Exercise Testing Protocols
for Different Abilities in the Older Population
Kristen Carr
Claudia Emes
Marianne Rogerson
ABSTRACT. Assessment of the physical capacity of the elderly can be
used for predicting falls, institutionalization, and mortality. Practitioners
can also determine program needs and evaluate how well the program
meets the needs of older participants. How and what to assess depends on
several factors including objectives of the program, needs of the participant, age, and existing functional capacity. This article reviews tests that
are currently used in relation to types of functional fitness. Lastly, it indicates which tests are practical for different levels of ability using
Spirduso’s classification system of five different functional levels: physically dependent, physically frail, physically independent, physically fit
and physically elite. [Article copies available for a fee from The Haworth
Document Delivery Service: 1-800-HAWORTH. E-mail address: <docdelivery@
haworthpress.com> Website: <http://www.HaworthPress.com> © 2003 by The
Haworth Press, Inc. All rights reserved.]
KEYWORDS. Assessment, functional capacity, fitness, older, elderly
Kristen Carr, BSc, CSCS, is MKin graduate candidate, University of Calgary, with
a special interest in fitness testing and assessment for older people.
Claudia Emes, PhD is Professor of Kinesiology, University of Calgary, with a specialization in adapted physical activity and gerontology.
Marianne Rogerson, BKin, BA, is exercise therapist, Kerby Center in Calgary.
Address correspondence to: Claudia Emes, PhD, Faculty KinesiologyKNB234,
University of Calgary, Calgary, Alberta, Canada, T2N 1N4 (E-mail: cemes@ucalgary.
ca) or Marianne Rogerson, BKin, BA, 1133 7th Avenue SW, Kerby Center, Calgary,
Alberta, Canada, T2P 1B2 (E-mail: mariannerogerson@hotmail.com).
Activities, Adaptation & Aging, Vol. 28(1) 2003
http://www.haworthpress.com/web/AAA
2003 by The Haworth Press, Inc. All rights reserved.
Digital Object Identifier: 10.1300/J016v28n01_04
49
50
ACTIVITIES, ADAPTATION & AGING
Assessment of the physical capacity of the elderly relative to their
strength, endurance, flexibility, balance and coordination is important
in different ways. It is used for predicting falls, institutionalization, and
mortality. It is also used to determine program needs and evaluate the
success of a program in meeting those needs. How and what to assess,
however, depends on several factors including objectives of the program, needs of the participant, age, and existing functional capacity.
Recent literature on aging and physical activity has increasingly focused on needs of people over 75 years (Fiatarone, O’Neill, Ryan,
Clements, Solares, Nelson, Roberts, Kehayias, Libsitz & Evans, 1994;
Puggaard, Larsen, Stovring, & Jeune, 2000; Skelton, Young, Greig, &
Malbut, 1995; Worm, Vad, Puggaard, Stovring, Lauitsen & Kragstrup,
2001). Using Spirduso’s (1995) hierarchical approach to understanding
physical function in older people, the purpose of this article is to present
an overview of physical fitness assessment tools that can be used with
people over 75.
Based on a classification system designed to help understand the vast
strata of physical ability of people over 75 years, Spirduso (1995) categorized physical functioning of the old (75-85 years) and the oldest-old
(86-120 years) into five different levels: physically dependent, physically frail, physically independent, physically fit, and physically elite.
This hierarchy is important in gerontology, due to the wide range of
abilities of those living beyond the seventh decade of life. Briefly, using
the foundation of the assessment of living skills and resources (Williams, Drinka, Greenberg, Farrell-Holtan, Euhardy, & Schram, 1991),
Spirduso characterizes each category as follows:
Physically Dependent: Ability to pass only some basic activities of
daily living (BADLs). These activities include walking, bathing, dressing, or eating. Clearly if an individual is unable to manage these activities, they need care in either their own home or a care facility.
Physically Frail: Capable of instrumental activities of daily living
(IADLs) such as light housekeeping, food preparation, and grocery
shopping. They are competent in all BADLs, but may have problems
with some IADLs.
Physically Independent: According to Spirduso (1995), the physically independent will routinely engage in low physical demand activities such as golf, crafts, woodworking, traveling and driving. They also
have the ability to do all IADLs.
Physically Fit: Capable of doing most hobbies and competent in
moderate physical activities. They will also participate in exercise 2-3
times each week for their health and well-being.
Carr, Emes, and Rogerson
51
Physically Elite: This final group trains heavily on a daily basis with
the goal of participating in a competition. They are a rare and unique
population who may compete in marathons, Senior Olympics, and masters tournaments.
According to Spirduso (1995), these are important categories for professionals who work with the elderly because of their numerous functions: (1) to predict which individuals are in need of institutional care,
(2) understanding the type of institutionalized care that is needed, (3) to
predict future health care and long term care needs, (4) a baseline of
function in order to evaluate current programs, and (5) to help increase
life expectancy as well as quality of life.
FUNCTIONAL FITNESS TESTING PROTOCOLS
FOR OLDER PEOPLE
Tables one to six present a comprehensive overview of fitness tests
that are useful for measuring physical functional capacity in older people including those who are frail and dependent. First, however, a brief
description of those tests will be presented consistent with the standard
testing protocols. Then a matrix follows that lists each test according to
its suitability within Spirduso’s five categories.
