Health Outcomes for Living Kidney Donors with Isolated Medical
advertisement

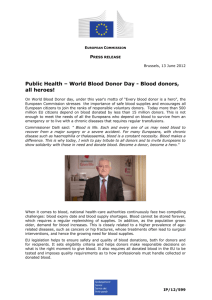
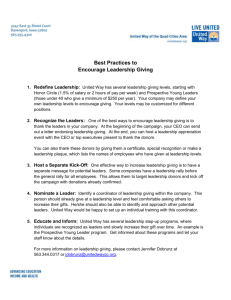
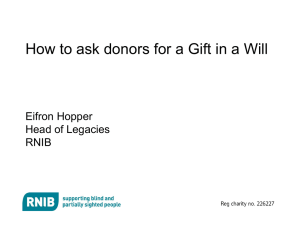
American Journal of Transplantation 2008; 8: 1878–1890 Wiley Periodicals Inc. C 2008 The Authors C 2008 The American Society of Journal compilation Transplantation and the American Society of Transplant Surgeons doi: 10.1111/j.1600-6143.2008.02339.x Health Outcomes for Living Kidney Donors with Isolated Medical Abnormalities: A Systematic Review A. Younga,b , L. Storsleyc , A. X. Garga,b, ∗ , D. Treleavend , C. Y. Nguane , M. S. Cuerdena and M. Karpinskic For the Donor Nephrectomy Outcomes Research (DONOR) Network a Division of Nephrology and b Department of Epidemiology and Biostatistics, University of Western Ontario, London, ON, Canada c Department of Medicine, University of Manitoba, Winnipeg, MB, Canada d Department of Medicine, McMaster University, Hamilton, ON, Canada e Department of Urologic Sciences, University of British Columbia, Vancouver, BC, Canada Donor Nephrectomy Outcomes Research (DONOR) Network Investigators: Neil Boudville, Laurence Chan, Christine Dipchand, Mona Doshi, Liane Feldman, Amit Garg, Colin Geddes, Eric Gibney, John Gill, Martin Karpinski, Scott Klarenbach, Greg Knoll, Charmaine Lok, Mauricio Monroy-Cuadros, Norman Muirhead, Christopher Y. Nguan, Chirag Parikh, Emilio Poggio, G. V. Ramesh Prasad, Leroy Storsley, Sudha Tata, Darin Treleaven, Robert Yang, Ann Young ∗ Corresponding author: Amit X. Garg, amit.garg@lhsc.on.ca Individuals with isolated medical abnormalities (IMAs) are undergoing living donor nephrectomy more frequently. Knowledge of health risks for these living donors is important for donor selection, informed consent and follow-up. We systematically reviewed studies with ≥3 living kidney donors with preexisting IMAs, including older age, obesity, hypertension, reduced glomerular filtration rate (GFR), proteinuria, microscopic hematuria and nephrolithiasis. We abstracted data on study and donor characteristics, perioperative outcomes, longer term renal and blood pressure outcomes and mortality and compared them to those of non-IMA donors. We found 22 studies on older donors (n = 987), 10 on obese donors (n = 484), 6 on hypertensive donors (n = 125), 4 on donors with nephrolithiasis (n = 32), 2 on donors with microscopic hematuria and one study each on donors with proteinuria or reduced GFR. Perioperative outcomes for donors with and without IMAs were similar. Few studies reported longer term (≥1 year) rates of hypertension, proteinuria or renal function. Studies were frequently retrospective and without a comparison group. Given the variability 1878 among studies and their methodological limitations, uncertainties remain regarding long-term medical outcomes for IMA donors. As transplant centers continue to cautiously screen and counsel potential IMA donors, rigorously conducted, longer term prospective cohort studies are needed. Key words: Hypertension, incremental risk, isolated medical abnormality, kidney transplantation, living donors, marginal donor Received 5 March 2008, revised 9 May 2008 and accepted for publication 7 June 2008 Introduction In recent years, living donor kidney transplantation rates have increased greatly in response to the growing need and longer waiting times for deceased donor transplantation. Increasingly, individuals who would have previously been deemed unsuitable as living donors due to relative medical contraindications are being considered. Described variably as having ‘isolated medical abnormalities (IMAs)’ (1,2), ‘asymptomatic urinary abnormalities’ (3) or as ‘complex’, ‘marginal’ or ‘at incremental risk’ (4–6), these living donors have conditions such as older age, obesity, hypertension, microscopic hematuria, proteinuria, reduced glomerular filtration rate (GFR) or nephrolithiasis (7). They may also have more than one abnormality. Some IMAs, namely older age, hypertension and albuminuria, are established risk factors for long-term renal impairment and cardiovascular disease (8–13). Long-term outcomes in healthy living kidney donors are frequently reported and help guide donor selection and followup. Outcomes among individuals with preexisting IMA(s) and a 50% reduction in renal mass via donor nephrectomy are less well known. This review aims to comprehensively assemble all relevant literature on outcomes of living kidney donors with IMAs. We examined short- and longer term medical outcomes, study quality and consistency of results. Herein, IMAs are defined as: (1) age: ≥60 years old, (2) obesity: BMI ≥30 kg/m2 , (3) hypertension: BP >140/90 mmHg or on antihypertensive medication, (4) hematuria: asymptomatic, microscopic, (5) proteinuria: ≥0.15 g/day, (6) GFR: ≤80 mL/min, (7) nephrolithiasis: ≥1 calculi. Living Kidney Donors with IMAs Methods Study selection The conduct and reporting of this systematic review and meta-analysis was guided by the Meta-analysis of Observational Studies in Epidemiology consensus statement (14). Cohort studies published in any language as full text or abstracts were relevant if they studied three or more living kidney donors with IMAs and reported at least one perioperative and/or longer term donor medical outcome. Results were considered longer term if donors were followed for at least 1 year after donation. Recipient outcomes and donor psychosocial or financial outcomes were not considered. We compiled citations from MEDLINE (1950–Jan/2008), EMBASE (1980– Jan/2008), CINAHL (1982–Jan/2008), BIOSIS Previews (1969–Jan/2008) and Cochrane Library bibliographic data bases. The search strategy included the terms living kidney donor combined with isolated medical abnormality, marginal donor, incremental risk, hypertension, hematuria, proteinuria, renal function, renal calculi, obesity or older. Terms were truncated to capture variations in terminology. Synonyms and related terms were also included. Searches used keywords over subject headings. The search strategy was pilot tested and modified to ensure that articles of known relevance were identified. Reference lists of included studies, the Science Citation Index and PubMed’s ‘see related articles’ were also searched. All citations were downloaded into Reference Manager 11.0 (Thomson ISI Research-Soft, Philadelphia, PA). Three authors (AY/MK/LS) independently evaluated each citation. Unsuitable articles were excluded on the basis of title or abstract. Any potentially relevant citations were retrieved in full text for a more detailed evaluation. Following evaluation, disagreements on article eligibility were resolved by consensus. When the same group of donors was described in multiple publications, we cited the article with the most IMA donors. Data abstraction Two authors (AY/MK) independently reviewed and abstracted study characteristics and methodological quality, baseline donor characteristics, surgical details and complications, pre- and postdonation blood