Cardiovascular complications of cocaine abuse
advertisement

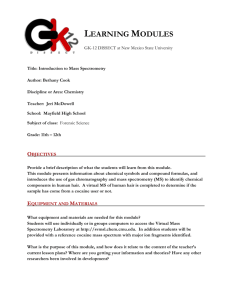
Cardiovascular complications of cocaine abuse James P Morgan, MD, PhD UpToDate performs a continuous review of over 350 journals and other resources. Updates are added as important new information is published. The literature review for version 14.2 is current through April 2006; this topic was last changed on May 9, 2006. The next version of UpToDate (14.3) will be released in October 2006. INTRODUCTION — Cocaine is the second most commonly used illicit drug in the United States, ranking after marijuana. It is most frequently used by males between the ages of 18 and 25 [1]. The 1998 National Household Survey on Drug Abuse (NHDSA) estimated that approximately 11 percent of the population has used cocaine at some point in their lifetime [1]. Another 1998 report estimated that about 2000 people use cocaine for the first time every day [2,3]. The great epidemic of cocaine abuse in the United States peaked in 1985, when 5.7 million people were current users of cocaine (3 percent of the population); the number of current users decreased to 1.4 million (0.7 percent of the population) by 1992, and by 1998 had not significantly changed, especially among persons over the age of 35 [1,4]. Crack cocaine use has also remained unchanged since 1988. Because even casual use of cocaine may be associated with acute or chronic toxicity, these large numbers of exposed individuals represent a reservoir of patients who may present with sequelae related to the cardiovascular or other systems in the body. Thus, identification of cocaine exposure is a legitimate goal of cardiovascular history taking, particularly with regard to the occurrence of symptoms associated with ischemic heart disease. The most common complaints from cocaine users entering emergency departments are related to the cardiovascular system [5], although a variety of other organ systems may be involved [6-8]. The vascular complications of cocaine toxicity include: Cardiac — myocardial ischemia, coronary vasospasm, myocardial infarction (MI), arrhythmias, myocarditis, and cardiomyopathy Neurologic — intracerebral hemorrhage, cerebral infarction, seizures, migraine headache, and vasculitis [9] Vascular — aortic dissection and rupture, hypertension, vasculitis [ 10] Gastrointestinal — mesenteric ischemia and infarction, gastrointestinal perforation [11] Pulmonary — pulmonary edema, infarction, hemoptysis [12] (see "Pulmonary complications of cocaine abuse"). Musculoskeletal — rhabdomyolysis, which can lead to acute renal failure [13] (see "Clinical features and prevention of heme pigment-induced acute tubular necrosis") Dermatologic (ischemia) Uterine, placental, obstetric and neonatal — abruptio placentae, spontaneous abortion, prematurity, developmental delays, growth retardation, and congenital abnormalities Genitourinary — renal and testicular infarction Venous — superficial and deep venous thrombosis and thrombophlebitis Among the cardiac complications, myocardial ischemia and infarction have been most commonly reported in clinical and autopsy studies, although their exact incidence is difficult to state with certainty since only a fraction of symptomatic patients come to medical attention. When not attributed to trauma or infection with HIV, the marked increase in fatalities among cocaine abusers is due to cardiovascular causes. There is no evidence to suggest that preexistent vascular disease or other abnormalities are essential prerequisites for the development of a cocaine-related cardiovascular event [7]. However, certain subgroups of patients may be at increased risk of manifesting cardiovascular toxicity if exposed to cocaine, including those who consume alcohol, are pregnant, or infected with HIV. PHARMACOLOGY OF COCAINE — Cocaine (benzoylmethylecgonine, C17, H21, NO4) is an alkaloid prepared from the leaves of the Erythroxylon coca plant. The crystalline form of cocaine is prepared by dissolving the alkaloid in hydrochloric acid to form the water soluble salt, cocaine hydrochloride. Street cocaine is typically in the form of hydrochloride salt. Crack is unpurified free base cocaine, which is formed by combining cocaine hydrochloride with an alkaline substance, such as sodium bicarbonate, and cooking it in water. This forms an oil-like substance that separates from water and solidifies into small pieces, or "rocks." These pieces can be combined with tobacco to form a cigarette or can be smoked in a water pipe. Free base is a purer form of cocaine that is ether-extracted and is not as widely available as crack [14]. Absorption — Cocaine is absorbed from mucus membranes, and the respiratory, gastrointestinal and genitourinary tracts in both the hydrochloride and base forms. Onset of action — The peak onset of action for the intravenous and inhalation routes is approximately one-half to two minutes. In comparison, the peak effect occurs later with the intranasal (up to 20 minutes) and gastrointestinal routes (up to 90 minutes). Half-life — After intravenous or inhalation administration, the plasma half-life approximates 60 minutes; cocaine's vasoconstrictive properties inhibit absorption by the intranasal route, prolonging the apparent plasma half-life to two to three hours [7]. Duration of action — The duration of effect is approximately 15 to 30 minutes by intravenous or inhalation routes, one hour by intranasal exposure, and as long as three hours after gastrointestinal absorption. Metabolism — Cocaine is detoxified by plasma and hepatic cholinesterase and nonenzymatic hydrolysis to the inactive water-soluble metabolites benzoylecgonine and ecgonine methyl ester, which are excreted in the urine along with small amounts of unchanged cocaine (10 to 20 percent). Cholinesterase activity is lower in the fetus, infants, pregnant women, the elderly, and those with liver disease or pseudocholinesterase deficiency. Thus, the use of cocaine by individuals in any of these categories carries increased risks. Metabolites — After administration, the urine remains positive for cocaine metabolites for 72 hours, which is useful for documenting recent exposure to the drug [15,16]. Norcocaine is the only known active metabolite of cocaine that is present in significant concentration in the blood. It is formed by an N-demethylation reaction and usually represents less than 5 percent of the total quantity of cocaine metabolites, but may mediate delayed effects of cocaine via enterohepatic recirculation [17]. When cocaine is administered as a smoke in "crack," another group of compounds is produced, either as by-products of the smoking procedure or as metabolites. Anhydroecgonine methyl ester (AEME) and noranhydroecgonine methyl ester (NAEME) are pyrolysis products of cocaine that have pharmacologic activity [18]. As a result, the potential influence of these products must be considered when evaluating the effects of cocaine on cardiovascular function. MECHANISM OF CARDIOVASCULAR EFFECTS — The major cardiovascular effects of cocaine and its active metabolite, norcocaine, appear to be caused by the inhibition of norepinephrine reuptake into the synaptic cleft by sympathetic neurons. Since reuptake is the major mechanism by which neurotransmitter is removed from its active receptor sites, this inhibition results in potentiation of the response to sympathetic stimulation of innervated organs and to infused catecholamine. Cocaine may also enhance the release of catecholamines from central and peripheral stores [19]. In addition to its effects as a sympathomimetic agent, cocaine is the only known naturally occurring local anesthetic. However, its use in ear, nose, eye, and throat surgery has steadily declined due to its perceived arrhythmogenic potential [20]. The cardiovascular responses produced by intravenous, intranasal, and inhaled cocaine are the same. The drug induces a dose-dependent increase in blood pressure and heart rate, which in usual recreational doses is, in most cases, relatively modest and well within the range of physiologic changes observed in normal humans. Fortunately, MIs and life-threatening arrhythmias are rare, even in patients with advanced coronary disease [19]. At the cellular level, cocaine's sympathomimetic actions are mediated by stimulation of the alpha- and beta-adrenergic receptors. Cocaine may also interact with the muscarinic receptors, and is known to inhibit reuptake of dopamine and serotonin by dopaminergic and serotonergic nerve endings, respectively [ 21]. As with other local anesthetic agents, cocaine inhibits sodium currents in excitable cells [ 22]. CARDIOVASCULAR SYNDROMES ASSOCIATED WITH COCAINE USE — Cocaine use is associated with a number of cardiac problems, including ischemia, myocarditis and the development of a cardiomyopathy, and arrhythmias. Myocardial ischemia — An acute coronary ischemic syndrome is the most common cardiac pathology associated with cocaine abuse and can occur with all routes of cocaine intake [23,24]. The precise incidence of myocardial ischemia, with or without infarction, is difficult to quantitate. It is probably safe to say that the number of patients in whom cocaine use is identified as a potential causative factor and who come to medical attention is small relative to the total population of abusers. In some cases, the relationship of the ischemic event to cocaine use is unclear based upon the time of onset of symptoms versus the known pharmacokinetics of cocaine and it metabolites [25]. Myocardial infarction — MI is a well-described complication among patients presenting with cocaine-induced ischemic symptoms. In one study of 246 patients presenting to an emergency department with cocaine-associated chest pain, 5.7 percent had an MI documented by elevated serum CK-MB [26]. One survey of 10,085 adults between the age of 18 and 45 found that 25 percent of nonfatal MIs were attributable to frequent cocaine use [27]. (See "Coronary heart disease and myocardial infarction in young men and women"). Most patients have their infarction within three hours of using cocaine, but the range varies from one minute to four days [24]. In a series of 3946 patients who had had an acute MI, 1 percent had used cocaine within the previous year [28]. In the latter group, approximately 25 percent used cocaine within the 60 minutes prior to the infarct. It was estimated that the risk of an MI was increased 24 times over baseline in the 60 minutes after cocaine use (show figure 1). The occurrence of MI after cocaine use is unrelated to the dose or frequency of use. The anterior wall is the most frequent site of infarction (77 percent in one review) among the patients with cocaine-associated infarction in whom coronary anatomy has been defined [29]. MI associated with cocaine abuse often occurs in patients with normal coronary arteries [24,29]. Most patients smoke cigarettes but many have no other cardiac risk factors [25,28-30]. Approximately one-half have noted previous episodes of chest pain [24]. These observations illustrate the importance of questioning all patients with an acute chest pain syndrome in the absence of trauma about possible cocaine use [ 31,32]. This is particularly true in younger patients [28]. (See "Pathophysiology and clinical presentation of ischemic chest pain"). Mechanisms — Four mechanisms have been proposed for cocaine-induced ischemia. It is difficult or even impossible to determine a predominant mechanism in most patients, and it is likely that more than one may be contributing to the clinical syndrome. Increased myocardial oxygen demand — Increased myocardial oxygen demand occurs secondary to the sympathomimetic actions of cocaine that increase myocardial inotropy, heart rate and systemic blood pressure [33]. This may pose a significant problem to patients in whom coronary blood flow is compromised by the presence of fixed stenoses. As noted above, however, most patients do not have significant underlying coronary disease [24,29]. Coronary artery vasoconstriction and spasm — Cocaine induces constriction of the large and small coronary vessels under some circumstances [33-35]. The vasoconstrictor effects of cocaine on the large coronary arteries are mediated primarily through stimulation of the alpha-adrenergic receptors [33]; cholinergic stimulation of microvessel contraction appears to play a role in some animal models of cocaine toxicity [36]. Cocaine also causes endothelial dysfunction and impairs endothelium-dependent vasorelaxation [37]. Coronary artery thrombosis — Pathologic and angiographic studies have demonstrated coronary thrombi in some patients with cocaine-related MI [26]. In vitro studies have demonstrated that cocaine can activate platelets, increase platelet aggregability, and potentiate thromboxane production; each of these changes can promote thrombus formation [38-40]. Coronary artery aneurysm — Coronary artery aneurysms may be relatively common in cocaine users who undergo angiography. This was illustrated in a review of 112 consecutive patients with a history of cocaine use who underwent coronary angiography, mostly for an acute coronary syndrome, stable angina or a positive stress test, heart failure, or atypical chest pain [41]. The patients were compared to a matched control group of similar age and risk factors in whom angiography was performed in the same time. Coronary artery aneurysms were noted in 34 of the cocaine users (30.4 percent) compared to 7.6 percent of controls. Myocarditis and cardiomyopathy — Myocarditis is a common autopsy finding among subjects dying from cocaine abuse, affecting as many as 20 to 30 percent of patients in some series [42-44]. Myocarditis has also been reported on myocardial biopsies of active users [43]. The precise mechanism of the myocarditis is not clear, and hypotheses range from hypersensitivity reactions leading to vasculitis and myocarditis to catecholamine-induced toxicity. In its early stages, cocaine induced myocarditis is fully reversible [45]. Several cases of dilated cardiomyopathy have been documented among cocaine users, although a cause and effect relationship has not as yet been definitively established [46]. The precise mechanism is not known but the following may contribute [47]: Cocaine exerts direct toxic effects on the heart, which lead to the destruction of myofibrils, interstitial fibrosis, myocardial dilation, and heart failure [ 44]. The cocaine-induced hyperadrenergic state may contribute via production of contraction band necrosis in the heart. Both myocarditis and cardiomyopathy may be caused by infectious agents in subjects who abuse cocaine parentally, either through direct invasion of the myocardium or stimulation of an autoimmune reaction. (See "Etiology and pathogenesis of myocarditis"). Cardiomegaly with otherwise unexplained heart failure in a young person should raise the possibility of cocaine abuse [47]. Abstinence