Clinical Electives Application for International Medical Students
advertisement
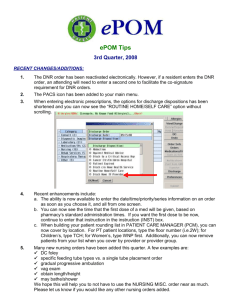
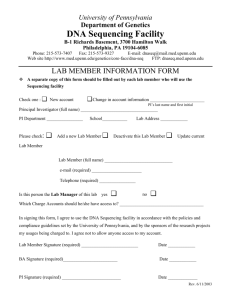
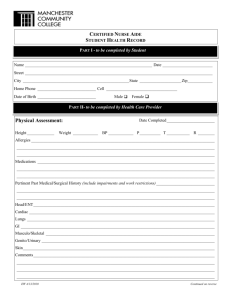
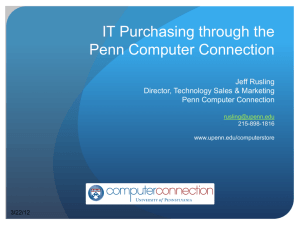
CENTER FOR GLOBAL HEALTH VISITING STUDENTS FROM INTERNATIONAL MEDICAL SCHOOLS APPLICATION FOR CLINICAL ELECTIVES 1. Date of Application (month/day/year) Personal Information 2. Last Name (Family/Surname) 3. First Name 4. Home Address (street, city, state, postal code, country) 5. Home Phone Number 6. Email Address(es) 7. Emergency Contact ( Male Female) (Name, Relationship, Phone Number) 8. Date & Place of Birth 9. Citizenship 10. First Language 11. English Skill (fluent; good; fair) 12. TOEFL Score (enclose official score report) (month/day/year) [Required for schools where English is not teaching language; minimum acceptable TOEFL scores are 250 (for computer-based test) and 600 (for paper-based test). For TOEFL® iBT, minimum scores are: 24 (Speaking) + 24 (Listening) + 20 (Reading) + 20 Writing. ] 13. Your Medical School Name/Location 14. Degree you will Earn (e.g. MD or MD/PhD) 15. Expected Graduation Date 16. Date to Begin* Clinical Elective(s) @ Penn (month/day/year) (month/day/year) (elective must start and end on elective dates indicated on our website: http://www.med.upenn.edu/globalhealth/intl_students.shtml) 17. # of Months to Spend @ Penn (two month maximum) 1 month 2 months Processing Your Application This application must be sent to the Center for Global Health by official representative of your home medical school. The following must be included in your application: page 1: personal information proof of personal health insurance that will cover student page 2: elective selection and student attestation while in the USA page 3: medical school official certification proof of $2050 per month to cover living expenses while page 4: immunization record (in English) student is in the USA official copy of student transcript (in English) photocopy of passport identification page copy of TOEFL score report (not required if English is the teaching language of the home medical school) Be sure to review “Preparing for Travel” and “Welcome to Philadelphia” information on CGH website, as early as possible: http://www.med.upenn.edu/globalhealth/intl_students.shtml *If you do not qualify for a visa waiver please allow 3-6 months to arrange visa 1 of 4 Perelman School of Medicine/ Center for Global Health / globhlth@mail.med.upenn.edu 09 08 15 CENTER FOR GLOBAL HEALTH VISITING STUDENTS FROM INTERNATIONAL MEDICAL SCHOOLS APPLICATION FOR CLINICAL ELECTIVES Clinical Electives Ranking Please note your clinical electives preferences by ranking every course that would be acceptable to you. The more courses you rank, the more likely you are to be placed. The courses listed are typically available; however, they are not guaranteed and it is possible that there will be no spots available for you in any of the courses you rank. Rank “1” for the elective most desired; rank higher #s for less desirable, but acceptable; do not rank unacceptable electives). You are obliged to start and end your elective at Penn on the specific dates posted on our website: http://www.med.upenn.edu/globalhealth/intl_students.shtml. No exceptions to this policy will be made. Fill in the dates in the section below the ranking table. Elective Course ANE300 Elective Course Rank Elective Course Rank ORT330 Ortho Extremity Reconstr PSY303 Child/Adoles/Famly Psych Pain Medicine OTO302 Otorhinolaryng Prim Care PSY311A PAT301 RAD320 Vasc/Interventl Radiology ANE303 GEN303/303A Rank Anesthesiology Medical Genetics MED314D PED302A Neonatology PED302D Neonatal ICU SUR300D General Surgery MED324A/D Hematology/Oncology PED305D Well Newborn SUR312A Cardiac Surgery MED334A/D/E Gastroenterology PED314 Pediatric Cardiology Nephrology PED323 Pediatric Oncology SUR318 Vascular Surgery Infectious Diseases PED324 Pediatric Hematology SUR341 Transplant Surgery MED343D/E MED354A RON300 Consult Psychiatry Cardiac Electrophysio MED316A Cardiology Clinical Pathology Radiation Oncology SUR314 Congenital Cardiac Surg MED364A/D/E Pulmonary Disease PED334 Pediatric Gastro-Intestinal SUR345A MED365 Cystic Fibrosis PED344 Pediatric Nephrology SUR346 Pediatric Urology MED384A Rheumatology PED354 Pediatric Infectious Disea SUR362 Plastic Surgery MED394A/D Endocrinology PED367 Pediatric Pulmonology SUR363 Pediatric Plastic Surgery Critical Care PED394 Pediatric Endocrinology SUR364 Plastic/Reconstrc Surgery MED410D NSG300 Neurosurgery* PMR300 Rehabiliation/Musculoske ORT304 Pediatric Orthopedics PMR301 ORT306 Sports Medicine PSY300 SUR365 Urology Surgery Trauma Pediatric Rehabilitation Inpatient Psychiatry * for Neurosurgery, CV and letter of recommendation must be submitted as part of this application Core Clerkships Must be