DEFINITION
advertisement

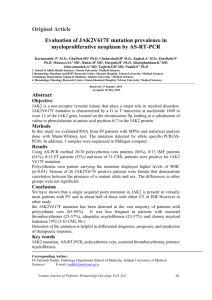
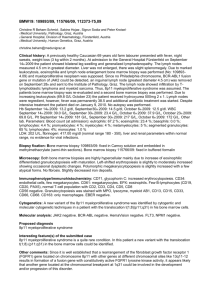
Myeloproliferative disorders • Clonal hematopoiesis (stem cell disorder) • Marrow hypercellularity • Overproduction of one or more cell lines (effective hematopoiesis) – Exception: myelofibrosis • Differentiation nearly normal The “common” bcr-abl negative myeloproliferative disorders • Polycythemia vera • Essential thrombocythemia • Myelofibrosis/myeloid metaplasia Less common conditions • • • • • Undifferentiated myeloproliferative disorder Mast cell disease Hypereosinophilic syndrome Chronic neutrophilic leukemia Myelodysplastic/myeloproliferative disorders – – – – CMML Atypical CML (BCR-ABL negative) Juvenile CML “Unclassifiable” MDS/MPD JAK-2 • Tyrosine kinase involved in signaling pathways initiated by EPO, TPO, G-CSF and other growth factors • V617F mutations in most cases of PV, ET, MF – Other JAK-2 mutations (exon 12, etc) in a minority of PV cases (almost all cases of PV have a JAK-2 mutation of some type) – Some cases of ET, MF lack JAK-2 mutation • Mutation releases cells from dependence on growth factors • Homozygosity for mutation seen mainly in P vera, associated with disease progression • Specific inhibitors of the kinase now in clinical trials Structure-function relationships in the JAK2 receptor Science 2014; 344:703 In Panel A, in the absence of ligand, the erythropoietin receptor (EPOR) binds JAK2 as an inactive dimer. In cells with wild-type JAK2 protein, the binding of erythropoietin (Epo) to its receptor induces conformational changes in the receptor, resulting in phosphorylation (P) of JAK2 and the cytoplasmic tail of the receptor. This leads to signaling through pathways made up of Janus kinases and signal transducers and activators of transcription (JAK–STAT), phosphatidylinositol 3 kinase (PI3K), and RAS and mitogen-activated protein kinase (RAS–MAPK). In cells with the V617F mutation, the signaling is constitutively increased, even in the absence of erythropoietin. In Panel B, the JAK2 protein binds to multiple cytokine receptors — EPOR, thrombopoietin receptor (MPL), granulocyte colony-stimulating factor receptor (G-CSFR), and probably others — that are important for hematopoietic stem-cell biology and differentiation. Therefore, the JAK2 protein with the V617F mutation exerts its effects at various stages of differentiation and in various lineages. In Panel C, the development of homozygosity for the V617F mutation is a two-step process, with the initial point mutation followed by mitotic recombination of chromosome 9p between the JAK2 locus and the centromere. This results in the loss of heterozygosity but a diploid DNA copy number. NEJM 2006; 355:2452 NEJM 2006; 355:2452 Polycythemia vera • Elevated RBC mass, typically high platelets and WBC – Some patients present with thrombocytosis and develop erythrocytosis subsequently • Hypercellular marrow with variable degree of reticulin fibrosis – Morphology fairly normal, some clustering and dysmorphism of megas • Splenomegaly in 70%, constitutional sx, increased risk of arterial & venous thrombosis (esp portal vein), microvascular disease (erythromelalgia, pruritus, headache, etc), hypermetabolic sx & gout Differential diagnosis of erythrocytosis • H&P – COPD or other possible causes of hypoxemia? – Smoker? – Splenomegaly, pruritus, erythromelalgia? • Concomitant thrombocytosis and/or leukocytosis? • Serum