Tests for Flexibility and Range of Motion
The Standard Sit and Reach Test: After a warm up is completed remove shoes. Sit with legs fully extended and soles of the feet flat against
a flexometer (a box with a slide ruler attached to the top). Stretch and
push the slide ruler as far forward as possible with knees straight and
hold for 2 seconds. After one practice trial, the best of three trials is recorded in cm (CSEP, 1998; Lemmink, van Heuvelen, Rispens, Brouwer, &
Bult, 2001; Morrow, Jackson, Disch, & Mood, 2000). In the Osness
(1996) protocol, the best of two test trials are recorded after two practice
trials. In the Miotto, Chodzko-Zajko, Reich, and Supler (1999) and the
Mobily and Mobily (1997) protocols, the best of four test trials are recorded. Although the standard format of this test that assesses flexibility
of the low back and hamstrings, it is more appropriate for those who are
fit or elite elderly. A popular modification that can be used more widely
across categories is the chair sit and reach test.
The Chair Sit and Reach: In this test which is better suited for independent or frail, sit on the edge of a chair and extend one leg straight out
52
ACTIVITIES, ADAPTATION & AGING
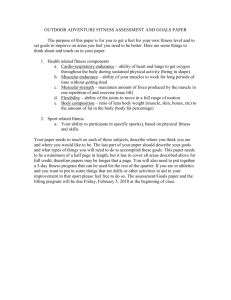
TABLE 1. Flexibility and ROM Fitness Tests for the Elderly
Test
Component Tested
Authors
CSEP, (1998)
Lemmink et al., (1995; 2001)
Miotto et al., (1999)- adapted
Mobily & Mobily, (1997)
Morrow et al., (2000)
Osness, (1996)
Sit &
Reach
Hamstring
flexibility
Chair Sit &
Reach
Hamstring
Flexibility
Morrow et al., (2000)
Rikli et al., (1998)
Back
Scratch
Upper body &
shoulder flexibility
Circumduction
Test
Shoulder
flexibility
Depend. Frail Independ.
Fit
Elite
Norms
No
No
Possibly
Yes
Yes
Norms are provided by
CSEP (but groups all
over the age of 60)
Yes
Yes
Yes
Yes
Yes
Percentile ranks are
provided by Rikli &
Jones, (1999b, 2001).
Miotto et al., (1999)
Morrow et al., (2000)
Rikli & Jones, (1999a)
Possibly
Yes
Yes
Yes
Yes
Percentile ranks are
provided by Rikli &
Jones, (1999b, 2001).
Lemmink et al., (2001)
Yes
Yes
Yes
Yes
Yes
For Self-Reporting
TABLE 2. Muscular Strength and Muscular Endurance Tests for the Elderly
Test
Component Tested
30 sec.
Lower body
Chair Stand muscular strength
& endurance
Arm Curl
Bicep muscle
strength &
endurance
Grip
Strength
Upper body
muscular strength
Leg
Extension
Test
Lower body
muscular strength
Leg Muscular
Muscular
Endurance Endurance of the
Test
Lower Body
Authors
Miotto et al., (1999)
Morrow et al., (2000)
Rikli & Jones, (1999a)
Depend. Frail Independ.
Fit
Elite
Norms
Percentile ranks are
provided by Rikli &
Jones, (1999b, 2001).
No
No
Possibly
Yes
Yes
Yes
Yes
Yes
Yes
Yes
CSEP, (1998)
Lemmink et al., (2001)
Corbin et. al., (2002)
Possibly Yes
Yes
Yes
Yes
Lemmink et al., (2001)
Possibly Yes
Yes
Yes
Yes
For Self-Reporting
Possibly
Yes
Yes
For Self-Reporting
Bravo et al., (1994)
Miotto et al., (1999)
Mobily & Mobily, (1997)
Morrow et al., (2000)
Osness, (1996)
Rikli & Jones, (1999a)-adapted
Kim and Tanaka, (1995)
Percentile ranks are
provided by
Rikli & Jones, (1999b,
2001).
Norms by CSEP, (1998)
No
No
with the foot flexed and the heel on the floor. The other leg is bent with
the foot flat on the floor. Just as in the “sit and reach” protocol, the objective is to reach as far forward at the hip joint and hold the stretch for 2
seconds. Using a ruler, measure the distance a participant can stretch
that is short of reaching the toe (minus score), reaching the toe (zero
score) or beyond the toe (plus score). Two practice trials are followed
by two test trials (Rikli, Jones, Max & Noffal, 1998; Morrow et al.,
2000).
Back Scratch: The back scratch is used as a measure of flexibility in
the shoulders and upper body. Begin in a standing position and place a
Carr, Emes, and Rogerson
53
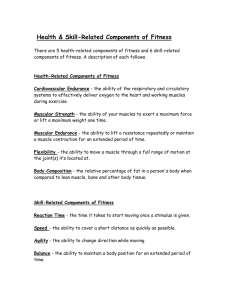
TABLE 3. Tests of Aerobic Capacity and Endurance for the Elderly
Test
Component Tested
Authors
2 Min. Step
Test
Aerobic
endurance &
lower body muscular
endurance
Miotto et al., (1999)
Morrow et al., (2000)
Rikli & Jones, (1999a)
No
Possibly
Yes
Yes Yes
3 Min. Step
Test
Aerobic
endurance & lower
body muscular
endurance
Golding et al., (1989)
No
Possibly
Yes
Yes Yes
880 m Walk
Aerobic
Endurance
Bravo et al., (1994)
Osness, (1996)
No
Possibly
Yes
Yes Yes
Peloquin et al., (1998)
No
Possibly
Yes
No
Possibly
Yes
Yes Yes
No
Possibly
Yes
Yes Yes
No
No
Yes
Yes Yes
No
No
No
Yes Yes
Calculations are
provided by ACSM,
(2000).
Possibly Yes Yes
Calculations are
provided by ACSM,
(2000).
5 Min. Walk
Aerobic
endurance &
lower body
muscular
endurance
Depend.
Frail
Independ. Fit Elite
Norms
Percentile ranks are
provided by
Rikli & Jones, (1999b,
2001).
