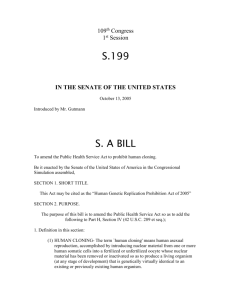
A Cross-Cultural Introduction to Bioethics 192 E1. Lifestyle and Fertility Chapter objectives. Some students are just considering about their fertility and others will not yet be considering whether to have children. Our lifestyle now affects our future health and fertility. There are some lifestyle choices everyone can make. This chapter aims to: 1. Consider the influences of lifestyle, environment and social development on personal empowerment and reproductive health. 2. Discuss the divide between fertility and infertility, and common causes of infertility. E1.1. Reproduction and Fertility The capability to bear healthy children depends on our genes, the conditions under which we live and the ways in which we behave. Many environmental and behavioral factors, including nutrition, exercise, poverty and drug abuse, contribute to ill health and poor fertility. Therefore fertility may be a good indicator of an individual’s overall health status in certain circumstances. About 15% of couples in developed countries are involuntarily infertile, with a much higher percentage in developing countries (30-40% of women in parts of tropical Africa). The main causes of infertility in developing countries are sexually transmitted diseases (principally gonorrhea and chlamydia) and repeated pregnancies coupled with poor hygiene at the time of childbirth, abortion or miscarriage causing secondary infertility. Pregnancy is the best way to judge a couple’s fertility. A couple is considered infertile if no conception has been achieved after 12 months or more of unprotected sex of average frequency. Fertility problems are equally likely to be caused by a disorder on the man’s side or on the woman’s side. Occasionally there is a problem on both sides, and in about 25% of cases the cause cannot be identified. Unexplained infertility characterizes childless couples where a thorough examination of both partners fails to reveal a specific cause of infertility. By their mid-thirties about one in four couples is infertile. The decline in fertility has several causes including more frequent failure of ovulation, decreasing sperm counts and sperm quality, and an increased likelihood of spontaneous abortion early in pregnancy. A woman’s menstrual cycles may become irregular in her early or mid-forties. This is the onset of the climacteric - the period of transition from fertility to infertility – and may last as long as 10 years. The final termination of menstrual cycles, or menopause, occurs at an average age of 50-52. A healthy postmenopausal woman can become pregnant with the aid of reproductive technology; donated oocytes can be fertilized in vitro and the embryo transferred to her womb or uterus. The pregnancy must be supported with hormone treatments. . Collaborating author: Irina Pollard, Australia © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> A Cross-Cultural Introduction to Bioethics 193 Q1. Do you want to have children? How many? E1.2 Fertility Declines with Age Female infertility is normally age dependent and increases from 30 years of age to the menopause; while age-related rise in male infertility is more gradual. Children who are born to older parents, especially older mothers, also stand a greater risk of having chromosomal abnormalities. One of these is Downs’s syndrome, caused by an extra copy of chromosome 21. Chromosomal abnormalities increase with maternal age because the mother’s oocytes, or eggs, remain ‘frozen’ in their first meiotic division from early in her fetal life. Increasing paternal age also raises the chances that a child will have certain medical problems. Genetic anomalies in a man’s sperm also increase over his lifetime because the sperm precursor cell stocks (immature spermatogonia) are constantly dividing to produce new sperm. Thus, an older man’s sperm are the product of a greater total number of cell divisions, and each round of DNA replication carries a chance of introducing a harmful mutation. Of pregnancies that proceed far enough to be detected clinically, about 15-20% are subsequently lost by spontaneous abortion or miscarriage, usually during the first three months or trimester. The majority of all spontaneously aborted embryos and fetuses have chromosomal abnormalities. This contrasts markedly with a 5% chromosome abnormality rate found in stillbirths, clearly illustrating the natural in utero selection processes that eliminate 95% of chromosomal damaged conceptions. 50 - 60% Unknown Etiology 20 - 25% Multifactorial Inheritance 7 - 10% Environmental Agents 7 - 8% Mutant Genes Figure 1: Causes of Human Congenital Abnormalities at Birth 6 - 7% Chromosomal Abnormalities E1.3 Many Conceptuses Do Not Survive More than half of all human conceptuses are genetically abnormal and have little or no chance of giving rise to a baby. It is generally recognized that human fecundity rate (= the probability of achieving a clinical recognized pregnancy within any given menstrual cycle) is about 25% and high levels of fertilization failures or early developmental death, are the norm at conception. Most abnormal conceptuses are lost at very early stages, failing to implant or © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> A Cross-Cultural Introduction to Bioethics 194 implanting so briefly before they die so that menstruation proceeds regularly and the mother is never aware of their existence. In some cases, environmental factors such as alcohol consumption, general anesthesia, or X-ray exposure around the time of ovulation or fertilization may trigger chromosomal abnormalities. Spontaneous abortion is one of nature’s way to counter negative environmental factors. The causes of most human congenital anomalies at birth are unknown because the majority of common disorders, such as heart disease, diabetes and cancer, are caused by a combination of genetic and environmental factors. If there are many factors we say that the cause is multifactorial in origin (Figure 1). Reproductive health depends upon the smooth succession of physical, physiological, behavioral, intellectual, emotional and spiritual change through which each individual passes from conception to death. Q2. Can you think of anything you do now which might affect your fertility? Q3. Make a list of factors which people think affect your fertility in positive and negative ways. Q4. Do you think that everyone has a right to have a child? E1.4. Maximizing Health and Fertility This section describes some of the factors that affect fertility. Think about what you can do. (i) Nutrition and Reproduction Food restriction and abnormal eating behavior (as in obesity and anorexia nervosa) lower normal fertility levels. Good nutrition is also vital during pregnancy. Underweight women risk producing an underweight child who will be more likely to suffer a variety of medical problems. Being either underweight or overweight increases the likelihood of premature birth, which is bad for both mother and baby. Besides enough calories, a pregnant woman needs to consume adequate amounts of other nutrients, especially protein, calcium, iron, vitamin A and folic acid (folate). Women who are overweight face an additional increased risk of certain serious disorders during pregnancy including diabetes and hypertension. Under normal conditions the fetus is adept at taking these nutrients from its mother and does not usually suffer any deficiency, but the mother may do so. © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> A Cross-Cultural Introduction to Bioethics 195 (ii) Exercise and Reproduction There is a positive correlation between exercise, improved fitness and enhanced sexuality and bearing a healthy child. Traditionally, pregnant women were thought of as fragile creatures who needed to avoid exercise. It’s now clear that, except in the case of certain problem pregnancies, exercise has a positive value in maintaining the woman’s health and sense of wellbeing. Therefore pregnant women should engage in moderate, low-impact forms of exercise, such as brisk walking and swimming, but should avoid exercises that significantly raise the body temperature. That’s because high maternal temperatures may increase the likelihood of fetal abnormalities and may also cause dehydration, which can overstress the mother and her fetus. As well as consuming the right foods and maintaining physical fitness, a couple wishing to make a baby has to avoid a number of agents that can harm the fetus. Alcohol and tobacco heads this list. Fetal Alcohol Syndrome (FAS) has a specific cluster of symptoms. It is not clear whether moderate drinking, like one or two drinks per day, is harmful but several studies have reported that two drinks a day does have ill effects, including reduced intelligence, on genetically vulnerable fetuses. The average IQ of the FAS children is about 70 with the severity of intellectual disability being related to the degree of alcohol exposure in utero. (iii) Substance Abuse and Reproduction Heavy alcohol consumption during fertilization and pregnancy increases the likelihood of birth defects and infant death. Drinking whilst pregnant is also associated with Fetal Alcohol Syndrome (FAS). FAS children have characteristic facial appearance and other physical anomalies, are intellectually disabled and may have behavioral problems such as attention-deficit hyperactivity disorder (ADHD). Since no safe level of alcohol intake has been established, women should abstain completely from drinking whilst attempting to conceive as well as during pregnancy. One of the most harmful practices a couple can engage in whilst planning to become pregnant and during pregnancy is