EPO • JAK-2 mutation testing Polycythemia Vera Natural History • Life expectancy decreased (3 deaths/100 pts/yr) • Cardiovascular mortality increased 1.4x • Major thrombosis in 3/100pts/yr • Risk of death from leukemia increased 36fold • Progressive myelofibrosis NEJM 2004; 350:99 NEJM 2004; 350:99 Oxygen delivery vs Hematocrit 180 Oxygen Transport 160 140 120 100 80 60 40 20 0 0 20 40 60 80 Hct J Clin Invest 1963;42:1150 Vaso-occlusion in P vera Thrombosis in myeloproliferative disorders • 41% of deaths in PV from cardiovascular causes – – – – 15% coronary dz 8% CHF 8% non hemorrhagic stroke 8% PE • Complex pathophysiology – Abnormal RBC/WBC/plt function – Activated PMNs/cytokines affect vascular endothelium – Prothrombotic microparticle release – Increased whole blood viscosity Risk factors for thrombosis in myeloproliferative disorders • Hx of thrombosis • Disease category (PV > ET, MF) • Cardiovascular risk factors (lipids, blood pressure, smoking, diabetes) • Age • OCP therapy (splanchnic vein clots) • JAK2 mutation status/allele burden • High hematocrit (PV) & WBC – Extreme thrombocytosis increases bleeding risk • Thrombophilic genetic traits? Prothrombotic effects of erythrocytosis Barbui et al. Blood 2013;122:2176-2184 Hematology 2005:201 Recommendations for treatment of patients with polycythemia vera • • • • Keep Hct < 45 (plebotomy) Low dose ASA unless contraindicated Manage reversible risk factors (BP, lipids, smoking) Consider cytoreduction if: – Intolerant to phlebotomy – Thrombocytosis or substantial leukocytosis – Symptomatic splenomegaly • Choice of cytoreductive therapy: – Age < 40: Interferon-alpha – Age > 40: hydroxyurea – Anagrelide or busulfan for patients intolerant of, or not responsive to, above choices Hematology 2005:201 Aspirin vs placebo in P vera Essential thrombocytosis • Thrombocytosis (typically > 600K) with variable leukocytosis, normal RBC count • About 50% have JAK2 mutation • Normal to mildly hypercellular marrow with marked increase in megakaryocytes, often with clustering • Minimal reticulin fibrosis • Splenomegaly in about 50% • Many patients asymptomatic at diagnosis • Increased risk of arterial and venous thrombosis as well as hemorrhage Thrombocytosis Differential diagnosis • Essential thrombocythemia • Other MPD P vera Myelofibrosis CML • Myelodysplasia (5q- et al) • Reactive Inflammation Surgery/trauma Non-myeloid malignancy Iron deficiency Hemolysis Acute blood loss Absence of spleen Rebound following thrombocytopenia Hematology 2005:201 Essential Thrombocytosis Natural History • • • • • 1-2 cases/100,000/yr Most patients >50, but occurs in young adults Woman more often affected than men Life expectancy normal to slightly decreased Patients > 60, or with prior thrombosis, at increased risk for thrombotic events • Very high platelet counts (>1.5 million) increase risk of bleeding, not thrombosis • Risk of myelofibrosis about 8% at 10 years • Risk of AML about 1% overall Essential Thrombocytosis Treatment • Low-risk patients (young, no vascular risk factors) may not require treatment • Aspirin decreases thrombotic events • Hydroxyurea • Anagrelide • Interferon • Other: busulfan (leukemogenic) Recommendations for treatment of patients with essential thrombocytosis • Manage reversible risk factors (BP, lipids, smoking) • If hx of thrombosis, or age >60, or plts > 1.5 million: – Hydroxyurea – Low dose ASA unless for plts > 1.5 m – 2nd line: Anagrelide