Noms are
provided by
Goulding et al., (1989).
For Self-Reporting
6 Min. Walk
Aerobic
endurance
Morrow et al., (2000)
Peel & Ballard, (2001)
Rikli & Jones, (1999a)
9 Min. Walk
Aerobic
Endurance
Miotto et al., (1999)
Rikli & Jones (1999a)
12 Min. Walk
Aerobic
endurance
ACSM, (2000)
Sidney & Shephard,
(1977)
Bruce
Test
Aerobic
endurance
Spirduso, (1995)
ACSM, (2000)
Balke-Ware
Test
Aerobic
Endurance
ACSM, (2000)
McArdle, et al. (1991)
Spirduso, (1995)
No
No
AstrandRhyming
Test
Aerobic
Endurance
ACSM, (2000)
No
No
Can be used to calculate
Yes Yes VO2 max. The equation is
provided by Peloquin et
al., (1998).
Percentile ranks are
provided by Rikli &
Jones, (1999b, 2001).
For Self-Reporting
Yes
Yes Yes
Calculations to
determine VO2 max are
provided by ACSM,
(2000).
Calculations and tables
are provided by ACSM,
(2000).
chosen hand over the same shoulder, reaching down the middle of their
back as far as possible. The hand of the other arm is placed at the base of
the back and reaches up in an attempt to touch or overlap the fingers of
both hands. During two practice trials the preferred hand positioning is
determined and then two test trials are completed. The distance of overlap or the distance between the middle fingers is measured to the nearest
0.5 inch (1.3 cm). The best score is recorded with a minus or plus sign
included (Morrow et al., 2000; Rikli & Jones, 1999a). In the Miotto et
al. (1999) protocol, all four trials are measured and the best result is recorded.
Circumduction Test: The advantage of the circumduction test is its
adaptability to any level of flexibility in the elderly population. The
downside of this test is the complicated mathematical method of calculating a score. For this test, which also measures shoulder flexibility, the
54
ACTIVITIES, ADAPTATION & AGING
TABLE 4. Agility and Balance Tests for the Elderly
Test
Component
Tested
8 Foot up &
Go
Physical agility &
dynamic balance
Agility/
Balance
Course
Romberg
Test
Sharpened
Romberg Test
Authors
Depend.
Frail
Independ.
Fit Elite
Yes
Yes
Yes
Yes Yes
Percentile ranks are given
by Rikli & Jones, (1999b,
2001).
Yes
Yes
Yes Yes
For Self-Reporting
Yes
Yes
Yes
Yes Yes
For Self-Reporting
Miotto et al., (1999)
Morrow et al.,(2000)
Rikli & Jones, (1999a)
Rose et al., (2002)
Bravo et al., (1994)
Agility and
Mobily & Mobily, (1997) Possibly
dynamic balance
Osness, (1996)
Balance
Grahn Kronhed et al.,
(2001)
Norms
Balance
Grahn Kronhed et al.,
(2001)
Yes
Yes
Yes
Yes Yes
For Self-Reporting
1-Legged
Balance Test
Balance
Grahn Kronhed et al.,
(2001)
No
Possibly
Yes
Yes Yes
For Self-Reporting
Balance
Board Test
Balance
Lemmink et al., (2001)
No
No
Yes
Yes Yes
For Self-Reporting
Balance
Berg et al., (1992)
Worm et al., (2001)
Yes
Yes
Yes
Yes Yes
For Self-Reporting
Balance
Guralnik et al., (1994)
Yes
Yes
Yes
Yes Yes
Percentile ranks are by
Guralnik et al., (1994).
Berg Balance
Test
Tests of
Standing
Balance
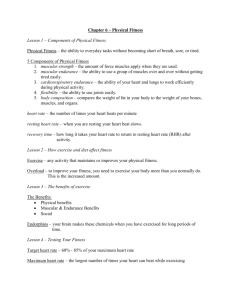
TABLE 5. Tests for Gait Assessment, Reaction Time, and Co-ordination in the
Elderly
Test
Component Tested
Authors
Gait
Assessment
Locomotor control
mechanisms
Tinetti , (1986)
Wolfson et al., (1990)
No
Yes
Yes
Yes Yes
For Self-Reporting
Reaction-Time
Test
Reaction time
Lemmink et al., (2001)
Yes
Yes
Yes
Yes Yes
For Self-Reporting
Block
Transfer Test
Manual
dexterity
Lemmink et al., (2001)
Yes
Yes
Yes
Yes Yes
For Self-Reporting
Bravo et al., (1994)
Mobily & Mobily, (1997)
Osness, (1996)
Yes
Yes
Yes
Yes Yes
For Self-Reporting
"Soda Pop"
Coordination
Test
Coordination
Depend. Frail Independ.
Fit Elite
Norms
subject uses a cord that has a fixed handle on one end and a sliding handle on the other end. According to the protocol by Lemmink et al.
(2001), the sliding handle must be adjusted so the length of the cord between the handles is equal to the participant’s shoulder width. During
the test, the subject holds both handles and brings the cord in front of the
body, over the head, and as far back as they can reach. One practice trial
is allowed followed by three test trials. To establish a score, the angle of
the arms fanning out is calculated in degrees using the formula (see
Limmink et al., 2001).
Carr, Emes, and Rogerson
55
TABLE 6. Body Composition Assessments for the Elderly
Test
Component Tested
Authors
BMI
Height &
Weight
ACSM, (2000)
Caprianica et al., (2001)
Morrow et al., (2000)
Rikli & Jones, (1999a)
Pondural Index
Height &
Weight
Waist-to-Hip Ratio
Body composition
Osness,(1996)
ACSM, (2000)
AHA, (1994)
Corbin et al., (2002)
Morrow et al., (2000)
Depend. Frail Independ.