smoking. It is testimony to the addictive power of tobacco that, even though its ill effects on fetal health are widely known, only about 20% of female smokers in the US actually quit during pregnancy. Smoking by either the father or mother increases the likelihood of spontaneous abortion, premature birth, low birth weight, congenital malformations and childhood cancer. Smoking's ill effects continue after a child is born where 25-40% of all cases of sudden infant death syndrome can be attributed to the mother’s smoking during pregnancy, and babies whose mothers smoke during pregnancy have a 59% higher chance of dying during infancy than those born to nonsmokers. Fetal exposure to addictive drugs such as cocaine, heroin and nicotine cause the baby to be born in an addicted state, as well as having the other harmful effects listed above. Lifestyle of both mother and father influences the health of the reproductive cells (sperm and eggs or gametes) and the baby. Drugs such as nicotine, alcohol, certain recreational drugs and narcotics including marijuana, cocaine, heroin and amphetamines, transmit their effects by increasing the frequency of abnormal sperm, and reducing sperm number, motility and fertilization ability. Self-induced infertility in fathers is a major concern not least because it increases the demand for assisted reproductive technology and associated risks. Q5. Do alcohol and tobacco have warnings for pregnancy written on them? What do the warnings say? Do you think people should smoke? © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> 196 A Cross-Cultural Introduction to Bioethics (iv) Other causes of male infertility and the environment There are many possible causes for insufficient or defective sperm. Overheating of the testes by prolonged strenuous exercise or wearing too-tight clothing can also cause a transient reduction in sperm count. More serious, however, are chemical and physical toxins introduced into the environment by human activity that may affect fertility rates in all animals including humans. The average sperm counts in a number of Western societies have dropped by nearly one-half (from 113 to 66 million sperm per milliliter of semen) between 1940 and 1990. During this period the prevalence of certain male reproductive disorders such as undescended testicles (called cryptorchidism) and testicular cancer, have significantly increased. Endocrine disruptors disturb sex hormone function regulating adult fertility by mimicking or antagonizing sex hormone activity. These hormone disruptors include agricultural pesticides and a variety of industrial chemicals such as the polychlorinated biphenyls (PCBs). Agricultural workers experience a decline in their sperm number proportional to the degree of pesticide exposure. Whether endocrine disruptors are also responsible for the observed sperm decline in the general population is not clear. However, if this steady decline continues then male fertility would be severely reduced within a few generations. Undescended testicles, sex chromosome anomalies, infections that cause blockage of the reproductive tract and chemotherapy can all cause irreversible reduction or failure of spermatogenesis. Environmental toxins that contribute to reducing male fertility are made more severe in individuals with pre-existing genetic or behavioral risk factors. There are many environmental concerns that may be explored in this context just one is given because it provides a good example illustrating the interconnectedness of all biological systems. Many factors may contribute to falling sperm counts and associated anomalies but most attention has been focused on a specific class of environmental pollutants. © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> A Cross-Cultural Introduction to Bioethics 197 (v) Immunological Factors in Human Infertility Immunological factors in human infertility are now easily bypassed by in vitro fertilization techniques such as intracytoplasmic sperm injection or ICSI (see the chapter on assisted reproductive technology). However, immunological factors are important in the understanding of infertility treatments because the presence of anti-sperm antibodies in the serum of the female partner may explain persistent infertility and IVF failure. (vi) Poverty, Population and Development Today in the industrialized countries the prospects for pregnant women and their fetuses are far better than they were in the past. For example, in the USA 80% of all established pregnancies culminate in the delivery of a live child, and once a child is born it has 99.3% chance for surviving infancy. Further, less than one in 10,000 pregnancies now leads to the death of the mother. However, certain social/ethnic minority groups are significantly disadvantaged compared to the general population. Indigenous people in Australia and the United States, for example, experience various forms of difficulties simultaneously, including social discrimination, which can be recognized by the high level of low birth weight infants and excessive neonatal mortality. “Good health is a basic human right, especially among poor people afflicted with disease who are isolated, forgotten, ignored, and often without hope. Just to know that someone cares about them can not only ease their physical pain but also remove an element of alienation and anger that can lead to hatred and violence.” Former U.S. President Jimmy Carter http://www.cartercenter.org/healthprograms Too often indigenous people live on a lower average family income, have a lower level of education, suffer a greater level of unemployment and are relegated to unacceptable overcrowded housing and poor sanitation. As a result many of the persistent health problems relate to alcoholism, other drug dependencies and depression, which then becomes the legacy for the next and subsequent generations. The relationships among environment, poverty and social development are complex and varied; however in the spirit of reconciliation major inequities are increasingly being addressed and it is hoped that this lesson will accelerate the process. In general terms there is broad agreement that personal empowerment and reproductive health is part of an essential package of health care and education. Reproductive health includes ensuring that individuals and couples can make their own choices about family size, spacing of their children and have confidence in a healthy outcome. Q6. Does every child in your society have an equal chance to grow up healthy? © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> A Cross-Cultural Introduction to Bioethics 198 E2. Assisted Reproduction Chapter objectives. There are many ways that we use medicine to improve our health. Reproduction is also part of human health, and there are ways to assist persons who are infertile. More and more technologies are being developed which change the roles of different persons involved in reproduction, including genetic and social parents. This chapter aims to: 1. Describe some assisted reproductive technologies. 2. Highlight major bioethical concerns. 3. Consider which technologies each person may choose. Q1. Look at the names of assisted reproductive technologies (ART) in Box 1, and list the ones you have heard of before. In this chapter most but not all of these techniques will be introduced and discussed. Box 1: Major Assisted Reproductive Technologies (ART) Artificial insemination by donor or by husband (AID; AIH) In vitro fertilization and embryo transfer (IVF-ET) Direct intra-peritoneal insemination (DIPI) Gamete intra-fallopian transfer (GIFT) Zygote intra-fallopian transfer (ZIFT) Intracytoplasmic sperm injection (ICSI) Sperm collection by way of microsurgery Embryo and sperm cryopreservation and storage Cytoplasmic transfer Preimplantation genetic diagnosis (PGD) Karyotyping and genetic manipulation Tissue banking Ovulation induction Laparoscopy and hysteroscopy Laser laparoscopy Hystero-sonography Ultrasound scanning Egg and embryo donation; posthumous gamete donation Flow cytometry Surrogacy Cloning technology . Collaborating author: Irina Pollard, Australia © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> A Cross-Cultural Introduction to Bioethics 199 E2.1. Assisted Reproductive Technology (ART) Since the first 'test-tube baby' Louise Brown was born in Britain in 1978, more than a million children have been born through assisted reproductive technology (ART). The original IVF technology involved mixing eggs and sperm in a laboratory dish (in vitro fertilization or IVF) and then implanting the resulting embryos (embryo transfer or ET) into the womb or uterus. The technique was developed to help women with blocked fallopian tubes and apart from their blocked tubes there were no additional fertility problems. Since early studies suggested that the new technology was without additional risk to mother and baby, IVF soon became widely accepted and modified developments for the treatment of complex types of infertility became available. E2.2. Male-Factor Infertility In this section some factors that affect male fertility are discussed. (i) Standard Semen Parameters A variety of factors (parameters = a factor we can measure) can indicate poor quality semen that reduces male fertility. These are sperm count (number), sperm motility (movement), sperm morphology (shape) and sperm fertilizability (joining of sperm with the egg). Sperm counts are easy to perform, so it is often used to assess fertility. Sperm morphology is one of the best indicators of fertility; however, examination with the light microscope can provide only limited information on their internal structure. The most