usually leads to complete reversal of the myocardial dysfunction [48-50]. Arrhythmias and conduction abnormalities — The arrhythmogenic potential of cocaine is poorly understood, but because of its pharmacological profile and ability to induce a hyperadrenergic state, it is likely that the drug can produce or exacerbate arrhythmias and conduction abnormalities under some circumstances [ 25,42]. Sinus tachycardia and bradycardia, bundle-branch block, sudden death (ventricular fibrillation or asystole), ventricular tachycardia and accelerated idioventricular rhythm, heart block, torsade de pointes, a variety of supraventricular arrhythmias, and an ECG pattern typical of Brugada syndrome (a pseudo-right bundle branch block and persistent ST segment elevation in V1 to V3), and QT prolongation have all been observed with cocaine use [5,23,51-56]. Cocaine acts like a class I antiarrhythmic agent, producing local anesthetic effects via sodium channel blockade in the heart [57]. When cocaine is used as a local anesthetic during laryngoscopy, the frequency of premature ventricular complexes increases. The potential mechanisms for arrhythmogenesis include: Altering automaticity by a direct effect on myocardium Altering autonomic balance by increasing circulating catecholamine levels Inducing ischemia with resultant electrical inhomogeneity Creating an anatomic substrate for reentrant arrhythmia Altering repolarization with QT prolongation Unless an MI occurs, the rhythm disturbances associated with cocaine abuse are transient and disappear when the drug is metabolized. Stroke — Cocaine abuse significantly increases the risk of ischemic stroke [ 58,59]. The etiology of cocaine-induced brain ischemia is multifactorial: Cocaine stimulates vasospasm, presumably by increasing levels of extracellular monoamines, particularly dopamine [60,61]. Cocaine may cause thrombus formation in the cerebral vasculature, in the same way that it causes coronary artery thrombosis (see above) [62]. Long-term cocaine use may cause pathologic changes in the cerebral vasculature (vasculitis) that impair cellular oxygenation by exacerbating nonlaminar blood flow and sludging in the vessels, with consequent increase in platelet aggregation and thrombus formation [10,63]. Regardless of the precise mechanism, cocaine-induced cerebral ischemia can cause marked hypoperfusion abnormalities associated with severe neurologic deficits. More subtle cognitive deficits also can occur [64]. Over time, repeated ischemic episodes and subsequent reperfusion can weaken vessel walls, thereby increasing the likelihood of cerebral hemorrhage [65]. The dihydropyridine calcium channel antagonists may prevent cocaine-induced cerebral vasospasm [65]; this requires further study. Miscellaneous cardiac complications — Cocaine abuse can produce a variety of other complications, including left ventricular hypertrophy, infectious endocarditis among intravenous users, and mesenteric ischemia [7]. In addition, an acute aortic dissection can result from the use of crack cocaine; it is a frequent cause of dissection in a young, inner city population (37 percent in one report) [ 66]. (See "Clinical manifestations and diagnosis of aortic dissection"). SPECIAL CONSIDERATIONS — There are several clinical situations in which the cardiovascular toxicity of cocaine may be exacerbated and thereby raise additional concerns. Pregnancy — Cocaine use during pregnancy has been associated with abruption placentae, premature labor and delivery, and fetal and neonatal neurologic abnormalities. The basic mechanism of these effects have not been elucidated, but because cocaine has significant cardiovascular actions, these may include direct actions upon the fetal heart and circulation in addition to maternal vasoconstriction and impairment of uterine blood flow [67]. Pregnant animals show accentuated heart rate and blood pressure responses to cocaine administration, an effect that may be mediated in part by reduced cholinesterase activity which reduces cocaine metabolism. Alcohol — A variety of epidemiologic, observational, and toxicology studies have suggested that the combination of alcohol and cocaine produces increased toxicity in addition to behavioral change. Alcohol alters cocaine kinetics and metabolism and results in the generation of new and pharmacologically active metabolites, such as cocaethylene. The pharmacologic properties of cocaethylene are similar to those of cocaine, and it has been hypothesized that the enhanced toxicity of the cocaine plus alcohol combination is due primarily to generation of this long-lasting metabolite [68,69]. Adulterants — All street forms of cocaine contain adulterants, some of which may have pharmacologic activity. The most common cocaine adulterants are sugars and stimulants, including ephedrine, phenylpropanolamine, caffeine, and amphetamines. Quinine and strychnine may be added, which can produce rhabdomyolysis and acute renal failure. Local anesthetics