When to Watch, When to Refer, When to Reassure
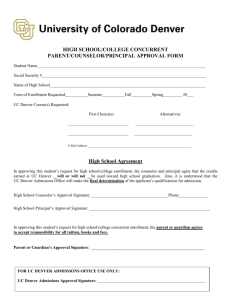
advertisement

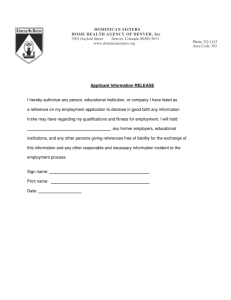
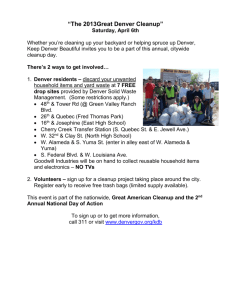
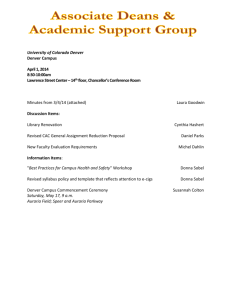
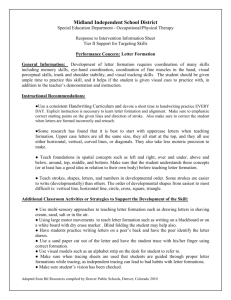
When to Watch, When to Refer, When to Reassure Case Authors: Emily Jean Davidson MD Carolyn Frazer, MD Harvard Medical School Children’s Hospital, Boston Case Advisor: William Frankenburg, MD University of Colorado School of Medicine Topic: Using the Denver Developmental Screening Test II (DENVER II) Abstract: Developmental delay is one of the most common childhood problems with a prevalence of 10%. Effective treatments including Early Intervention and special education are available for children with developmental delays. Therefore, clinicians need to be able to identify developmental delays early on and make appropriate referrals for further evaluation and treatment. The Denver Developmental Screening Test II (DENVER II) has been widely used in clinical practice, is easy to learn to administer and score, and provides a structured approach to developmental assessment in the office setting. This educational exercise includes eight brief case descriptions that provide an introduction to using the DENVER II to screen children for developmental delay. Discussion includes initial management and indications for further evaluation of children with delay. Goal: To improve clinical skills in administering and interpreting the DENVER II. Objectives: As a result of this training, clinicians will learn: 1. To monitor and record developmental observations using the DENVER II. 2. To score and interpret results of the DENVER II. 3. To recognize normal and abnormal patterns of development in children under age 6 years through use of this standardized tool. 4. To develop an initial management plan for children with suspected developmental delay. Pre-requisite Cases: N/A Related Cases: "Will David Catch Up?" (Global Delay) "The Tongue Tied Toddler" (Language Delay) "Jose's New Family" (Atypical Behaviors, Developmental Delay) Themes: Child Development and Behavior Key Words: Child development, Denver II, developmental screening, language delay, early intervention, special education Supported by a grant from The Genentech Foundation for Growth and Development. These materials may be freely reproduced, but may not be modified without written consent of the authors. Bright Futures Core Concepts: While all of the Core Concepts are included in each case, this particular case can be used to highlight communication, partnership, advocacy, and prevention/health promotion. Materials Provided: • Facilitator's Guide (including answer key and discussion for each case and teaching tips) • 8 Case vignettes with DENVER II results • Handout #1: How to perform the DENVER II • Handout #2: Early Intervention and School Referral • Bibliography Preparation for the Session: Facilitators should thoroughly review this guide and the other materials provided. The DENVER II Test forms and DENVER II Test Kit, as well as training materials including The DENVER II Training Videotape (Introduction), The DENVER II Item Administration Videotape, The DENVER II Training Manual, and The DENVER II Technical Manual, may be purchased directly from: Denver Developmental Materials, Inc. PO Box 6919 Denver, CO 80206-0919 Tel. 1-800-419-4729 The training materials should be reviewed by the teacher and may be given to students before or between teaching sessions. Overview of Format for Two 1-Hour Sessions (or a single 2-hour session): We anticipate that case facilitators will modify implementation of the case sessions to best fit their educational setting and learners. For detailed recommendations on case facilitation, please see the chapter entitled, “A Brief Guide to Facilitating Case-Discussion,” found in The Case Teaching Method; and Growth in Children and Adolescents (book 1 of this series). First hour: 1. Discussion of DENVER II basics. (30 minutes) 2. Live/video demonstration of DENVER II with a child. The demonstration of the DENVER II with a live child or children has been very popular with residents and medical students. Volunteer children can often be found by asking seminar participants who are parents to bring one of their children along to the session. Using an older (4-6 year old) child to demonstrate items may get better cooperation in front of the group. (15-30 minutes) 3. Practice item administration not covered during child’s demonstration. (0-15 minutes) Between sessions: 1. Participants should read the DENVER II manual and/or watch the training video on item administration. 2. Participants should be asked to practice administering the DENVER II. If possible, this should be done under the supervision of an experienced clinician. Second hour: 1. Begin by asking participants about their experiences practicing the DENVER II and any questions remaining about administering it. (5 min) 2. Review key concepts that have not already been covered during the discussion. (5 min) 3. Lead the group in scoring the DENVER II for each case using an overhead projector. A brief discussion on interpreting the results should follow. More cases may be covered if time permits, however, mini-cases 1-4 should be covered with each group. Detailed Teaching Tips Session 1: 1) Session format: a) Didactic teaching session on performing DENVER II (30 minutes) b) Demonstration with child (15-30 minutes) c) Continued demonstration of items for remainder of session 2) Materials needed: a) Session 1: Denver Basics b) Handout #1: How to perform the Denver II c) Blank DENVER II forms for all students d) Overhead transparencies of pages 14, 15, 16 from DENVER II training manual e) Copy of blank DENVER II on an overhead transparency f) Denver kit (preferably a few kits) 3) Preparation for session: a) Review “Session 1: Denver Basics” and Handout #1. b) Review DENVER II training manual and DENVER II item administration video. c) Read through teaching materials and read selected references. d) Invite child for demonstration (preferably 2 children of different ages). 4) Running the session: a) Introduction: Begin the session by asking learners what they know about the DENVER II and what they would like to learn. Then present background information on the DENVER II in question-and-answer format to help elicit learner participation. The background portion of the talk needs to be completed efficiently and should not take more than 10 minutes. b) Basic Instruction: The section on the basics of performing the DENVER II should take at least 20 minutes. • Begin this part by distributing Handout #1. • Pass around the items in the kit as they are discussed. • Show the age calculations on the board or an overhead. • Demonstrate drawing the age line on an overhead transparency of a DENVER II. • Refer to the overhead transparencies of pages 14-16 of the DENVER II to explain interpretation. c) Demonstration: The demonstration with a live child draws students in very effectively. It is helpful to invite two children of different ages. It is especially nice to have an older child with whom you can demonstrate not only the age-appropriate items but items appropriate for a younger child as well. Letting the child play quietly in a corner of the room during the didactic session can help the child relax and be comfortable with the people in the room before the demonstration begins. If the child refuses at the last minute, a video demonstration can be substituted or the facilitator can ask a learner to role-play as a child. Once the child has done as much as possible, the facilitator can continue to demonstrate item administration with learners. Have an observer time the administration of the DENVER II. Learners are often surprised at how little time it takes to complete. d) Practice: At the end of the session, ask learners to practice performing the DENVER II at least once or twice on their own patients (or other children) before the next session. Ideally, this practice should take place under the supervision of a clinician experienced in the administration of the DENVER II who can provide individualized instruction and feedback. In addition, learners should read the DENVER II manual and watch the item administration video. Session 2: 1) Session format: a) Review of student experiences with practice DENVER II (5 minutes) b) Review of key concepts not covered in above discussion (5 minutes) c) Use of cases to demonstrate interpretation of findings (30-50 minutes) 2) Materials needed: a) Handout #1: How to Perform the DENVER II (extra copies for learners) b) DENVER II manual for reference c) Handout #2: Early Intervention and School Referral (extra copies for learners) d) Create 4 overhead transparencies of blank DENVER II sheets (and overhead projector). e) Create overhead transparencies of cases 1-4 and 5-8 (optional) f) Denver kit 3) Preparation for session: Review DENVER II materials as for session 1. 