common group of conditions affecting fertility is characterized by insufficient or poor-quality sperm in the man’s semen (see the Chapter on infertility for lifestyle/social factors). The usual rule of thumb is that a man is likely to be subfertile if there are fewer than 20 million sperm per milliliter of semen or if the fraction of the sperm that has normal motility is less than 50%. Q2. Do you know where in your city there are frozen sperm collections? (ii) Artificial insemination If sperm numbers are too low, semen can be collected over a period of time and frozen. Then the entire collected amount can be placed in the woman’s vagina or directly into her uterus at a time coinciding with ovulation. Partner insemination is usually called artificial insemination by the husband (AIH). It has been also used in cases of forced separation of couples (e.g., prisoners on long-term sentences). The procedure can also be done proactively where men with normal sperm counts may store their own sperm in advance of medical procedures that could affect their fertility; such as chemotherapy, radiation treatment and surgery on the testes or reproductive tract including sterilization. If the male partner is completely sterile or the couple does not want to use his sperm as, for example, when he carries a gene for a serious genetic disease, women can use artificial insemination by donor or AID. Donor insemination (DI) is also employed for single women who want to become pregnant, or for women who are partnered by other women. © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> 200 A Cross-Cultural Introduction to Bioethics Internationally recognized insemination centers restrict donor recruitment to men who are healthy, free from transmissible genetic disorders and sexually-transmitted disease and have semen with a high fertilization potential. Information about potential donors’ physical appearance, profession and other interests is usually available to potential recipients. Donor insemination is more successful than partner insemination, does not carry an increased risk of spontaneous abortion or congenital anomalies, and has advantages over adoption in that the child is genetically related to the mother and the couple can experience conception, pregnancy and delivery. It is, therefore, one of the major treatments for male infertility (see also the section on ‘Sperm, Egg and Embryo Donation). Q3. Do you think there should be restrictions on who can use donor insemination? What sorts of restrictions? (iii) Intracytoplasmic sperm injection (ICSI) Intracytoplasmic sperm injection or ICSI, in conjunction with IVF technology, has given hope to men with severe infertility problems. This technique involves the injection, via a micropipette, of a single sperm directly into the cytoplasm of the oocyte (egg) and can be used for non-motile or otherwise damaged sperm. Even a man who produces no mature sperm at all may be able to father a child. Immature spermatids (sperm precursor cells) can be harvested by needle aspiration of the man’s testis and used to fertilize the egg. Soon after the development of the ICSI technology it became the standard treatment for severe male-factor infertility but there remain unanswered questions relating to unidentified risks in the children conceived by this procedure. Debate is also continuing as to its use when the male has normal semen parameters. In the presence of normal semen parameters, fertilization by ICSI does not show an advantage over conventional IVF treatment, however, some centers use ICSI for all cases of IVF in order to protect against the possibility of fertilization failure. © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> A Cross-Cultural Introduction to Bioethics 201 E2.3. Female-Factor Infertility About 20% of female infertility is caused by abnormalities of the reproductive tract with the commonest being abnormal fallopian tubes. They can become scarred, obstructed, or denuded of cilia as a consequence of pelvic inflammatory disease – a general term for infections of the uterus or oviducts, usually caused by sexually transmitted organisms such as chlamydia or gonorrhea. Another condition that can interfere with fertility is endometriosis, a condition where endometrial (uterine) tissue grows at unusual locations such as on the ovaries or oviducts. Although surgery can sometimes restore fertility in such conditions, it often fails to do so. In such cases it is possible to bypass the fallopian tubes by performing IVF and placing the resulting embryos directly into the uterus. Another 20% or so of infertility cases are caused by failure to ovulate. These conditions can be caused by a variety of physical and psychological stresses (see the Chapter on Fertility). Menstrual irregularity may be caused by, for example, excessive weight loss, strenuous athletic training, anxiety, grief, depression and certain drugs. Q4. Do you think the government should fund ways to help people have children if their infertility was the result of their unhealthy lifestyle during their younger days? E2.4. In Vitro Fertilization (IVF) Technology In vitro fertilization can circumvent many sperm problems. ‘In vitro’ means ‘in glass’ – short for in a petri dish. In the standard IVF procedure the woman is given hormones to promote the development of a batch of follicles on a precisely timed schedule. When the follicles are nearly ready to ovulate, a fine needle is passed into each one under ultrasound control, and the oocyte is flushed out. As many as twenty oocytes can be harvested in a single procedure. The collected oocytes are placed in a Petri dish, and the partner’s sperm are then added. Regardless of the exact IVF procedure used, the artificially fertilized oocytes – now embryos - are kept in tissue culture for several days, during which time they divide several times. It is possible at this stage to remove a cell or two from the conceptuses without harming them; the sex and genetic makeup of the removed cells can then be determined. This preimplantation genetic screening procedure is useful if one of the parents carries a disease-causing gene and the couple wants to ensure that their child does not inherit it (as discussed in section E2.5). One or two embryos are placed in the woman’s uterus at the same time in order to maximize the chances that at least one will implant. If several embryos are transferred and all implant, the woman may be offered the opportunity to have the number reduced by a fetal reduction abortion. This practice presents ethical problems. High-number or multiple pregnancies such as triplets or quadruplets are associated with all kinds of serious risks to the fetuses and to the mother. Serious outcomes are still births, birth defects and other disabilities, including intellectual, evident by the age of 2 years. A more common problem, however, is not multiple fetuses, but having no fetuses. About a quarter of the attempts achieve pregnancy and birth. The prospects are particularly poor for women over 40 years of age where only about 8% will achieve a successful pregnancy after a single IVF attempt. Q5. How many times would you try IVF in order to have a child? © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> A Cross-Cultural Introduction to Bioethics 202 E2.5. Preimplantation Genetic Diagnosis (PGD) The risk of genetic disorders is a major problem for many couples when thinking about pregnancy. Special tests can detect fetal abnormalities and congenital disorders. These tests include ultrasound scans, amniocentesis, chorionic villus sampling and preimplantation genetic diagnosis. These procedures can also be used to determine the fetus's sex. Preimplantation genetic diagnosis is now considered a valuable approach, which in combination with IVF techniques, enables the screening for genetic disorders before the corresponding embryo is transferred to the expectant mother. Reasons for preimplantation genetic diagnosis include: for carriers of single gene diseases such as cystic fibrosis that is especially frequent in infertile male populations; for carriers of thalassemias that are endemic in the Mediterranean area; for sex-linked diseases; to prevent the transfer of chromosomally abnormal embryos obtained from 'at risk' groups such as older women. E2.6. Sperm, Egg and Embryo Donation Please read the section on Artificial Insemination before this one. There may be surplus embryos generated during IVF treatment that are not transferred into the uterus. Before treatment begins, the couple is required to write their wish regarding the fate of surplus IVF embryos, should there be any. Spare embryos may be discarded, stored frozen for later use, donated to infertile couples or donated to research. If a woman's oocytes cannot be used, oocytes can also be obtained from donors. Obtaining oocytes from female donors is more complex and expensive than sperm donation because the donor must undergo hormone treatment followed by oocyte aspiration (see IVF section). There are certain risks for the donor, including the risk of injury or infection associated with the procedure itself, the risk of unwanted pregnancy (because the donor cannot use oral contraceptives during the period before the donation), the risk of psychological trauma, and a small chance of negative effect on future fertility. Still many women altruistically become donors. Reproductive technologies such as IVF and ICSI are increasingly used by couples experiencing infertility. In many countries they have become standard procedures and the number of children born with their help is increasing annually (even in Japan alone more than 11,000 IVF babies were born in the year 