Temporary Epicardial Cardiac Pacing
advertisement

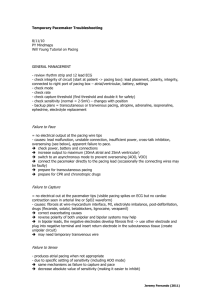
Temporary Epicardial Cardiac Pacing 30/11/10 PY Mindmaps USES/INDICATIONS – post cardiac surgery - conduction abnormality (bradyarrhythmias) - tachycardia (AV junctional tachycardia, SVT, VT, atrial flutter) - other: restoration of AV synchrony, HOCM to prevent SAM DESCRIPTION - produce electrical current with subsequent depolarisation + sensing function Unipolar - negative wire attached to the epicardium - positive wire attached to subcutaneous tissues Bipolar - a single wire with two conductors insulated from one another which both run to the epicardial surface - smaller distance for current to run -> threshold less - more suitable for dual chamber applications - require less energy to begin with and may have greater longevity compared to unipolar system. METHOD OF INSERTION AND/OR USE Jeremy Fernando (2010) Typical Settings - atrial and ventricular output 10mA - lower rate 80/min - atria and venticular sensitivity 2-5mV - PR interval 150ms or ‘auto’ (determined by rate) - PVARP 250ms or ‘auto’ (determined by rate) = post ventricular (pacing spike) atrial refractory period OTHER INFORMATION Daily Checks - assess underlying rhythm (turn pacemaker rate down and assess) - test sensitivity (minimum current that the pacemaker is able to sense -> place in VVI, AAI or DDD, increase sensitivity until the sense indicator stops flashing -> asynchronous pacing should take place, then turn sensitivity down until sense indicator flashes which each endogenous depolarisation -> this equals the pacing threshold -> set pacing generator at half the pacing threshold) - capture threshold (minimum output required to stimulate an action potential in the myocardium -> set rate above native rate, then reduce output until QRS no longer follows pacing spike = capture threshold, leave output at twice the threshold) Jeremy Fernando (2010) COMPLICATIONS - infection myocardial damage perforation tamponade disruption of coronary anastomoses undersensing oversensing failure to capture unstable lead position Removal of wire - gentle traction allowing cardiac motion to help dislodgement - if they get cut, cut close to skin so they will retract. MRI - can’t have MRI’s c/o the amount of ferrous material in pacing box - controversial regarding in situ epicardial wires IABP - if IABP is timed according to ECG with high frequency filter disabled (allowing pacing spikes to become visible) -> pacing spikes can be misinterpreted by the IABP as QRS complexes - IABP should be timed according the arterial pulse or the high frequency filter applied - less problematic with bipolar leads Jeremy Fernando (2010)