4) Running the session: There are several ways to use the 8 case vignettes to teach learners about interpreting the DENVER II. a) The facilitator may ask a student to administer the test while he/she acts as the child in the vignette. Have the group participate in making the age line and score each item demonstrated on the blank DENVER II overhead. Once the DENVER II is complete, discuss interpretation and further evaluation. b) Show the overhead of the completed DENVER II with case vignette and discuss the interpretation and appropriate further management. c) Hand out the cases with completed DENVER II. Learners can spend 10-15 minutes reading and interpreting them independently before discussing them as a group. Guiding Questions for Discussion: For each brief case description and accompanying DENVER II record form, the following two questions should be discussed by the group: 1. What is your interpretation of the DENVER II for this case? 2. What is your next step? This facilitator’s guide contains the answers to the above questions and a brief discussion guide for each DENVER II case vignette. Facilitators may wish to copy some of these and distribute to the learners after the case is discussed. Session 1: Denver Basics Overview: This information should be presented during the first hour of a two-hour unit on using the Denver Developmental Screening Test-II in clinical practice. The first hour will include a presentation of basic information about administering and scoring the DENVER II, followed by a demonstration with a volunteer child. Whenever possible, facilitators should encourage group discussion. The second hour will utilize mini-cases to focus on scoring and interpretation of DENVER II results, recognition of developmental problems, and making appropriate referrals. I: Background Primary care visits provide a unique opportunity for ongoing developmental surveillance. However, without a structured format for developmental screening, identifying children with delays is difficult for even the most experienced clinician. The Denver Developmental Screening Test was first published in 1967. It has since been used on more than 50 million children worldwide.4 In 1990, it was revised to include more language items, two new articulation items, a new age scale, a new category of item interpretation to identify milder delays, a behavioral rating scale, and new training materials. The revised DENVER II was re-normed using a more diverse population of 2,000 children.3 What functional areas does the DENVER II assess? The DENVER II consists of 125 items assessing four areas of functioning: 1. Personal-Social (relating to people and caring for personal needs) 2. Fine Motor-Adaptive (eye-hand coordination, manipulation of small objects and problem solving) 3. Language (hearing, understanding and using language) 4. Gross Motor (sitting, walking, jumping and overall large muscle coordination) For what age child is the DENVER II designed? The DENVER II is designed for children from birth to 6 years of age. The Committee on Children with Disabilities of the American Academy of Pediatrics recommends administering it at every well child check.5 How should the DENVER II be used? The DENVER II is a screening test and as such, should be used as part of routine developmental surveillance to identify children with areas of concern. Children with potential concerns should undergo further evaluation. The DENVER II is not an intelligence or IQ test, a predictor of future ability or a diagnostic tool. Although the results may suggest certain problems or diagnoses, the DENVER II alone should never be used to make a diagnosis. Is the DENVER II the only developmental screening test available? No. There are several other developmental screening tests including the Clinical Adaptive Test/Clinical Linguistic and Auditory Milestone Scale (CAT/CLAMS),6 Early Language Milestones (ELMS), the Battelle Developmental Inventory Screening test, and The Screening Children for Related Early Educational Needs (SCREEN).7 Is the DENVER II alone sufficient for screening child behavior and development? The DENVER II alone is not enough. Other strategies for obtaining developmental information: 1. Elicit parental concerns. There is a very high correlation between parental concern and presence of developmental delay. This is especially true of language delay.10 2. Ask open-ended questions. Good examples of these questions, specific to the age of the child, can be found in the Bright Futures Guidelines for Health Supervision. 3. Observe and interact with the child throughout the interview and exam process. 4. Consider asking parents to keep records of behavior at home. 5. Obtain reports from daycare providers, teachers and other professionals working with the child. Why is developmental screening important? What is the value of identifying children at risk for developmental delay? Knowing how to assess a child at risk for developmental delay allows the clinicians to intervene and enhance the care they provide. Amendments to the Individuals with Disabilities Education Act, enacted in 1992, require that children age 3 and over who have disabilities receive services through the public school system. For children under 3 years, each state runs Early Intervention services, often through the Department of Public Health. These services are funded through private insurance and public funds. There is no direct cost to the family. Early Intervention has explicit criteria for entry but any child can be referred by physician, teacher, or parent for evaluation (See Handout #2: Early Intervention and School Referral) . By understanding these criteria and how to screen for them, clinicians become better equipped to offer their patients these available resources. Session 2: Discussion Guide Case 1 Josephina is an 18-month old former 27-week premature girl whom you have followed since her discharge from the neonatal intensive care unit. Her NICU course was notable for a Grade III intraventricular hemorrhage, respiratory distress syndrome, intubation for 3 weeks, and mild residual bronchopulmonary dysplasia. She was receiving services from Early Intervention, but these were discontinued at her first birthday because “She was doing so well.” Question 1: What is your interpretation of the DENVER II for this case? Answer: (b) suspect Key Teaching Points: Josephina has two cautions (scribbles, and walk well) and one delay (thumb finger grasp) on her testing. Question 2: What is your next step? Answer: (c) Refer to Early Intervention Discussion: Ongoing developmental surveillance of at-risk children is crucial. Your background information tells you that Josephina was premature and had an intraventricular hemorrhage, this puts her at risk for cerebral palsy. The most common type of cerebral palsy in premature infants is spastic diplegia. Although the lower extremities are most involved, fine motor control can be problematic as well. Josephina’s fine and gross motor delays merit further evaluation. A referral to Early Intervention can lead to a more in depth evaluation of fine motor, gross motor and cognitive skills and appropriate treatment can be instituted. In addition, referrals to neurology and orthopedics should be considered. (See Handout #2: Early Intervention and School Referral). Case 2 Jimmy is a 12-month old boy who is new to your practice. His clinic record indicates that he has not been seen for a well child visit since he was 6 months old. The last immunizations he received were his “4 month shots.” His mother, Isabel reports that his 10 year old brother provides much of Jimmy’s care. During his physical exam, you observe that he has not been washed recently. During the Denver II, Isabel reports “I never gave him a cup - he loves the bottle.” When asked if Jimmy imitates, she asks, “What do you mean?” Jimmy looks confused when you try to play ball with him, although he does reach up to be held. Question 1: What is your interpretation of the DENVER II for this case? Answer: (a) normal Key Teaching Points: Jimmy has only one caution (wave bye-bye) and no delays. Question 2: What is your next step? Answer: (b) Referral to social services (c) A referral to EI is also an acceptable plan. Discussion: While the results of the Denver II per se do not suggest developmental delay, you make some observations that raise concerns about Jimmy’s home situation. Missing several primary care visits, having care provided by a 10 year old, and poor hygiene all raise concerns about the resources available to Jimmy’s mother and the safety of the home situation. The types of tasks Jimmy is unable to perform raise concerns about whether he has adequate opportunity for developmental stimulation. This family should have further evaluation and support provided by a social services consultation. Where social services are not available, the clinician will need to undertake this investigation himself or herself. Questions to consider include the following. What is the housing situation? Does Isabel have sufficient money to buy food, clothing and diapers? Is an alternative child care arrangement possible? Does Isabel need help with parenting skills? A referral to Early Intervention services may provide access to parent support groups, parent training, etc. (Teachers should include information on resources provided by their home state. For example, the Massachusetts Society for the Prevention of Cruelty to Children has parenting classes and can provide support. Women and Infants with Children (WIC) can provide funding for groceries if Isabel meets the financial criteria.) Case 3 Daniel is a 2-year old boy who has been in your office at least 5 times this winter for otitis media. Otherwise, he has been quite well. His mother, Sandra, reports that “he is a delightful, friendly kid who gets along great with his brother and sisters and Brandy, our Golden Retriever.” She notes, “Daniel is my quiet one, he talks less than the others but of course they always talk for him.” You ask Daniel some questions and he smiles at you but his speech is very difficult to understand. You rely on Sandra to translate for him. Question 1: What is your interpretation of the DENVER II for this case? Answer: (b) Suspect. Daniel has 2 cautions (body parts, point 2 pictures). Question 2: What is your next step? Answer: (a) Further medical evaluation Discussion: Language delay is the most common form of developmental delay, occurring in up to 5-10% of preschoolers. Daniel’s current language skills are significantly delayed based on your brief history and observation. By two years of age, a child should have a large expressive vocabulary (over 200 words), use two or three word combinations to communicate, point to several body parts, use “no” and express a question through rising intonation. Despite parental reports that a child “understands everything,” many children with language delay may rely