2000). Many parents feel unsure about how, if at all, to communicate the method of their child's conception with their child and significant others. Sharing of information is especially significant when donor material has been used since failure to do so denies the child access to its identifying heritage. Knowing one's origins © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> A Cross-Cultural Introduction to Bioethics 203 provides emotional security in terms of identity and belonging and in terms of medical history, as genetic knowledge is sometimes indispensable. It is for this reason that access issues are a major aspect of prenatal ART counseling services. By way of protecting children's best interests, parents are now expected to tell the truth about their conception at some point, preferably before they reach the age of consent. The importance of access to information applies equally whether the child is the result of adoption, donor gametes, donor embryos, some variant of surrogacy or just technological support. Q6. If you were born from donated eggs or sperm, or were an adopted baby, do you think your parents should tell you who your genetic parents are? E2.7. Summary The main difficulty in evaluating new technology for effectiveness is that we have no good way of seeing how they all work together with each other. It would be wrong to look upon assisted reproduction as the panacea for all causes of childlessness. Instead the technologies are assessed one by one, as if they exist in isolation when what is needed is to assess the impact of ART innovation as a whole. Thus, when forced to choose among several ART possibilities, the logical clinical protocol is to integrate the best available evidence from the literature with clinical expertise and tailor it to the individual situation. Certainly there is also the responsibility for researchers to assess the risks posed by assisted reproduction. This requires epidemiological follow-up studies to determine whether the ART created children bear any cellular or molecular abnormalities beyond the expected in the population at large. Some recent studies have started to raise doubts about the safety of IVF, but for most children born they are merely grateful for the means for their creation. For the sake of future generations of assisted reproduction children, research on human embryos should be encouraged. Finally, taking into consideration new scientific insights, we may be able to retain what is biologically relevant and adaptive, and modify what is not. © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> A Cross-Cultural Introduction to Bioethics 204 E3. Surrogacy Surrogacy is when someone does something in place of another person. Some women get pregnant for another woman. Gay male couples who wish to have children may also ask a surrogate mother since they cannot get pregnant. In genetic or partial surrogacy the surrogate mother agrees to be artificially inseminated using the sperm from the partner of the woman, and she then carries any resulting fetus or fetuses to term. If the woman who cannot sustain a pregnancy can nevertheless produce healthy oocytes, those oocytes can be fertilized with the partner’s sperm by IVF and then implanted into the surrogate’s uterus. This procedure is called gestational or total surrogacy. Either way, when the child is born, the surrogate gives it up for adoption by the couple. Modern surrogacy challenges traditional assumptions about parenthood because assisted reproduction procedures make it possible to separate out the various phases of the reproductive process. It is now possible for a child to be subject to multiple parenting with two men (genetic and adoptee) fulfilling the functions of ‘father’ and up to three women (genetic, gestational and adoptee) fulfilling the differing functions of ‘mother’. The birth of such children also holds wider kin implications for grandparents or other relatives. Q1. Do you think surrogate mothers should be paid? Q2. Would you consider being a surrogate mother as a part-time job? Q3. In some countries only married women who already have children are allowed to be surrogates. Why do you think that law was made? © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> A Cross-Cultural Introduction to Bioethics 205 E4. Choosing Your Children’s Sex and Designer Children Chapter objectives. There is a long history of discrimination against females in many cultures. In some cultures there is a lower number of females compared to males that indicates there is sex selection against females. This chapter aims to: 1. Describe sex selection. 2. Discuss some of the ethical issues associated with its practice. 3. Consider the question of designer children. E4.1. Sex Selection Some people would prefer their child to be of one particular sex. Sometimes their preference has specific medical reasons; for example, in instances of sex-linked genetic disorders the couple may want a child of the other sex. This usually means a girl, because most sex-linked disorders affect boys. Another reason why couples would prefer a child of a particular sex is for specific social or even religious reasons. The presence of both the sex chromosomes, X and Y, generally results in the birth of a male child while the presence of two X chromosomes leads to the birth of a female. A sperm can either carry the X or the Y chromosome along with the halved number of other chromosomes (22), the autosomes, which do not play a very important role in sex determination. The ova are of the same type with 22 autosomes and one X chromosome. This XX-XY sex determination mechanism in nature presents an equal chance of conceiving a female or a male child. Box 1: Some Definitions Sex selection: To prefer to continue/terminate a pregnancy as per the desired sex of the unborn child. Sex determination: The endeavour to know the sex of the unborn child for medical/genetic reasons or for sex selection. Family spacing: To terminate a pregnancy in case there are already very young children in the family. Family planning: To terminate a pregnancy in case the child is not wanted by the couple. Sex ratio: The number of females per thousand males. Embryo: (Greek word meaning – to swell) term given to a human conceptus from conception until 8 weeks gestation. Fetus: (Latin word meaning – little one, young one or offspring) term given to the human conceptus from 8 weeks gestation until birth. . Collaborating authors: Gursatej Gandhi, India and Irina Pollard, Australia © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> A Cross-Cultural Introduction to Bioethics 206 Q1. Would you like to have a girl or a boy? If you already had 3 boys would you like to have the next child be a girl? E4.2. Pregnancy Termination Abortion or the deliberate termination of termination is a medical procedure in which a fetus is not allowed to develop fully to term but is forced out of the mother’s womb. The process can be unsafe for the mother and can cause complications and even her death, especially in countries where access to experienced and safe medical clinics is restricted for economic or legal reasons. There are rarely grave medical conditions in which such a procedure is the only means to safeguard the health of the mother. Many a times however, the simplicity of the procedure and the failure in upholding the life of the unborn has led to its misuse in various regions. Ultrasonography (the use of sound waves to form an image visible on a monitor) and a number of medical genetic techniques have made it easier to identify the sex of a child prenatally (before birth) thereby facilitating its use for sex selection, sex determination, family spacing and family planning (See Box 1). The issue of abortion raises a number of issues pertaining to the ethical (right and wrong actions), social and legal implications. It has become a matter for even greater societal concern in the wake of the falling sex ratios, i.e. the birth of unequal number of girls and boys, which are seen in some states in India, Korea and China. There are laws against abortion for reasons of gender selection in many Asian countries, but the practice still occurs. Advances in instrumentation and technology meant for diagnosis of diseased conditions can reveal the sex of an unborn child, sometimes associated with a genetic disorder (See chapter on Prenatal Diagnosis). However, this technology has been misused in many parts of the world to terminate a pregnancy for non-medical reasons (and there will always be an ethical debate over termination in the case of a fetus having a genetic disease). The vast majority of abortions are for normal fetuses not wanted by the parents at that time or because there are too many children already in the family. Q2. What will an embryo or a fetus develop into? What is the chances of a fetus at 12 weeks being born if left to the natural course of pregnancy? Q3. Is it right to terminate a pregnancy because the parents do not want a child? How about if it is because it is a girl child? © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> A Cross-Cultural Introduction to Bioethics 207 E4.3. Designer Children In societies where males are preferred for family succession and females shunned, or for economic factors, for example, because of the dowry system in India, such practices have mushroomed being misconstrued and misused both by the medical professional and the people. This has resulted in less number of girls as compared to boys. The situation has long term consequences when there will be scarcity of brides in a particular society; men will quarrel over brides, killing each other and especially targeting