pressure, proteinuria, hematuria, renal function and mortality. Another author (LS) independently confirmed the accuracy of all abstracted data. Disagreements on abstracted data were resolved by consensus. Primary study authors were contacted to clarify interpretations or to provide additional data. When a study described more than one IMA, data on each IMA with three or more living donors were abstracted independently. Quality appraisal of the studies was guided by Hayden et al. (15). Statistical analysis Interrater reliability was assessed using Fleiss’ generalized j, which describes the chance-corrected agreement among more than two raters (16,17). Analysis was done using Nichols’ MKAPPASC.SPS macro (18) with SPSS statistical software 15.0 (Chicago, IL). Descriptive statistics (e.g. group means) were weighted by the number of donors in each study group. Variance estimates for pre-post donation changes in outcomes such as blood pressure were not reported; they were 2 2 calculated as r2 = rpre + rpost − 2qrprerpost , where q represents the correlation between the pre- and postdonation values. We used a correlation of 0.5 to impute the missing change variance estimates in the final metaanalysis (19). Sensitivity analyses were performed on the choice of correlation, and results were qualitatively similar. For study-level meta-analysis, Cochran’s Q statistic was used to determine the presence of between-study heterogeneity by summing the squared de- American Journal of Transplantation 2008; 8: 1878–1890 viations of each study’s estimate from the meta-analytic estimate, weighting each study by the inverse variance of its effect estimator (20). The statistic was compared to the v 2 distribution with k -1 degrees of freedom, where k was the number of studies. The I2 statistic describes the percentage of total variation across studies that is due to heterogeneity rather than chance; I2 values of 25%, 50% and 75% were indicative of low, moderate and extreme heterogeneity, respectively (21). Results were mathematically pooled when I2 was ≤50%, using a random effects method that accounts for within- and between-study heterogeneity (22,23). Renal function is usually assessed by creatinine clearance or GFR and is often standardized to body surface area (BSA). In pooled estimates, we described all estimates of renal function as GFR, reported in ml/min (per 1.73 m2 ). Meta-analyses were conducted using Review Manager 4.2 (Cochrane Collaboration, Oxford, UK). Results were graphed in R 2.0.1 (R Foundation for Statistical Computing, Vienna, Austria). Results Study selection We screened 3510 citations, from which 90 full text articles were retrieved for detailed evaluation (Figure 1). Forty-three articles met the criteria for review. Six were subsequently excluded because they described the same groups of donors (24–29). Thus, we identified 37 articles with perioperative and/or longer term (≥ 1 year) medical outcomes for three or more living kidney donors with preexisting IMAs (5,30–65). Chance-corrected agreement for article eligibility between three independent reviewers was substantial (j = 0.71) (66). Description of included articles The 37 studies were published between 1986 and 2007 and were all in English. Thirty were full text articles and seven were conference abstracts (38,48,50,52,55,61,63). Potentially relevant publications identified: citations or abstracts screened for retrieval (n = 3510) Publications excluded on the basis of title and abstract (n = 3420) Full-text publications retrieved for more detailed evaluation (n = 90) Publications excluded with reasons (n = 53): • No IMAs of interest reported (n = 8) • Citation about living kidney recipients and not donors (n = 14) • Inclusion criteria not met (n = 19) • No distinct analysis of IMA donors (n = 6) • Duplicate citation or same donors described in multiple publications (n = 6) Publications included in the review (n = 37) Figure 1: Flow diagram outlining selection of studies of living kidney donors with IMAs. 1879 Young et al. The studies were from 13 countries: mostly North America (46%: USA: 15 studies, Mexico: 2 studies), followed by Europe (38%: Germany: 3 studies; Greece, Switzerland, Turkey: 2 studies each; Italy, Norway, Republic of Macedonia, Slovenia, Yugoslavia: 1 study each), then Asia (16%: India, Japan: 3 studies each). We successfully contacted 11 primary authors; 9 kindly supplied additional data (33,34,36,38,47,49,51,54,55,57,60). Some studies described more than one IMA, resulting in: 22 studies on older donors (5,30–50), 10 on obese donors (49,51–59), 6 on hypertensive donors (5,38,41,48,49,60), 4 on donors with nephrolithiasis (5,63–65), 2 on donors with microscopic hematuria (61,62) and one study each on donors with proteinuria (38) or reduced GFR (38) (Table 1). Only four studies reported the proportion of IMA donors lost to follow-up; all exceeded 10% (range 10–60%) (43,57,58,63). Donor outcomes assessed across studies of living kidney donors with IMAs are summarized in Table 2. Perioperative outcomes Older and younger donors were compared on operative time (32,36,46), surgical blood loss (32,36) and length of hospital stay (32,36,46), with no significant differences (Figure 2A). Similarly, obese and nonobese donors were compared on operative time (51–54,56,58), blood loss (51,52,54,56) and hospital stay (51–54,56,58) (Figure 2B). Differences were statistically significant but clinically insignificant. Surgical complications (e.g. minor infections, hemorrhage, pneumonia or pneumothorax) were not significantly higher for older or obese donors. Older donors, longer term outcomes Twenty-two articles reported on 987 older living kidney donors (mean age: 66 years old; range: 60–85 at donation). Older donors were most commonly defined as ≥60 years (68% of studies) with other studies defining older as ≥61 (45), ≥65 (36,38,44,47) and ≥66 years (30,42). Six were prospective cohort studies (35,38,45–47,49) and 16 were retrospective cohort studies (5,30–34,36,37,39–44,48,50). Sixteen studies had a comparison group of donors <60 years old (weighted mean age at donation: 47 years). Of these, six studies enrolled younger donors contemporaneously with older donors (35,38,45–47,49), while the rest used historical controls. Loss to follow-up was reported in only 1 of 22 studies. Older donors were followed for a median of 1.8 years (range from postop to 10 years). Fifteen of 22 studies had mean follow-up periods of 1 year or longer after donation, of which only 4 had mean follow-up periods of ≥5 years. Long-term renal function was reported in 8 of 15 studies; 1 study each described postdonation GFR (44) and change in GFR from 3 months to 1 year postdonation (41), 4 studies described change in serum creatinine from predonation to follow-up (37,40,43,49) and 3 studies described change in GFR from predonation to follow-up (38,49,50). Long-term 1880 blood pressure and proteinuria changes were reported in only 2 and 1 study, respectively. Meta-analysis of four studies comparing 181 older donors