on visual or situational cues to understand. Parents may unknowingly simplify language by breaking commands into single steps or repeating directions frequently. Clinical impressions of hearing status are often inaccurate. Children with more mild hearing loss may use visual cues to aid comprehension and thus not appear hearing impaired. Hearing loss, particularly before age 5 years, impacts significantly on language development. Even fluctuating, mild to moderate conductive hearing loss related to serous otitis media may affect acquisition of language in the younger child. All children with suspected language delay should have a formal hearing evaluation to rule out any hearing loss contributing to the language delay. There are several types of tests available: Tympanometry: assesses ear drum mobility and middle ear pressure; helpful in diagnosing middle ear effusion; does not assess hearing. Behavioral audiometry: may be used in children 6 months and older; visual reinforcement technique where sound presented in sound room, reinforcement (often a toy or puppet) appears if infant or child correctly turns to sound source. Pure tone audiometry: evaluates hearing over the range of frequencies most critical for speech (250 8000 Hz); headphones used to assess hearing in each ear separately. Brainstem evoked auditory response: electrophysiological test used to assess sensorineural hearing loss; examines hearing over all components of the neural pathway. After, or concomitant with, the audiologic evaluation, Daniel should have a speech and language assessment. This may be performed through Early Intervention or through the speech/language department at the local medical center. Speech and language therapy, which Daniel is likely to need, is usually provided as well by the Early Intervention Program. Although this presentation suggests isolated language delay secondary to hearing loss, it is also important to obtain a comprehensive developmental evaluation to be sure that other areas of development are not affected. Language development is a better predictor of cognitive development than is motor development, and “speech delay” is the most common presenting complaint for global developmental disorders. In addition to isolated delay in language development, the differential diagnosis for speech delay includes global developmental delay, mental retardation, pervasive developmental disorder/autism, and impoverished environment or neglect. Case 4 Eleanor is a 3-year-old girl who is new to your clinic. Her mother, Susan, reports that she is healthy but that “She is still not interested in potty training.” Eleanor has been in a playgroup but seems to prefer playing by herself. She is unable to name a friend other than “Mommy.” She does not point to the pictures but smiles and repeats “meow” when you asks “which one says meow.” Despite multiple demonstrations, Eleanor cannot stand on one foot. After completing a tower of 5 blocks, she looks at both you and her mother, claps and laughs. Question 1: What is your interpretation of the DENVER II for this case? Answer: (b) Suspect Key Teaching Points: Eleanor has 3 delays (tower of 6 cubes, point 4 pictures, body parts) and 9 cautions (name friend, tower of 8 cubes, imitate vertical line, know 2 adjectives, know 2 actions, name 4 pictures, speech ½ understandable, balance each foot 1-second, broad jump). Question 2: What is your next step? Answer: (a) Refer for a school-based evaluation Discussion: This profile is concerning with delays in fine motor adaptive and language skills and cautions in all domains. There has been no loss of milestones, and Eleanor is sociable and interactive (only cautions in the personal-social domain). This profile is more consistent with a global developmental delay and less consistent with Pervasive Developmental Disorder or Autism. Eleanor should be referred for a schoolbased evaluation. The evaluation should include cognitive, speech and language, and occupational therapy assessments. (See Handout #2: Early Intervention and School Referral). If a thorough medical and developmental history, family history, and physical examination indicate concerns for other medical problems, these should be pursued as well. Hearing and vision tests should be performed and other diagnostic testing (such as electroencephalogram or chromosomes) may be indicated. Mental retardation cannot reliably be diagnosed before age 3. After age 3, intelligence tests such as the Wechsler Intelligence Scale for Children—Revised (WPPSI-R, 1989, The Psychological Corporation, San Antonio, TX) can be used to assess cognitive functioning. Although cognitive testing in pre-school children can be helpful, testing performed in school age (5-7 years) children is more predictive of long term functioning. To be diagnosed with mental retardation, a child must have impairment in adaptive or functional skills in addition to impairment in cognitive skills. Adaptive skills can be quantified using the Vineland Adaptive Behavior Scales (Sara S. Sparrow, David A. Balla, and Domenic V. Cicchetti, 1984, American Guidance Service, Inc. Circle Pines, MN) (Please see the case: “Will David Catch Up?” for a more extensive discussion of global developmental delay). Case 5 Shenika is a 4 year old girl who presents for her preschool screening visit. Her older sister Sharde was followed by you in the past for lead poisoning. Shenika comes right into the exam room, sits down in the chair next to you and asks, “Are you my doctor? Are you going to check my heart?” Shenika’s mother Jackie laughs and states that Shenika “is always talking!” She reports that Shenika loves to fix her own breakfast, dresses herself and loves to play “Chutes and Ladders” with Sharde. While you are taking the history, Shenika stacks the blocks and sings her ABCs. She tells you her favorite color is purple and she begins pointing at different colors around the room and tells you that the tiles in your office are “salmon.” You attempt to administer a Denver II, but Shenika refuses activities or laughs and says, “I’m not gonna tell you!” You are able to observe her during the visit, and gather some information by history from Jackie. Question 1: What is your interpretation of the DENVER II for this case? Answer: Untestable Question 2: What is your next step? Answer: (e) Reassure parent, rescreen on next visit. Discussion: The DENVER-II manual indicates that Shenika should be retested in 1- 2 weeks. However, several features of her presentation suggest that this would be unnecessary. She passes all items in the personal-social domain and she can do an advanced item in the fine motor domain (drawing a person with 6 parts). Although she refuses to wiggle her thumb, her success with the advanced drawing items makes this less concerning. Although she refuses several language items, she was able to name one color before beginning the Denver II. She refused many items in the gross motor section but her mother reports that she does these at home. Thus, it would be reasonable to wait for her next visit to retest. Case 6 Jacob comes for his 2-year visit. His mother Anna’s biggest concern is that “Jacob has terrible temper tantrums and doesn’t talk as much as his sister did at his age.” Anna’s parents have told her not to worry because the temper tantrums are part of “the terrible twos” and “because you spoil him.” Jacob makes screeching noises but does not use any words in the office. Anna reports that he struggles when she brushes his hair or tries to dress him. He does not throw the ball you offer, however he does nearly hit you in the head when he throws a toy overhand. He jumps up and down and flaps his hands. Question 1: What is your interpretation of the DENVER II for this case? Answer: (b) Suspect Key Teaching Points: Jacob has 10 delays (feed doll, help in house, tower of 4 cubes, tower of 2 cubes, dump raisin demonstrated, put block in cup, body parts, name 1 picture, combine words, point 2 pictures, 6 words) and 5 cautions (brush teeth with help, put on clothing, tower of 6 cubes, speech ½ understandable, point 4 pictures). Question 2: What is your next step? Answer: (c) Referral to Early Intervention (a) Further medical evaluation is also an acceptable plan. Discussion: Jacob manifests delays in personal-social, fine motor, and language skills. Beyond the delays noted on the DENVER II, there are several features to Jacob’s presentation that suggest a significant problem. He shows difficulty with socially oriented skills, including dressing and tooth brushing. He does not follow commands well and he has stereotyped or atypical behaviors such as hand flapping. This profile is suggestive of a child with Pervasive Developmental Disorder (PDD) or Autism. PDD is used to describe a spectrum of disorders characterized by language delay, impairment in social interaction, and stereotyped or atypical behaviors. The diagnosis of PDD requires further developmental assessment including speech and language and cognitive testing. In addition, further medical work-up may be indicated such as metabolic testing, Fragile X testing, or EEG to rule out Landau-Kleffner syndrome (acquired epileptic aphasia). Early Intervention services can perform the developmental testing and so a referral to EI would be a good first step. (See Handout #2: Early Intervention and School Referral for more information). However, referral to a medically based developmental team may be necessary. In addition, a thorough physical examination and past medical and family history should be obtained. A child who is diagnosed with PDD/autism will need intensive educational services. The program should include speech/language therapy, and general development and behavioral training for home and school. Jacob will need a referral to the school system when he turns 3 years old. Children with developmental disabilities who are over age 3 are eligible to receive services in the public school system. Case 7 