Fit
Elite
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Norms
Percentile ranks are
given by Rikli &
Jones, (1999b,
2001).
Pondural index table
is given by Osness et
al., (1996).
A table on disease
risk is given by
ACSM, (2000).
Tests for Muscular Strength and Endurance
30-Second Chair Stand: This test is an ideal way for measuring anaerobic power, leg strength, and balance. It is easily administered to all
abilities and requires virtually no set-up. Count the number of times
within 30 seconds (score) that the participant can rise from a seated position on the chair to a full stand with arms folded across the chest
(Miotto et al., 1999; Morrow et al., 2000; Rikli & Jones, 1999a).
Arm Curl: This test measures muscular strength in primarily the biceps muscle using a hand weight (5lbs for women and 8lbs for men)
during a biceps curl through a full range of motion in 30 seconds. The
arm position for this test starts out with the thumb up (as in a handshake
grip) when the arm is at full extension. The participant then supinates
their hand during the flexion phase of the motion. The lower arm of the
subject must touch the hand of the evaluator, which has been placed on
the subject’s biceps. The maximum number of repetitions is recorded in
one trial (Bravo, Gauthier, Roy, Tessier, Gaulin, Dubois, & Peloquin,
1994; Morrow et al., 2000; Rikli & Jones, 1999a).
In the Osness (1996) protocol, the weight lifted and the hand position
are different. Women lift 4lbs and the hand remains in the “handshake
grip” position during the entire phase of the lift.
In the protocols by Miotto et al. (1999) and Mobily and Mobily
(1997) there are three trials with one-minute rest periods between. The
highest number of repetitions completed is the final score.
Grip Strength Test: There is a proven high correlation between grip
strength and upper body muscular strength (Corbin, Lindsay, Welk, &
Corbin, 2002). The grip strength test is very easy to use and is practical
for numerous functional abilities within the elderly population.
56
ACTIVITIES, ADAPTATION & AGING
This test requires a hand dynamometer calibrated to 100kg of force
that is squeezed as hard as possible with the preferred hand while standing and with the other arm down. One practice trial is allowed followed
by three test trials, each with 30 seconds of rest between and the best
score is recorded (CSEP, 1998; Lemmink et al., 2001).
Leg-Extension Strength Test: This test measures the strength of the
right quadriceps muscle. In this protocol by Lemmink et al. (2001), a
specially constructed box is used with arm supports. The participant sits
on a table with his or her legs hanging over the edge and arms resting on
the box for support. Knees must have a 90-degree flexion. A shin guard
that is wrapped around the right shin of the subject is attached to a resistance. The objective of this test is to extend the knee using maximum
strength and hold the position for 3 seconds. One practice trial is allowed followed by three test trials with 30-second rests between. The
best score is recorded in kilograms of force.
Leg Muscular Endurance Test: The participant is positioned with his
back, head, and buttocks flat against a wall. Knees are flexed to 90 degrees, thighs are parallel to the floor, and feet are set 20 cm apart. According to the protocol described by Kim and Tanaka (1995) the subject
maintains this position for as long as possible. Score is recorded in minutes and seconds.
Tests for Aerobic Fitness
2-Minute Step Test: According to Rikli and Jones (1999a), this test is
an alternative to the 5, 6, 8, 9, and 12 minute walks. This assessment is
therefore more practical for those who are unable to walk for at least 5
minutes.
The protocol for this test involves determining the number of times in
two minutes that an individual can step in place with raised knees (halfway between the iliac crest and the middle of the patella) (Rikli &
Jones, 1999a). The score is the number of right-leg steps taken in two
minutes. Miotto et al. (1999) and Morrow et al. (2000) also followed
this protocol.
3-Minute Step Test: This is a test for people who are able to step up
and down with ease. Those who have balance problems or are severely
deconditioned should be discouraged from participating in this fitness
test. In this protocol described by Golding, Myers, and Sinning (1989),
a 12-inch high box or bench is used for the stepping. Facing the bench
and in time with a metronome set at 96 beats per minute, one foot steps
up (first beat), then the second foot steps up (second beat), the first foot
Carr, Emes, and Rogerson
57
steps down (third beat), and finally the other foot steps down (fourth
beat). There is no practice as it will affect heart rate. Immediately upon
completion of a 3-minute stepping sequence, the participant sits down
so the examiner can take a full 1-minute heart rate. The heart rate is the
score for the test that is compared with a table of norms that is supplied
by Golding et al. (1989).
880 Yard Walk: This test is assessed by timing an 880-yard walk
around an indoor track (Bravo et al., 1994; Osness, 1996).
5-Minute Walk: Participants are instructed to walk as far as possible
in 5 minutes at a manageable pace around a measured track. Before
starting the test, each participant is given a marker to place on the floor
to designate where on the track she finished the test. The examiner then
counts the number of laps completed and if the final lap isn’t complete,
the distance can be measured with a measuring wheel and added to the
total number of laps completed (Peloquin, Gauthier, Bravo, Lacombe &
Billard, 1998).
6-Minute Walk: This test measures maximum distance possible in 6
minutes walking around a 50-yard track (Morrow et al., 2000; Peel &
Ballard, 2001; Rikli & Jones, 1999a).
9-Minute Walk: This test implemented by Miotto et al. (1999) is similar to the 6-minute walk protocol by Rikli and Jones (1999a). As in
other walking tests, the participants are instructed to cover as much distance as possible in 9 minutes. The final score is the total number of
yards walked to the nearest 5 yards.