or interferon-alpha • Age < 60, no other risk factors: – Low dose ASA Hematology 2005:201 Myelofibrosis • 0.5-1.5 cases/100,000/yr • Most patients >60 • Marrow fibrosis with extramedullary hematopoiesis in spleen, liver, many other tissues – “Prefibrotic” stage with hypercellular marrow & abnormal megakaryocytes • Peripheral leukoerythroblastosis, teardrop cells, often with anemia. WBC and platelet counts may be high, normal or low • Splenomegaly, constitutional symptoms • Poor prognosis: marrow failure, AML in 5-30% Improving survival in MF Median survival 6.5 yrs Median survival 4.5 yrs J Clin Oncol 2012;30:2981 DDx of Marrow Fibrosis • Myeloproliferative disorders • MF > > P vera, ET, CML • Other heme neoplasm • Megakaryocytic leukemia • Hodgkins • Hairy cell leukemia • Non-heme cancer • Non-malignant conditions • Renal osteodystrophy • Autoimmune disease • Vitamin D deficiency Mayo Clin Proc 2004;79:503 SPLENOMEGALY IN MYELOFIBROSIS Myelofibrosis Treatment • Supportive care – Transfusions – Splenectomy • Thalidomide/lenalidomide (low dose) – Reduce transfusion requirements, reduce spleen size • Chemotherapy (limited data; myelosuppression often dose-limiting) – Cladribine – Azacytidine/decitabine – Low dose cytarabine • Marrow transplant in selected patients • JAK inhibitor therapy: Ruxolitinib (inhibits JAK-1 and JAK-2) Ruxolitinib treatment of myelofibrosis Spleens shrink Symptoms improve Better survival NEJM 2012;366:799 Eosinophilia • • • • Non-clonal/secondary (common) Clonal Idiopathic hypereosinophilic syndrome Familial (very rare) Mild: Moderate: Severe: AEC 500-1500 AEC 1500-5000 AEC > 5000 Hypereosinophilia (AEC > 5000) • • • • • • • • • • • • Parasitic infection Drug reaction Allergic gastroenteritis Eosinophilic fasciitis Churg-Strauss syndrome Pulmonary eosinophilia Eosinophilia-myalgia syndrome IL-2 therapy Hyper-IgE syndrome AML Eosinophilic leukemia Hypereosinophilic syndrome Clinical manifestations of hypereosinophilia • Skin: pruritus, angioedema, ulcers, papular or nodular lesions • Heart: endocardial fibrosis, valvular disease, mural thrombi, cardiomyopathy, incr troponin • Lungs: infiltrates, nodules, pleural effusion • Neurologic: poly- or mononeuropathy, transverse myelitis, optic neuritis, CNS vasculitis • GI: hepatosplenomegaly, gastroenteritis, sclerosing cholangitis • Heme: marrow fibrosis, cytopenias • Kidney: thrombotic microangiopathy Secondary Eosinophilia • Infection – Usually parasitic • Allergy – Asthma, allergic rhinitis, dermatitis, urticaria/angioedema, drug reaction • Autoimmune/inflammatory disorders (many) • Paraneoplastic – Solid tumors, lymphomas (Hodgkin>NHL) • Endocrinopathy – Adrenal insufficiency, growth hormone deficiency • Clonal T-cell disorder (→ IL-5) Most cases with IL-5 overproduction Clonal Eosinophilia • Acute leukemia (AML>ALL) • Chronic myeloid disorders – CML (bcr-abl) – Systemic mastocytosis (c-Kit) – 8p11 myeloproliferative disorder (FGFR-1) – PDGFRA and PDGFRB mutations – “Classic” MPD (JAK-2) – MDS – Chronic eosinophilic leukemia Clonal eosinophilic disorders caused by mutations in tyrosine kinase genes • PDGFRA, PDGFRB – May be cytogenetically silent→ FISH testing for dx – Marrow fibrosis, incr mast cells, elevated tryptase → variant of mast cell dz? – Male predominance – Imatinib-responsive (100-400 mg/d) • FGFR1 – Associated with 8p11 translocations – Stem cell disorder → aggressive MPD associated with T-lymphoblastic