Heather is 18 months old. Her mother Kathleen brings her to clinic quite worried that Heather is no longer doing the things she could previously do. Kathleen’s pregnancy, labor and delivery were uncomplicated. Looking through her chart you note that Heather’s Denver II screening tests were interpreted as normal during her first year. At her one-year visit, Heather was just beginning to walk independently, able to put a block in a cup and said “baba” and “doggie” in addition to “mama” and “papa.” Question 1: What is your interpretation of the DENVER II for this case? Answer: (b) Suspect Key Teaching Points: Heather has 8 delays (help in house, drink from cup, imitate activities, play ball with examiner, scribbles, 2 words, 1 word, stoop and recover) and at least 5 cautions (use spoon/fork, tower of 2 cubes, dump raisin-demonstrated, 3 words, runs). Question 2: What is your next step? Answer: (a) Further medical evaluation (EI is also correct, but priority should be given to further medical evaluation). Discussion: Loss of developmental milestones is very concerning. Although there is a fair amount of normal variation in the acquisition of milestones, losing milestones is never a variant of normal. In Heather’s case, she has lost motor and language milestones and failed to gain personal-social milestones. Developmental regression can be caused by a variety of conditions, such as significant medical illness with prolonged hospitalization. Other causes of developmental regression include: Pervasive Developmental Disorders including Autism, Rett’s syndrome and childhood disintegrative disorder; metabolic disorders; and neuromuscular disorders. These would all require further medical evaluation starting with a detailed medical and family history and thorough physical examination. Whatever the underlying cause and prognosis, a referral to Early Intervention services would be appropriate concomitantly with further medical evaluation. Referral to social services for family support may also be needed. Case 8 Manuel is a 9-month-old boy who has been coming to your practice since birth for his well child care. Pregnancy, labor, and delivery were all normal. His mother, Maria, is concerned that “Manuel still doesn’t sleep through the night and won’t share his toys with his big brother.” Question 1: What is your interpretation of the DENVER II for this case? Answer: Normal Key Teaching Points: No cautions or delays Question 2: What is the next step? Answer: (e) Reassure parent, retest next visit. Discussion: Manuel’s profile does not raise suspicion of developmental delay. It is appropriate to reassure Maria about his development. It is also important to address her concerns about sleep and sharing toys. At nine months, Manuel is not developmentally capable of understanding sharing. His brother should be taught to use trading (get Manuel really interested in a different toy and then exchange that toy). By age four months, when nighttime feeding is no longer needed, it is possible for a child to sleep through the night. However, many things can interfere with sleep. The clinician should ask, “Where does Manuel sleep? How is he put to sleep each night? Is he taking bottles during the night? When does he wake during the night and what happens when he does?” Helpful suggestions include setting a consistent bed time and bedtime routine, eliminating bottles in bed, putting Manuel down in his crib drowsy but awake, and using brief periods of reassurance if Manuel awakes during the night. For more information on this topic please see bibliography. Case 1 Josephina is an 18-month old former 27-week premature girl whom you have followed since her discharge from the neonatal intensive care unit. Her NICU course was notable for a Grade III intraventricular hemorrhage, respiratory distress syndrome, intubation for 3 weeks, and mild residual bronchopulmonary dysplasia. She was receiving services from Early Intervention, but these were discontinued at her first birthday because “She was doing so well.” 1. Interpretation of Denver II: a) Normal b) Suspect c) Untestable 2. Your next step: a) Further medical evaluation b) Refer to Social Services c) Refer to Early Intervention d) Refer for School Evaluation e) Reassure parent, rescreen next visit When to Watch, When to Refer, When to Reassure Case #1: “Josephina” DA FORM 5694, MAY 1988 Denver II MONTHS 2 Name: Josephina Birthdate: Case #1 ID No.: Examiner: Date: YEARS 4 6 9 12 15 18 24 3 4 5 6 R PREPARE CEREAL Percent of children passing 25 50 75 R BRUSH TEETH, NO HELP Corrected age 90 R PLAY BOARD/CARD GAMES R 4 DRESS, NO HELP R 1 TEST ITEM 86% NAME FRIEND 15 COPY R WASH & DRY HANDS 16 DRAW PERSON 6 PARTS R 3 BRUSH TEETH WITH HELP "She tries but she drops it a lot." 13 COPY R PUT ON CLOTHING FEED DOLL 14 COPY R REMOVE GARMENT 16 DRAW PERSON 3 PTS R USE SPOON FORK 12 COPY R HELP IN HOUSE F DEFINE 7 WORDS TOWER OF 8 CUBES PERSONAL - SOCIAL P F 1 SMILE RESPONSIVELY 25 DEFINE 5 WORDS NAME 4 COLORS F DUMP RAISIN, DEMONSTRATED F SCRIBBLES C 24 UNDERSTAND 4 PREPOSITIONS SPEECH ALL UNDERSTANDABLE PUT BLOCK IN CUP 20 KNOW 4 ACTIONS R BANG 2 CUBES HELD IN HANDS P SMILE SPONTANEOUSLY 22 USE OF 3 OBJECTS 23 COUNT 1 BLOCK 9 THUMB-FINGER GRASP 22 USE OF 2 OBJECTS P TAKE 2 CUBES P 8 PASS CUBE P RAKE RAISIN REGARD FACE NAME 1 COLOR KNOW 2 ADJECTIVES 7LOOK FOR YARN 20 KNOW 2 ACTIONS "mama" "doggy" "dada" "kitty" "bottle" "truck" "juice" "baby" 5 FOLLOW 180º FINE MOTOR - ADAPTIVE 30 HEEL-TO-TOE WALK SPEECH HALF UNDERSTANDABLE REGARD RAISIN HANDS TOGETHER 6 GRASP RATTLE 5 FOLLOW PAST MIDLINE P P P P 19 BODY PARTS-6 BALANCE EACH FOOT 1 SECOND 29 BROAD JUMP R 2 WORDS 28 THROW BALL OVERHAND R ONE WORD JUMP UP KICK BALL FORWARD F R27 WALK UP STEPS F RUNS TEST BEHAVIOR (Check boxes for 1st, 2nd, or 3rd test) R WALK BACKWARDS P STAND ALONE P STAND-2 SECS. TURN TO VOICE 17 TURN TO RATTLING SOUND R GET TO SITTING R SQUEALS PULL TO STAND R LAUGHS R "OOO/AAH" STAND HOLDING ON R VOCALIZES HOPS BALANCE EACH FOOT 2 SECONDS 18 POINT 2 PICTURES F WALK WELL C P STOOP AND RECOVER R SINGLE SYLLABLES BALANCE EACH FOOT 3 SECONDS R COMBINE WORDS R 3 WORDS F R IMITATE SPEECH SOUNDS BALANCE EACH FOOT 4 SECS. 18 NAME 1 PICTURE R DADA/MAMA SPECIFIC R DADA/MAMA NON-SPECIFIC BALANCE EACH FOOT 5 SECS. 18 POINT 4 PICTURES P R 6 WORDS FOLLOW 5 TO MIDLINE P R JABBERS P R COMBINE SYLLABLES LANGUAGE BALANCE EACH FOOT 6 SECONDS 18 NAME 4 PICTURES REACHES SIT-NO SUPPORT RESPOND TO BELL 23 COUNT 5 BLOCKS TOWER OF 4 CUBES F TOWER OF 2 CUBES R FEED SELF P 26 OPPOSITES-2 10IMITATE VERTICAL LINE TOWER OF 6 CUBES 21 KNOW 3 ADJECTIVES P R WAVE BYE-BYE P R INDICATE WANTS P R PLAY PAT-A-CAKE WORK FOR TOY 88% 11 THUMB WIGGLE R DRINK FROM CUP P R IMITATE ACTIVITIES P PLAY BALL WITH EXAMINER R 2 REGARD OWN HAND DEMONSTR. 13 PICK LONGER LINE Typical Yes No 1 2 3 Compliance (See Note 31) Always Complies Usually Complies Rarely Complies 1 2 3 Interest in Surroundings 1 2 3 1 2 3 1 2 3 Alert Somewhat Disinterested Seriously Disinterested PULL TO SIT - NO HEAD-LAG R ROLL OVER Fearfulness CHEST UP-ARM SUPPORT None Mild Extreme BEAR WEIGHT ON LEGS SIT-HEAD STEADY HEAD UP 90º Attention Span HEAD UP 45º Appropriate Somewhat Distractible Very Distractible RLIFT HEAD EQUAL MOVEMENTS MONTHS 2 4 6 FOR USE OF THIS FORM, SEE AR 600-75 RPUT ON T-SHIRT ©1969, 1989, 1990 W. K. Frankenburg and J. B. Dodds© May pass by report Footnote no. (see back of form) 9 12 15 18 24 3 YEARS 4 5 6 Case 2 Jimmy is a 12-month old boy who is new to your practice. His clinic record indicates that he has not been seen for a well child visit since he was 6 months old. The last immunizations he received were his “4 month shots.” His mother, Isabel reports that his 10 year old brother provides much of Jimmy’s care. During his physical exam, you observe that he has not been washed recently. During the Denver II, Isabel reports “I never gave him a cup - he loves the bottle.” When asked if Jimmy imitates, she asks, “What do you mean?” Jimmy looks confused when you try to play ball with him, although he does reach up to be held. 1. Interpretation of Denver II: a) Normal b) Suspect c) Untestable 2. Your next step: a) Further medical evaluation b) Refer to Social Services c) Refer to Early Intervention d) Refer for School Evaluation e) Reassure parent, rescreen next visit When to Watch, When to Refer, When to Reassure Case #2: “Jimmy” DA FORM 5694, MAY 1988 Denver II MONTHS 2 Name: Jimmy Birthdate: Case ID No.: Examiner: Date: #2 YEARS 4 6 9 12 15 18 24 3 4 5 6 R PREPARE CEREAL R BRUSH TEETH, NO HELP R PLAY BOARD/CARD GAMES Percent of children passing 25 50 75 R 4 DRESS, NO HELP 90 R 1 TEST ITEM RPUT ON T-SHIRT 86% NAME FRIEND 15 COPY R WASH & DRY HANDS 16 DRAW PERSON 6 PARTS R 3 BRUSH TEETH WITH HELP 13 COPY R PUT ON CLOTHING "He's on the bottle" 14 COPY R REMOVE GARMENT 16 DRAW PERSON 3 PTS R USE SPOON FORK 12 COPY R HELP IN HOUSE No. "What do you mean?" P P DEFINE 7 WORDS TOWER OF 8 CUBES R IMITATE ACTIVITIES P R INDICATE WANTS P R PLAY PAT-A-CAKE 25 DEFINE 5 WORDS NAME 4 COLORS DUMP RAISIN, DEMONSTRATED 24 UNDERSTAND 4 PREPOSITIONS SCRIBBLES SPEECH ALL UNDERSTANDABLE F PUT BLOCK IN CUP WORK FOR TOY P 20 KNOW 4 ACTIONS R BANG 2 CUBES HELD IN HANDS P SMILE SPONTANEOUSLY P 1 SMILE RESPONSIVELY 21 KNOW 3 ADJECTIVES TOWER OF 4 CUBES TOWER OF 2 CUBES R FEED SELF R 2 REGARD OWN HAND 22 USE OF 3 OBJECTS 23 COUNT 1 BLOCK 9 THUMB-FINGER GRASP 22 USE OF 2 OBJECTS P TAKE 2 CUBES REGARD FACE NAME 1 COLOR 8 PASS CUBE KNOW 2 ADJECTIVES RAKE RAISIN 7LOOK FOR YARN 20 KNOW 2 ACTIONS REACHES REGARD RAISIN FINE MOTOR - ADAPTIVE HANDS TOGETHER 6 GRASP RATTLE 5 FOLLOW PAST MIDLINE P P BALANCE EACH FOOT 1 SECOND 29 BROAD JUMP 28 THROW BALL OVERHAND JUMP UP KICK BALL FORWARD R 27 WALK UP STEPS TEST BEHAVIOR RUNS (Check boxes for 1st, 2nd, or 3rd test) R WALK BACKWARDS P STAND ALONE P STAND-2 SECS. P R SQUEALS P R LAUGHS R "OOO/AAH" R GET TO SITTING PULL TO STAND STAND HOLDING ON R VOCALIZES SIT-NO SUPPORT RESPOND TO BELL HOPS BALANCE EACH FOOT 2 SECONDS 18 POINT 2 PICTURES F WALK WELL F STOOP AND RECOVER TURN TO VOICE 17 TURN TO RATTLING SOUND BALANCE EACH FOOT 3 SECONDS R COMBINE WORDS R 2 WORDS P R JABBERS P R COMBINE SYLLABLES P R DADA/MAMA NON-SPECIFIC R SINGLE SYLLABLES BALANCE EACH FOOT 4 SECS. 18 NAME 1 PICTURE R 3 WORDS R DADA/MAMA SPECIFIC R IMITATE SPEECH SOUNDS BALANCE EACH FOOT 5 SECS. 18 POINT 4 PICTURES 19 BODY PARTS-6 P R ONE WORD P 30 HEEL-TO-TOE WALK SPEECH HALF UNDERSTANDABLE R 6 WORDS FOLLOW 5 TO MIDLINE BALANCE EACH FOOT 6 SECONDS 18 NAME 4 PICTURES "bye" "birdie" "milk" "mama" "babo" [bobby] 5 FOLLOW 180º LANGUAGE 23 COUNT 5 BLOCKS TOWER OF 6 CUBES C R WAVE BYE-BYE 26 OPPOSITES-2 10IMITATE VERTICAL LINE PLAY BALL WITH EXAMINER Typical Yes No 1 2 3 Compliance (See Note 31) Always Complies Usually Complies Rarely Complies 1 2 3 Interest in Surroundings 1 2 3 1 2 3 1 2 3 ©1969, 1989, 1990 W. K. Frankenburg and J. B. Dodds© PERSONAL - SOCIAL F F 88% 11 THUMB WIGGLE R DRINK FROM CUP F DEMONSTR. 