married men to marry their widows, or seek brides outside their caste and social set-up. This will lead to insecurity of married life with detrimental affects for the children also. The problems with pregnancy termination hence raise ethical queries into the status and rights of the unborn child, of the girl child, pregnancy termination as a family planning and spacing method, failure of medical ethics and legislation formulation and implementation. Some of the long-term consequences include social and marital implications, insecurity for married men and their children, lack of brides, etc. Assisted reproductive technology (ART) can also be used for designer children. This means to design the characters in children before they are born or conceived. Preimplantation diagnosis (See chapter E2) can allow embryo selection at 3 days of age when an 8-cell embryo, and parents can then choose which embryo to implant. Most individuals who donate gametes (eggs or sperm) are motivated principally by the desire to help infertile couples and do it for free or a modest fee. However, the question arises whether the ARTs should be available to all to try to improve selected qualities in their children which are unrelated to health. Athletic achievement, beauty, brains, social skills come immediately to mind. It is a fact that some wealthy couples, in the hope of having gifted or attractive children, are willing to pay large sums of money to donors they feel produce gametes of outstanding genetic quality. This demand has led, particularly in the US, to the development of competitive markets for superior sperm and oocytes dubbed “über-eggs” raising disconcerting echoes of eugenics (selective breeding programs) and related fears. The commercialization of oocyte donation, for instance, may coerce women to ignore the possible risks of IVF procedures or to conceal undesirable aspects of their and their family’s medical history (payment for organ donations is widely prohibited for this reason). An additional concern is whether extraordinary payments for gametes converts the child into a mere commodity. Q4. List both short term and long term consequences of an act where sex ratio is deliberately altered. Q5. Would you like to choose gametes from famous persons? From clever persons? From strong persons? Or just from the person you love? © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> A Cross-Cultural Introduction to Bioethics 208 E5. Prenatal Diagnosis of Genetic Disease Chapter objectives Genetic disease affects many persons, and in cases where it is severe, some families decide not to have children. For many parents they only realize this after the birth of the first affected child. Prenatal diagnosis allows the conditions of the embryo or fetus to be checked prior to birth, which presents several options to parents. This chapter aims to: 1. Describe methods for prenatal diagnosis. 2. Highlight major bioethical concerns associated with the choices that can be made. 3. Emphasize that the state should never force selective abortions because of prenatal diagnosis and discuss the ethical limits of parental choice. E5.1. Prenatal screening Prenatal diagnosis or screening has become associated with normal prenatal care in most industrialised countries. There are some important non-genetic screening programmes. For example, if a woman is not immune to rubella, she should be immunised before becoming pregnant. Recombinant DNA techniques were first used for prenatal selection of sickle cell disease in 1982. However the most common screening used in most countries is based on protein screening because for many diseases it is the lack of functional enzyme that is important, it may not matter what allele you have as long as some protein can be made (see the earlier example of PKU). For a growing number of known genetic diseases, methods have been developed to detect the genetic defect early in fetal life (For methods of genetic screening see the Chapter on Genetic Technology). These methods rely on removing a sample from the fetal material and analysing it. There are different stages at which fetuses can be screened for genetic disease or abnormalities. As far as the ethics and the distress and the health risk to the mother are concerned, the earlier the better. Fetal sampling is laborious so that currently only a small proportion of the population, can be screened even if it is considered desirable. Ultrasound is routinely used, and has the advantage of being non-invasive. Different methods may be combined, for instance the first screening may be maternal blood sampling, and if the level of certain proteins (e.g. alpha-fetoprotein) is abnormal, there is greater risk that the fetus may have some problem such as spina bifida or a chromosomal problem, like Down's syndrome. Then further testing is needed to check the result of a blood protein test, as still in most cases with an unusual protein level the fetus is normal. © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> A Cross-Cultural Introduction to Bioethics 209 Samples of placenta or fetal tissue may be taken from those fetuses considered at high risk, i.e. those of older mothers or parents who have a history of genetic disease. The older technique used is amniocentesis, where cells from the amniotic fluid are removed and grown in the laboratory for analysis. No harm is done to the fetus as the fetus is surrounded by discarded cells in the amniotic fluid which are no longer needed for further growth. The fetal samples can be taken at 11-16 weeks. It is now possible using very sensitive genetic probes to take a sample of the chorionic villi (membranes around the fetus) at 6-9 weeks and analyse the fetal DNA directly to determine whether it has a specific genetic defect, with the technique of chorionic villi sampling. Like amniocentesis there is a 1-2% risk of miscarriage after the sampling due to the procedure, which is why they are not general. We are still unable economically, ethically, or socially, to screen every fetus for so many diseases, with these techniques. Currently efforts and resources are focused on parents with higher risk, however, the latest screening techniques allow hundreds of samples to be tested with over ten thousand different probes simultaneously, which allows low cost routine screening, which could enter widespread use. In the mid-1990s mail order companies in the UK conducted cystic fibrosis tests. In the future it will be possible to routinely use the technique where the few fetal cells that can be found in the mother's blood are isolated, and analysed. It is already possible to use preimplantation diagnosis to look at an embryo before implanting it in the mother, when IVF is used. However, IVF is not an option for general use in developing countries at present as medical resources are limited. It may be an option for those parents who refuse abortion of a fetus, but have a high risk of passing on a genetic disease. Q1. Would you be interested to know the genetic profile of your embryo/fetus before birth? Why? E5.2. Therapy or abortion after prenatal diagnosis? The general aim of prenatal diagnosis is to reassure mother's who are worried that their fetus has some disease. They may avoid pregnancy without the possibility of such reassurance that the fetus did not inherit some disease, or abort because they worried about some ill effect from a drug used before the mother knew she was pregnant. Prenatal diagnosis does not always mean an affected fetus will be aborted. In fact, medically it should be separated. There are a number of advantages for the parents who want to bear a child regardless of the fetus's condition. The first is that some therapy may be possible to solve the problem, or even to lessen the seriousness of the condition. There are even cases of surgery being performed on a fetus and the fetus being returned to the mother's womb. Another benefit is knowledge, to be informed before birth and emotionally prepared. Human procreation is associated with a high degree of error, because when genetic elements rearrange there are often mistakes. The number of fertilised embryos with genetic abnormalities may be about 70%. Most of the genetically abnormal embryos are never implanted, or are spontaneously abort in early pregnancy. But some babies are born and will die later, some have a painful life, while others do not. © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> A Cross-Cultural Introduction to Bioethics 210 Q2. Is it right to terminate a pregnancy if the unborn child has a genetic/medical defect which cannot be treated? Is it right to terminate a pregnancy if the unborn child has a genetic/medical defect which can be treated? E5.3. Ethical issues of prenatal diagnosis If a fetus has a serious genetic impairment, with a consequence of serious mental deficiency, some people might say that the fetus does not, and will not in the future, have a "life" as "normal" humans have a life. While the potentiality is different, it is impossible to define what is a normal human life, and it is discriminatory to claim that some human beings do not have a life worth living. One of the achievements of the twentieth century has been to fight for the rights of all persons, and to not allow some people to claim other people are inferior. There are quality of life issues, but can we deny the potential for spiritual relationship between God and the most diseased forms of human life? Severely retarded individuals may not appear spiritually aware - but can people judge? Many religions would argue there are no "worthless" lives. We should build a society to prevent discrimination, and make life easier for