are common adulterants that may cause central stimulation or cardiovascular depression in large doses [14]. Human immunodeficiency virus — Patients with HIV infection can develop cardiac dysfunction via a variety of mechanisms. Among the complications in such patients are pericarditis, myocarditis, ventricular tachycardia, infective endocarditis, metastatic involvement from Kaposi's sarcoma, and dilated cardiomyopathy. ( See "Cardiac involvement in HIV-infected patients"). Since cocaine use increases libido and impairs judgment, it may lead to an increased incidence of sexually transmitted diseases, including HIV-infection and AIDS [14]. Whether or not cocaine increases the risk of cardiac involvement in patients with HIV-infection, and, in particular, myocarditis, is currently under active investigation. MANAGEMENT OF COCAINE-RELATED CHEST PAIN — Chest pain is the most common cocaine-related medical problem, and has been estimated to result in the emergency department evaluation of over 64,000 patients annually for possible MI. ( See "Diagnostic approach to chest pain in adults"). Of these patients, 57 percent are admitted to the hospital [26]. In 2002, an ACC/AHA Task Force published guidelines for the management of patients with chest pain after cocaine use (show table 1) [70]. Diagnosis — As noted above, the typical patient with a cocaine-related MI is a young man with a history of repetitive cocaine use but without cardiac risk factors other than tobacco smoking [25,28-30]. The chest pain is often accompanied by anxiety, dyspnea, palpitations, and nausea. The risk of infarction is greatest within the first hour after cocaine use, elevated almost 24-fold over baseline, and decreases progressively thereafter (show figure 1) [28]. As a result, all patients with an acute coronary syndrome, particularly those with the above characteristics, should be carefully questioned about cocaine use [31,32]. Toxicology assays for the drug or its metabolites may be useful if exposure to cocaine is suspected or requires confirmation. Electrocardiogram — The electrocardiogram (ECG) is particularly difficult to interpret in young patients who have a relatively high incidence of early repolarization changes and left ventricular hypertrophy. As an example, up to 84 percent of patients with cocaine-associated chest pain may have abnormal electrocardiograms; up to 43 percent of cocaine abusers without an MI may have ST segment elevation 0.1 mV in two or more contiguous ECG leads [26,30]. On the other hand, MIs occur in some patients with an ECG that is normal or has only nonspecific findings. Because of the difficulty in identifying cocaine users with chest pain who are at low risk of infarction, most are admitted to the hospital [26]. Serum markers — Some of the newer markers of ischemia, such as serum troponin I or troponin T, appear to be specific for cardiac damage [70,71]. In contrast, chemical markers such as myoglobin, CK, and CK-MB may be elevated in the absence of infarction if skeletal muscle injury, rhabdomyolysis, or increased motor activity have occurred. This was illustrated in a study of 97 patients presenting with chest pain, 20 percent of whom had recent cocaine use [72]: The specificity of myoglobin was altered by recent cocaine use The specificity of CK-MB was affected less The specificity of cardiac troponin I was unaffected (See "Troponins, creatine kinase, and CK isoforms as biomarkers of cardiac injury" and see "Biomarkers of cardiac injury other than troponins and creatine kinase"). Treatment — There have been no well-designed, randomized, prospective clinical trials to compare treatment strategies for cocaine-associated coronary ischemia. However, a general approach to such patients has been proposed by an ACC/AHA task force, based upon well-controlled trials in animals, experimental trials in the catheterization laboratory, observational studies, case series, and case reports ( show table 1) [30,70]. The three first-line drugs are benzodiazepines, aspirin, and nitrates. Benzodiazepines reduce blood pressure and heart rate in part through their anxiolytic effects and are therefore recommended for patients with cocaine-associated ischemia who are hypertensive, tachycardic, or anxious. Aspirin should be administered to prevent thrombus formation and nitrates to reverse cocaine-induced coronary artery vasoconstriction. The administration of oxygen should also be considered as a measure to limit ischemia. Several other therapies can be considered if the patient continues to have chest pain or ischemic changes after initial therapy. Calcium channel blockers and alpha-blockers (phentolamine), which are coronary vasodilators, are reasonable additions to, or replacements for, therapy with nitrates. As noted above, the coronary vasoconstriction induced by cocaine is largely mediated by alpha-adrenergic stimulation [33]. On the other hand, beta blockers and drugs with mixed alpha and beta-adrenergic blocking properties