13 PICK LONGER LINE FEED DOLL FOR USE OF THIS FORM, SEE AR 600-75 May pass by report Footnote no. (see back of form) Alert Somewhat Disinterested Seriously Disinterested PULL TO SIT - NO HEAD-LAG R ROLL OVER Fearfulness CHEST UP-ARM SUPPORT None Mild Extreme BEAR WEIGHT ON LEGS SIT-HEAD STEADY HEAD UP 90º Attention Span HEAD UP 45º Appropriate Somewhat Distractible Very Distractible RLIFT HEAD EQUAL MOVEMENTS MONTHS 2 4 6 9 12 15 18 24 3 YEARS 4 5 6 Case 3 Daniel is a 2-year old boy who has been in your office at least 5 times this winter for otitis media. Otherwise, he has been quite well. His mother, Sandra, reports that “he is a delightful, friendly kid who gets along great with his brother and sisters and Brandy, our Golden Retriever.” She notes, “Daniel is my quiet one, he talks less than the others but of course they always talk for him.” You ask Daniel some questions and he smiles at you but his speech is very difficult to understand. You rely on Sandra to translate for him. 1. Interpretation of Denver II: a) Normal b) Suspect c) Untestable 2. Your next step: a) Further medical evaluation b) Refer to Social Services c) Refer to Early Intervention d) Refer for School Evaluation e) Reassure parent, rescreen next visit When to Watch, When to Refer, When to Reassure Case #3: “Daniel” DA FORM 5694, MAY 1988 Denver II MONTHS 2 Name: Daniel Birthdate: Case ID No.: Examiner: Date: #3 YEARS 4 6 9 12 15 18 24 3 4 5 6 R PREPARE CEREAL R BRUSH TEETH, NO HELP R PLAY BOARD/CARD GAMES Percent of children passing 25 50 75 R 4 DRESS, NO HELP 90 R 1 TEST ITEM RPUT ON T-SHIRT P P P P P 13 COPY R PUT ON CLOTHING FEED DOLL 14 COPY 16 DRAW PERSON 3 PTS 12 COPY DEFINE 7 WORDS F TOWER OF 8 CUBES 25 DEFINE 5 WORDS NAME 4 COLORS 24 UNDERSTAND 4 PREPOSITIONS SCRIBBLES SPEECH ALL UNDERSTANDABLE PUT BLOCK IN CUP 20 KNOW 4 ACTIONS R 2 REGARD OWN HAND R BANG 2 CUBES HELD IN HANDS P SMILE SPONTANEOUSLY 22 USE OF 3 OBJECTS 23 COUNT 1 BLOCK 9 THUMB-FINGER GRASP 1 SMILE RESPONSIVELY 22 USE OF 2 OBJECTS TAKE 2 CUBES NAME 1 COLOR REGARD FACE 8 PASS CUBE KNOW 2 ADJECTIVES RAKE RAISIN 7LOOK FOR YARN 20 KNOW 2 ACTIONS F REACHES (points to eyes & nose) HANDS TOGETHER 6 GRASP RATTLE 5 FOLLOW PAST MIDLINE FOLLOW 5 TO MIDLINE P P F SPEECH HALF UNDERSTANDABLE F 18 POINT 4 PICTURES F 19 BODY PARTS-6 C F 18 NAME 1 PICTURE P R COMBINE WORDS F 18 POINT 2 PICTURES C P R DADA/MAMA SPECIFIC TEST BEHAVIOR (Check boxes for 1st, 2nd, or 3rd test) WALK WELL STOOP AND RECOVER R SINGLE SYLLABLES STAND ALONE TURN TO VOICE STAND-2 SECS. 17 TURN TO RATTLING SOUND R GET TO SITTING R SQUEALS PULL TO STAND R LAUGHS R "OOO/AAH" STAND HOLDING ON R VOCALIZES SIT-NO SUPPORT RESPOND TO BELL HOPS BALANCE EACH FOOT 2 SECONDS P JUMP UP P R27 WALK UP STEPS P RUNS R WALK BACKWARDS R IMITATE SPEECH SOUNDS BALANCE EACH FOOT 3 SECONDS 28 THROW BALL OVERHAND P KICK BALL FORWARD R DADA/MAMA NON-SPECIFIC BALANCE EACH FOOT 5 SECS. BALANCE EACH FOOT 4 SECS. 29 BROAD JUMP P R 2 WORDS P R ONE WORD R COMBINE SYLLABLES 30 HEEL-TO-TOE WALK BALANCE EACH FOOT 1 SECOND R 6 WORDS R 3 WORDS R JABBERS BALANCE EACH FOOT 6 SECONDS 18 NAME 4 PICTURES Typical Yes No 1 2 3 Compliance (See Note 31) Always Complies Usually Complies Rarely Complies 1 2 3 Interest in Surroundings 1 2 3 1 2 3 1 2 3 ©1969, 1989, 1990 W. K. Frankenburg and J. B. Dodds© REGARD RAISIN 5 FOLLOW 180º FINE MOTOR - ADAPTIVE 23 COUNT 5 BLOCKS 21 KNOW 3 ADJECTIVES P TOWER OF 2 CUBES P DUMP RAISIN, DEMONSTRATED P R FEED SELF WORK FOR TOY 26 OPPOSITES-2 10IMITATE VERTICAL LINE P TOWER OF 6 CUBES P TOWER OF 4 CUBES R INDICATE WANTS 88% 11 THUMB WIGGLE R DRINK FROM CUP R WAVE BYE-BYE DEMONSTR. 13 PICK LONGER LINE R REMOVE GARMENT PLAY BALL WITH EXAMINER PERSONAL - SOCIAL 16 DRAW PERSON 6 PARTS R 3 BRUSH TEETH WITH HELP P R USE SPOON FORK P R HELP IN HOUSE R PLAY PAT-A-CAKE 15 COPY R WASH & DRY HANDS R IMITATE ACTIVITIES LANGUAGE 86% NAME FRIEND P FOR USE OF THIS FORM, SEE AR 600-75 May pass by report Footnote no. (see back of form) Alert Somewhat Disinterested Seriously Disinterested PULL TO SIT - NO HEAD-LAG R ROLL OVER Fearfulness CHEST UP-ARM SUPPORT None Mild Extreme BEAR WEIGHT ON LEGS SIT-HEAD STEADY HEAD UP 90º Attention Span HEAD UP 45º Appropriate Somewhat Distractible Very Distractible RLIFT HEAD EQUAL MOVEMENTS MONTHS 2 4 6 9 12 15 18 24 3 YEARS 4 5 6 Case 4 Eleanor is a 3-year-old girl who is new to your clinic. Her mother, Susan, reports that she is healthy but that “She is still not interested in potty training.” Eleanor has been in a playgroup but seems to prefer playing by herself. She is unable to name a friend other than “Mommy.” She does not point to the pictures but smiles and repeats “meow” when you asks “which one says meow.” Despite multiple demonstrations, Eleanor cannot stand on one foot. After completing a tower of 5 blocks, she looks at both you and her mother, claps and laughs. 1. Interpretation of Denver II: a) Normal b) Suspect c) Untestable 2. Your next step: a) Further medical evaluation b) Refer to Social Services c) Refer to Early Intervention d) Refer for School Evaluation e) Reassure parent, rescreen next visit When to Watch, When to Refer, When to Reassure Case #4: “Eleanor” DA FORM 5694, MAY 1988 Denver II MONTHS 2 Name: Eleanor Birthdate: Case ID No.: Examiner: Date: #4 YEARS 4 6 9 12 15 18 24 3 4 5 6 R PREPARE CEREAL R BRUSH TEETH, NO HELP R PLAY BOARD/CARD GAMES R 4 DRESS, NO HELP 90 R 1 TEST ITEM May pass by report Footnote no. (see back of form) P P P F RPUT ON T-SHIRT F NAME FRIEND C 16 DRAW PERSON 6 PARTS R 3 BRUSH TEETH WITH HELP P 13 COPY R PUT ON CLOTHING 14 COPY 16 DRAW PERSON 3 PTS R USE SPOON FORK 12 COPY R HELP IN HOUSE F 11 THUMB WIGGLE F TOWER OF 8 CUBES C F 10IMITATE VERTICAL LINE C R DRINK FROM CUP R IMITATE ACTIVITIES F TOWER OF 6 CUBES PLAY BALL WITH EXAMINER 25 DEFINE 5 WORDS 24 UNDERSTAND 4 PREPOSITIONS SCRIBBLES F SPEECH ALL UNDERSTANDABLE WORK FOR TOY PUT BLOCK IN CUP R F 20 KNOW 4 ACTIONS R BANG 2 CUBES 2 REGARD OWN HAND HELD IN HANDS F 22 USE OF 3 OBJECTS P SMILE SPONTANEOUSLY 9 THUMB-FINGER F 23 COUNT 1 BLOCK GRASP 1 SMILE F 22 USE OF 2 OBJECTS RESPONTAKE 2 CUBES SIVELY F NAME 1 COLOR REGARD 8 PASS CUBE FACE 2 F KNOW ADJECTIVES RAKE RAISIN (speech 1/3 7LOOK FOR YARN F 20 KNOW 2 ACTIONS C understandable) BALANCE EACH FOOT 6 SECONDS REACHES F 18NAME 4 PICTURES C 30 HEEL-TO-TOE WALK SPEECH HALF UNDERSTANDABLE REGARD RAISIN F C (points to BALANCE EACH FOOT 5 SECS. 5 FOLLOW 180º tummy) F 18 POINT 4 PICTURES BALANCE EACH FOOT 4 SECS. HANDS F 19 BODY PARTS-6 BALANCE EACH FOOT 3 SECONDS TOGETHER P 18 NAME 1 PICTURE ice" ju t HOPS an "w GRASP 6 R COMBINE WORDS RATTLE P BALANCE EACH F FOOT 2 SECONDS P 18 POINT 2 PICTURES 5 FOLLOW PAST MIDLINE BALANCE EACH R 6 WORDS F FOOT C FOLLOW 1 SECOND 5 TO R 3 WORDS MIDLINE F 29 BROAD JUMP C R 2 WORDS P 28 THROW BALL OVERHAND R ONE WORD P JUMP UP R DADA/MAMA SPECIFIC P KICK BALL FORWARD R JABBERS P R27 WALK UP STEPS R COMBINE SYLLABLES TEST BEHAVIOR RUNS R DADA/MAMA NON-SPECIFIC (Check boxes for 1st, 2nd, or 3rd test) R WALK BACKWARDS WALK WELL R IMITATE SPEECH SOUNDS STOOP AND RECOVER R SINGLE SYLLABLES STAND ALONE TURN TO VOICE STAND-2 SECS. 17 TURN TO RATTLING SOUND LANGUAGE 23 COUNT 5 BLOCKS R GET TO SITTING R SQUEALS PULL TO STAND R LAUGHS R "OOO/AAH" STAND HOLDING ON R VOCALIZES SIT-NO SUPPORT RESPOND TO BELL Typical Yes No 1 2 3 Compliance (See Note 31) Always Complies Usually Complies Rarely Complies 1 2 3 Interest in Surroundings 1 2 3 1 2 3 1 2 3 ©1969, 1989, 1990 W. K. Frankenburg and J. B. Dodds© PERSONAL - SOCIAL FINE MOTOR - ADAPTIVE R FEED SELF 26 OPPOSITES-2 NAME 4 COLORS P DUMP RAISIN, DEMONSTRATED R PLAY PAT-A-CAKE 88% DEFINE 7 WORDS 21 KNOW 3 ADJECTIVES P TOWER OF 4 CUBES P TOWER OF 2 CUBES R INDICATE WANTS DEMONSTR. 13 PICK LONGER LINE FEED DOLL R REMOVE GARMENT R WAVE BYE-BYE 86% 15 COPY R WASH & DRY HANDS Alert Somewhat Disinterested Seriously Disinterested PULL TO SIT - NO HEAD-LAG R ROLL OVER Fearfulness CHEST UP-ARM SUPPORT None Mild Extreme BEAR WEIGHT ON LEGS SIT-HEAD STEADY HEAD UP 90º Attention Span HEAD UP 45º Appropriate Somewhat Distractible Very Distractible RLIFT HEAD EQUAL MOVEMENTS MONTHS 2 4 6 9 12 15 FOR USE OF THIS FORM, SEE AR 600-75 Percent of children passing 25 50 75 18 24 3 YEARS 4 5 6 Case 5 Shenika is a 4 year old girl who presents for her preschool screening visit. Her older sister Sharde was followed by you in the past for lead poisoning. Shenika comes right into the exam room, sits down in the chair next to you and asks, “Are you my doctor? Are you going to check my heart?” Shenika’s mother Jackie laughs and states that Shenika “is always talking!” She reports that Shenika loves to fix her own breakfast, dresses herself and loves to play “Chutes and Ladders” with Sharde. While you are taking the history, Shenika stacks the blocks and sings her ABCs. She tells you her favorite color is purple and she begins pointing at different colors around the room and tells you that the tiles in your office are “salmon.” You attempt to administer a Denver II, but Shenika refuses activities or laughs and says, “I’m not gonna tell you!” You are able to observe her during the visit, and gather some information by history from Jackie. 