Completed Before Arriving @ Penn – Please fill in details below Core Clerkship Duration (# of weeks) Date Completed Grade Medicine Obstetrics/Gynecology Pediatrics Psychiatry Surgery Student Attestation – Please check each item and sign at the end of this section The information I have provided in my application form and all attachments is accurate. If I am accepted and enrolled at Penn, I understand that I remain a student in my home school and that the ultimate responsibility for patient care resides with the University of Pennsylvania Perelman School of Medicine (hereafter referred to as PSOM) and its staff will respect the confidential nature of all medical records and personally identifiable information related to patients will act prudently within the limits of my knowledge, experience, and training; follow policies related to procedures and etiquette; and wear attire acceptable to the PSOM shall respect all property belonging to the PSOM and its affiliated institutions and I understand that I will be responsible for the repair or replacement of any property damaged or destroyed by me will be responsible for my own housing and transportation to and from the PSOM understand that if I am unable to attend scheduled activities, I must notify the PSOM and my home school certify that I have no preexisting conditions that would preclude or adversely affect me from being in any clinical areas or participating in the Program. I am not aware that I have any infectious disease. Signature________________________________________________________ Date___________________________ Be sure to review “Preparing for Travel” and “Welcome to Philadelphia” information on CGH website, as early as possible: http://www.med.upenn.edu/globalhealth/intl_students.shtml *If you do not qualify for a visa waiver please allow 3-6 months to arrange visa 2 of 4 Perelman School of Medicine/ Center for Global Health / globhlth@mail.med.upenn.edu 09 08 15 CENTER FOR GLOBAL HEALTH VISITING STUDENTS FROM INTERNATIONAL MEDICAL SCHOOLS APPLICATION FOR CLINICAL ELECTIVES International Medical School Official Certification For Completion by Dean/Designated Official of Student’s Home Medical School STUDENT: Last Name : First Name: This is to certify that the medical student named above is in good standing at this institution, that the information provided on pages 1 and 2 of this application is correct, and that the student does have our permission to enroll for clinical electives at the University of Pennsylvania Perelman School of Medicine. The student has completed all required core clerkships (as noted on page 2). The student is covered by personal health insurance (attach proof) which covers the student while away from our school and in the United States. In addition, the signature below serves to certify that we have no record of this student’s ever having engaged in criminal activity of any kind. Important: Within a few weeks of the clinical elective end date, course directors submit evaluations via OASIS, an online system. The Registrar’s Office notifies students by email when the student can access the evaluation online. It is the student’s responsibility to forward the evaluation to their home institution, if required. URL to view sample evaluation: http://www.med.upenn.edu/globalhealth/documents/MedicalStudentSampleEvaluation.pdf Additional forms requested by student or student’s home school cannot be completed, signed, or sealed. MEDICAL SCHOOL OFFICIAL: Last Name : First Name: Official Title: Email Address: Medical School Name: Location: (city/country) Is instruction at your medical school in English? Yes No (if English is not the principal language of instruction, student’s TOEFL exam results must be provided) Signature of Medical School Official Date Application Submission Complete application must be sent to the Center for Global Health by the official representative of the home medical school. The application must include: page 1: personal information page 2: elective selection and student attestation page 3: medical school official certification page 4: immunization record (in English) official copy of student transcript (in English) copy of TOEFL score report (not required if English is the teaching language of the home medical school) proof of personal health insurance that will cover student while in the USA proof of $2050 per month to cover living expenses while student is in the USA photocopy of passport identification page Scan complete application to send as email attachment to: globhlth@mail.med.upenn.edu or mail hard copy to: Center for Global Health / U of Penn Perelman School of Medicine / 240 John Morgan Bldg. / 3620 Hamilton Walk / Phila, PA 19104-4882 Be sure to review “Preparing for Travel” and “Welcome to Philadelphia” information on CGH website, as early as possible: http://www.med.upenn.edu/globalhealth/intl_students.shtml *If you do not qualify for a visa waiver please allow 3-6 months to arrange visa 3 of 4 Perelman School of Medicine/ Center for Global Health / globhlth@mail.med.upenn.edu 09 08 15 GLOBAL HEALTH PROGRAMS VISITING STUDENTS FROM INTERNATIONAL MEDICAL SCHOOLS IMMUNIZATION RECORD APPLICANT NAME: Last First BIRTHDATE The University of Pennsylvania Perelman School of Medicine (Penn) requires all of the information listed below for a student to be considered for placement. *Quantitative results require lab reports indicating titer and reference range. This form must be completed, signed and dated by a health care provider. Applicants should be free from symptoms of infectious disease upon arrival. Applicant: If you become ill with a communicable disease while at Penn, you must notify the Center for Global Health and your course director/mentor. MEASLES, MUMPS, RUBELLA (MMR) Two doses of MMR are required (1st dose must be administered after the 1st birthday and 2nd dose a minimum of 4 weeks later). who have not had MMR as specified may satisfy this requirement with the alternate regimen listed below OR positive titers Students MMR Dose 1 ____/____/____ Dose 2 ____/____/____ Alternative regimen OR positive *titer verifying immunity MEASLES Dose 1 ____/____/____ Dose 2 ____/____/____ OR *Titer quantity _________ Lab report attached MUMPS Dose 1 ____/____/____ OR *Titer quantity _________ Lab report attached RUBELLA Dose 1 _____/____/____ OR *Titer quantity _________ Lab report attached HEPATITIS B Requirement: Three doses (doses one and two given four weeks apart, and the third dose at least 4 to 6 months after the first dose) AND a blood test showing *titer quantity/quantitative result (lab report, indicating titer and reference range required). Dose 1 ____/____/____ Dose 2 ____/____/____ Dose 3 ____/____/____ AND *Titer quantity _________ Lab report attached ______________________________________________________________________________________________________________ VARICELLA (Chicken Pox) Requirement: Two doses of chicken pox vaccine are required at least one month apart (must be administered after 1995) OR positive *titer verifying immunity (for positive titers, lab report including reference range, is required). Dose 1 ____/____/____ Dose 2 ____/____/____ OR *Titer quantity _________ Lab report attached _______________________________________________________________________________________________________________ TETANUS-DIPHTHERIA and PERTUSSIS (Tdap) Requirement: One dose administered in 2005 or later. Dose 1 ____/____/____ ________________________________________________________________________________________________________________ POLIO Requirement: Student must have completed primary series of polio immunizations – note below date series was completed. Oral Polio Vaccine (OPV) ____/____/____ OR Enhanced Inactivated Polio Vaccine (E-IPV) ____/____/____ ________________________________________________________________________________________________________________ TTBI (Test of Tuberculosis Infection) Requirement: Two PPDs OR one QuantiFERON/IGRA, all within 12 months of the requested elective start date (regardless of prior vaccination with BCG). Any student with a positive TTBI must include with this application reports of the positive reaction, subsequent chest x-ray, and a TB symptom check done within 12 months of the elective start date. Dates and results of last two PPD tests: ____/____/____ Negative Date and result of QuantiFERON/IGRA blood test for TB infection Positive ____/____/____ ____/____/____ Negative Negative Positive OR Positive **Reminders** 1) Both PPDs must be done 1 year or less before the elective start date. 2) TTBI (PPD or QuantiFERON/IGRA) positive? If yes, check box and attach radiology report: INFLUENZA Requirement: Students must have current influenza vaccine(s) if they will be at Penn anytime in October through March. Please note that if you received your flu vaccine in a country in the southern hemisphere we may require re-vaccination. Flu Vaccine Date ____/____/____ Health Care Provider Print Name_____________________________________________________________ Phone #______________________________ Signature_______________________________________________________________ Date_________________________________ Address________________________________________________________________________________________________________ Be sure to review “Preparing for Travel” and “Welcome to Philadelphia” information on CGH website, as early as possible: http://www.med.upenn.edu/globalhealth/intl_students.shtml *If you do not qualify for a visa waiver please allow 3-6 months to arrange visa 4 of 4 Perelman School of Medicine/ Center for Global Health / globhlth@mail.med.upenn.edu 09 08 15
 0
0
advertisement



Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users