those with disability, whether or not we accept using prenatal screening. The ethical issues that remain are questions of whether mother’s can choice to follow up diagnostic tests of the embryo or fetus, which can provide useful information for preventative action, with choices for abortion. This controversial issue will remain a divided question in the following centuries the same as it has for millennia in writings about the ethical issues of abortion. Different countries have contrasting approaches to these questions. This book chapter does not take a position on this topic, except an observation that it is a difficult moral dilemma and each culture has different ways to cope with the lack of consensus that is universal on the morality of these questions. E5.4. Whose choice? We can take the viewpoint of the child to be, the mother, or the family, and all views are important in cultures which are family-centred. Once we start to take society’s broader view, there are more ethical questions about interference in reproductive rights of persons. Although we will continue to see ethical division over the morality of prenatal genetic screening, with some people continuing to reject it, ethically we need a system to respect the informed choice of families. They must decide their responsibility to present dependents and future children, and think firstly of the children's quality of life. The correct decision is not to say do not abort or abort, but it may be the decision made by the informed mother. Society may put limits on the extent of this choice, e.g. maybe for sex selection, and maybe for fears of misuse. Q3. Imagine you are the government minister in a resource-poor country with a large population. What policy options to govern health services related to prenatal diagnosis would you offer? © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> A Cross-Cultural Introduction to Bioethics 211 E6. Female Infanticide Chapter Objectives. In some parts of the world still today, families kill girl children when born are killed within 24 to 48 hours of their birth. This chapter aims to: 1. Introduce the concept and history of female infanticide. 2. Discuss the case study of female infanticide in India 3. Discuss the causes for female infanticide, and how to prevent female infanticide around the world. E6.1. Female Infanticide Generally Female Infanticide is the act of killing a new born girl baby within 24 to 48 hours of birth. This doesn’t happen to male infants. Is this not a grave concern for humanity? Among the creatures in the world there is a tendency of the strongest one to dominate over the weakest one. This is true with human beings also. Although we can find female infanticide in various forms and ways in different countries, most of the countries stopped this cruel method by the middle of the late 19th century. However in certain countries like India, female infanticide still prevails to some degree. The people of Duma sacrifice a child every year to please their deity. The Romans were also accused of this type of practice, and it is said that this practice prevailed in northern Europe also. The Suevi and Scandinavians held it as a fixed principle that their happiness and security could be obtained only at the expense of the lives of others. The Pagan Arabs buried their daughters alive. E6.2. Female Infanticide in India In India female infanticide prevails to a significant extent, even after the 19th century attempts to stop it. In India the customs of female infanticide originated as a sacrifice to the god in some parts of Bengal. In some parts of Orissa when a couple had no children for a long time they took a vow to the goddess Ganga that if she bestowed upon them children, they would offer the first born to her. If they were blessed with children the eldest was reared for three or four years and on an auspicious day, it was a given a holy bath in the river; the child was encouraged to go further and further into the water till it was carried away by the stream. . Collaborating authors: Arockiam Thaddeus, M. Jothi Rajan, and Senthil Kumaran, India © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> A Cross-Cultural Introduction to Bioethics 212 This kind of offering is still practiced in some parts of Orissa. In Tamil Nadu the horrible fact of killing female children has been reduced but has not stopped yet. There are several causes for female infanticide in India today. The poor economic status of the family plays a major role. The raising of girls is said to be inauspicious with the Dowry System still prevailing as an incentive to avoid financial costs of marrying daughters. Other factors include illiteracy of the parents, and negative influence of some neighbors and society. E6.3. Why Should Female Infanticide be stopped? Female infanticide affects the immediate society as well as the larger society. When the mother, the father and the siblings are affected by killing a child in the family, the larger community feels ashamed. Female infanticide results in psychological shocks. Therefore they keep the fact as a secret even though the practice is very common in the community. The bioethical immaturity of the family should be exposed and proper counseling should be given to the members of the family. To prevent female infanticide around the world, parents should be educated. A baby of any gender should be considered to be the greatest gift of God. In the process of procreation nothing can happen without the presence of the female. Female infanticide is a social injustice to women. © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> A Cross-Cultural Introduction to Bioethics 213 Drama Groups of students can play out this skit in the presence of the teachers. First Family A baby boy is born. The whole family is very happy and all members of the family distribute sweets to their neighbors on this occasion. Neighboring Family A baby girl is born and the whole family seems to be sad and the neighbors come and complain to the mother for giving birth to a baby girl. This hurts the mother acutely and she takes the new born away to a distant place to kill the child. As she is snatching the child, the grandmother of the newborn baby watches this and follows her child. After walking for a distance she asked her daughter why she had taken her new born daughter to a distant place. The mother replies that the agony of giving birth to a girl child has been pricking her mind and so she has made up her mind to kill the newborn. The grandmother politely says to the newborn’s mother if she had killed her when she was born as a female child, what would have been the plight of the family. The grandmother advises her child and the mother repents for her act and immediately falls down at the feet of her mother and asks for her pardon. Now the newborn baby, her mother and her grandmother return home and give sweets to all the neighboring houses and celebrated the birth of the new girl child. Questions for Reflection Q1. What is Female Infanticide? Q2. Can we allow Female Infanticide? Who can be blamed? Q4. What is your action plan if you happen to see an incident of attempted female infanticide? © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> A Cross-Cultural Introduction to Bioethics 214 E7. Human Cloning Cloning is the process of asexually producing a group of cells (clones), all genetically identical to the original ancestor. The word is also used in recombinant DNA manipulation procedures to produce multiple copies of a single gene or segment of DNA. It is more commonly known as the production of a cell or an organism from a somatic cell of an organism with the same nuclear genomic (genetic) characters - without fertilization. A clone is a collection of cells or organisms that are genetically identical. Some vegetables are made this way, like asparagus, or flowers like orchids. From Scientific American November 24, 2001 (http://www.sciam.com/) Human reproductive cloning is the production of a human fetus from a single cell by asexual reproduction. In 2001 a cloned embryo was reported made by nuclear transfer, though in 1993 cloned embryos were made by splitting human embryos. Since the late 1990s reproductive cloning was used to produce clones of the adults of a number of mammalian species, including cats, dogs, cows, sheep, mice and pigs. The most famous of these was Dolly, the sheep. Many countries rushed to outlaw the possibility of reproductive cloning in humans. Most mammalian embryos can only be split into 2-4 clones, after that the cells lack the ability to start development into a human being. Therapeutic cloning is the cloning of embryos containing DNA from an individual's own cell to generate a source of embryonic stem (ES) cell-progenitor cells that can differentiate into the different cell types of the body. ES cells are capable of generating all cell types, unlike multipotent adult-derived stem cells which generate many but not all cell types. The aim is to produce healthy replacement tissue that would be readily available. Since it is from the same body it is immunocompatible so that the recipients would not have to take immunosuppressant drugs for the rest of their lives, as they do if they receive an organ from another person. Q1. Is there a difference between identical twins made in nature or ones made by human cloning? Q2. Such clones could be born at different times and/or from different mothers? Are they still twins? Q3. Should teachers be able to clone good students, or parents clone good children? Discuss the ethical issues of cloning. © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> A Cross-Cultural Introduction to Bioethics 