The Cooper Test (12-Minute Walk): In this classic test for aerobic endurance, the participant is instructed to walk for 12 minutes (Sidney &
Shephard, 1977). Aerobic power is estimated from the walk distance
with a coefficient of variation of 10% in the men and 16% in the
women. American College Sports Medicine (ACSM) (2000) provides
calculations to determine predicted VO2 max values.
The Bruce Test: This is a commonly used treadmill protocol for determining predicted VO2 max. Due to its large increments (MET’s per
stage) every three minutes, it is better suited for those who are classified
as being physically fit or elite (ACSM, 2000). Stage one of this test will
begin with 1.7 MPH and a 10% grade. Every three minutes, the MPH
and % grade increases (ACSM, 2000; Spirduso, 1995). Calculations for
VO2 max prediction are provided by ACSM (2000).
The Balke-Ware Test: With its smaller increments (1 MET or lower
per stage), this test is more practical for use in unfit elderly populations
than the Bruce protocol. For this particular test, the speed stays set at 3.3
MPH for the duration of the test. The grade of the treadmill will gradu-
58
ACTIVITIES, ADAPTATION & AGING
ally increase each minute (ACSM, 2000). A predetermined heart rate
will be the cut-off point for this test.
In the protocol designed by McArdle, Katch, and Katch (1991) a preliminary stage was added. The test commenced with a 2-3 minute stage
at 2 MPH and a 0% grade.
Spirduso (1995) describes a protocol using 2 MPH throughout the
duration of the test with the increases in percent grade occurring every 2
minutes. She further recommends that the participant not exceed 15
minutes for the test duration
Astrand-Rhyming Test: Although this test is a popular method of assessing aerobic fitness in the general population the ACSM (2000) suggest fit elderly can also participate in this protocol. It is a cycle
ergometer test lasting 6 minutes. Average heart rates will range around
128-138 BPM. The tables and the Astrand-Rhyming nomogram needed
for calculations are provided by ACSM (2000).
Tests for Measuring Agility and Balance
8 Foot Up and Go Test: This test is particularly beneficial in predicting those who have greater risk of falling (Rose, Jones & Lucchese,
2002). It tests for agility, speed, and balance and is popular because of
the simplicity of its set up and administration. The starting position is
seated on a chair. The object is to rise up off the chair, walk 8 feet to and
around a cone, and return to sit in the chair in the quickest time possible
(Morrow et al., 2000; Rikli & Jones, 1999). There is one practice trial
and then the fastest time is recorded to the nearest tenth of a second from
the two test trials. In the Miotto et al. (1999) protocol, there are three test
trials.
Agility/Dynamic Balance Course: Osness (1996) established this
protocol for measuring dynamic balance and agility. A chair with arms
and two cones are needed. The course is set up with the chair positioned
in the center of the floor with the cones six feet to either side and five
feet back of the chair. Starting from a seated position with both feet on
the ground, at the “Ready, Go” command, the participant stands up and
moves to the right, going around the inside and to the back of the cone
(counterclockwise). She returns to the chair and must lift her feet one
half inch from the floor. Immediately following, she must repeat to the
left, once again going on the inside of the cone and around the back
(clockwise) and returning to the seated position in the chair in order to
complete one circuit. One trial consists of two circuits, therefore the
participant immediately stands up and starts the second circuit. A prac-
Carr, Emes, and Rogerson
59
tice trial is administered to determine that the protocol is well understood. Two trials are given with 30 seconds rest between them. The
better time of the two is recorded to the nearest 0.1 second (Bravo et al.,
1994; Osness, 1996). The protocol by Mobily and Mobily (1997) included three trials.
Romberg Test: The subject stands with both feet together and proceeds to open and close their eyes for 30 seconds. The examiner must
observe the postural sway of the subject and note any movement in their
stance (Grahn Kronhed, Moller, Olsson, & Moller, 2001).
Sharpened Romberg Test: Standing with the heel of one foot touching the toe of the other foot (tandem feet) the participant switches foot
position and then repeats the test again. This test is done with open and
closed eyes and once again, the examiner observes the amount of postural sway and whether or not the participant moves their feet from the
original location on the floor (Grahn Kronhed et al., 2001).
One-Legged Balance Test: The position for this test is held for a
maximum of 30 seconds as the participant stands on one leg with the opposite foot lifted halfway up the calf of the supporting leg. Once in this
position the head turns with the eyes opened and then closed. The arms
are at rest at the sides of the body. Timing is stopped if the supported
foot leaves its original position on the floor or the other foot touches the
floor. This test is then repeated on the other leg (Grahn Kronhed et al.,
2001).
Balance Board Test: This test is a more difficult balance test to administer to the elderly because it requires special equipment and it is
more challenging than other balance tests. It is not recommended for dependent and frail participants. Standing ability on balance board with
heels 15 cm apart up to 30 seconds, is tested by the examiner who stops
the timer when the board touches the floor and records the score in
terms of “counts.” One count is equal to .3 seconds and 100 counts is the
full 30 seconds. One practice trial is allowed followed by the best of
three trials (Lemmink et al., 2001).
Berg’s Balance Scale: This is a simple and reliable method for measuring physical function of those who are having problems with their
mobility. Berg’s balance test involves 14 items that are common daily
activities. Examples of tasks included in this test are the ability to pick
an object up from the floor or to sit and stand without extra support. Test
items were observed and then given a rating on a scale from 0-4 (Berg,
Wood-Dauphinee, Williams, & Maki, 1992; Worm, Vad, Puggaard,
Stovring, Lauritsen, & Kragstrup, 2001).
60
ACTIVITIES, ADAPTATION & AGING
Tests of Standing Balance: These tests include tandem, semi-tandem,
and side-by-side stands. First the stand is demonstrated by the examiner, then the participant is assisted into a position or stance. When the
participant is ready, the examiner releases his support and the timer is
started. If the feet move or if support is needed, the timer is stopped. The
test is also terminated after 10 seconds of successful standing (Guralnik,
Simonsick, Ferrucci, Glynn, Berkman, Blazer, Scherr & Wallace,
1994).