1. Interpretation of Denver II: a) Normal b) Suspect c) Untestable 2. Your next step: a) Further medical evaluation b) Refer to Social Services c) Refer to Early Intervention d) Refer for School Evaluation e) Reassure parent, rescreen next visit When to Watch, When to Refer, When to Reassure Case #5: “Shenika” DA FORM 5694, MAY 1988 Denver II YEARS 4 6 9 Percent of children passing 25 50 75 12 15 18 "she won't let me help her" 90 R 1 TEST ITEM May pass by report Footnote no. (see back of form) 24 P P P R 3 BRUSH TEETH WITH HELP R IMITATE ACTIVITIES P TOWER OF 6 CUBES P TOWER OF 4 CUBES PLAY BALL WITH EXAMINER R WAVE BYE-BYE PERSONAL - SOCIAL PUT BLOCK IN CUP 9 THUMB-FINGER GRASP TAKE 2 CUBES REGARD FACE 8 PASS CUBE RAKE RAISIN 7LOOK FOR YARN "she does these at home" REACHES REGARD RAISIN FINE MOTOR - ADAPTIVE 5 FOLLOW 180º HANDS TOGETHER 6 GRASP RATTLE 5 FOLLOW PAST MIDLINE R 6 WORDS FOLLOW 5 TO MIDLINE R 3 WORDS R 2 WORDS R ONE WORD R DADA/MAMA SPECIFIC R JABBERS P R COMBINE SYLLABLES P TEST BEHAVIOR (Check boxes for 1st, 2nd, or 3rd test) R WALK BACKWARDS STOOP AND RECOVER R SINGLE SYLLABLES STAND ALONE TURN TO VOICE STAND-2 SECS. 17 TURN TO RATTLING SOUND LANGUAGE R KICK BALL FORWARD R 27 WALK UP STEPS WALK WELL R IMITATE SPEECH SOUNDS R GET TO SITTING R SQUEALS PULL TO STAND R LAUGHS R "OOO/AAH" STAND HOLDING ON R VOCALIZES SIT-NO SUPPORT RESPOND TO BELL 21 KNOW 3 ADJECTIVES P 24 UNDERSTAND 4 PREPOSITIONS P SPEECH ALL UNDERSTANDABLE P 20 KNOW 4 ACTIONS P 22 USE OF 3 OBJECTS P 23 COUNT 1 BLOCK P 22 USE OF 2 OBJECTS R NAME 1 COLOR 2 P KNOW ADJECTIVES P 20 KNOW 2 ACTIONS BALANCE EACH FOOT 6 SECONDS 18 NAME 4 PICTURES R 30 HEEL-TO-TOE WALK P SPEECH HALF UNDERSTANDABLE F BALANCE EACH FOOT 5 SECS. 18 POINT 4 PICTURES R BALANCE EACH FOOT 4 SECS. 19 BODY PARTS-6 R BALANCE EACH FOOT 3 SECONDS 18 NAME 1 PICTURE R HOPS "I'm R COMBINE WORDS BALANCE EACH R FOOT not gonna 2 SECONDS 18 POINT 2 PICTURES hop!" BALANCE EACH R FOOT 1 SECOND R 29 BROAD JUMP R 28 THROW BALL OVERHAND P JUMP UP RUNS R DADA/MAMA NON-SPECIFIC 88% R 25 DEFINE 5 WORDS R NAME 4 COLORS TOWER OF 2 CUBES R BANG 2 CUBES HELD IN HANDS 1 SMILE RESPONSIVELY P DUMP RAISIN, DEMONSTRATED SCRIBBLES P SMILE SPONTANEOUSLY 86% 15 COPY R 11 THUMB WIGGLE DEFINE 7 WORDS P TOWER OF 8 CUBES R 26 OPPOSITES-2 P 10IMITATE VERTICAL LINE R 23 COUNT 5 BLOCKS R HELP IN HOUSE R DRINK FROM CUP R 2 REGARD OWN HAND 6 P16 DRAW PERSON 6 PARTS P13 COPY DEMONSTR. R 13 PICK LONGER LINE "Can't make me" R 14 COPY P 16 DRAW PERSON 3 PTS P 12 COPY R WASH & DRY HANDS R REMOVE GARMENT R FEED SELF 5 P RPUT ON T-SHIRT P NAME FRIEND R USE SPOON FORK WORK FOR TOY R PREPARE CEREAL R BRUSH TEETH, NO HELP R PUT ON CLOTHING R PLAY PAT-A-CAKE 4 P P R PLAY BOARD/CARD GAMES P R4 DRESS, NO HELP FEED DOLL R INDICATE WANTS 3 Typical Yes No 1 2 3 Compliance (See Note 31) Always Complies Usually Complies Rarely Complies 1 2 3 Interest in Surroundings 1 2 3 1 2 3 1 2 3 Alert Somewhat Disinterested Seriously Disinterested PULL TO SIT - NO HEAD-LAG R ROLL OVER Fearfulness CHEST UP-ARM SUPPORT None Mild Extreme BEAR WEIGHT ON LEGS SIT-HEAD STEADY HEAD UP 90º Attention Span HEAD UP 45º Appropriate Somewhat Distractible Very Distractible RLIFT HEAD EQUAL MOVEMENTS MONTHS 2 4 6 9 12 FOR USE OF THIS FORM, SEE AR 600-75 2 ©1969, 1989, 1990 W. K. Frankenburg and J. B. Dodds© MONTHS Name: Shenika Birthdate: Case #5 ID No.: Examiner: Date: 15 18 24 3 YEARS 4 5 6 Case 6 Jacob comes for his 2-year visit. His mother Anna’s biggest concern is that “Jacob has terrible temper tantrums and doesn’t talk as much as his sister did at his age.” Anna’s parents have told her not to worry because the temper tantrums are part of “the terrible twos” and “because you spoil him.” Jacob makes screeching noises but does not use any words in the office. Anna reports that he struggles when she brushes his hair or tries to dress him. He does not throw the ball you offer, however he does nearly hit you in the head when he throws a toy overhand. He jumps up and down and flaps his hands. 1. Interpretation of Denver II: a) Normal b) Suspect c) Untestable 2. Your next step: a) Further medical evaluation b) Refer to Social Services c) Refer to Early Intervention d) Refer for School Evaluation e) Reassure parent, rescreen next visit When to Watch, When to Refer, When to Reassure Case #6: “Jacob” DA FORM 5694, MAY 1988 Denver II MONTHS 2 Name: Jacob Birthdate: Case ID No.: Examiner: Date: #6 YEARS 4 6 9 12 15 18 24 3 4 5 6 R PREPARE CEREAL Percent of children passing 25 50 75 "dressing & brushing teeth are a big struggle" 90 R PLAY BOARD/CARD GAMES R 4 DRESS, NO HELP R 1 TEST ITEM RPUT ON T-SHIRT P F F P P F 14 COPY 16 DRAW PERSON 3 PTS 12 COPY 1 SMILE RESPONSIVELY F TOWER OF 8 CUBES 26 OPPOSITES-2 F 10IMITATE VERTICAL LINE 23 COUNT 5 BLOCKS F TOWER OF 6 CUBES C 21 KNOW 3 ADJECTIVES 25 DEFINE 5 WORDS NAME 4 COLORS F DUMP RAISIN, DEMONSTRATED 24 UNDERSTAND 4 PREPOSITIONS P SCRIBBLES F PUT BLOCK IN CUP 2 CUBES P RBANG HELD IN HANDS repeatedly lines cubes up in a straight line 9 THUMB-FINGER GRASP TAKE 2 CUBES REGARD FACE SPEECH ALL UNDERSTANDABLE 20 KNOW 4 ACTIONS 22 USE OF 3 OBJECTS 23 COUNT 1 BLOCK 22 USE OF 2 OBJECTS NAME 1 COLOR 8 PASS CUBE KNOW 2 ADJECTIVES RAKE RAISIN F F 18NAME 4 PICTURES 7LOOK FOR YARN 20 KNOW 2 ACTIONS REACHES 6 GRASP RATTLE "mamma" F R 6 WORDS "cookie" P R 3 WORDS "train" "juice" P R 2 WORDS R 28 THROW BALL OVERHAND P R ONE WORD P JUMP UP R DADA/MAMA SPECIFIC P KICK BALL FORWARD R JABBERS P R27 WALK UP STEPS R COMBINE SYLLABLES P RUNS 5 FOLLOW PAST MIDLINE FOLLOW 5 TO MIDLINE R DADA/MAMA NON-SPECIFIC WALK WELL STOOP AND RECOVER R SINGLE SYLLABLES STAND ALONE TURN TO VOICE STAND-2 SECS. 17 TURN TO RATTLING SOUND R GET TO SITTING R SQUEALS Refuses to throw ball but throws doll overhand. PULL TO STAND R LAUGHS R "OOO/AAH" STAND HOLDING ON R VOCALIZES SIT-NO SUPPORT 29 BROAD JUMP TEST BEHAVIOR (Check boxes for 1st, 2nd, or 3rd test) R WALK BACKWARDS R IMITATE SPEECH SOUNDS BALANCE EACH FOOT 1 SECOND PULL TO SIT - NO HEAD-LAG Typical Yes No 1 2 3 Compliance (See Note 31) Always Complies Usually Complies Rarely Complies 1 2 3 Interest in Surroundings 1 2 3 1 2 3 1 2 3 ©1969, 1989, 1990 W. K. Frankenburg and J. B. Dodds© FINE MOTOR - ADAPTIVE HANDS TOGETHER RESPOND TO BELL BALANCE EACH FOOT 6 SECONDS 30 HEEL-TO-TOE WALK F SPEECH HALF UNDERSTANDABLE C BALANCE EACH FOOT 5 SECS. F 18 POINT 4 PICTURES C BALANCE EACH FOOT 4 SECS. 19 F BODY PARTS-6 BALANCE EACH FOOT 3 SECONDS F 18 NAME 1 PICTURE HOPS F R COMBINE WORDS BALANCE EACH FOOT 2 SECONDS 18 POINT 2 PICTURES F REGARD RAISIN 5 FOLLOW 180º LANGUAGE 88% 11 THUMB WIGGLE F TOWER OF 4 CUBES F TOWER OF 2 CUBES R INDICATE WANTS P DEMONSTR. 13 PICK LONGER LINE FEED DOLL PLAY BALL WITH EXAMINER P SMILE SPONTANEOUSLY 13 COPY DEFINE 7 WORDS R WAVE BYE-BYE R 2 REGARD OWN HAND 16 DRAW PERSON 6 PARTS C R REMOVE GARMENT R DRINK FROM CUP R PLAY PAT-A-CAKE 15 COPY C R PUT ON CLOTHING P R USE SPOON FORK F R HELP IN HOUSE R FEED SELF 86% NAME FRIEND R 3 BRUSH TEETH WITH HELP R IMITATE ACTIVITIES WORK FOR TOY F R WASH & DRY HANDS FOR USE OF THIS FORM, SEE AR 600-75 May pass by report Footnote no. (see back of form) PERSONAL - SOCIAL R BRUSH TEETH, NO HELP Alert Somewhat Disinterested Seriously Disinterested R ROLL OVER Fearfulness CHEST UP-ARM SUPPORT None Mild Extreme BEAR WEIGHT ON LEGS SIT-HEAD STEADY HEAD UP 90º Attention Span HEAD UP 45º Appropriate Somewhat Distractible Very Distractible RLIFT HEAD EQUAL MOVEMENTS MONTHS 2 4 6 9 12 15 18 24 3 YEARS 4 5 6 Case 7 Heather is 18 months old. Her mother Kathleen brings her to clinic quite worried that Heather is no longer doing the things she could previously do. Kathleen’s pregnancy, labor and delivery were uncomplicated. Looking through her chart you note that Heather’s Denver II screening tests were interpreted as normal during her first year. At her one-year visit, Heather was just beginning to walk independently, able to put a block in a cup and said “baba” and “doggie” in addition to “mama” and “papa.” 1. Interpretation of Denver II: a) Normal b) Suspect c) Untestable 2. Your next step: a) Further medical evaluation b) Refer to Social Services c) Refer to Early Intervention d) Refer for School Evaluation e) Reassure parent, rescreen next visit When to Watch, When to Refer, When to Reassure Case #7: “Heather” DA FORM 5694, MAY 1988 Denver II MONTHS 2 Name: Heather Birthdate: Case #7 ID No.: Examiner: Date: YEARS 4 6 9 12 15 18 24 3 4 5 6 R PREPARE CEREAL R BRUSH TEETH, NO HELP R PLAY BOARD/CARD GAMES Percent of children passing 25 50 75 R 4 DRESS, NO HELP 90 R 1 TEST ITEM RPUT ON T-SHIRT 86% NAME FRIEND 15 COPY R WASH & DRY HANDS 16 DRAW PERSON 6 PARTS R 3 BRUSH TEETH WITH HELP 13 COPY R PUT ON CLOTHING FEED DOLL 14 COPY F R REMOVE GARMENT F R USE SPOON FORK F R HELP IN HOUSE F P P P TAKE 2 CUBES 25 DEFINE 5 WORDS NAME 4 COLORS 24 UNDERSTAND 4 PREPOSITIONS SPEECH ALL UNDERSTANDABLE 20 KNOW 4 ACTIONS 22 USE OF 3 OBJECTS 23 COUNT 1 BLOCK 22 USE OF 2 OBJECTS NAME 1 COLOR REGARD FACE 8 PASS CUBE KNOW 2 ADJECTIVES RAKE RAISIN 7LOOK FOR YARN 20 KNOW 2 ACTIONS FINE MOTOR - ADAPTIVE no longer says any of these ma" "mama" d "da a" "bab gy" "dog e" "mor 6 GRASP RATTLE R SQUEALS BALANCE EACH FOOT 5 SECS. 18 POINT 4 PICTURES HANDS TOGETHER 5 FOLLOW PAST MIDLINE 30 HEEL-TO-TOE WALK SPEECH HALF UNDERSTANDABLE REGARD RAISIN 5 FOLLOW 180º FOLLOW 5 TO MIDLINE BALANCE EACH FOOT 6 SECONDS 18 NAME 4 PICTURES REACHES LANGUAGE 23 COUNT 5 BLOCKS 21 KNOW 3 ADJECTIVES "she used to scribble but can't anymore" 9 THUMB-FINGER GRASP 26 OPPOSITES-2 10IMITATE VERTICAL LINE TOWER OF 6 CUBES F TOWER OF 4 CUBES F TOWER OF 2 CUBES C F DUMP RAISIN, DEMONSTRATED C 2 CUBES P RBANG HELD IN HANDS 1 SMILE RESPONSIVELY TOWER OF 8 CUBES F SCRIBBLES P PUT BLOCK IN CUP R FEED SELF WORK FOR TOY P SMILE SPONTANEOUSLY DEFINE 7 WORDS PLAY BALL WITH EXAMINER R WAVE BYE-BYE 88% 11 THUMB WIGGLE F R IMITATE ACTIVITIES P R INDICATE WANTS P R PLAY PAT-A-CAKE R 2 REGARD OWN HAND 12 COPY BALANCE EACH FOOT 4 SECS. 19 BODY PARTS-6 BALANCE EACH FOOT 3 SECONDS 18 NAME 1 PICTURE R COMBINE WORDS HOPS BALANCE EACH FOOT 2 SECONDS 18 POINT 2 PICTURES BALANCE EACH F R 6 WORDS FOOT 1 SECOND P R 3 WORDS F C 29 BROAD JUMP P R 2 WORDS F F28 THROW BALL OVERHAND P R ONE WORD F JUMP UP P R DADA/MAMA SPECIFIC F KICK BALL FORWARD P R JABBERS F R27 WALK UP STEPS TEST BEHAVIOR P R COMBINE SYLLABLES F RUNS C (Check boxes for 1st, 2nd, or 3rd test) P R WALK BACKWARDS P R DADA/MAMA NON-SPECIFIC P WALK WELL R IMITATE SPEECH SOUNDS 2 1 Typical F STOOP AND RECOVER R SINGLE SYLLABLES Yes P STAND ALONE No TURN TO VOICE P STAND-2 SECS. Compliance (See Note 31) 17 TURN TO 2 1 RATTLING SOUND GET TO P RSITTING Always Complies STAND HOLDING ON R VOCALIZES Interest in Surroundings SIT-NO SUPPORT RESPOND TO BELL 3 Usually Complies Rarely Complies TO P PULL STAND R LAUGHS R "OOO/AAH" 3 ©1969, 1989, 1990 W. K. Frankenburg and J. B. Dodds© PERSONAL - SOCIAL P 16 DRAW PERSON 3 PTS C R DRINK FROM CUP F DEMONSTR. 