post hoc ergo propter hoc
advertisement

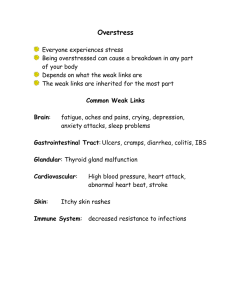
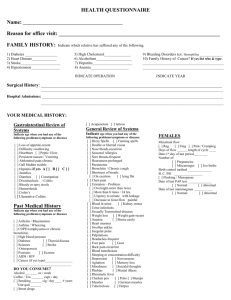
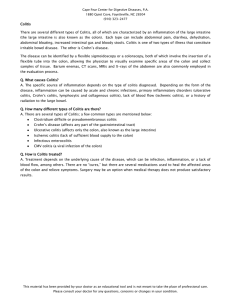
post hoc ergo propter hoc General Internal Medicine Conference Case Presentation April 16 2008 Pedro Salinas HPI 60 y/o woman with h/o IBS 3 week h/o vomiting, diarrhea and right upper quadrant pain 10 episodes/day watery stools, maladorous, non-relieved by fasting. No blood or mucus seen H&P Cont.. Last colonoscopy 2 year ago (OSH), which reported normal per patient PMH HTN h/o PE RA-seronegative Osteopenia Raynaud’s Migraines IBS Benign breast mass GERD 1995 Diagnosed with Undefined Connective Tissue disease. Seronegative . High inflammatory markers 2002 GI Nausea, weight loss. CT pancreatic head fullness Normal ERCP and pancreatogram 2005 EGD and EUS Home Medications ASA 81 mg PO qd Lisinopril 10 mg PO qd Metoprolol 50 mg PO bid Simvastatin 40 mg PO qhs MVI PO qd Amitriptylline 50 mg qhs Ca/Vit D PO bid FiberCon PO qd Nifedipine ER 90 mg PO qd H&P Cont.. Allergies: Penicillin and Naproxen FamHx: Father died age 64 from massive stroke. Mother died age 69 lung cancer. No colon cancer. SocHx:Lives at Friendship, WI. +tobacco 1ppd. 1-2 drinks/wk. No illicit drug use. H&P Cont.. T 97.7 HR 100 RR 16 BP 138/73 O2 98% on RA HEENT: PERRLA, EOMI, no oral lesions. No thyromegaly. CV: PMI non-diplaced, RRR, S1/S2 3/6 SEM radiating base neck Lungs: CTAB Abdomen: Mild tenderness RUQ. No guarding. +BS Ext: no edema. Skin: no rash. Addendum written that morning on record: I saw….. Prolonged course for her typical IBS… Will contact GI for need to investigate for microscopic colitis…… On GI Consult Note: Reason for consultation: Diarrhea Labs CRP 8 Normal Stool Gap Guiac neg. C diff. Neg TTG Antibodies Neg Microscopic Colitis Lymphocytic colitis and collagenous colitis Sixth decade of life CC 10-15.7/100 000 LC 14.2/100 000 Female:male ratio 7:1 in CC and 2:1 in LC Concomitant autoimmune diseases Microscopic colitis Chronic non-bloody diarrhea, abdominal pian, weight loss. Fatigue, nausea and fecal incontinence. Enteropathic arthritis in 7%, seronegative and nonerosive Clinical course is most often chronic relapsing and benign Macroscopically normal or near normal mucosa Histopathology Microscopic assessment of colonic mucosal biopsies Edema, erythema or abnormal vascular pattern 30% Colagenous colitis: thickening of subepithelial collagen layer beneath basal membrane Lymphocytic colitis: characteristic increase in intraepithelial lymphocytes >20 IEL/100 epithelial cells Treatment Cochrane Database Review 2007 Only one RCT with Bismuth with clinical improvement but not statistically significant or histologic improvement Mostly anecdotal evidence and extrapolation from collagenous colitis Confirmation Bias selective focus upon evidence that supports their beliefs or what they want or believe to be true, while ignoring evidence that serves to disconfirm those ideas Francis Bacon described confirmation bias as follows in 1620 The human understanding when it has once adopted an opinion (either as being the received opinion or as being agreeable to itself) draws all things else to support and agree with it. And though there be a greater number and weight of instances to be found on the other side, yet these it either neglects and despises, or else by some distinction sets aside and rejects; in order that this great and pernicious predetermination the authority of its former conclusions may remain inviolate