Tests for Measuring Gait, Reaction Time, and Coordination
Gait Assessment: Gait assessment is an important tool for predicting
those who are more at risk of falls. The gait in those with a history of
falls is characterized by decreased walking speed, shortened stride
lengths, and a greater variability in the length of successive steps as
compared with others (Wolfson, Whipple, Amerman, & Tobin, 1990).
A trained professional most commonly administers a gait assessment. Wolfson et al. (1990) devised a gait abnormality rating scale
(GARS) for easy use in the clinical setting. Using video cameras set in
strategic locations, the participant’s gait is recorded while she walks
along a designated path. Examiners look at 16 variables for certain patterns in foot contact, stride length, and unexpected partial losses of balance. The rating system uses a 4 point scale (0 = normal to 3 = severely
impaired) and the sum of the scores is calculated. The higher the score,
the greater the gait impairment (Wolfson et al., 1990). An assessment of
gait and movement that uses activities such as rising from a chair, turning balance, and bending down has also been documented by Tinetti
(1986).
Reaction-Time Test: This is a unique test that requires a specially designed timer (Lemmink et al., 2001). The participant holds the timer and
is responsible for responding as quickly as possible by pressing a button
when a red light shows in the timer display panel. Reaction time, measured in milliseconds, is shown on the timer.
Block-Transfer Test: This protocol for this test also requires a special
piece of equipment. Unfortunately, this complicated set up will probably have to be handmade as there is an unlikely chance that it is available for immediate purchase. Two boards are used in this test, each
having 40 holes in it (4 cm diameter, 1.1 cm depth) and 40 blocks (3.5
cm in diameter, 2.2 cm in height). Participants must move the 40 blocks
from the first to the second board in a prescribed sequence as fast as pos-
Carr, Emes, and Rogerson
61
sible and the score is recorded in seconds. A practice trial with 5 blocks
is allowed (Lemmink et al., 2001).
The “Soda Pop” Coordination Test: This test is well designed to
measure coordination and mobility of the forearm, wrist, and fingers.
Follow the set-up procedure as explained in the protocol by Osness
(1996). Seated at a table, the participant uses her preferred hand to grasp
can #1 with the thumb up. In response to the examiner’s signal, the can
is turned upside down, placing can #1 over square 2. This is followed by
can #2 being placed over square 4 and can # 3 over square 6. Immediately all three cans are returned to their original positions by grasping
the cans this time with the thumbs down. This circuit is completed two
times in one trial. Two practice trials are given and then two test trials
are recorded. The best score is recorded to the nearest 0.1 of a second
(Bravo et al., 1994; Osness,1996). Four trials are implemented in the
Mobily and Mobily (1997) protocol.
Tests for Measuring Body Composition
BMI: To determine BMI, weight in kilograms is divided by height in
meters squared (BMI = kg/m2). The value is then located on a conversion table to get a rating (ACSM, 2000; Capranica, Tiberi, Figura, &
Osness, 2001; Morrow et al., 2000; Rikli & Jones, 1999). A table, which
gives a classification of disease risk, is provided by ACSM (2000) and
another table, which gives a ranking for those 60 and older is provided
by Rikli and Jones (1999b).
Pondural Index: Body weight is measured on a calibrated scale and
height is taken with a tape measure. The weight (lbs) is noted on the
right scale and height (inches) is on the left scale. A line is drawn, connecting the two points through a center scale, which provides the results
of the Pondural Index. The score is taken to the nearest .1 of one unit. A
higher index score reveals a greater degree of leanness (Osness, 1996).
Waist-to-Hip Ratio: This simple protocol calculates the body composition risk factor. It is well known that the location of body fat can affect
an individuals’ health. Abdominal obesity has been linked with a
greater risk of health problems such as heart disease (Corbin et al.,
2002). To calculate the waist-to-hip ratio, the circumference of the
waist is divided by the hip circumference. Ratios greater than 1.0 for
men and .80 for women have been shown to have high correlations with
higher risks of CHD, stroke, breast cancer, and death (AHA, 1994;
Corbin et al., 2002; Morrow et al., 2000). According to the ACSM
62
ACTIVITIES, ADAPTATION & AGING
(2000) for those aged 60-69, men who have ratios of 1.03 and women
who are at or above .90 are considered to be at a very high risk of health
problems. The ACSM (2000) has also recently shifted more focus on
just the waist circumference alone as being an indicator of health since
abdominal obesity is the main issue.
HIERARCHY OF PHYSICAL FUNCTION
AND FUNCTIONAL FITNESS TESTS
Following is the matrix of fitness tests in relation to Spirduso’s physical function hierarchy. Each test is evaluated according to its appropriateness for use within the hierarchy of elite, fit, independent, frail, and
dependent levels of physical function. The sources for the protocols as
well as the availability of norms are reported.
It is important to note the need for more research on testing functional fitness in the diverse older population. It is also important to caution that not all tests are appropriate for everyone within a certain
functional category. Individual needs vary, for example, the sit and
reach test is contraindicated for people with oesteoarthritis regardless of
their functional level. The matrix provided here offers recommendations that are tempered by potentially complicating health issues. Simplicity is key to successful administration of a test therefore unusual or
complicated equipment like that used in the reaction time tests reduces
their utility. With the greater knowledge in assessing and measuring
physical performance in older people, more understanding can be generated on how to reduce the loss of function in the later years.
Tables 1-6 offer health professionals in various settings several fitness testing options. These environments can include long-term care facilities, home care, community fitness centers, and clinical settings.