13 PICK LONGER LINE FOR USE OF THIS FORM, SEE AR 600-75 May pass by report Footnote no. (see back of form) 1 2 3 1 2 3 1 2 3 Alert Somewhat Disinterested Seriously Disinterested PULL TO SIT - NO HEAD-LAG R ROLL OVER Fearfulness CHEST UP-ARM SUPPORT None Mild Extreme BEAR WEIGHT ON LEGS SIT-HEAD STEADY HEAD UP 90º Attention Span HEAD UP 45º Appropriate Somewhat Distractible Very Distractible RLIFT HEAD EQUAL MOVEMENTS MONTHS 2 4 6 9 12 15 18 24 3 YEARS 4 5 6 Case 8 Manuel is a 9-month-old boy who has been coming to your practice since birth for his well child care. Pregnancy, labor, and delivery were all normal. His mother, Maria, is concerned that “Manuel still doesn’t sleep through the night and won’t share his toys with his big brother.” 1. Interpretation of Denver II: a) Normal b) Suspect c) Untestable 2. Your next step: a) Further medical evaluation b) Refer to Social Services c) Refer to Early Intervention d) Refer for School Evaluation e) Reassure parent, rescreen next visit When to Watch, When to Refer, When to Reassure Case #8: “Manuel” DA FORM 5694, MAY 1988 Denver II MONTHS 2 Name: Manuel Birthdate: Case ID No.: Examiner: Date: #8 YEARS 4 6 9 12 15 18 24 3 4 5 6 R PREPARE CEREAL R BRUSH TEETH, NO HELP R PLAY BOARD/CARD GAMES Percent of children passing 25 50 75 R 4 DRESS, NO HELP 90 R 1 TEST ITEM RPUT ON T-SHIRT 86% NAME FRIEND 15 COPY R WASH & DRY HANDS 16 DRAW PERSON 6 PARTS R 3 BRUSH TEETH WITH HELP 13 COPY R PUT ON CLOTHING FEED DOLL 14 COPY R REMOVE GARMENT 16 DRAW PERSON 3 PTS R USE SPOON FORK 12 COPY R HELP IN HOUSE DEFINE 7 WORDS TOWER OF 8 CUBES R IMITATE ACTIVITIES P P TOWER OF 4 CUBES 25 DEFINE 5 WORDS TOWER OF 2 CUBES NAME 4 COLORS DUMP RAISIN, DEMONSTRATED 24 UNDERSTAND 4 PREPOSITIONS R FEED SELF SCRIBBLES SPEECH ALL UNDERSTANDABLE PUT BLOCK IN CUP 20 KNOW 4 ACTIONS R 2 REGARD OWN HAND P P SMILE SPONTANEOUSLY R BANG 2 CUBES HELD IN HANDS F 1 SMILE RESPONSIVELY 22 USE OF 3 OBJECTS 23 COUNT 1 BLOCK 9 THUMB-FINGER GRASP 22 USE OF 2 OBJECTS P TAKE 2 CUBES P P NAME 1 COLOR 8 PASS CUBE P KNOW 2 ADJECTIVES RAKE RAISIN 7LOOK FOR YARN 20 KNOW 2 ACTIONS BALANCE EACH FOOT 6 SECONDS 18 NAME 4 PICTURES REACHES 30 HEEL-TO-TOE WALK SPEECH HALF UNDERSTANDABLE REGARD RAISIN 5 FOLLOW 180º FINE MOTOR - ADAPTIVE 23 COUNT 5 BLOCKS TOWER OF 6 CUBES 21 KNOW 3 ADJECTIVES P R WAVE BYE-BYE F R INDICATE WANTS P R PLAY PAT-A-CAKE WORK FOR TOY REGARD FACE BALANCE EACH FOOT 5 SECS. 18 POINT 4 PICTURES BALANCE EACH FOOT 4 SECS. 19 BODY PARTS-6 HANDS TOGETHER BALANCE EACH FOOT 3 SECONDS 18 NAME 1 PICTURE 6 GRASP RATTLE R COMBINE WORDS HOPS BALANCE EACH FOOT 2 SECONDS 18 POINT 2 PICTURES 5 FOLLOW PAST MIDLINE BALANCE EACH R 6 WORDS FOOT 1 SECOND "he says mama to me R 3 WORDS 29 BROAD JUMP but sometimes R 2 WORDS 28 THROW BALL OVERHAND calls his R ONE WORD JUMP UP brother F R DADA/MAMA SPECIFIC KICK BALL FORWARD dada" P R JABBERS R 27 WALK UP STEPS TEST BEHAVIOR P R COMBINE SYLLABLES RUNS R DADA/MAMA (Check boxes for 1st, 2nd, or 3rd test) R WALK BACKWARDS P NON-SPECIFIC FOLLOW 5 TO MIDLINE PR WALK WELL IMITATE SPEECH SOUNDS P RSINGLE SYLLABLES STOOP AND RECOVER P TURN TO VOICE STAND ALONE STAND-2 SECS. 17 TURN TO RATTLING SOUND LANGUAGE 26 OPPOSITES-2 10IMITATE VERTICAL LINE PLAY BALL WITH EXAMINER F R SQUEALS P R LAUGHS R "OOO/AAH" P R VOCALIZES P RESPOND TO BELL P R GET TO SITTING PULL TO STAND STAND HOLDING ON SIT-NO SUPPORT Typical Yes No 1 2 3 Compliance (See Note 31) Always Complies Usually Complies Rarely Complies 1 2 3 Interest in Surroundings 1 2 3 1 2 3 1 2 3 ©1969, 1989, 1990 W. K. Frankenburg and J. B. Dodds© PERSONAL - SOCIAL P 88% 11 THUMB WIGGLE R DRINK FROM CUP "sometimes" DEMONSTR. 13 PICK LONGER LINE FOR USE OF THIS FORM, SEE AR 600-75 May pass by report Footnote no. (see back of form) Alert Somewhat Disinterested Seriously Disinterested PULL TO SIT - NO HEAD-LAG R ROLL OVER Fearfulness CHEST UP-ARM SUPPORT None Mild Extreme BEAR WEIGHT ON LEGS SIT-HEAD STEADY HEAD UP 90º Attention Span HEAD UP 45º Appropriate Somewhat Distractible Very Distractible RLIFT HEAD EQUAL MOVEMENTS MONTHS 2 4 6 9 12 15 18 24 3 YEARS 4 5 6 When to Watch, When to Refer, When to Reassure Handout #1: How to Perform the DENVER II What you need: The items needed to perform the DENVER II can be purchased from Denver Developmental Materials, Inc. as a complete set in a carrying case. These include: • • • • • • red yarn pom-pom raisins or O shaped cereal rattle with narrow handle ten 1-inch square colored wooden blocks small, clear plastic bottle with 5/8"opening small bell • • • • • • small plastic doll small plastic feeding bottle for doll red pencil plastic cup with handle blank paper tennis ball 1. Calculate the child’s chronological age. a) Subtract the child’s date of birth from the date of the examination using 12 months to a year and 30 days to a month if you need to borrow. For example, if today is 10/18/97 and the baby’s date of birth is 11/20/95, calculations are performed as follows. 1) months = [(10-1 )+12] - 11 = 10 2) days = (18+30) - 20 =28 3) years = 96-95 = 1 (12) (30) 97 10 18 - 95 11 20 96 21 48 à - 95 11 20 01 10 28 Age = 1 year 10 months 28 days. b) Adjust for prematurity (if more than 2 weeks early): divide the number of weeks premature into months and days and subtract from the calculated age. Once a child is over 2 years it is no longer necessary to correct for prematurity. 2. Using a straight edge, draw a line down the DENVER II Record Form at the appropriate age line, and write the date of testing at the top of the line. 3. Make the exam as efficient and enjoyable as possible. a) The best time to perform the DENVER II may be at the beginning of the office visit, before the child has had a chance to get upset by other procedures. Keep the child fully clothed, be playful, help the child to relax. b) Make sure that parents understand that the DENVER II is not an IQ test and that the child is not expected to pass every item. c) Ask about “report” items first (these items are identified by an “R”). d) Perform gross motor items last (after you have gained the child’s confidence and when you are less likely to lose the child’s attention). e) Perform items requiring the test kit all at once. Try to keep kit in your lap, and the table free from distractions as much as possible. f) In babies, administer all of the items for which the child is supine at one time. 4. Start with easier items (those completely to the left of the line). Proceed next towards the right. The only exception is when an easier item reveals the answer to a harder item. For example, a child who has shown that he can copy a square following a demonstration can no longer be tested to see if he can copy a square without a demonstration. 5. Administer only as many items as you need for your purposes: a) To see if a child is at risk (a minimum); do three items that are completely to the left of the line and every item that intersects the age line in each sector. If the child cannot do any of these items (fails, refuses, has had no opportunity on reported items), keep going with items to the left of the line until child passes three items in each sector. b) To test strengths , proceed as above but also administer every item intersected by the line and continue towards the right until three failures are recorded in each sector. 6. Be strategic to minimize time needed to complete the DENVER II: a) Allow the child to play with the toys in the kit during the parent interview. The child may complete numerous tasks even before the testing starts. b) Give the child paper and pencil and allow him/her to draw. 7. The child may attempt (and be shown) each item 3 times. After that, item should be marked “fail.” You may document the ability to pass on subsequent trials in your notes. 8. Fill in the “Test Behavior” box in the lower right hand corner. This describes features of the child’s performance that may help you better interpret test results. If a toddler is having a temper tantrum during the session, results of the testing are unlikely to reflect the child’s best performance. Ask the parent if the child’s behavior is typical. Fill in the other observations yourself. 