to 666 younger donors on change in serum creatinine from predonation to follow-up is presented in Figure 3A (37,40,43,49). Median follow-up was 2 years (range 1.0– 6.7 years). Results were too statistically heterogeneous to mathematically pool (v 2 = 31.90, p < 0.00001, I2 = 91%). One study reported that older donors had a 10 lmol/L (0.1 mg/dL) significantly greater increase in serum creatinine after donation over the increase for younger donors (49). Another study reported a 21 lmol/L (0.2 mg/dL) increase, but the confidence interval was wide and insignificant (40). Change in GFR from predonation to follow-up was reported in three studies comparing 23 older donors to 541 younger donors (38,49,50). GFR was assessed by inulin or radioisotope (38,49) or not reported (50). There was low-to-moderate statistical heterogeneity between the three studies (v 2 = 3.20, p = 0.20, I2 = 38%) (Figure 3B). When results were mathematically pooled, the decrement in GFR after donation was significantly less for older than younger donors (weighted mean difference: −6.38 mL/min (per 1.73 m2 ), 95% CI: −2.56 to −10.21). This pooled estimate is driven by one study with results contrary to what is expected (49). Long-term changes in blood pressure and proteinuria were not well characterized for older donors. Rather than an increase, one study reported a decrease in blood pressure for older donors compared to a small increase in younger donors after 1 year (SBP: −4.3 vs. 1.2 mmHg; DBP: −0.9 vs. 1.4 mmHg) (38). Another study reported a minimal difference in mean arterial blood pressure by age group after 6.7 years (49). One study reported no increase in albumin:creatinine ratio for either donors ≥65 years or <65 years, 1 year after donation (38). There were 27 deaths among older donors and 6 among younger donors, all unrelated to nephrectomy. Obese donors, longer term outcomes Ten studies examined 484 obese living donors with a mean BMI of 34.5 kg/m2 at donation (range: 32–39 kg/m2 ). Eight studies (78%) used an obesity cutpoint of 30 kg/m2 ; the other studies used definitions of BMI ≥31 (56) and 35 kg/m2 (51). Five studies prospectively followed a cohort of obese living donors (49,53–55,59), four were retrospective cohort studies (51,56–58) and one collected retrospective and prospective data (52). All studies compared obese donors to nonobese donors with BMI <30 kg/m2 (weighted mean BMI 24.4 kg/m2 ). Only two studies reported loss to follow-up rates (41% and 60%) (57,58). The median follow-up time for obese donors was 2.4 months (range from postdonation hospital discharge to 6.7 years). Long-term follow-up occurred in only 2 of 10 studies, with follow-up of 4.2 (59) and 6.7 years (49). Both studies described long-term change in serum creatinine American Journal of Transplantation 2008; 8: 1878–1890 Living Kidney Donors with IMAs Table 1: Characteristics of studies examining outcomes of living kidney donors, stratified by type of donor IMA Older donors Source∗ Hayashi et al., (30) Berardinelli et al., (31) Jacobs et al., (32) Haberal et al., (33) Shimmura et al., (34) Fauchald et al., (35) Tsuchiya et al., (36) Lezaic et al., (37) Tsinalis et al., ‡ (38) Kumar et al., (39) Nyberg et al., (40) Srivastava et al., (41) Grekas et al., (42) Kostakis et al., (43) Hsu et al., (44) Siebels et al., (45) Kumar et al., (5) Neipp et al., (46) Ivanovski et al., (47) Sahin et al., ‡ (48) Gracida et al., (49) Pabico et al., ‡ (50) Primary location Ehime, Japan Milan, Italy Baltimore, USA Ankara, Turkey Tokyo, Japan Oslo, Norway Akita, Japan Belgrade, Yugoslavia Basel, Switzerland Lucknow, India Minneapolis, USA Delhi, India Thessaloniki, Greece Athens, Greece Baltimore, USA Munich, Germany Lucknow, India Hannover, Germany Skopje, Macedonia Istanbul, Turkey Mexico City, Mexico Rochester, USA Prospective IMA Non-IMA study donors donor controls No No No No No Yes No No Yes No No No No No No Yes No Yes Yes No Yes No 41 39 42 34 241 70 14 50 13 21 5 46 25 161 6 19 82 35 28 20 6 4 None 193 42 None 518 165 48 99 75 25 10 None 35 174 None 141 None 158 50 None 422 14 Year(s) of donation 1980–1993 1969–2002 1996–2002 1975–1989 1982–1995 1985–1988 1998–2004 1987–1992 1988–1998 1989–1993 1971–1995 1996–2004 1976–1985 1986–1996 1995–2001 1994–2001 1988–2001 1996–2005 1991–1999 1983–1999 1992–2001 1976 Older donor age, Proportion lost mean ± SD (range), y† to follow-up, % 71 ± . . . (66–80) 64 ± 4 (60–72) 65 ± 4 (. . .) 62 ± . . . (60–76) 64 ± 4 (60–78) 66 ± . . . (60–81) 69 ± 4 (65–77) 66 ± 4 (60–85) 69 ± 4 (65–80) 64 ± . . . (. . .) 69 ± 10 (62–87) 62 ± 3 (60–71) . . . (66–76) 68 ± 6 (60–82) 69 ± 3 (65–74) . . . (>61) 63 ± 3 (. . .) 65 ± 4 (. . .) 69 ± . . . (65–81) . . . (>60) 62 ± . . . (. . .) 66 ± . . . (60–73) ... ... ... ... ... ... ... ... ... ... ... ... ... 24 ... ... ... ... ... ... ... ... Obese donors Source∗ Jacobs et al., (51) Chavin et al.,‡ (52) Chow et al., (53) Mateo et al., (54) Bachmann et al., ‡ (55) Kuo et al., (56) Rea et al., (57) Heimbach et al., (58) Espinoza et al., (59) Gracida et al., (49) Primary location Baltimore, USA Charleston, USA Rochester, USA Los Angeles, USA Basel, Switzerland Washington, USA Rochester, USA Minnesota, USA Mexico City, Mexico Mexico City, Mexico Prospective study IMA donors Non-IMA donor controls Year(s) of donation IMA donor BMI, mean ± SD (range), kg/m2 † Proportion lost to follow-up, % No ... Yes Yes Yes No No No Yes Yes 41 23 34 12 23 12 49 172 37 81 41 64 75 35 180 28 41 381 537 422 1996–1999 1998–2001 1999–2000 1999–2002 ... 1998–1999 2000–2003 1999–2003 1992–1999 1992–2001 39 ± 4 34 ± 1 34 ± 4 32 ± 2 . . . (>30) 34 ± 4 38 ± 5 34 ± 3 33 ± 2 33 ± . . . ... ... ... ... ... ... 60 41 ... ... Hypertensive donors Source∗ Primary location Prospective study IMA donors Non-IMA donor controls Year(s) of donation Textor et al., (60) Rochester, USA Yes 24 124 2001–2002 Tsinalis et al., ‡ (38) Basel, Switzerland Yes 46 75 1988–1998 Srivastava et al., (41) Delhi, India No 18 None 1996–2004 Kumar et al., (5) Lucknow, India No 12 None 1988–2001 Sahin et al., ‡ (48) Gracida et al., (49) Istanbul, Turkey Mexico City, Mexico No Yes 9 16 None 422 1983–1999 1992–2001 Definition of hypertensive donor BP > 140/90 by RN or > 135/85 by ABPM BP > 150/90 or antiHTN meds HTN controlled by a single med HTN controlled by a single med ... HTN controlled by diet or a single med Proportion lost to follow-up, % ... ... ... ... ... ... Continued. American Journal of Transplantation 2008; 8: 1878–1890 1881 Young et al. Table 1: Continued Reduced glomerular filtration rate (GFR) Source∗ Primary location Prospective study IMA donors Non-IMA donor controls Year(s) of donation Definition of IMA Proportion lost to follow-up, % Tsinalis et al.,‡ (38) Basel, Switzerland Yes 16 75 1988–1998 GFR < 70 mL/min by inulin clearance ... Tsinalis et al.,‡ (38) Basel, Switzerland Yes 8 Proteinuria 75 1988–1998 Alb/Cr > 10 mg/mmol OR Pro/Cr > 0.02 g/mmol ... Reinhardt et al.,‡ (61) Goettingen, Germany Ljubljana, Slovenia Yes ... Yes 3 None Presence of microhematuria IgA