should probably be avoided, since these drugs may exacerbate cocaine-induced vasoconstriction, increase the incidence of complications, and, perhaps, even decrease survival [73]. (See "Antiischemic agents in the management of unstable angina and acute non-ST elevation (non-Q wave) myocardial infarction"). Acute myocardial infarction — Patients in whom acute myocardial infarction is likely or definitively diagnosed may require cardiac catheterization for diagnosis followed by primary angioplasty or thrombolytic therapy [74]. (See "Overview of the management of acute ST elevation (Q wave) myocardial infarction"). Patients with an acute MI secondary to cocaine use have similar complications to those seen in the absence of drug abuse. As an example, one study of 130 patients with cocaine-associated acute MI found that 36 percent had a complication, including heart failure and sustained ventricular and supraventricular tachyarrhythmias; these complications typically within the first 12 hours [75]. Antiarrhythmic agents should be used with caution during the early period after exposure to cocaine, since the proarrhythmic and proconvulsant effects of these drugs may be additive to that of cocaine. However, the use of lidocaine or related drugs is rational after the immediate period of exposure has passed. Sodium bicarbonate may be a safer approach to reversing cocaine-mediated conduction abnormalities and rhythm disturbances, but this modality is still under investigation [26]. Undifferentiated chest pain — Short-term evaluation of patients for 12 to 24 hours in a chest pain observation unit is becoming an increasingly popular approach to patients with chest pain who have a low likelihood of significant coronary disease. (See "Evaluation and management of suspected acute coronary syndrome in the emergency department"). A similar approach can be taken to cocaine-related chest pain, since the incidence of late complications among patients who have been ruled out for an MI appears to be extremely low. This was illustrated in a study of 203 patients with cocaine-associated chest pain; the one-year survival was 98 percent and the incidence of late MI was only 1 percent [76]. Further confirmation of the value of a chest pain observation unit for such patients was provided by a subsequent prospective study that evaluated 344 patients presenting with chest pain who reported cocaine use within the prior week and/or had a positive urine test for cocaine metabolites [77]. Forty-two patients (12 percent) were directly admitted due to ST segment elevation or depression of 1 mm or more for at least one minute, elevated cardiac enzyme levels, recurrent ischemic chest pain, or hemodynamic instability. The remaining 302 patients were evaluated in a chest pain observation unit for nine to twelve hours. None of these patients developed heart failure or dysrhythmias during observation; 158 underwent exercise testing, which led to catheterization in four. At 30 days, there were no cardiovascular deaths and no sustained ventricular arrhythmias. There were four subsequent MIs, all in patients who continued to use cocaine. Cessation of cocaine use — Cessation of cocaine use is obviously essential for secondary prevention, although modification of other risk factors, in particular, tobacco smoking, may also play a role. Unfortunately, among patients with cocaineassociated chest pain, approximately 60 percent admit to continued cocaine use in the year after a symptomatic episode [76]. (See "Overview of the recognition and management of the drug abuser"). Use of UpToDate is subject to the Subscription and License Agreement. REFERENCES 1. 2. 3. 4. 5. 6. 7. 8. 9. 10. 11. 12. 13. 14. 15. 16. National Household Survey on Drug Abuse: Main Findings. Department of Health and Human Services, Substance Abuse and Mental Health Services Administration, Rockville, MD 2000. National Household Survey on Drug Abuse: Population Estimates 1998, Substance Abuse and Mental Health Services Administration, August 1999. www.health.org/dynatable/ndu.asp. NIDA Research Report - Cocaine Abuse and Addiction: NIH Publication No. 99-4342, 1999. Lange, RA, Hillis, LD. Cardiovascular complications of cocaine use. N Engl J Med 2001; 345:351. Brody, SL, Slovis, CM, Wrenn, KD. Cocaine-related medical problems: Consecutive series of 233 patients. Am J Med 1990; 88:325. Goldfrank, LR, Hoffman, RS. The cardiovascular effects of cocaine. Ann Emerg Med 1991; 20:165. Warner, EA. Cocaine abuse. Ann Intern Med 1993; 119:226. Daras, M, Tuchman, AJ, Marks, S. Central nervous system infarction related to cocaine abuse. Stroke 1991; 22:1320. Krendel, DA, Ditter, SM, Frankel, MR, Ross, WK. Biopsy-proven cerebral vasculitis associated with cocaine abuse. Neurology 1990; 40:1092. Niazi, M, Kondru, A, Levy, J, Bloom, AA. Spectrum of ischemic colitis in cocaine users. Dig Dis Sci 1997; 42:1537. Haim, DY, Lippmann, ML, Goldberg, SK, Walkenstein, MD. The pulmonary complications of crack cocaine. A comprehensive review. Chest 1995; 107:233. Roth, D, Alarcon, FJ, Fernandez, JA, et al. Acute rhabdomyolysis associated with cocaine intoxication. N Engl J Med 1988; 319:673. Hannan, DJ, Adler, AG. Crack abuse. Do you known enough about it?. Postgrad Med 1990; 88:141. Das, G. Cardiovascular effects of cocaine abuse. Int J Clin Pharmacol Ther Toxicol 1993; 31:521. Om, A, Ellahham, S, DiSciascio, G. Management of cocaine-induced cardiovascular complications. Am Heart J 1993; 125:469. Inaba, T, Stewart, DJ, Kalow, W. Metabolism of cocaine in man. Clin Pharmacol Ther 1978; 23:547. 