle – the means by which a ventilator ends the inspiratory phase; may be either pressure, volume, time, or flow. D. Limit – the set variable that cannot be exceeded during mechanical ventilation, but does not end the inspiratory phase. E. Spontaneous breath – patient initiates the start time and the tidal volume; the entire breath is controlled by the patient alone. F. Mandatory breath – ventilator sets the start time and/or the tidal volume; the machine both triggers and cycles the breath. Traditional ventilation types. A. Volume controlled ventilation. 1. Cycling mechanism – volume. 2. Controls available. a. Respiratory rate. b. PEEP. c. FIO2. d. Inspiratory time. e. Tidal volume. 3. Advantages. a. Known VT delivered resulting in more stable 𝑉̇E. III. b. More stable blood gases, especially with unstable lung mechanics. 4. Disadvantage – risk of volutrauma. 5. Primary uses. a. Majority of patients do well in this mode. b. Patients in OR. B. Pressure controlled ventilation. 1. Cycling mechanism – pressure. 2. Controls available. a. Rate. b. PEEP. c. FIO2. d. Inspiratory time. e. Peak inspiratory pressure. 3. Advantages. a. Cycles off when maximum set pressure is reached. b. Decreases risk of barotrauma. c. Allows better synchronization with patient due to variable flow. 4. Disadvantages. a. No guarantee of VT. b. May allow excessive volumes should lung compliance change. 5. Primary uses. a. Patients at risk from increased pressures. b. Patients with ARDS. c. Newborns. Theoretical determinants of modes of ventilation. A. Objective of mechanical ventilation – delivery of appropriate minute volume required to meet the patient’s respiratory needs while not damaging the pulmonary system, compromising circulation, or increasing the patient’s discomfort. B. Mode of ventilation is the manner in which the ventilator achieves the objective through a combination of parameters. 1. Breathing pattern. a. Breath control variable. i. Volume control. a) Tidal volume and inspiratory flow are preset. b) Airway pressure dependent upon volume, flow, elastance, and resistance. ii. Pressure control. a) Airway pressure waveform is preset (PIP and PEEP). b) Tidal volume and flow dependent upon PIP, PEEP, elastance, and resistance. iii. Dual control – ventilator automatically switches between pressure and volume control in order to guarantee minute ventilation while maximizing patient synchrony. a) Volume-assured, pressure support (VAPS) – breath begins in pressure control and switches to volume control before the breath ends. b) Pmax (e.g., Drager) – begin inspiration in volume control and switch to pressure control. b. Breath sequence. i. ii. iii. Continuous mandatory ventilation (CMV) – all breaths are mandatory. Continuous spontaneous ventilation (CSV) – all breaths are spontaneous. Intermittent mandatory ventilation (IMV) – breaths can be either mandatory or spontaneous. 2. Control type. a. Open loop control. i. Flow was a function of relationship between impedances between respiratory system and exhalation manifold. ii. Delivered pressures and volumes affected by any change in lung mechanics, patient effort, or leaks. b. Closed loop control. i. Volumes, pressures, and flows made to match or respond to specific input values, unaffected by changes in patient condition or leaks in system. ii. Closed loop control systems. a) Setpoint control. 1) Used by all ventilators. 2) Output set to match a preset input such as volume or pressure. 3) Control maintained within each breath. b) Auto setpoint control. 1) Advanced version of setpoint control. 2) Ventilator “decides” whether each breath will be volume or pressure controlled. c) Servo control. 1) Ventilator tracks and follows patient’s flow pattern. 2) Allows ventilator to support the abnormal ventilatory work load while the patient’s own muscles handle the normal work load. 3) Control maintained within each breath. d) Adaptive control. 1) Automatic adjustment of one setpoint to maintain a second, operator-selected setpoint. 2) Feedback loop operates between breaths. 3) Feedback of volume allows ventilator to adapt to changes in patient lung mechanics. e) Optimal control. 1) Similar to adaptive control, but allows ventilator to set both volume and pressure setpoints. 2) Operator sets target minute ventilation; ventilator then makes all subsequent adjustments to volume and pressure. 3) Operator input still required for other parameters such as PEEP and FIO2. f) Knowledge-based control. 1) Ventilator obtains information regarding patient condition such as respiratory rate, saturation, and rate of change of values. 2) Results are integrated with a pre-defined range of values representing the patient’s status. 3) Expert rules from a lookup table are applied to the results and used to adjust the ventilator. 4) In theory, no operator is necessary. IV. g) Artificial neural net control. 1) Theoretical system at present. 2) Uses an artificial system or neural net. 3) Is able to weigh the inputs received. 4) When a threshold is reached, the net responds with a change to the ventilator. 