nephropathy confirmed by biopsy Strang et al.,‡ (63) Birmingham, USA Yes 9 Renal calculi None 2005–2006 10 Martin et al.,(64) Indianapolis, USA Yes 5 None 2003–2005 Rashid et al., (65) Ann Arbor, USA Yes 10 None 1996–2000 Kumar et al., (5) Lucknow, India No 8 None 1988–2001 Computed tomographic (CT) positive screening Computed tomographic (CT) positive screening Incidental, unilateral renal lithiasis Stone = < 1 cm Koselj et al., (62) Microscopic hematuria 5 None ... ... ... ... ... ... Alb/Cr = albumin to creatinine ratio; ABPM = ambulatory blood pressure monitoring; BP = blood pressure; Pro/Cr = protein to creatinine ratio; RN = registered nurse. †Age and BMI are reported at the time of donation. Ellipses (. . .) indicate not reported. ∗ Studies are arranged by the average number of years after donation. ‡Published as an abstract from a conference proceeding. and GFR (assessed using inulin or radioisotopes) from predonation to follow-up. Missing and nonimputable variance estimates precluded pooling of results. The two studies had conflicting results for the change in serum creatinine: one reported a 17 lmol/L greater increase in obese donors (59), while the other reported a 5 lmol/L greater increase in nonobese donors (49). The studies also had conflicting reports on change in GFR after donation: one reported no substantive difference between obese and nonobese donors (−40 vs. −38 mL/min (per 1.73 m2 )) (59), while the other described a 10 mL/min (per 1.73 m2 ) greater decrement in GFR for nonobese donors over the decrement seen in obese donors (49). One study also reported an increase of 4.6 mmHg for obese donors and 3 mmHg for nonobese donors in mean arterial pressure (no variance estimates reported) (49). Neither study reported proteinuria as an outcome. There were no deaths reported among obese donors. Hypertensive donors, longer term outcomes Six studies described 125 hypertensive donors (5,38,41, 48,49,60). Definitions for hypertension varied substantially, 1882 from blood pressure cutpoints of 135/85 to 150/90 mmHg to controlled blood pressure on a single antihypertensive agent or combinations thereof. Some studies did not provide a definition (48,49). Only one study reported measurement of blood pressure by health professionals (60); others did not specify how blood pressure was measured. Half of the studies were prospective cohort studies (38,49,60) with normotensive donors enrolled contemporaneously. The remaining used a retrospective design with no control group (5,41,48). None of the studies reported loss to follow-up. Follow-up ranged from 10 months to 6.7 years (median: 2.6 years). Five of six studies had mean follow-up periods of 1 year or more, of which two had mean follow-up periods ≥5 years. One long-term study only described the change in GFR from 3 months postdonation to 1-year follow-up in hypertensive donors (41). Of the remaining long-term studies, two assessed renal function. One found that hypertensive donors experienced a 14 lmol/L greater increase in serum creatinine over that of normotensive donors 6.7 years after donation. Two studies compared 62 American Journal of Transplantation 2008; 8: 1878–1890 Living Kidney Donors with IMAs Figure 2: (A) Meta-analyses of perioperative outcomes for older donors. (B) Meta-analyses of perioperative outcomes for obese donors. American Journal of Transplantation 2008; 8: 1878–1890 1883 Young et al. A Increase in serum creatinine (μmol/L)* Source Lezaic et al., 1996 Nyberg et al., 1997 Kostakis et al., 1997 Gracida et al., 2003 Length of follow-up (years) 1.0 (…) 1.8 (0.1-4.0) 2.1 (…) 6.7 (0.5-9.5) IMA donors N Mean (SD) 9 (4) 50 58 (18) 4 19 (8) 121 28 (5) 6 Non-IMA donors Older donor increase in serum creatinine N Mean (SD) mean difference (umol/L) 95% CI 11 (7) -2 (-3,0) 99 37 (24) 21 (-1,44) 11 2 (-1,4) 134 17 (9) 10 (6,14) 422 19 (6) -25 Increase in serum creatinine less for older donors B 0 25 50 Increase in serum creatinine greater for older donors Decrement in GFR (mL/min (per 1.73 m2))* Source Tsinalis et al., 1999 Gracida et al., 2003 Pabico et al., 1986 Pooled estimate Length of follow-up (years) 1.0 (…) 6.7 (0.5-9.5) 10.0 (…) Older donor decrement in GFR mean IMA donors Non-IMA donors N Mean (SD) N Mean (SD) 13 33 (18) 105 34 (16) 30 (5) 6 422 38 (12) 47 (14) 4 14 43 (21) 23 541 Test for overall effect: Z = 3.27 (P = 0.001) 0 (-11,10) -8 (-12,-4) 4 (-14,22) -6 (-10,-3) -25 0 Decrement in GFR less for older donors 25 Decrement in GFR greater for older donors Note: Graphed results are the difference between IMA and non-IMA donors on the change in outcome from before donation to after donation. † See Table 1 for mean donor age (…) indicates missing value * Results were not pooled for I > 50% hypertensive donors to 527 normotensive donors on change in inulin or radioisotope GFR (38,49). The results were conflicted, substantially heterogeneous and not pooled (v 2 = 12.12, p = 0.0005, I2 = 92%) (Figure 4). urine albumin. Another study reported on 10 living donors with reduced GFR; however, we believed the defined predonation GFR of ≤ 45 mL/min was a reporting error (5). Attempts to contact the authors for clarification were unsuccessful; thus, we excluded these 10 donors. Change in blood pressure after donation was quantified in one study. Blood pressure did not increase 1 year after donation; rather systolic and diastolic blood pressures reportedly decreased by 5 mmHg and 6 mmHg more, respectively, in hypertensive than normotensive donors (38). One study assessed change in mean arterial blood pressure after donation, which also decreased more often in hypertensive donors (49). One year after donation, neither hypertensive nor normotensive donors experienced an increase in albumin:creatinine ratio (38). There were two cases of donor mortality, both unrelated to nephrectomy. Two studies considered donors with preexisting microscopic hematuria (61,62). One had 5 donors from Alport syndrome families. After a mean follow-up of 4.7 years, 2 developed new onset hypertension, 3 had proteinuria and 3 had creatinine clearances ranging from 31 to 52 mL/ min (61). The other study followed 3 donors with biopsyconfirmed IgA nephropathy. After 7 years, 2 had normal renal function, urinalysis and blood pressure and one had a GFR < 15 mL/min per 1.73 m2 (62). One study considered donors with proteinuria, defined as a urine albumin:creatinine ratio > 10 mg/mmol or urine protein:creatinine ratio > 20 mg/mmol (38). After 1 year, donors with proteinuria maintained blood pressures below 140/90 mmHg (38) and albumin excretion decreased. Postdonation GFR assessed using inulin was no different between donors with and without preexisting proteinuria. Donors with other IMAs One abstract considered 16 donors with reduced GFR, defined as ≤70 mL/min (38). Eight years after donation, the donor with the lowest predonation GFR (60 mL/min assessed using inulin) had stable renal function and normal A Figure 3: Meta-analyses of long-term medical outcomes for older donors. Decrement in GFR (mL/min (per 1.73 m2))* Source Tsinalis et al., 1999 Gracida et al., 2003 Length of follow-up (years) 1.0 (…) 6.7 (0.5-9.5) IMA donors N Mean (SD) 46 38 (17) 16 29 (8) Non-IMA donors N Mean (SD) 105 34 (16) 422 38 (12) Hypertensive donor decrement in GFR 4 (-1,10) -8 (-12,-4) -15 Decrement in GFR less for hypertensive donors 0 15 Decrement in GFR greater for hypertensive donors Note: Graphed results are the difference between IMA and non-IMA donors on the change in outcome from before donation to after donation. † See Table 1 for definitions of hypertensive donor in each study (…) indicates missing value * Results were not pooled for I > 50% 1884 Figure 4: Meta-analyses of long-term medical outcomes for hypertensive donors. American Journal of Transplantation 2008; 8: 1878–1890 Living Kidney Donors with IMAs Table 2: Donor outcomes assessed across studies of living kidney donors with IMAs (stratified by type of IMA) Perioperative Source∗ Hayashi et al., 1995 Berardinelli et al., 2003 Jacobs et al., 2004 Haberal et al., 1991 Shimmura et al., 1999 Fauchald et al., 1991 Tsuchiya et al., 2006 Lezaic et al., 1996 Tsinalis et al., 1999 Kumar et al., 1994 Nyberg et al., 1997 Srivastava et al., 2005 Grekas et al., 1989 Kostakis et al., 1997 Hsu et al., 2002 Siebels et al., 2003 Kumar et al., 2003 Neipp et al., 2006 Ivanovski et al., 2001 Sahin et al., 2000 Gracida et al., 2003 Pabico et al., 1986 Jacobs et al., 2000 Chavin et al., 2002 Chow et al., 2002 Mateo et al., 2003 Bachmann et al., 2005 Kuo et al., 2000 Rea et al., 2006 Heimbach et al., 2005 Espinoza et al., 2006 Gracida et al., 2003 Surgical details Complications √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ Textor et al., 2004 Tsinalis et al., 1999 Srivastava et al., 2005 Kumar et al., 2003 Sahin et al., 2000 Gracida et al., 2003 Tsinalis et al., 1999 Kumar et al., 2003 Tsinalis et al., 1999 Reinhardt et al., 2007 Koselj et al., 1997 Strang et al., 2007 Martin et al., 2007 Rashid et al., 2004 Kumar et al., 2003 Kumar et al., 2003 Longer term Years after donation (range) Blood pressure Older donors Until postop Until d/c Until d/c . . . (0.1–3.6) . . . (1—13.8) 0.3 (. . .) 0.5 (. . .) 1 (. . .) 1 (. . .) 1.8 (. . .) 1.8 (0.1–4) 1.8 (0.5—4.2) 2 (. . .) 2.1 (. . .) 2.1 (0.3–4.5) 3.2 (0.04–5.2) 3.3 (0.3–7.4) 4.3 (0.1–9.1) 5 (. . .) 5.3 (1.8–7.4) 6.7 (0.5–9.5) 10 (. . .) Obese donors Until d/c Until d/c Until d/c Until d/c 5 days 0.4 (. . .) 0.9 (0.1–2.7) 0.9 (0.1–4.1) 4.2 (. . .) 6.7 (0.5–9.5) Hypertensive donors 0.8 (0.4–1.2) 1 (. . .) 1.8 (0.5–4.2) 3.3 (0.3–7.4) 5.3 (1.8–7.4) 6.7 (0.5–9.5) Proteinuria Renal function √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ Reduced renal function √ 1 (. . .) 3.3 (0.3–7.4) √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ √ Mortality √ √ √ √ √ √ Proteinuria √ √ √ 1 (. . .) Microscopic hematuria √ √ √ 4.7 (1–12) √ 7 (. . .) Renal calculi 0.9 (. . .) 1.9 (. . .) 3 (. . .) 3.3 (0.3–7.4) Studies assessed development of new renal calculi 3.3 (0.3–7.4) and stone-related complications after donation d/c = discharge; postop = postoperatively. American Journal of Transplantation 2008; 8: 1878–1890 1885 1886 IMA 100 (12) Tsinalis et al., 1999 102 (16) 102 (16) To convert serum creatinine from lmol/L to g/dL, divide by 88.4. † Reported as creatinine clearance (mL/min), an estimate of GFR. ‡ Assessment of CrCl and GFR are described in the ‘Results’ section. 62 (5) 80 (. . .) 88 (. . .) 100 (22) 102 (16) 116 (. . .) 118 (16) 116 (. . .) 112 (14) 112 (. . .) 94 (20) 102 (19) 108 (. . .) 103 (18) 111 (41)† 116 (. . .) 128 (22)† 102 (16) 91 (20)† 79 (15)† 100 (36)† NonIMA 101 (16) 122 (39)† 101 (. . .) 103 (14)† Tsinalis et al., 1999 95 (10) 96 (9) Textor et al., 2004 Tsinalis et al., 1999 Gracida et al., 2003 80 (9) 75 (19) 80 (9) 106 (18) 93 (15) 80 (9) 80 (. . .) 80 (4) 89 (27) 88 (18) 88 (8) 95 (13) 71 (9) 80 (. . .) 80 (. . .) 88 (27) 72 (16) 84 (. . .) 86 (21) 44 (. . .) 87 (20)† 67 (9)† 80 (15) 90 (3) 107 (19)† IMA GFR (mL/min (per 1.73 m2 ))‡ 80 (18) NonIMA Jacobs et al., 2000 Mateo et al., 2003 Kuo et al., 2000 Rea et al., 2006 Heimbach et al., 2005 Espinoza et al., 2006 Gracida et al., 2003 Hayashi et al., 1995 64 (. . .) Jacobs et al., 2004 80 (18) Haberal et al., 1991 Shimmura et al., 1999 81 (15) Tsuchiya et al., 2006 Lezaic et al., 1996 95 (3) Tsinalis et al., 1999 Kumar et al., 1994 106 (18) Nyberg et al., 1997 84 (15) Kostakis et al., 1997 88 (. . .) Hsu et al., 2002 Gracida et al., 2003 87 (. . .) Pabico et al., 1986 Source∗ Serum Creatinine (lmol/L) Before donation IMA Obese donors Until d/c Until d/c 115 (20) 0.4 (. . .) 124 (18) 0.9 (0.1–2.7) 115 (18) 0.9 (0.1–4.1) 126 (21) 4.2 (. . .) 115 (27) 6.7 (0.5–9.5) 94 (. . .) Hypertensive donors 0.8 (0.4–1.2) 133 (17) 1 (. . .) 6.7 (0.5–9.5) 121 (. . .) Reduced renal function 1 (. . .) Proteinuria 1 (. . .) 98 (. . .) 124 (11) 102 (21) 115 (18) 124 (18) 120 (. . .) 106 (18) 98 (. . .) 98 (. . .) 109 (27) 101 (. . .) 105 (20) 88 (17.7) 100 (8) 124 (27) NonIMA 65 (9) 52 (11) 61 (22) 64 (14) 78 (. . .) 72 (10) 84 (. . .) 107 (6)† 72 (15) 71 (. . .) 56 (14)† 53 (10) 58 (12)† IMA 68 (15) 68 (15) 68 (11) 68 (15) 79 (. . .) 80 (16) 79 (. . .) 118 (4)† 65 (12) 79 (. . .) 85 (19)† 68 (15) 64 (16)† NonIMA GFR (mL/min (per 1.73 m2 )) After donation Serum Creatinine (lmol/L) Older donors Until postop 97 (. . .) Until d/c 124 (27) . . . (0.1–3.6) 97 (9) . . . (1–13.8) 108 (21) 0.5 (. . .) 93 (17.7) 1 (. . .) 104 (4) 1 (. . .) 1.8 (. . .) 1.8 (0.1–4) 133 (19) 2.1 (. . .) 107 (. . .) 2.1 (0.3–4.5) 109 (36) 6.7 (0.5–9.5) 115 (. . .) 10 (. . .) Years after donation (range) Table 3: Studies of living kidney donors with IMAs that assessed GFR after donation 33 (9) 37 (15) 26 (24) 35 (18) 27 (15) 31 (19) 44 (23) 14 (. . .) 28 (5) 49 (18) 19 (8) 9 (4) 27 (19) 33 (. . .) 44 (23) IMA 19 (6) 29 (11) 27 (20) 35 (15) 18 (18) 27 (17) 27 (15) 19 (. . .) 19 (6) 37 (24) 17 (9) 10 (7) 25 (18) 44 (23) NonIMA Serum Creatinine (lmol/L) −38 (16) −38 (16) −38 (. . .) −32 (19) −34 (16) −38 (16) −34 (16) −34 (16) −40 (12) −28 (. . .) −33 (21) −38 (17) −29 (11) −10 (10) −35 (11) −38 (12) −43 (21)† −34 (16) −27 (18)† NonIMA −29 (16) −30 (5) −47 (14)† −33 (18) −29 (18)† IMA GFR (mL/min (per 1.73 m2 )) Change Young et al. American Journal of Transplantation 2008; 8: 1878–1890 Living Kidney Donors with IMAs Four studies examined 32 donors with renal calculi at the time of nephrectomy (5,63–65). Stone size ranged from 1 mm to 8 mm. One study reported that after 2 years, 1 donor experienced anuria from a stone in the lower ureter; after emergency stenting, the stone was removed via ureteroscopy (5). The other studies reported no recurrence of stone disease or stone-related complications (mean follow-up: 2.3 years). Discussion We comprehensively reviewed the literature on outcomes of living kidney donors with IMAs. Reassuringly, perioperative outcomes such as surgical time, blood loss and length of hospital stay were similar for donors with and without IMAs. Few studies adequately examined intermediate or long-term medical