18. Schindler, CW, Tella, SR, Erzouki, HK, Goldberg, SR. Pharmacological mechanisms in cocaine's cardiovascular effects. Drug Alcohol Depend 1995; 37:183. 19. Gradman, AH. Cardiac Effects of Cocaine: A review. Yale J Biol Med 1988; 61:137. 20. Orr, D, Jones, I. Anaesthesia for laryngoscopy. A comparison of the cardiovascular effects of cocaine and lignocaine. Anaesthesia 1968; 23:194. 21. Xiao, YF, Morgan, JP. Cocaine blockade of the acetylcholine-activated muscarinic K+ channel in ferret cardiac myocytes. J Pharmacol Exp Ther 1998; 284:10. 22. Mouhaffel, AH, Madu, EC, Satmary, WA, Fraker, TD Jr. Cardiovascular complications of cocaine. Chest 1995; 107:1426. 23. Isner, JM, Estes, NA, Thompson, PD, et al. Acute cardiac events temporally related to cocaine abuse. N Engl J Med 1986; 315:1438. 24. Hollander, JE, Hoffman, RS. Cocaine-induced myocardial infarction: an analysis and review of the literature. J Emerg Med 1992; 10:169. 25. Lange, RA, Willard, JE. The cardiovascular effects of cocaine. Heart Dis Stroke 1993; 2:136. 26. Hollander, JE, Hoffman, RS, Gennis, P, et al. Prospective multicenter evaluation of cocaine-associated chest pain. Cocaine Associated Chest Pain (COCHPA) Study Group. Acad Emerg Med 1994; 1:330. 27. Qureshi, AI, Suri, MF, Guterman, LR, Hopkins, LN. Cocaine Use and the Likelihood of Nonfatal Myocardial Infarction and Stroke: Data From the Third National Health and Nutrition Examination Survey. Circulation 2001; 103:502. 28. Mittleman, MA, Mintzer, D, Maclure, M, et al. Triggering of myocardial infarction by cocaine. Circulation 1999; 99:2737. 29. Minor, RL Jr, Scott, BD, Brown, DD, Winniford, MD. Cocaine-induced myocardial infarction in patients with normal coronary arteries. Ann Intern Med 1991; 115:797. 30. Hollander, JE, The management of cocaine-associated myocardial ischemia. N Engl J Med 1995; 333:1267. 31. Clinical policy for the initial approach to adults presenting with a chief complaint of chest pain, with no history of trauma. American College of Emergency Physicians. Ann Emerg Med 1995; 25:274. 32. Hollander, JE, Brooks, DE, Valentine, SM. Assessment of cocaine use in patients with chest pain syndromes. Arch Intern Med 1998; 158:62. 33. Lange, RA, Cigarroa, RG, Yancy, CW Jr, et al. Cocaine-induced coronary-artery vasoconstriction. N Engl J Med 1989; 321:1557. 34. Vitullo, JC, Karam, R, Mekhail, N, et al. Cocaine-induced small vessel spasm in isolated rat hearts. Am J Pathol 1989; 135:85. 35. Kalsner, S. Cocaine sensitization of coronary artery contractions: mechanism of drug-induced spasm. J Pharmacol Exp Ther 1993; 264:1132. 36. Wang, Y, Nunez, BD, Morgan, JP, Sellke FW. Cocaine and the porcine coronary microcirculation: effects of chronic cocaine and hypercholesterolemia. J Cardiothorac Vasc Anesth 1995; 9:290. 37. Havranek, EP, Nademanee, K, Grayburn, PA, Eichhorn, EJ. Endothelium-dependent vasorelaxation is impaired in cocaine arteriopathy. J Am Coll Cardiol 1996; 28:1168. 38. Togna, G, Tempesta, E, Togna, AR, et al. Platelet responsiveness and biosynthesis of thromboxane and prostacyclin in response to in vitro cocaine treatment. Haemostasis 1985; 15:100. 39. Kugelmass, AD, Shannon, RP, Yeo, EL, Ware, JA. Intravenous cocaine induces platelet activation in the conscious dog. Circulation 1995; 91:1336. 40. Heesch, CM, Withelm, CR, Ristich, J, et al. Cocaine activates platelets and increases the formation of circulating platelet containing microaggregates in humans. Heart 2000; 83:688. 17. Satran, A, Bart, BA, Henry, CR, et al. Increased prevalence of coronary artery aneurysms among cocaine users. Circulation 2005; 111:2424. 42. Kloner, RA, Hale, S, Alker, K, Rezkalla, S. The effects of acute and chronic cocaine use of the heart. Circulation 1992; 85:407. 43. Peng, SK, French, WJ, Pelikan, PC. Direct cocaine cardiotoxicity demonstrated by endomyocardial biopsy. Arch Pathol Lab Med 1989; 113:842. 44. Virmani, R, Robinowitz, M, Smialek, JE, Smyth, DF. Cardiovascular effects of cocaine: an autopsy study of 40 patients. Am Heart J 1988; 115:1068. 45. Isner, JM, Chokshi, SK. Cardiovascular complications of cocaine. Curr Probl Cardiol 1991; 16:89. 46. Wiener, RS, Lockhart, JT, Schwartz, RG. Dilated cardiomyopathy and cocaine abuse. report of two cases. Am J Med 1986; 81:699. 47. Willens, HJ, Chakko, SC, Kessler, KM. Cardiovascular manifestations of cocaine abuse. A case of recurrent dilated cardiomyopathy. Chest 1994; 106:594. 