5) Over time, the weights given to inputs will be modified allowing the system to “learn”. 3. Control strategy. a. Phase variables. i. Parameters which vary within the phase of ventilation, e.g., trigger, limit, and cycle variables. ii. May be different dependent upon whether breaths are mandatory or spontaneous. b. Operational logic. i. The operational method by which the spontaneous and mandatory breaths are delivered. ii. Mandatory and spontaneous breaths may have different controls and limits. iii. May be either mandatory or spontaneous controls or both. Currently employed modes of ventilation. A. Positive end-expiratory pressure (PEEP). 1. Definition – increase in the baseline airway pressure to a value greater than atmospheric. 2. Purpose. a. Used in conjunction with other ventilator modes. b. Improve oxygenation status. c. Increase the functional residual capacity (FRC) to reverse/prevent functional loss of alveoli. 3. Indications. a. Presence of intrapulmonary shunt with refractory hypoxemia. b. Decrease in FRC and lung compliance. 4. Physiology of action. a. Positive pressure increases alveolar distending pressure. b. The increase in distending pressure recruits alveoli, increasing the FRC. c. Ventilation increases. d. Improvement in ventilation/perfusion (V/Q) ratio. e. Improvement in oxygenation. f. Decrease in work of breathing. 5. Complications. a. Decrease in venous return secondary to increase in mean airway pressure. b. Barotrauma – increase in pressure leading to excessive volume causing alveolar rupture. c. Increase in intracranial pressure secondary to impedance of venous return. d. Changes in kidney function secondary to decreased perfusion; may lead to renal failure. B. Continuous positive airway pressure (CPAP). 1. Definition – increase in baseline airway pressure to a value greater than atmospheric in a spontaneously breathing patient. 2. Purpose, indications, physiology of action, and complications as for PEEP. C. Controlled mandatory ventilation (CMV). 1. Definition – delivery of a preset tidal volume at a time-triggered respiratory rate. 2. Purpose – to control the patient’s minute volume. 3. Indications. a. Patient “fighting” or “bucking” the ventilator. b. Tetanus. c. Seizure disorders. d. Complete rest for the patient (usually no more than 24 hours). e. Patients with paradoxical chest movement (crushed chest). 4. Physiology of action. a. Patient locked out of triggering breaths on the ventilator. b. Patient must be properly medicated with combination of sedatives, respiratory depressants, and neuromuscular blockers. c. Ventilator assumes all responsibility for ventilation. 5. Complications. a. Potential for apnea and hypoxemia secondary to accidental disconnection. b. Hypoventilation or hyperventilation through inappropriate settings. D. Assist/control mode (AC). 1. Definition – delivery of a minimum number of breaths by the ventilator which may be increased through patient effort triggering additional breaths. 2. Purpose – guarantee a minimum minute volume to the patient while permitting the patient to initiate additional breaths. 3. Indications. a. Patient with stable respiratory drive capable of triggering the ventilator. b. Frequently used when patient is first placed on ventilatory support. 4. Physiology of action. a. Patient is stable enough to continuously provide triggering of breaths from the ventilator. b. Ventilator is typically set at two to four breaths per minute less than patient’s spontaneous rate. c. Ventilator serves as “safety net” for patient in the event of episodes of apnea. d. Work of breathing for the patient is minimized. e. Allows patient to normalize the PaCO2 by controlling respiratory rate. 5. Complication – alveolar hyperventilation, especially if patient’s respiratory center is injured or diseased. E. Intermittent mandatory ventilation (SIMV or IMV). 1. Definition – delivery of set number of control (mandatory) breaths, but allows the patient to breathe spontaneously at any tidal volume or rate that the patient is capable of between those breaths. 2. Purpose – provide a spontaneous breathing workload that gradually increases the patient’s muscle strength and endurance. 3. Indications. a. Frequently used routinely after the patient has been on either CMV or AC for 24 hours. b. Used to wean amount of ventilatory support. 4. Physiology of action. a. Synchronization window – typically 0.5 period prior to control breath during which patient can trigger assisted breath. b. All other non-controlled breaths initiated by the patient with the volume and frequency determined by the patient. c. Spontaneous breaths have beneficial effects for patient. i. Allow exercise of respiratory muscles, preventing loss of strength. ii. Decrease V/Q mismatch which usually increases during control breaths. iii. Decrease in mean airway pressure. 5. Complication – therapist may try to wean to rapidly, creating a high work of breathing, muscle fatigue, and weaning failure. F. Mandatory minute ventilation (MMV). 1. Definition – provision of a pre-determined minute ventilation when the patient’s spontaneous breathing effort becomes inadequate. 2. Purpose – prevention of hypoventilation for a patient receiving IMV secondary to a decrease in the patient’s spontaneous breaths. 3. Indications – used as a feature of some manufacturer’s ventilators in conjunction with IMV. 4. Physiology of action. a. During periods of apnea or decreased spontaneous effort, the ventilator automatically ensures that the patient will have minimum minute ventilation. b. If, during spontaneous breaths, the patient’s frequency increases, alveolar hypoventilation may occur secondary to increase in deadspace ventilation. c. Example. i. Patient spontaneous frequency – 14 breaths/min.; spontaneous VT – 300 mL; spontaneous 𝑉̇ - 4.2 L; spontaneous 𝑉̇A – 2.1 L. ii. Patient spontaneous frequency – 24 breaths/min.; spontaneous VT – 175 mL; spontaneous 𝑉̇ - 4.2 L; spontaneous 𝑉̇A – 0.6 L. iii. Change in spontaneous volume and frequency result in 86% decrease in 𝑉̇A. 5. Complication – see example above. G. Pressure support ventilation (PSV). 1. Definition – application of a preset pressure plateau to a patient’s airway for the duration of a spontaneous breath. 2. Purpose – lower the work of breathing during spontaneous ventilation. 3. Indications. a. Typically used to in IMV mode to facilitate weaning. b. Need to decrease the work of breathing during spontaneous ventilation. c. Overcome airway resistance of endotracheal tube. 4. Physiology of action. a. Demand valve of ventilator opens when patient initiates breath, increasing airway pressure to preset limit and maintaining it for the duration of the patient’s spontaneous effort. b. Increases spontaneous tidal volume. c. Decreases spontaneous frequency. d. Decreases work of breathing. 5. Complication – when used without a back up ventilator rate, may allow patient to hypoventilate should spontaneous pattern change. H. Adaptive support ventilation (ASV). I. J. 1. Definition – mode of ventilation that changes the number of mandatory breaths and pressure support level according to the patient’s breathing pattern. 2. Available on limited number of ventilators currently. 3. Initiation of mode. a. Therapist inputs patient body weight and percent of minute volume. b. Machine uses predetermined minute volume setting of 100 mL/min./kg for adults. c. Ventilator determines system compliance, airway resistance, and intrinsic PEEP using test breaths. d. Ventilator then selects frequency, inspiratory time, I:E ratio, and high pressure limit for mandatory and spontaneous breaths. e. As patient begins to trigger breaths, the ventilator decreases the number of mandatory breaths and the pressure support level until a calculated tidal volume is able to provide adequate alveolar ventilation (VT = VA + 2.2 mL/kg VD). Proportional assist ventilation (PAV). 1. Definition – mode of ventilation that changes the pressure support level according to the volume, elasticity, airflow resistance, and flow demand. 2. Purpose – provide variable pressure support in proportion to the patient’s pulmonary characteristics. 3. Physiology of action. a. Achieved through use of a positive feedback control allowing changes with the patient’s breathing efforts, providing greater patient/ventilator synchrony. b. Improves ventilation. c. Reduces neuromuscular drive and work of breathing. d. When used with CPAP, reduction of muscle work approaches values of normal subjects. 4. Complications. a. Occur when elastance or airway resistance improve suddenly. b. Overdistension of alveoli. c. Increase in air trapping. d. Barotrauma. Volume-assured pressure support (VAPS). 1. Definition – mode of ventilation that assures a stable tidal volume by incorporating inspiratory pressure support ventilation with conventional volume assisted cycles. 2. Purpose – provide stable tidal volume to patients with irregular breathing patterns. 3. Initiation of mode. a. Minimum tidal volume and pressure support level set by therapist. b. Once breath is triggered by either the ventilator or the patient, the machine will reach the pressure support level as quickly as possible. c. The volume delivered at that point is compared to the preset tidal volume. d. If delivered VT equals preset VT, the breath is a pressure support breath; this allows volume to be greater than preset volume since breaths are dependent upon patient effort. e. If delivered VT is less than preset VT, then the ventilator switches to a volume limited breath until the preset volume is delivered. f. Inspiratory time may be prolonged automatically when in volume limited mode. 4. Complications. a. Result from prolonged inspiratory time. K. L. M. N. b. Air trapping. c. Cardiovascular effects may result. Pressure-regulated volume control (PRVC). 1. Definition – mode of ventilation designed to provide volume support with the lowest pressure possible by changing the flow and inspiratory time. 2. Purpose – achieve volume support while keeping peak inspiratory pressure at lowest possible level in order to minimize side effects. 3. Initiation of mode. a. Maximum peak inspiratory pressure is determined. b. Ventilator senses changes in airway resistance and lung compliance. c. Ventilator then alters flow and inspiratory time to maintain the PIP at 5 cmH2O below the preset pressure limit. Volume ventilation plus (VV+). 1. Definition – mode that combines volume control plus and volume support. 2. Volume control plus (VC+) is used to deliver mandatory breaths during AC and IMV modes, but with a higher level of patient synchrony. a. Target tidal volume and inspiratory time are set. b. Ventilator delivers a single breath to determine relative compliance. c. Pressure is adjusted for subsequent breaths to compensate for tidal volume differences. d. Flow is adjusted automatically to minimize inadequate flow. 3. Volume support (VS) is used to provide a controlled tidal volume and increased patient comfort; used frequently in weaning from anesthesia. a. Only target tidal volume is set. b. Ventilator rate and minute ventilation determined by triggering effort of patient. c. Ventilator delivers single spontaneous pressure support breath and uses variable pressure support to achieve tidal volume. d. As patient resumes a higher spontaneous tidal volume, ventilator decreases pressure support. e. If spontaneous tidal volume decreases, ventilator increases pressure support to maintain tidal volume. Pressure control ventilation (PCV). 1. Definition – mode in which once inspiration begins, a pressure plateau is determined and maintained for a preset inspiratory time. 2. Indication. a. Patients with severe ARDS who require extremely high peak inspiratory pressure during mechanical ventilation in the volume-cycle mode. b. Generally able to maintain oxygenation and ventilation while reducing peak inspiratory pressure. c. Significantly reduces risk of barotrauma. 3. Initiation of mode. a. Frequency is preset; best if patient sedated. b. After initiation of breath by ventilator, pressure plateau is established and maintained by servo-controlled inspiratory flow, similar to pressure support. c. Pressure is maintained only for a preset inspiratory time, not for the duration of the patient’s spontaneous inspiratory effort. Airway pressure release ventilation (APRV). 1. Definition – mode of ventilation in which spontaneous breaths are at an elevated baseline, returning to zero periodically to facilitate expiration. 2. Indication – alternative to conventional volume-cycled ventilation for patients with markedly decreased compliance. 3. Mode of action. a. Patient is breathing spontaneously. b. During expiratory phase, PEEP is dropped or released to a lower level, simulating effective exhalation. c. Mandatory inspiration begins with the time-triggered closing of the release valve. d. Pressure increases rapidly to baseline CPAP level and maintained for duration of inspiration. e. Mandatory inspiration ends with time-triggered opening of release valve, allowing circuit pressure to decrease as patient exhales. f. Tidal volume will vary with changes in lung compliance and resistance, necessitating close monitoring. Mode Control Assist-control (AC) Intermittent mandatory ventilation (SIMV) Mandatory minute ventilation (MMV) Pressure support ventilation (PSV) Proportional assist ventilation (PAV) Pressure-regulated volume control (PRVC) Pressure control ventilation (PCV) Airway pressure release ventilation (APRV) Type of breath Trigger Mechanism Cycle Mechanism Each breath delivered is Time triggered Delivery of preset tidal preset tidal volume volume Each breath delivered is Patient triggered Primary – delivery of preset tidal volume (assist) preset tidal volume Time triggered Secondary – reach high (mechanical) pressure limit Vent delivers preset Mandatory breaths Mandatory breaths are tidal volume at a either time triggered volume cycled preset rate or patient triggered Patient controls Patient breaths Spontaneous breaths spontaneous rate spontaneously are patient triggered and volume between mechanical breaths Ventilator increases Mandatory rate Mandatory breaths are mandatory frequency increase triggered by volume cycled decrease in actual Patient controls minute ventilation spontaneous rate below preset level and volume Breaths are considered Breaths are patient Breaths are flow cycled spontaneous triggered by minimum spontaneous flow controlled by patient Used during assisted Pressure or flow Cycles when patient’s breaths only triggered volume or demand is met Depends upon Time triggered or Volume cycled ventilator: CMV in patient triggered some, IMV in others Only mandatory breaths Time triggered by Mandatory breaths are available preset rate time cycled by preset May be patient inspiratory time triggered for additional breaths Mandatory breaths with Mandatory breaths are Mandatory breaths are patient allowed to time triggered time cycled by preset breath spontaneously Patient controls inspiratory time between mandatory spontaneous breaths breaths