outcomes of principal interest to donors, recipients and transplant professionals. For this reason and the methodological limitations therein, the risks of this form of transplantation remain uncertain. Strengths and limitations of the review To our knowledge, this is the first comprehensive review of this topic. We believe our search strategy was robust and identified all relevant articles. Using multiple reviewers minimized potential selection biases and ensured accuracy of the abstracted data. We successfully contacted primary authors to clarify interpretations of study results and to obtain additional data. For some outcomes, we justified mathematically pooling results, mindful of the small number of studies (65). The most significant limitation of any review is the quality of the primary studies. There are very few studies documenting important health outcomes among living kidney donors with IMAs. Across all IMAs groups, longer term assessments (≥1 year) of blood pressure, proteinuria and renal function were reported in only 3, 2 and 10 studies, respectively. Only 17 of the 37 studies had prospective data collection. Only one prospective study reported the loss to follow-up (10%) and 3 retrospective studies reported loss to follow-up of 24–60%, raising concerns about the representativeness of the results. Study size was also frequently small; for the prospective studies, only 3 followed ≥30 donors. Some studies reported differential lengths of follow-up between IMA and non-IMA donors. Overall, the ability of these studies to identify significant differences in long-term medical risks, should they in truth exist, is limited. Variable definitions of IMA donors confounded the comparison of studies. Some studies were excluded because IMA definitions did not meet our criteria for review. For example, some studies defined ‘older’ as ≥55 years of age and included donors over 60. Without data on each patient, our review excluded some eligible older donors. Furthermore, some donors may have had more than one IMA (e.g. hyAmerican Journal of Transplantation 2008; 8: 1878–1890 pertensive, older donors). While we stratified results by IMA, overlaps of conditions were often unclear, leading to potential misclassification. It is possible that risk outcomes attributable to any IMA may be confounded by other health conditions or other IMAs. Last, we cannot exclude the possibility of a publication bias from the underreporting of adverse outcomes for IMA donors. While there are methods to assess such bias, such as Egger’s test for funnel plot asymmetry (67), too few studies precluded such proper assessments. IMA donors in perspective Long-term follow-up studies in living kidney donation suggest that the risks for a healthy donor are low. Although donors may be more likely to develop hypertension and proteinuria (68,69), they do not appear to be at increased risk of accelerated loss of renal function, kidney failure or cardiovascular disease (70–72). Many of these studies are small, retrospective, have limited long-term follow-up (∼10 years), considerable losses or unsuitable controls (73–75). Notwithstanding these methodological concerns and uncertainties, living donation is a globally accepted practice. The Amsterdam Forum report contains recommendations for an international standard of care in an effort to ‘define and affirm the responsibility of the transplant community for the live kidney donor ’ (7). The guidelines suggest that potential IMA donors should generally be precluded from donation due to substantial uncertainty for the long-term risks of nephrectomy compared to donors in good general health. Donors with IMAs are, however, being accepted with increasing frequency. Analysis of the OPTN/UNOS data base found that of 9319 kidney donations from July 2004 to December 2005, 2143 (23%) of donors were over 65 years of age or had hypertension, obesity or proteinuria (76). Furthermore, a survey of transplant programs in the USA indicates that they are more willing to accept older or hypertensive donors than a decade ago (77). The overall growth of living donation and the acceptance of more IMA donors may be driven by the success of the procedure, accumulation of long-term experience in nonIMA donors, a perpetual shortage of deceased donor organs and a greater emphasis on donor autonomy among transplant teams. The living donor population may also be changing over time; baseline prevalence of IMAs may be increasing or donors may be more determined to donate than ever before. Within reasonable limits, donors have the right to accept personal risk when making an informed decision with their recipients. In the absence of reliable data, transplant teams must still provide responsible counsel as more individuals with IMAs come forward for assessment. For readers, we efficiently summarized all available literature on outcomes among living kidney donors with IMAs. 1887 Young et al. Unfortunately, the existing literature does little to inform clinical practice or guide informed consent procedures. Better data and further studies are needed to make definitive conclusions. Until then, potential donors with IMAs are either excluded from donation, or physicians must extrapolate the risks and uncertainties using population data. One approach, advocated by Steiner, considers the prevalence of an IMA (e.g. hypertension) in the general population and the reported incidence of kidney failure associated with the IMA to approximate the risk of renal disease for IMA donors (78). One must be mindful that this approach does not consider the role of a donor nephrectomy in risk (if any) and is not possible for IMAs without robust population data (e.g. borderline GFR). Moreover, this approach cannot be used to estimate many other relevant donor outcomes such as severity of hypertension or cardiovascular risk. Hopefully, the few existing studies of IMA donors designed to assess longer term outcomes will report follow-up data in the future (38,60). Recent efforts to develop living donor registries may also aid in assessing the long-term risks for IMA donors. Well-designed prospective cohort studies in living kidney donation have been called for, including further studies of IMA donors. In designing such studies, we highlight several methodological considerations. To increase generalizability and facilitate recruitment, future studies should be multicentre efforts with standardized definitions for IMAs. In addition to IMAs, other risk factors for adverse donor outcomes should be considered, including family history of renal failure and hypertension and race (79–81). General population controls with IMAs would likely be unsuitable appreciating that they are not evaluated to the same degree that IMA donors are. Thus, healthy donor controls would need to be considered. Assessment of blood pressure, renal outcomes and other clinically significant outcomes would need to be standardized and rigorously performed over the long term. Finally, for donors with multiple