48. Henzlova, MJ, Smith, SH, Prchal, VM, Helmcke, FR. Apparent reversibility of cocaineinduced congestive cardiomyopathy. Am Heart J 1991; 122:577. 49. Om, A, Ellahham, S, Ornato, JP. Reversibility of cocaine-induced cardiomyopathy. Am Heart J 1992; 124:1639. 50. Chokshi, SK, Moore, R, Pandian, NG, Isner, JM. Reversible cardiomyopathy associated with cocaine intoxication. Ann Intern Med 1989; 111:1039. 51. Bauman, JL, Grawe, JJ, Winecoff, AP, Hariman, RJ. Cocaine-related sudden cardiac death: a hypothesis correlating basic science and clinical observations. J Clin Pharmacol 1994; 34:902. 52. Om, A, Ellenbogen, KA, Vetrovec, GW. Cocaine-induced bradyarrhythmias. Am Heart J 1992; 124:232. 53. Schrem, SS, Belsky, P, Schwartzman, D, Slater, W. Cocaine-induced torsades de pointes in a patient with the idiopathic long QT syndrome. Am Heart J 1990; 120:980. 54. Nanji, AA, Filipenko, JD. Asystole and ventricular fibrillation associated with cocaine intoxication. Chest 1984; 85:132. 55. Littmann, L, Monroe, MH, Svenson, RH. Brugada-type electrocardiographic pattern induced by cocaine. Mayo Clin Proc 2000; 75:845. 56. Magnano, AR, Talathoti, NB, Hallur, R, et al. Effect of acute cocaine administration on the QTc interval of habitual users. Am J Cardiol 2006; 97:1244. 57. Tisdale, JE, Shimoyama, H, Sabbah, HN, Webb, CR. The effect of cocaine on Ventricular fibrillation threshold in the normal canine heart. Pharmacotherapy 1996; 16:429. 58. Petitti, DB, Sidney, S, Quesenberry, C, Bernstein, A. Stroke and cocaine or amphetamine use. Epidemiology 1998; 9:596. 59. Klonoff, DC, Andrews, BT, Obana, WG. Stroke associated with cocaine use. Arch Neurol 1989; 46:989. 60. Kaufman, MJ, Levin, JM, Maas, LC, et al. Cocaine decreases relative cerebral blood volume in humans: a dynamic susceptibility contrast magnetic resonance imaging study. Psychopharmacology (Berl) 1998; 138:76. 61. Johnson, B, Lamki, L, Fang, B, et al. Demonstration of dose-dependent global and regional cocaine-induced reductions in brain blood flow using a novel approach to quantitative single photon emission computerized tomography. Neuropsychopharmacology 1998; 18:377. 62. Konzen, JP, Levine, SR, Garcia, JH. Vasospasm and thrombus formation as possible mechanisms of stroke related to alkaloidal cocaine. Stroke 1995; 26:1114. 63. Martinez, N, Diez-Tejedor, E, Frank, A. Vasospasm/thrombus in cerebral ischemia related to cocaine abuse. Stroke 1996; 27:147. 64. Robinson, JE, Heaton, RK, O'Malley, SS. Neuropsychological functioning in cocaine 41. abusers with and without alcohol dependence. J Int Neuropsychol Soc 1999; 5:10. Johnson, BA, Devous MD, Sr, Ruiz, P, Ait-Daoud, N. Treatment advances for cocaine-induced ischemic stroke: focus on dihydropyridine-class calcium channel antagonists. Am J Psychiatry 2001; 158:1191. 66. Hsue, PY, Salinas, CL, Bolger, AF, et al. Acute aortic dissection related to crack cocaine. Circulation 2002; 105:1592. 67. Chao, CR. Cardiovascular effects of cocaine during pregnancy. Semin Perinatol 1996; 20:107. 68. Foltin, RW, Fischman, MW, Levin, FR. Cardiovascular effects of cocaine in humans: laboratory studies. Drug Alcohol Depend 1995; 37:193. 69. Cami, J, Farre, M, Gonzalez, ML, et al. Cocaine metabolism in humans after use of alcohol. Clinical and research implications. Recent Dev Alcohol 1998; 14:437. 70. Braunwald, E, Antman, E, Beasley, J, et al. ACC/AHA 2002 guideline update for the management of patients with unstable angina and non-ST-segment elevation myocardial infarction-summary article. A report of the American College of Cardiology/American Heart Association task force on practice guidelines (Committee on the Management of Patients With Unstable Angina). J Am Coll Cardiol 2002; 40:1366. 71. McLaurin, M, Apple, FS, Henry, TD, Sharkey, SW. Cardiac troponin I and T concentrations in patients with cocaine-associated chest pain. Ann Clin Biochem 1996; 33:183. 72. Hollander, JE, Levitt, MA, Young, GP, et al. Effect of recent cocaine use on the specificity of cardiac markers for diagnosis of acute myocardial infarction. Am Heart J 1998; 135:245. 73. Kloner, RA, Hale, S. Unraveling the complex effects of cocaine on the heart. Circulation 1993; 87:1046. 74. Hollander, JE, Burstein, JL, Hoffman, RS, et al. Cocaine-associated myocardial infarction. Clinical safety of thrombolytic therapy. Cocaine Associated Myocardial Infarction (CAMI) Study Group. Chest 1995; 107:1237. 75. Hollander, JE, Hoffman, RS, Burstein, JL, et al. Cocaine-associated myocardial infarction. Mortality and complications. Cocaine-Associated Myocardial Infarction Study Group. Arch Intern Med 1995; 155:1081. 76. Hollander, JE, Hoffman, RS, Gennis, P, et al. Cocaine-associated chest pain: oneyear follow-up. Acad Emerg Med 1995; 2:179. 77. Weber, JE, Shofer, FS, Larkin, GL, et al. Validation of a brief observation period for patients with cocaine-associated chest pain. N Engl J Med 2003; 348:510. 65. GRAPHICS Risk of MI with cocaine ACC AHA chest pain cocaine