lymphoma – High dose chemotherapy + allo-HSCT Chronic eosinophilic leukemia WHO diagnostic criteria • • • • • • Eosinophil count > 1500 No Ph chromosome or BCR-ABL fusion No PDGFRB, PDGFRA or FGFR1 rearrangement Blast count in blood and marrow < 20% No inv (16) or other variant characteristic of AML Presence of clonal cytogenetic or molecular abnormality OR blasts >2% in blood or >5% in marrow Idiopathic Hypereosinophilic Syndrome • Persistent moderate or severe eosinophilia (AEC > 1500) with end-organ damage • Other causes of eosinophilia ruled out • Male predominance • Can evolve into overt myeloid or lymphoid neoplasm • Potentially fatal – 10 yr survival < 50% • Treatment – Asymptomatic: corticosteroids vs watchful waiting – Symptomatic patients: corticosteroids, IFNα, hydroxyurea, imatinib, various myelosuppressive agents Laboratory evaluation of hypereosinophilia • • • • Marrow biopsy with cytogenetics FISH for PDGFR mutations Serum tryptase T-cell immunophenotyping and gene rearrangement study • Serum IL-5 • Serum IgE • Screen for organ damage – Echo, troponin level – CXR, PFTs Classification of Mast Cell Disease WHO classification and frequency in Mayo Clinic series • Indolent – often limited to skin (urticaria pigmentosa (46%) • Associated with myeloproliferative disorder (40%) • “Aggressive” mastocytosis – with lymphadenopathy & eosinophilia (12%) • Mast cell leukemia (1%) Blood 2009;113:5727 WHO Diagnostic Criteria for Mast Cell Disease • Major: multifocal dense infiltrates of mast cells (15+) in marrow or other extracutaneous organs • Minor – >25% spindle shaped or otherwise atypical MC – c-KIT codon 816 mutation – MC in marrow or other extracutaneous organ express CD2 and/or CD25 – Serum tryptase persistently >20 ng/ml in the absence of another clonal myeloid disorder Diagnosis requires major + 1 minor criterion or at least 3 minor criteria Stuff in mast cell granules that could make you sick Metcalfe, Blood 2008;112:946 Clinical & laboratory features of mast cell disease • Skin: Urticaria pigmentosa, Darier sign (dermatographism), telangiectasias • Lymphadenopathy • Hepatosplenomegaly • Constitutional symptoms • Recurrent anaphylaxis • GI symptoms (N/V, diarrhea, abd pain, peptic ulcer) • Elevated serum/urinary histamine levels • Elevated serum tryptase (96%) • Cytopenias • Eosinophilia • Coagulopathy (heparin in mast cells) – rare • Lytic or blastic bone lesions ISM: Indolent MCD SM-ANMD: associated with clonal non-mast cell lineage disease ASM: Aggressive MCD MCL: Mast cell leukemia Blood 2009; 113: 5727 Mastocytosis in bone marrow H&E Tryptase Mastocytosis in bone marrow Skin findings in mast cell disease Dermatographism Urticaria pigmentosa Telangiectasia macularis eruptiva perstans Molecular biology of mast cell disease • A majority of patients have D816V mutation in c-KIT tyrosine kinase gene (imatinib-insensitive) – A minority have other mutations, may be imatinib-sensitive – Occasionally found together with JAK2 V617F • Some patients have eosinophilia & PDGFRA mutation (imatinib-responsive) Treatment of mast cell disease • • • • • Antihistamines, PPIs Vit D/Calcium, bisphosphonates Glucocorticoids Epinephrine (for anaphyactic reactions) For aggressive disease: – Interferon – Imatinib (if there is an imatinib-sensitive mutation) • Other TKIs (dasatinib, nilotinib)? – Cladribine – Combination chemotheapy – Allo-HSCT Survival of patients with MCD Blood 2009; 113: 5727