Each of these environments cater to a range of abilities within Spirduso’s
(1995) classification system. For professionals who are working in
these settings, periodic testing can provide valuable information about
the stability of a person’s functional ability. Declining performance
may suggest loss of functional ability, strength, or endurance. Such loss
may be an early signal for increased risk of falling or the need for higher
levels of care. Therefore testing batteries are suggested in relation to
program settings:
Carr, Emes, and Rogerson
63
1. Long term care facilities: The population within this setting are
commonly those who are classified as physically frail or dependent. Nurses, physiotherapists, occupational and recreational therapists may therefore choose tests applicable to this population such
as the Circumduction Test, Soda Pop Coordination Test, and
Tests of Standing Balance to assess balance, flexibility, and coordination.
2. Home care: Physically frail individuals often require this type of
assistance. Nurses and home care providers may choose the Berg
Balance Test, 30-Second Chair Stand, and Chair Sit and Reach.
All of these tests are easy to administer with little or no specialized equipment.
3. Community Fitness Programs: This population includes primarily
the physically elite, fit and independent individuals who may be
participating in programs offered at a recreational center, senior
center, or community center. Kinesiologists, certified fitness
trainers, and day program leaders have the option of conducting
more advanced testing such as Body Composition (BMI or waist
to hip ratio), 6-Minute Walk, and the Standard Sit and Reach Test.
4. Clinical settings: Physically fit, elite, and independent individuals
who see kinesiologists, physiotherapists, occupational therapists,
and nurses in a clinical setting generally have access to more sophisticated equipment therefore more advanced testing procedures can be applied such as Gait Assessment, Bruce Test, and
Balance Board Test.
These tests are highly reliable and valid provided there is tester consistency when administering these protocols. Many require little training and can be efficiently administered in a variety of settings. The
tester should also consider that there may be contraindications limiting
certain individuals from participating in certain tests. Pre-screening
measures must be taken to determine testing suitability.
It is also important to note the need for more research on testing functional fitness in our diverse older population. The tables provided here
offer professionals an assortment of recommendations. The benefits of
periodic testing include the evaluation of current programming, prediction of future health care requirements, and selecting the next course of
action to meet an individual’s needs. This will generate a greater knowledge of physical function in the elderly populations, improve quality of
life and reduce the loss of function in later years.
64
ACTIVITIES, ADAPTATION & AGING
REFERENCES
ACSM. (2000). ACSM’s guidelines for exercise testing and prescription (6th ed.). Baltimore, MD: Lippincott Williams & Wilkins.
American Heart Association. (1994). Heart and stroke facts. Dallas: AHA.
Berg, K.O., Wood-Dauphinee, S.L., Williams, J.I., & Maki, B. (1992). Measuring balance in the elderly: Validation of an instrument. Canadian Journal of Public
Health, 83 (suppl. 2), 7-11.
Bravo, G., Gauthier, P., Roy, P., Tessier, D., Gaulin, P., Dubois, M., & Peloquin, L.
(1994). The functional fitness assessment battery: Reliability and validity data for
elderly women. Journal of Aging and Physical Activity 2 (1), 67-79.
Capranica, L., Tiberi, M., Figura, F., & Osness, W. (2001). Comparison between
American and Italian older adult performances on the AAHPERD functional fitness
test battery. Journal of Aging and Physical Activity, 9 (1), 11-18.
Corbin, C., Lindsey, R., Welk, G., & Corbin, W. (2002). Concepts of fitness and
wellness. (4th ed.). Toronto: McGraw-Hill.
CSEP. (1998). The Canadian physical activity fitness & lifestyle appraisal: CSEP’s
plan for healthy active living (2nd ed.). Ottawa: CSEP.
Fiatarone, M. A., O’Neill, E.F., Ryan, N.S.D., Clements, K.M., Solares, G.R., Nelson,
M.E., Roberts, S.B., Kehayias, J.J., Libsitz, L.A., & Evans, W.J. (1994). Exercise
training and nutritional supplementation for the physical frailty in very elderly people. New England Journal of Medicine, 330, 1769-1775.
Golding, L.A., Myers, C.R., & Sinning, W.E. (1989). Y’s way to physical fitness: The
complete guide to fitness testing and instruction (3rd ed.). Human Kinetics: Champaign, IL.
Grahn Kronhed, A., Moller, C., Olsson, B., & Moller, M. (2001). The effect of
short-term training on community-dwelling older adults. Journal of Aging and
Physical Activity, 9 (1), 19-31.
Guralnik, J.M., Simonsick, E.M., Ferrucci, L., Glynn, R.J., Berkman, L.F., Blazer,
D.G., Scherr, P.A., & Wallace, R.B. (1994). A short physical performance battery
assessing lower extremity function: Association with self-reported disability and
prediction of mortality and nursing home admission. Journal of Gerontology, 49
(2), M85-M94.
Kim, H.S., & Tanaka, K. (1995). The assessment of functional age using “Activities of
Daily Living” performance tests: A study of Korean women. Journal of Aging and
Physical Activity, 3 (1), 39-53.
Lemmink, K.A.P.M., van Heuvelen, M.J.G., Rispens, P., Brouwer, W.H., & Bult, P.
(1995). The Groningen fitness test for the elderly: Composition and application in
large-scale fitness events. In Harris, S., Heikkenen, E., & Harris, W.’s Physical Activity, Aging and Sports. Albany, NY: Center for the Study of Aging.
Lemmink, K.A.P.M., Han, K., de Greef, M.H.G., Rispens, P., & Stevens, M. (2001).
Reliability of the Groningen fitness test for the elderly. Journal of Aging and Physical Activity, 9 (2), 194-212.
