Male genital lymphedema: clinical features and management in 25
advertisement

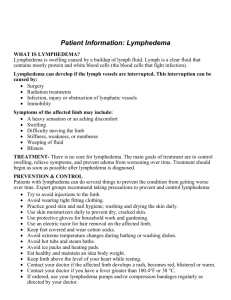
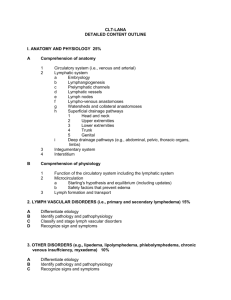
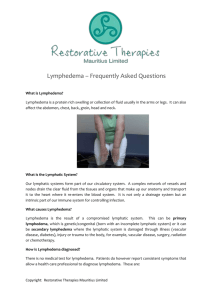
Journal of Pediatric Surgery 49 (2014) 1647–1651 Contents lists available at ScienceDirect Journal of Pediatric Surgery journal homepage: www.elsevier.com/locate/jpedsurg Male genital lymphedema: clinical features and management in 25 pediatric patients☆,☆☆ Carolyn C. Schook a, c, Ann M. Kulungowski b, c, Arin K. Greene a, c, Steven J. Fishman b, c,⁎ a b c Department of Plastic and Oral Surgery, Boston Children's Hospital, Boston, MA 02115, USA Department of Surgery, Boston Children's Hospital, Boston, MA 02115, USA Vascular Anomalies Center, Boston Children's Hospital, Harvard Medical School, Boston, MA 02115, USA a r t i c l e i n f o Article history: Received 13 February 2014 Received in revised form 26 May 2014 Accepted 29 May 2014 Key words: Genital Lymphedema Swelling Lymphatic malformation Vascular anomaly a b s t r a c t Purpose: Genital lymphedema in the pediatric population is poorly understood. The purpose of this study was to determine the epidemiology, morbidity, and treatment outcomes for males with genital lymphedema. Materials and methods: Male patients with genital lymphedema evaluated at our vascular anomalies center between 1995 and 2011 were reviewed. Etiology, age-of-onset, location, morbidity, and treatment were analyzed. Results: Of the 3889 patients with vascular anomalies, 25 (0.6%) had genital lymphedema: 92% (23/25) with primary and 24.0% (6/25) with familial/syndromic lymphedema. For primary disease, the mean age-of-onset was 4.5 ± 6.3 years with 60.9% (14/23) presenting in infancy, 13.0% (3/23) in childhood, and 26.1% (6/23) in adolescence. Combined penoscrotal lymphedema was identified in 72.0% (18/25) of patients; 19 children (76.0%) had concomitant lower extremity involvement. The most common complication was cellulitis (24.0%). Surgical contouring was performed in 44.0% (11/25) of patients. Patients with operative intervention and follow-up (n = 6) had sustained improvement after a median of 4.2 years (range: 0.3–11.0). Conclusions: Lymphedema of the male genitalia is typically idiopathic. Most patients develop swelling in infancy but can present in adolescence and occasionally childhood. The penis and scrotum are usually both involved and concurrent lower-extremity swelling is common. