IV Therapy - Moodle at Southeastern
advertisement

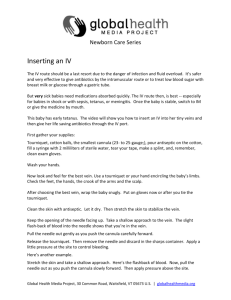
A guide to starting IV Therapy Barbara Gibbs RN, BSN Southeastern Louisiana University NURS 634 May 3, 2009 For clinical lab this week, we will be initiating IV therapy. Please read the selection in the Nurses’Guide to Clinical Procedures on p. 181-194. Also read Manual of IV Therapeutics p. 281-344. You may also want to go to the lab and spend some time with the simulator prior to class. Please call the lab coordinator to arrange that. We asked that you don’t use your poor family members and friends for practice! In this lesson, I will use the Adult Education Theory. According to our textbook on p. 207, most adults like being involved in the learning process. They take on the responsibility of learning (Billings & Halstead, 2009). I chose IV therapy because I am constantly teaching other nurses at work how to start IVs. Most are still intimidated by them, but style and technique comes with practice. Many student nurses enjoy getting to do “hands-on” skills. Pre-Lab Survey In this lesson, I will use a Course-Related Self-Confidence Survey (Angelo & Cross, 1993, CAT 32). My teaching goal is to help the nursing student gain knowledge, self-confidence, and self-esteem (Angelo & Cross, TGI Goal 45) 1. Rate your self-confidence – how you feel about starting IVs – by circling the appropriate number below: 1. Extremely Low 2. Low 3. Average for me 4. High 5. Extremely High 2. Briefly explain why you gave yourself the the rating above. 3. Overall, for the semester, how would you rate your selfconfidence? 1. Extremely low 2. Low 3. Average for me 4. High 5. Extremely High 4. An instructor could raise (or has raised) my self-confidence by: Answer the following questions: Please post your answers on discussion board linked with this assignment 1. By posting their answers, the student will also utilize the internet along with the textbook readings. I have used two different CATs with the lesson to help initiate the learning process. It is up to the adult learner to complete assignments prior to class. What is the very first step in the initiation of IV therapy? a. Gather all the necessary equipment b. Wash hands c. Explain the procedure to the patient d. Check the physician’s order 2. Why is the antecubital vein not the best vein for IV therapy even though it is usually easy to cannulate? 3. Do you know the policy for accidental needle sticks? 4. Where would this policy be found or how can you find it? History of Infusion Therapeutics (Phillips, 2001, p. 1,2) 1616 Sir William Harvey discovered the circulation of blood 1660 Sir Christopher Wren produced the first hypodermic needle 1662 Johann Majors used the needle to inject compounds into humans (resulted in death) 1667 Jean Baptiste Denis infused from animal to human (resulted in death) 1687 Animal to human transfusions prohibited in Europe – 150 years go by 1832 Dr. Thomas Latta infuses saline to treat diarrhea from cholera (banned in the US) 1867 Lister’s work on sterility and Louis Pasteur’s Germ Theory accepted 1889 William Halsted and Goodyear Rubber Co. introduce rubber gloves 1925 Dextrose used, but only in the critically ill Massachusetts General Hospital has the first designated IV nurses 1950 Rochester needle introduced 1957 McGaw Lab introduced small vein sets with foldable wings as grips 1958 Intracath, a plastic catheter within the lumen of a needle in sterile packaging 1960s Momentum for change with a variety of solutions Indications for IV Therapy • Provides venous route for administration of fluids, medications, blood, or nutrients • Urgency in which medication is needed • Oral route is not available • Patient must have drugs that would be destroyed by digestion (Smith-Temple & Johnson, 2002, p.181) Vascular Access Devices VADs • Peripheral IV access (which we will practice) • Midline catheters • Central venous access device CVAD *non-tunneled *tunneled *implantable ports • Peripherally inserted central catheter PICC (Scales, 2008, p.S4) Sensory Receptors of the Venous System Mechanoreceptors process skin tactile sensations and deep tissue sensation (palpation of veins) Thermoreceptors process temperature and pain (application of heat or cold) To decrease pain, keep the skin taut by applying traction to it. Move quickly past the pain receptors. Four of the five types of sensory receptors affect parenteral therapy. These receptors transmit along afferent fibers. Nociceptors process pain (puncture or insertion of the cannula) Chemoreceptors process osmotic changes in blood and decreased arterial pressure (decreased circulating blood volume) (Phillips, p.286-287) Steps to Success • Check the physician’s orders • Educate the patient • Gather and prepare the necessary supplies • Meticulous handwashing • Site selection • Needle selection • Gloving • Site preparation • Vein entry • Catheter stabilization • Dressing application • Equipment disposal • Documentation (Phillips, p.293) Check the physician’s orders A doctor’s order is needed to initiate IV therapy. The orders should be dated and timed. If it is a verbal order, then it must be signed within the specified time period. Remember to look for the name of the fluid, the route of administration, the dosage, volume, and rate. Check the patient’s allergies. Educate the Patient • Explain the purpose and procedure to the patient • Listen to his suggestions or fears and attempt to decrease any anxiety • Provide comfort and privacy for the patient Why I need IV Therapy! Gather and prepare the necessary supplies Some facilities have IV start kits, others, such as ours, have individual supplies. You will need: • a tourniquet (most are now Latex free, but check your patient’s chart for allergies) •Alcohol wipes or Chlorhexidine wipes •Jelcos (I usually take a 20 and 22 gauge) •2 x 2 gauge •Tape •Occlusive dressing •IV pigtail or extension •Saline flush Handwashing Handwashing is the first line of defense against cross contamination. Hands should be washed for 20 seconds with an antibacterial soap, rinsed, and dried with a disposable paper towel. Turn the faucet off with the paper towel and dispose. (CDC, 2007) Site Selection • Veins of the hands and arms are the most commonly used. • Carefully choose the site by considering ease of insertion and access, size or type of catheter, comfort and safety for the patient, and most effective site for the patient’s situation (Phillips, 2001, p. 290) Image from http://www.nda.ox.ac.uk/wfsa/html/ulz/u1213t03 .gif Retrieved 4/16/09. Site Selection & Needle Selection Factors to consider: • Type of solution: Hypertonic solutions such as antibiotics (Vancomycin) and potassium chloride are irritating. Choose a large vein and start at the lowest, best vein. • Condition of vein: Palpate the vein. It should feel elastic like a rubber band. Older patients or hypovolemic patients’ veins collapse more easily. You should stay away from the dorsal metacarpal veins and search for a larger vein. Avoid sites that are bruised, red, swollen, near previously infected areas or near a previously discontinued site. DO NOT start an IV on an extremity with a dialysis access or on a patient’s side of an old mastectomy. • Duration of therapy: IVs are good for 72 hours in most facilities. Alternate arms with each subsequent venipuncture and go distally proximal to the previous IV. Avoid joint flexion as patient’s usually bend arms during sleep or movement. • Cannula size: The gauge should be as small as possible unless the patient will be receiving blood. An 18-20 gauge is preferred to prevent hemolysis of the cells. • Patient age: For the purpose of this lesson, we are cannulating adult patients 18 and older. Remember that veins in the elder are fragile. Fragile veins sometimes work better if no tourniquet is used. (Phillips, p. 295-297) Gloving and Site Preparation Prior to procedure, and after handwashing, don clean gloves. 1. Gravity: Place extremity lower than heart level. 2. Fist Clenching: Patient may open and close fist. 3. Tapping: Tapping the vein causes it to release histamines beneath the skin and to dilate. 4. Warm compresses: Applying warm compresses also will also cause the vein to dilate. 5. Blood pressure cuff: This can also cause dilation by pumping the cuff up to about 30mmHg. (Phillips, p. 298) Cleanse the area with 70% alcohol or Chlorhexidine to reduce the potential for infection. Vein Entry • With the nondominant hand, pull the skin taut for stabilization. • Using dominant hand, insert the needle bevel up at about 15-30°. • Maintain parallel alignment and advance through the subcutaneous tissue. You should start to see a flash of blood in the chamber. • Release the tourniquet with the nondominant hand and “allow the vein to get used to the idea”. Slowly advance the cannula while retracting the needle. You will hear a click when it is locked in place. (Phillips, p. 303) Forward the catheter while withdrawing the needle until you hear a click. You should see blood in the flash chamber. Remove the catheter at the hub and attach the IV pigtail or extension. You can keep this bloodless by applying pressure at the distal end of the catheter. You may also place a 2x2 gauze at the connection to prevent a mess. Flush the catheter with normal saline. Check for any swelling to make sure the vein has not infiltrated and that the site is good. Stabilize the catheter using the Chevron Method Dressing Application • Catheters must be stabilized and an occlusive dressing applied in a manner that does not interfere with assessment and monitoring of the site. (Phillips, p.305) • After placing an occlusive dressing, usually a tegaderm, label the site with your initials, type of catheter, and the date. • We gratefully appreciate our victim here, who is also my father, Mr. Grant. At the time of this photo, I did not have a tegaderm. So, in this case, it is a do as I say, not as I do. Equipment Disposal • Needles, syringes, and any bloody items should go in a biohazard container to prevent needlestick injuries and the spread of bloodborne pathogens. • Dispose all other paper and plastic supplies in the trash bin. • Check the patient’s bed and linens for lose supplies. Documentation • We all know the drill, “Not documented, Not done” • Example documentation might be: 20 gauge heplock started x 1 attempt to R FA. Flushes well with + blood return. Dressing applied to site. No signs of infiltration. L FA heplock d/c’d with catheter intact, pressure drsg applied. Pt tolerated well…Bgibbs RN. Grading and Competency Criteria Clinical Skill 1. Checks the physician’s orders 2. Educates the patient 3. Gathers the necessary supplies 4. Performs proper handwashing 5. Site Selection, can name basic veins and anatomy 6. Needle Selection, can give rationale for size 7. Gloving, can verbalize rationale for precautions 8. Performs Site Preparation 9. Attempts entry of vein using proper technique 10. Applies good catheter stabilization 11. Applies dressing properly and labels 12. Disposes all equipment per protocol 13. Documents well 14. Can verbalize needlestick policy for facility The student must be able to perform at 85% or better. The student does not have to cannulate the vein, but must make an attempt. Shows Skill Shows Need Post Clinical Skills Lab 1. 2. 3. Identify techniques that you have observed in clinical that may help you in the future. Why is it necessary to check for patency during the shift? Label the veins on p. 329, Copy them and turn it in next week. References Angelo, T. & Cross, P. (1993) Classroom Assessment Techniques: A Handbook for College Teachers. San Francisco: Jossey Bass, 87-88 Billings, D. & Halstead, J. (2009) Teaching in Nursing: A Guide for Faculty. 3rd ed. St. Louis: Saunders Elsevier, 207 CDC recommendations and Reports (2007) Retrieved April 15, 2009 from http://www.cdc.gov/mmwr/preview/mmwrhtml/rr5605a4.htm Phillips, L. (2001) Manual of I.V. Therapeutics. 3rd ed. Philadelphia: F.A. Davis, 281-344 Scales, K. (2008) Intravenous therapy: A guide to good practice. British Journal of Nursing. 17(19), S4-S12. Retrieved from CINAHL full text database. Smith-Temple, J. & Johnson, J. (2002) Nurses’ Guide to Clinical Procedures. 4th ed. Philadelphia: Lippincott, 181-194 Images obtained from Microsoft Clip Art and from www.images.google.com A special thank you to Mr. Grant who served as our model vein for the photography used in this powerpoint