215 E8. United Nations Declaration on Human Cloning Chapter Objectives In order to illustrate an example of the politics surrounding human cloning below is the Declaration and the extended press release which includes the viewpoints of some countries. Consider the issues behind the Declaration, which followed several years of hot debate. E7.1. United Nations Declaration on Human Cloning [59/280.] © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> 216 A Cross-Cultural Introduction to Bioethics E7.2. Press Release of the United Nations Declaration on Human Cloning Press Release 8 March 2005 GA/10333 Fifty-Ninth General Assembly Plenary 82nd Meeting (AM) GENERAL ASSEMBLY ADOPTS UNITED NATIONS DECLARATION ON HUMAN CLONING BY VOTE OF 84-34-37 The General Assembly this morning adopted the United Nations Declaration on Human Cloning, by which Member States were called on to adopt all measures necessary to prohibit all forms of human cloning inasmuch as they are incompatible with human dignity and the protection of human life. Acting on the recommendation of the Sixth Committee (Legal), contained in its report A/59/516/Add.1, the Assembly adopted the text by a vote of 84 in favour to 34 against, with 37 abstentions (See Annex). By further terms of the Declaration, Member States were also called on to protect adequately human life in the application of life sciences; to prohibit the application of genetic engineering techniques that may be contrary to human dignity; to prevent the exploitation of women in the application of life sciences; and to adopt and implement national legislation in that connection. The Declaration adopted today was the product of a Working Group established by the Assembly to finalize the text of a United Nations declaration on human cloning, which met in New York last month. Last November, the Sixth Committee averted a divisive vote on the © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> A Cross-Cultural Introduction to Bioethics 217 question of an international convention against human reproductive cloning by deciding to take up the issue as a declaration. Regretting the failure to achieve consensus, several delegations said they had voted against the text today because the reference to “human life” could be interpreted as a call for a total ban on all forms of human cloning. The Assembly had missed an opportunity to adopt a convention prohibiting reproductive cloning, said the United Kingdom representative, because of the intransigence of those who were not prepared to recognize that other sovereign States might decide to permit strictly controlled applications of therapeutic cloning. Echoing the views of a number of speakers, he said the Declaration was a non-binding political statement, which would not affect his country’s position on the issue. Those in favour of the Declaration welcomed its adoption, saying it constituted an important step in the protection of human dignity and the promotion of human rights, as well as a stepping stone in the process towards a complete ban on human cloning. The text, noted Costa Rica’s representative, sought to advance science in a clear framework of ethical norms. The text, added Ethiopia’s representative, sent a clear message against unethical research which made human life the object of experimentation. Explanations after Vote The representative of Mexico, speaking in explanation of position after the vote, said that those negotiating the Declaration had had to take into account uncertainty over new scientific advances, as well as its ethical, cultural and religious implications. There was a dichotomy between reproductive and therapeutic cloning and, during the entire process, Mexico had focused on seeking a consensus, first on the negotiation of a mandate and subsequently on the text itself. Regretfully, it had not been possible to achieve a consensus that would facilitate a universal norm, he said. Despite the fact that some delegations had decided not to yield in their original positions, many of their concerns had, in fact, been included in the final text just adopted. The text had the fundamental concern of guaranteeing human dignity and it reflected a realistic form of compromise. Hopefully, the National Parliament would take the necessary action, as the letter and spirit of the Declaration were in step with Mexican legislation and jurisprudence. The representative of China, also speaking in explanation after the vote, said that different countries varied in their understanding of the text’s inherent moral, ethical and religious aspects, and it was regrettable that the Declaration failed to give effect to the concerns of those countries. The prohibitions contained in the text could be misunderstood as covering all forms of cloning. Having voted against the Declaration, the Chinese Government would continue to adhere to its position against reproductive human cloning, while maintaining strict controls over therapeutic cloning. The representative of India expressed deep regret that the Sixth Committee had been unable to recommend to the plenary a text that was acceptable to all Member States on a matter of such paramount importance as an international convention against the reproductive cloning of human beings. India had voted against the political Declaration, as some of the provisions of the Declaration could be interpreted as a call for a total ban on all forms of human cloning. India remained totally opposed to reproductive cloning owing to the doubtful nature of its safety, success, utility and ethical acceptability, he said. However, the merits of therapeutic © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> 218 A Cross-Cultural Introduction to Bioethics cloning were considered on a case-by-case basis within the bioethical guidelines laid down with the approval of the National Bioethical Committee. The Declaration voted upon today was non-binding and did not reflect agreement among the wider membership of the General Assembly. India’s approach to therapeutic cloning, thus, remained unchanged. Belgium’s representative regretted that it was not possible to find agreement on a Declaration that could have found consensus in the Assembly. Today’s vote reflected the wide divergence in the international community on the text. Rather than bringing States together, it had divided them. It was essential that reproductive human cloning be prohibited. However, it was reasonable to preserve, at the national level, the possibility of carrying out therapeutic cloning. The representative of the United Kingdom said he voted against the Declaration, because the reference to “human life” could be interpreted as a call for a total ban on all forms of human cloning. He could not accept such an ambiguous Declaration, which might sow confusion about the acceptability of that important field of research. The Assembly had missed an opportunity to adopt a convention prohibiting reproductive cloning because of the intransigence of those who were not prepared to recognize that other sovereign States might decide to permit strictly controlled applications of therapeutic cloning. The Declaration voted on today was a weak, non-binding political statement that did not reflect anything approaching consensus within the Assembly, and would not affect the United Kingdom’s strong support of stem cell research. Hungary’s representative said he voted in favour of the Declaration because it attached the utmost importance to sending a strong message that the birth of cloned human beings was not acceptable. Furthermore, during the conduct of life sciences, there was a need for a delicate balance between the freedom of research and the adequate protection of human life and dignity. Also, the Declaration was in line with the existing obligations of Hungary under international law. He hoped the Declaration was only one step in the consideration of human cloning, and not the final stage. Hungary was open for further discussions in the international community at the appropriate time. The representative of the Republic of Korea said his country had voted against the political Declaration, which had not achieved a political consensus. It was not binding and would not affect the Republic of Korea’s future position on therapeutic cloning, which would reaffirm human dignity by relieving pain and suffering. The representative Thailand expressed regret that the General Assembly and the Sixth Committee had been unable to adopt a consensus Declaration. The Declaration just adopted was not binding and the text was ambiguous. In light of that, Thailand had voted against the Declaration and felt that it should be left to Member States to use their own interpretation as to whether or not to prohibit therapeutic cloning. The representative of Spain said that the term “human life” contained in the text was confusing and should be replaced by the term “human being” as used in scientific texts. The Declaration did not cover the well known fundamental differences between the two types of cloning. The fact that there had been no consensus on the issue after four years of discussion showed just how precarious the text was as adopted. Spain was opposed to reproductive cloning, but favoured therapeutic cloning, which was looked upon positively by the scientific community. The issue would now be passed on to the National Parliament. © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> A Cross-Cultural Introduction to Bioethics 219 Japan’s representative said he had voted against the resolution. The Declaration was difficult to interpret and did not respect the various views of Member States. The adopted text would not affect Japan’s