IMAs, analytic methods would need to be used to minimize confounding on the incremental effect of any given IMA on long-term outcomes. Future studies considering these issues would ultimately address the effect of expanding the living donor pool with IMA donors and translate to better centre policy. As transplant centers continue to cautiously screen and counsel potential IMA donors, we strongly advocate for the initiation and concurrent data collection from such rigorously designed studies. Acknowledgments We thank Ms. Heather Thiessen-Philbrook, MMath for her statistical advice. We also thank the 11 primary authors of the included studies who generously confirmed and provided information for this review. This review was supported by the Multi Organ Transplant Program of the London Health Sciences Centre, London, Ontario, Canada. Ms. Ann Young was supported by a Canada Graduate Scholarship from the Canadian In- 1888 stitutes of Health Research, a Schulich Graduate Scholarship from the University of Western Ontario and a research award from the Lawson Health Research Institute. Dr. Amit Garg was supported by a Clinician Scientist Award from the Canadian Institutes of Health Research. Conflict of Interest: None declared. References 1. Davis CL, Delmonico FL. Living-donor kidney transplantation: A review of the current practices for the live donor. J Am Soc Nephrol 2005; 16: 2098–2110. 2. Steiner RW. Risk appreciation for living kidney donors: Another new subspecialty? Am J Transplant 2004; 4: 694–697. 3. Vadivel N, Stankovic A, Rennke HG, Singh AK. Accepting prospective kidney donors with asymptomatic urinary abnormalities: Are we shooting in the dark? Kidney Int 2007; 71: 173–177. 4. Reese R, Caplan A, Kesselheim A, Bloom R. Creating a medical, ethical, and legal framework for complex living kidney donors. Clin J Am Soc Nephrol 2006; 1: 1148–1153. 5. Kumar A, Das SK, Srivastava A. Expanding the living related donor pool in renal transplantation: Use of marginal donors. Transplant Proc 2003; 35: 28–29. 6. The Canadian Council for Donation and Transplantation. Enhancing living donation: A Canadian Forum. Report and recommendations. 2006. Edmonton, AB. 7. Delmonico FA. Report of the Amsterdam forum on the care of the live kidney donor: Data and Medical guidelines. Transplantation 2005; 79(6 Suppl): S53–S66. 8. Wang Y, Chen X, Song Y, Caballero B, Cheskin LJ. Association between obesity and kidney disease: A systematic review and meta-analysis. Kidney Int 2008; 73: 19–33. 9. Iseki K, Iseki C, Ikemiya Y, Kinjo K, Takishita S. Risk of developing low glomerular filtration rate or elevated serum creatinine in a screened cohort in Okinawa, Japan. Hypertens Res 2007; 30: 167– 174. 10. Jafar TH, Stark PC, Schmid CH et al. Proteinuria as a modifiable risk factor for the progression of non-diabetic renal disease. Kidney Int 2001; 60: 1131–1140. 11. Klag MJ, Whelton PK, Randall BL et al. Blood pressure and end-stage renal disease in men. N Engl J Med 1996; 334: 13– 18. 12. Peterson JC, Adler S, Burkart JM et al. Blood pressure control, proteinuria, and the progression of renal disease. The Modification of Diet in Renal Disease Study. Ann Intern Med 1995; 123: 754– 762. 13. Vasan RS, Larson MG, Leip EP et al. Impact of high-normal blood pressure on the risk of cardiovascular disease. N Engl J Med 2001; 345: 1291–1297. 14. Stroup DF, Berlin JA, Morton SC et al. Meta-analysis of observational studies in epidemiology: A proposal for reporting. MetaAnalysis Of Observational Studies in Epidemiology (MOOSE) group. JAMA 2000; 283: 2008–2012. 15. Hayden JA, Cote P, Bombardier C. Evaluation of the quality of prognosis studies in systematic reviews. Ann Intern Med 2006; 144: 427–437. 16. Fleiss J. Measuring nominal scale agreement among many raters. Psychol Bull 1971; 76: 378–382. 17. Siegel S, Castellan N. Nonparametric Statistics for the Behavioral Sciences. 2nd Ed. ed. New York: McGraw-Hill, 1988. 18. MKAPPASC.SPS/MKAPPASC.TXT (SPSS Macro/SPSS read me). 1997. American Journal of Transplantation 2008; 8: 1878–1890 Living Kidney Donors with IMAs 19. Follmann D, Elliott P, Suh I, Cutler J. Variance imputation for overviews of clinical trials with continuous response. J Clin Epidemiol 1992; 45: 769–773. 20. Cochran W. The combination of estimates from different experiments. Biometrics 1954; 10: 101–129. 21. Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. Br Med J 2003; 327: 557–560. 22. DerSimonian R, Kacker R. Random-effects model for meta-analysis of clinical trials: An update. Contemp Clin Trials 2007; 28: 105– 114. 23. Laird NM, Mosteller F. Some statistical methods for combining experimental results. Int J Technol Assess Health Care 1990; 6: 5–30. 24. Berardinelli L, Beretta C, Carini M. How to restore youth to old living donor kidneys for transplantation. Nephrol Dial Transplant 2002; 17(Abstracts Suppl 1). 25. Fauchald P, Holdaas H, Albrechtsen D, Flatmark A. The use of elderly living donors. Kidney Int 1989; 35: 513. 26. Berardinelli L, Beretta C, Raiteri M, Carini M. Early and long-term results using older kidneys from cadaver or living donors. Clin Transpl 2001;157–166. 27. Ivanovski N, Popov Z et al. Living related renal transplantation–the use of advanced age donors. Clin Nephrol 2001; 55: 309–312. 28. Kostakis AJ, Kyriakidis S, Garbis S et al. The fate of renal transplants from elderly living related donors. Transplant Proc 1990; 22: 1432–1433. 29. Haberal M, Sert S, Gulay H et al. Is donor nephrectomy a safe procedure in the elderly? Transplant Proc 1988; 20: 791–793. 30. Hayashi T, Koga S, Higashi Y et al. Living-related renal transplantation from elderly donors (older than 66 years of age). Transplant Proc 1995; 27: 984–985. 31. Berardinelli L. Living donor transplantations with marginal kidneys. Transplant Proc 2003; 35: 941–943. 32. Jacobs SC, Ramey JR, Sklar GN, Bartlett ST. Laparoscopic kidney donation from patients older than 60 years. J Am Coll Surg 2004; 198: 892–897. 33. Haberal M, Sert S, Altunkan S, Gulay H, Hamaloglu E, Bulut O. Kidney transplantation from elderly living donors. Int J Artif Organs 1991; 14: 335–337. 34. Shimmura H, Tanabe K, Ishikawa N et al. Influence of donor renal reserve on the long-term results of living kidney transplantation from elderly donors. Transplant Proc 1999; 31: 2874–2876. 35. Fauchald P, Sodal G, Albrechtsen D et al. The use of elderly living donors in renal transplantation. Transpl Int 1991; 4: 51–53. 36. Tsuchiya N, Satoh S, Sato K et al. Hand assisted retroperitoneoscopic living donor nephrectomy in elderly donors. J Urol 2006; 175: 230–234. 37. Lezaic V, Djukanovic L, Blagojevic-Lazic R et al. Living related kidney donors over 60 years old. Transpl Int 1996; 9: 109–114. 38. Tsinalis D, Binet I, Steiger J, Gasser T, Thiel G. Can “borderline” living kidney donors (BLKD) be used safely for transplantation? Kidney Blood Press Res 1999; 22 : 388–389. 39. Kumar A, Kumar RV, Srinadh ES et al. Should elderly donors be accepted in a live related renal transplant program? Clin Transplant 1994; 8: 523–526. 