9. Scoring: every item should be marked with one of the following: P = pass F = fail N.O. = no opportunity (e.g., for reported items—it would not be accurate to “fail” a child on tooth brushing when she has never been allowed to brush her teeth). R = refusal (Child refuses to do test item). Minimize these by telling the child to do the item. Say, “Feed the baby?” rather than asking “Do you want to feed the baby?” Enlist the care-giver as your ally. 10. Interpreting individual items: Advanced = passing an item completely to the right of the age line (advanced items are not used in interpreting the examination). Normal = failing or refusing an item completely to the right of the age line; passing, failing or refusing an item in which the age line intersects the white (<75%) portion of the item bar (normal items are not used in interpreting the examination). Caution = failing an item in which the age line intersects the dark (75-90%) portion of the item bar Delayed = failing or refusing an item completely to the left of the age line No Opportunity = reported items the child has not had a chance to try 11. Interpreting the test as a whole: Normal = no delays, and maximum of one caution Suspect = two or more cautions, or one or more delays Untestable = refusal on one or more items completely to the left of the age line or on more than one item intersected by the age line in the 75-90% (dark) area. 12. What to do next: The DENVER II manual suggests that you should retest a child in 1-2 weeks if the interpretation is suspect or untestable. If the Denver II profile is very suspicious, you should refer the child right away. When to Watch, When to Refer, When to Reassure Handout #2: Early Intervention and School Referral I. Early Intervention: What are Early Intervention Programs (EIP)? Early Intervention programs are designed to provide integrated developmental services for eligible children ages birth to three years. Early Intervention is administered by the Department of Public Health. Early Intervention programs have teams of professionals including: occupational and physical therapists, speech therapists, developmental educators, social workers, nurses and psychologists. The teams rely on an interdisciplinary (multiple disciplines working together) and transdisciplinary (members of the team cross discipline boundaries incorporating information from other team members into their work) models and strive to provide family focused care. What are eligibility criteria? 1.The child has a known disabling physical or mental condition including but not limited to diagnosed chromosomal, neurological, metabolic disorders; visual or hearing impairment not corrected by medical intervention or prosthesis; or the presence of a delay in one or more areas of development, including cognitive development, physical development, vision, hearing, communication development, adaptive development, or psychosocial development. OR 2. Any four or more risk factors from either of the two following lists are present: Child Characteristics Family Characteristics *Birthweight <1200 grams *Gestational age <32 weeks *NICU admission more than 5 days *Diagnosis of intrauterine growth retardation (IUGR) or small for gestational age (SGA) *Weight or height <5% for age; weight for height <5%; weight for age dropped >2 major centiles in 3 mo for children <12 mo of age (or in 6 mo. for children 12-24 mo. of age) *Chronic feeding difficulties *Insecure attachment/interactional difficulties *Blood lead levels > 15 mg/dl *Suspected central nervous system abnormality *Multiple trauma or losses *Maternal age at child’s birth <17 or maternal history of 3 or more births before age 20 *Parental chronic illness or disability affecting care giving ability *Family lacking social supports *Inadequate food, shelter, clothing *Open or confirmed protective service case *Substance abuse in the home *Domestic violence in the home Guideline: Developmental delay by age and number of months delayed AGE DELAY BY 6 months 1.5 months 12 months 3 months 18 months 4 months 24 months, 30 months 6 months Who can refer to EIPs? Physicians, nurses, social workers, teachers, parents can all refer to Early Intervention. How does one make a referral? A referral should be make directly to the Early Intervention Program located near the family. A book listing the programs in your area should be available in every primary care setting. Referral should include the following information: names of child and parent(s), address, phone number (home and work), child’s date of birth, primary care provider, other involved services, physicians, reason for referral, and insurance coverage. What happens after a referral to an EIP? Within 45 working days an assessment will take place and an Individualized Family Service Plan will be developed by the Early Intervention team along with family members. The IFSP documents the goals and resources of the family and the services that will be provided by Early Intervention. How is Early Intervention funded? EI evaluation and services are funded through the Department of Public Health, private insurance, and Medicaid. II. School Services Children with special needs are eligible for special services in the public school system. There are several relevant pieces of legislation: Federal: The Individuals with Disabilities Education Act (IDEA, formerly entitled the Education of the Handicapped Act, often referred to as P.L. 94-142) calls for a free public education for all children in the least restrictive environment which meets their learning needs. Section 504 of the Rehabilitation Act of 1973 is the federal civil rights law that prohibits recipients of federal funds from discriminating against otherwise qualified disabled persons. State: State laws vary from state to state. As an example, in Massachusetts, Chapter 766 is the state version of the Federal law. Who can refer to School Services? Physicians, nurses, social workers, teachers, parents can make direct referrals. How does one make a referral? There is a formal process whereby any child may be referred to their local public school system for an evaluation to determine if there are any special learning needs. Parents must specifically request such an evaluation before the process can begin. What happens after a referral to School Services? Following the evaluation, the school staff meets with the parents to present the results and drafts an Individualized Educational Plan (IEP) if such needs are identified. The IEP includes an individual student learning profile, a list of objectives, and documentation of the specific services to be provided. Parents may then sign the plan, indicating their agreement and the services will start. Parents also have a right to dispute the results and request an outside opinion. There are a number of models or prototypes for providing special education and the “least restrictive” environment which meets the child’s needs is used. These prototypes range from services provided within a regular classroom, to some services given in a resource room, to all academics taught in a resource room or separate small classroom. When to Watch, When to Refer, When to Reassure Bibliography: 1. First L, Palfrey J. The infant or young child with developmental delay. New England Journal of Medicine 1994; 330:478-483. 2. Dworkin PH. Developmental screening: (still) expecting the impossible? [comment]. Pediatrics 1992; 89:1253-5. 3. Frankenburg W, Dodds J, Archer P, Shapiro H, Bresnick B. The DENVER II: A major revision and restandardization of the Denver Developmental Screening Test. Pediatrics 1992; 89:91-97. 4. Frankenburg W, Dodds J, Archer P, et al. DENVER II: Training Manual. Denver: Denver Developmental Materials, Inc.; 1992 5. American Academy of Pediatrics Committee on Children with Disabilities. Screening infants and young children for developmental disabilities. Pediatrics 1994;93:863-5. 6. Wachtel RC, Shapiro BK, Palmer FB, Allen MC, Capute AJ. CAT/CLAMS. A tool for the pediatric evaluation of infants and young children with developmental delay. Clinical Adaptive Test/Clinical Linguistic and Auditory Milestone Scale. Clinical Pediatrics 1994; 33:410-5. 7. Glascoe FP, Martin ED, Humphrey S. A comparative review of developmental screening tests. Pediatrics 1990; 86:547-54. 8. Dworkin PH. Detection of behavioral, developmental, and psychosocial problems in pediatric primary care practice. Current Opinion in Pediatrics 1993; 5:531-6. 9. Glascoe FP, Dworkin PH. Obstacles to effective developmental surveillance: errors in clinical reasoning. Journal of Developmental & Behavioral Pediatrics 1993; 14:344-9. 10. Glascoe FP, Dworkin PH. The role of parents in the detection of developmental and behavioral problems. Pediatrics 1995; 95:829-36. 11. Green M, editor. Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents. Arlington: National Center for Education in Maternal and Child Health; 1994. 12. Green M, Palfrey, JS, editors. Bright Futures: Guidelines for Health Supervision of Infants, Children, and Adolescents, Second edition. Arlington, VA : National Center for Education in Maternal and Child Health; 2000. Suggested Readings (Annotated) First LR and Palfrey JS. The Infant or Young Child with Developmental Delay. The New England Journal of Medicine 1994;330:478-483. This review article reinforces the importance of early identification of developmental delay and provides a step by step approach in developmental assessment appropriate for the primary care clinician. Gilbride, KE. Developmental Testing. Pediatrics in Review 1995;16(8):338-45. This review article outlines the battery of developmental screening and testing measures most commonly used. It delineates the role of each measure in a child’s overall assessment based on the validity, sensitivity, specificity, and population for which the tests were designed. McInerny TK. Children who have difficulty in school: A primary pediatrician’s approach. Pediatrics in Review 1995;16(9):325-32. This article presents a comprehensive overview of management of school failure in primary care office practice. It includes a discussion of the etiologies, a guide to diagnosis, a list of commonly used tests, and clinician’s guide to management strategies. Resources: The DENVER II Test forms and DENVER II Test Kit, as well as training materials including The DENVER II Training Videotape (Introduction), The DENVER II Item Administration Videotape, The DENVER II Training Manual, and The DENVER II Technical Manual, may be purchased directly from: Denver Developmental Materials, Inc. PO Box 6919 Denver, CO 80206-0919 Tel. 1-800-419-4729