domestic legislation on the issue. The representative of Brazil regretted the lack of consensus on the text adopted, which highlighted the deep division in the international community on the issue. He also regretted that the Sixth Committee had deviated from its original mandate to elaborate an international convention on human cloning. He had voted against the text, which did not contain language consistent with his country’s position on the issue. Singapore’s representative said he had voted against the resolution because it did not capture the diversity of views on the issue. Four years ago, the Assembly endorsed an initiative to begin work on an international convention on human cloning. There was still unanimity that reproductive cloning should be banned. It was unfortunate that that initiative was hijacked, and culminated today in the adoption of a text which sought to impose a single set of regulations on States regarding all forms of human cloning. The representative of the United States, welcoming the adoption of the Declaration, recalled that his delegation had explained its position in the Sixth Committee and would not give a further explanation today. The full text of that explanation was on the web site of the Permanent Mission of the United States. The representative of Poland said his delegation had voted in favour of the Declaration and unequivocally opposed the cloning of human embryos. Any use of human stem cells should be permitted only when the stem cells or stem cell lines were obtained from supernumerary cells, or when donors had expressed their willingness to permit it. The representative of South Africa said his delegation had abstained from the vote and found that the language of the text was deliberately ambiguous so as not to infringe on the rights of those who wished to continue with research in their own jurisdictions. South Africa was against reproductive human cloning and would continue with the strict regulation of therapeutic cloning. South Africa considered therapeutic cloning to be aimed at protecting human life and, as such, it was not inconsistent with the Declaration just adopted. The representative of Canada, emphasizing that his country’s position was clear, said reproductive cloning was illegal in Canada in whatever form. The ambiguity of the Declaration might give rise to certain political and other concerns. Norway’s representative said that his Government opposed both reproductive human cloning and therapeutic cloning, as reflected in its domestic legislation. It had sought to contribute to the elaboration of an international convention on the issue. At the same time, it had been willing to go along with a declaration, as long as it enjoyed consensus. He had voted against the Declaration, since it did not reflect the views of all States and did not enjoy consensus. The representative of Costa Rica said the adoption of the Declaration today constituted a historic step to promote human rights and guarantee human dignity in all circumstances. The text urged the scientific community to advance, bearing in mind the value of human dignity and human life. It was impossible to reach a consensus because a small group of States had rejected all reference to human life in the text. The Declaration sought to advance science in © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> 220 A Cross-Cultural Introduction to Bioethics a clear framework of ethical norms. It was of concern that some delegations had undermined the value of the Declaration, which had received majority support. France’s representative said she regretted the failure to find consensus. She was convinced that there was a clear consensus regarding the prohibition of reproductive human cloning. Also, given the threat of dangerous experimentation, it was essential to prohibit reproductive human cloning. However, she could not agree on prohibiting all forms of cloning. France had voted against the Declaration, and regretted the inability of the Assembly to send a universal message on such a vital issue. The representative of Nigeria regretted that he was not in the room when the voting took place. He was fully in favour of the Declaration. His country supported the Declaration because there was no alternative to it, for the time being. Human life was sacrosanct, and there was no reason for its violation. It was an inconceivable paradox that proponents of therapeutic cloning would sacrifice the life of one in order to serve another. He stressed that human cloning was unethical and a direct assault on human dignity. Today’s Declaration was only a stepping stone in the process towards a convention on a complete ban on human cloning. The representative of Mali said, had his delegation been present, it would have abstained from the vote, in accordance with the common position of the Organization of the Islamic Conference. The representative of the Russian Federation said that the question involved complex scientific and ethical issues and that his country had always been in favour of consensus. Regrettably, there had been no consensus. But, the Russian Federation had voted in favour of the Declaration, in order to send a message to the international community about the impermissibility of reproductive human cloning. The representative of Uganda said that her country had voted in favour of the Declaration because it opposed the destruction of human embryos and believed in the protection of human dignity. The Declaration was consistent with humanity’s responsibility to protect the sanctity of human life. The representatives of the Netherlands said his country had opposed the Declaration because it could be interpreted as a total ban on all forms of cloning. There was a need for strict oversight, but not a total ban. The Declaration just adopted was not binding. The representative of Ethiopia said he had voted in favour of the Declaration, which sent a clear message against unethical research, that made human life the object of experimentation. He hoped the funding for research into human cloning could be redirected towards research and development to find cures for those affected by HIV/AIDS, tuberculosis and malaria. The representative of Antigua and Barbuda said that, had she been in the room during the vote, she would have voted in favour of the text. Kyrgyzstan’s representative also said that, had he been in the room, he would have voted in favour. © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508> A Cross-Cultural Introduction to Bioethics 221 Libya’s representative congratulated the international community for adopting the Declaration, which was a step forward in the process towards a future convention to ban all forms of human cloning. The Declaration was a starting point in the protection of human dignity. He had voted in favour of the Declaration. ANNEX Vote on Declaration on Human Cloning The United Nations Declaration on Human Cloning (document A/59/516/Add.1) was adopted by a recorded vote of 84 in favour to 34 against, with 37 abstentions, as follows: In favour: Afghanistan, Albania, Andorra, Australia, Austria, Bahrain, Bangladesh, Belize, Benin, Bolivia, Bosnia and Herzegovina, Brunei Darussalam, Burundi, Chile, Comoros, Costa Rica, Côte d’Ivoire, Croatia, Democratic Republic of the Congo, Djibouti, Dominican Republic, Ecuador, El Salvador, Equatorial Guinea, Eritrea, Ethiopia, Georgia, Germany, Grenada, Guatemala, Guyana, Haiti, Honduras, Hungary, Iraq, Ireland, Italy, Kazakhstan, Kenya, Kuwait, Lesotho, Liberia, Liechtenstein, Madagascar, Malta, Marshall Islands, Mauritius, Mexico, Federated States of Micronesia, Monaco, Morocco, Nicaragua, Palau, Panama, Paraguay, Philippines, Poland, Portugal, Qatar, Rwanda, Saint Kitts and Nevis, Saint Lucia, Saint Vincent and the Grenadines, Samoa, San Marino, Sao Tome and Principe, Saudi Arabia, Sierra Leone, Slovakia, Slovenia, Solomon Islands, Sudan, Suriname, Switzerland, Tajikistan, The former Yugoslav Republic of Macedonia, Timor-Leste, Trinidad and Tobago, Uganda, United Arab Emirates, United Republic of Tanzania, United States, Uzbekistan, Zambia. Against: Belarus, Belgium, Brazil, Bulgaria, Cambodia, Canada, China, Cuba, Cyprus, Czech Republic, Democratic People’s Republic of Korea, Denmark, Estonia, Finland, France, Gabon, Iceland, India, Jamaica, Japan, Lao People’s Democratic Republic, Latvia, Lithuania, Luxembourg, Netherlands, New Zealand, Norway, Republic of Korea, Singapore, Spain, Sweden, Thailand, Tonga, United Kingdom. Abstain: Algeria, Angola, Argentina, Azerbaijan, Bahamas, Barbados, Burkina Faso, Cameroon, Cape Verde, Colombia, Egypt, Indonesia, Iran, Israel, Jordan, Lebanon, Malaysia, Maldives, Mongolia, Myanmar, Namibia, Nepal, Oman, Pakistan, Republic of Moldova, Romania, Serbia and Montenegro, Somalia, South Africa, Sri Lanka, Syria, Tunisia, Turkey, Ukraine, Uruguay, Yemen, Zimbabwe. Absent: Antigua and Barbuda, Armenia, Bhutan, Botswana, Central African Republic, Chad, Congo, Dominica, Fiji, Gambia, Ghana, Greece, Guinea, Guinea-Bissau, Kiribati, Kyrgyzstan, Libya, Malawi, Mali, Mauritania, Mozambique, Nauru, Niger, Nigeria, Papua New Guinea, Peru, Russian Federation, Senegal, Seychelles, Swaziland, Togo, Turkmenistan, Tuvalu, Vanuatu, Venezuela, Vietnam. © Eubios Ethics Institute 2005 A Cross-Cultural Introduction to Bioethics < http://www.unescobkk.org/index.php?id=2508>
 0
0
advertisement
Related documents





Download
advertisement
Add this document to collection(s)
You can add this document to your study collection(s)
Sign in Available only to authorized usersAdd this document to saved
You can add this document to your saved list
Sign in Available only to authorized users