McArdle, W.D., Katch, F.I., & Katch, V.L. (1991). Exercise physiology (3rd ed.).
Malvern, PA: Lea & Febiger.
Carr, Emes, and Rogerson
65
Miotto, J. M., Chodzko-Zajko, W., Reich, J., & Supler, M.M. (1999). Reliability and
validity of the Fullerton functional fitness test: An independent replication study.
Journal of Aging and Physical Activity, 7, 339-353.
Mobily, K.E., & Mobily, P.R. (1997). Reliability of the 60+ functional fitness test battery for older adults. Journal of Aging and Physical Activity, 5 (2), 150-162.
Morrow, J.R. Jr., Jackson, A.W., Disch, J.G., & Mood, D.P. (2000). Measurement and
evaluation in human performance (2nd ed.). Champaign, IL: Human Kinetics.
Osness,W. H. (1996). Functional fitness assessment for adults over 60 years: A field
based assessment (2nd ed). Dubuque, IA: Kendall/Hunt Publishing.
Peel, C., & Ballard, D. (2001). Reproducibility of the 6-minute-walk test in older
women. Journal of Aging and Physical Activity, 9 (2), 184-193.
Peloquin, L., Gauthier, P., Bravo, G., Lacombe, G., & Billard, J.S. (1998). Reliability
and validity of the five-minute walking field test for estimating VO2 peak in elderly
subjects with knee osteoarthritis. Journal of Aging and Physical Activity, 6, 36-44.
Puggaard, L., Larsen, J.B., Stovring, H., & Jeune, G. (2000). Maximal oxygen uptake,
muscle strength and walking speed in 85 year-old women: Effects of increased
physical activity. Aging, Clinical, and Experimental Research, 12, 1-10.
Rikli, R., & Jones, J. (1998). The reliability and validity of a 6-minute walk test as a
measure of physical endurance in older adults. Journal of Aging and Physical Activity, 6 (4), 363-375.
Rikli, R., Jones, J., Max, J., & Noffal, G. (1998). The reliability and validity of a chair
sit-and-reach test as a measure of hamstring flexibility in older adults. Research
Quarterly for Exercise and Sport, 69 (4), 338-343.
Rikli, R. & Jones, J. (1999a). Development and validation of a functional fitness test
for community-residing older adults. Journal of Aging and Physical Activity, 7,
129-161.
Rikli, R. & Jones, J. (1999b). Functional fitness normative scores for community-residing older adults, ages 60-94. Journal of Aging and Physical Activity, 7, 162-181.
Rikli, R. & Jones, J. (2001). Senior Fitness Test Manual. Champaign, IL: Human Kinetics.
Rose, D.J., Jones, C.J., & Lucchese, N. (2002). Predicting the probability for falls in
community residing older adults using the 8-Foot Up-and-Go: A new measure of
functional mobility. Journal of Aging and Physical Activity, 19, 466-475.
Skelton, D.A., Young, A., Greig, C.A., & Malbut, K.E. (1995). Effects of resistance
training on strength, power and selected functional abilities of women aged 75 and
older. Journal of the American Geriatrics Society, 43, 1081-1087.
Spirduso, W.W. (1995). Physical Dimensions of Aging. Champaign, IL: Human Kinetics.
Tinetti, M.E. (1986). Performance-oriented assessment of mobility problems in elderly
patients. Journal of the American Geriatrics Society, 34, 119-126.
Williams, J.H., Drinka, T.J.K., Greenberg, J.R., Farrell-Holtan, J., Euhardy, R., &
Schram, M. (1991). Development and testing of the assessment of living skills and
resources (ALSAR) in elderly community-dwelling veterans. The Gerontologist,
31, 84-91.
66
ACTIVITIES, ADAPTATION & AGING
Wolfson, L., Whipple, R., Amerman, P., & Tobin, J.N. (1990). Gait assessment in the
elderly: A gait abnormality rating scale and its relation to falls. Journal of Gerontology, 45, M12-19.
Worm, C. H., Vad, E., Puggaard, L., Stovring, H., Lauitsen, J., & Kragstrup, J. (2001).
Effects of a multicomponent exercise program on functional ability in community-dwelling, frail older adults. Journal of Aging and Physical Activity, 9 (4),
414-424.
RECEIVED: 01/03
REVISED: 06/03
ACCEPTED: 09/03
For FACULTY/PROFESSIONALS with journal subscription
recommendation authority for their institutional library . . .
If you have read a reprint or photocopy of this article, would you like to
make sure that your library also subscribes to this journal? If you have
the authority to recommend subscriptions to your library, we will send you
a free complete (print edition) sample copy for review with your librarian.
1. Fill out the form below and make sure that you type or write out clearly both the name
of the journal and your own name and address. Or send your request via e-mail to
getinfo@haworthpress.com including in the subject line “Sample Copy Request” and
the title of this journal.
2. Make sure to include your name and complete postal mailing address as well as your
institutional/agency library name in the text of your e-mail.
[Please note: we cannot mail specific journal samples, such as the issue in which a specific article appears.
Sample issues are provided with the hope that you might review a possible subscription/e-subscription with
your institution's librarian. There is no charge for an institution/campus-wide electronic subscription
concurrent with the archival print edition subscription.]
Please send me a complimentary sample of this journal:
(please write complete journal title here–do not leave blank)
I will show this journal to our institutional or agency library for a possible subscription.
Institution/Agency Library: ______________________________________________
Name: _____________________________________________________________
Institution: __________________________________________________________
Address: ___________________________________________________________
City: ____________________ State: __________ Zip: ____________________
Return to: Sample Copy Department, The Haworth Press, Inc.,
10 Alice Street, Binghamton, NY 13904-1580