40. Nyberg SL, Manivel JC, Cook ME et al. Grandparent donors in a living related renal transplant program. Clin Transplant 1997; 11(5 Pt 1): 349–353. 41. Srivastava A, Sinha T, Varma PP et al. Experience with marginal living related kidney donors: Are they becoming routine or are there still any doubts? Urology 2005; 66: 971–975. 42. Grekas D, Alivanis P, Kalekou H, Spanos P, Tourkantonis A. Kidney transplantation from living donors over 66 years of age. Transplant Proc 1989; 21: 3851–3852. American Journal of Transplantation 2008; 8: 1878–1890 43. Kostakis A, Bokos J, Stamatiades D et al. The 10 years single center experience of using elderly donors for living related kidney transplantation. Geriatr Nephrol Urol 1997; 7: 127–130. 44. Hsu TH, Su LM, Ratner LE, Kavoussi LR. Laparoscopic donor nephrectomy in the elderly patient. Urology 2002; 60: 398–401. 45. Siebels M, Theodorakis J, Schmeller N et al. Risks and complications in 160 living kidney donors who underwent nephroureterectomy. Nephrol Dial Transplant 2003; 18: 2648–2654. 46. Neipp M, Jackobs S, Jaeger M et al. Living kidney donors >60 years of age: Is it acceptable for the donor and the recipient? Transpl Int 2006; 19: 213–217. 47. Ivanovski N, Popov Z, Kolevski P et al. Use of advanced age donors in living renal transplantation—Is it justified? Transplant Proc 2001; 33: 1227–1228. 48. Sahin S, Kayacan S, Kazancioglu R et al. Transplantation from living related marginal donors. Nephrol Dial Transplant 2000; 15 : A275. 49. Gracida C, Espinoza R, Cedillo U et al. Kidney transplantation with living donors: Nine years of follow-up of 628 living donors. Transplant Proc 2003; 35: 946–947. 50. Pabico RC, Mckenna BA, Sandroni S, Freeman RB. Should healthy subjects 60 years old or older be accepted as living related kidney donors (LRKD)? Age 1986; 9: 120. 51. Jacobs SC, Cho E, Dunkin BJ et al. Laparoscopic nephrectomy in the markedly obese living renal donor. Urology 2000; 56: 926–929. 52. Chavin KD, Baillie M, Ashcraft E et al. Laparoscopic donor nephrectomy is safe for the obese living kidney donor. J Am Soc Nephrol 2002; 13(Program and Abstracts Issue): 597A. 53. Chow GK, Prieto M, Bohorquez HE, Stegall MD. Hand-assisted laparoscopic donor nephrectomy for morbidly obese patients. Transplant Proc 2002; 34: 728. 54. Mateo RB, Sher L, Jabbour N et al. Comparison of outcomes in noncomplicated and in higher-risk donors after standard versus hand-assisted laparoscopic nephrectomy. Am Surg 2003; 69: 771– 778. 55. Bachmann A, Ruszat R, Giannini O et al. Obese donors report more pain after donor nephrectomy. Eur Urol Suppl 2005; 4: 168. 56. Kuo PC, Plotkin JS, Stevens S, Cribbs A, Johnson LB. Outcomes of laparoscopic donor nephrectomy in obese patients. Transplantation (Baltimore) 2000; 69: 180–182. 57. Rea DJ, Heimbach JK, Grande JP et al. Glomerular volume and renal histology in obese and non-obese living kidney donors. Kidney Int 2006; 70: 1636–1641. 58. Heimbach JK, Taler SJ, Prieto M et al. Obesity in living kidney donors: Clinical characteristics and outcomes in the era of laparoscopic donor nephrectomy. Am J Transplant 2005; 5: 1057–1064. 59. Espinoza R, Gracida C, Cancino J et al. Effect of obese living donors on the outcome and metabolic features in recipients of kidney transplantation. Transplant Proc 2006; 38: 888–889. 60. Textor SC, Taler SJ, Driscoll N et al. Blood pressure and renal function after kidney donation from hypertensive living donors. Transplantation 2004; 78: 276–282. 61. Reinhardt J, Weber M, Fries J, Mueller G, Gross O. Living donor kidney transplantation from relatives with mild urinary abnormalities in alport syndrome: Risk, benefit and outcome in six families. J Am Soc Nephrol 2007; 18 (Program and Abstracts Issue). 62. Koselj M, Rott T, Kandus A, Vizjak A, Malovrh M. Donor-transmitted IgA nephropathy: Long-term follow-up of kidney donors and recipients. Transplant Proc 1997; 29: 3406–3407. 63. Strang AM, Lockhart ME, Burns JR, Amling CL, Kolettis PN. Short term outcomes of living donor allograft nephrolithiasis in renal transplant donors and recipients. J Urol 2007; 177(4, Suppl. S). 64. Martin G, Sundaram CP, Sharfuddin A, Govani M. Asymptomatic urolithiasis in living donor transplant kidneys: Initial results. Urology 2007; 70: 2–5. 1889 Young et al. 65. Rashid MG, Konnak JW, Wolf JS Jr. et al. Ex vivo ureteroscopic treatment of calculi in donor kidneys at renal transplantation.[see comment]. J Urol 2004; 171: 58–60. 66. Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics 1977; 33: 159–174. 67. Egger M, Davey SG, Schneider M, Minder C. Bias in meta-analysis detected by a simple, graphical test. Br Med J 1997; 315: 629– 634. 68. Boudville N, Ramesh Prasad GV, Knoll G et al. Meta-Analysis: Risk for hypertension in living kidney donors. Ann InternMed 2006; 145: 185–196. 69. Garg AX, Muirhead N, Knoll G et al. Proteinuria and reduced kidney function in living kidney donors: A systematic review, metaanalysis, and meta-regression. Kidney Int 2006; 70: 1801–1810. 70. Najarian J, Chavers BM, McHugh L, Matas A. 20 Years or more of follow-up of living kidney donors. Lancet(British Edition) 1992; 3408823: 807–810. 71. Williams SL, Oler J, Jorkasky DK. Long-term renal function in kidney donors: A comparison of donors and their siblings. Ann Intern Med 1986; 105: 1–8. 72. Johnson EM, Remucal MJ, Gillingham KJ et al. Complications and risks of living donor nephrectomy. Transplantation 1997; 64: 1124– 1128. 73. Talseth T, Fauchald P, Skrede S et al. Long-term blood pressure and renal function in kidney donors. Kidney Int 1986; 29: 1072– 1076. 1890 74. Vincenti F, Mend WJ Jr., Kaysen G et al. Long-term renal function in kidney donors. Sustained compensatory hyperfiltration with no adverse effects. Transplantation 1983; 36: 626–629. 75. Watnick T, Jenkins R, Rackoff P, Baumgarten A, Bia M. Microalbuminuria and hypertension in long-term renal donors. Transplantation 1988; 45: 59–65. 76. Reese P, McBride M, Anderson K, Bloom R. Substantial variation in acceptance of complex living kidney donors across renal transplant centres in the USA. Am J Transplant 2007; 7 (Suppl 2): 170– 171. 77. Mandelbrot DA, Pavlakis M, Danovitch et al. The medical evaluation of living kidney donors: A survey of US transplant centers. Am J Transplant 2007; 7: 2333–2343. 78. Steiner RW, Gert B. A technique for presenting risk and outcome data to potential living renal transplant donors. Transplantation 2001; 71: 1056–1057. 79. Iglesias-Marquez RA, Calderon S, Santiago-Delpin EA et al. The health of living kidney donors 20 years after donation. Transplant Proc 2001; 33: 2041–2042. 80. Laskow DA, Jones P, Deierhoi MH et al. Are black livingrelated renal donors at greater long-term risk of renal complications than white donors? Transplant Proc 1991; 23(1 Pt 2): 1328–1329. 81. Gibney EM, King AL, Maluf DG, Garg AX, Parikh CR. Living kidney donors requiring transplantation: Focus on African Americans. Transplantation 2007; 84: 647–649. American Journal of Transplantation 2008; 8: 1878–1890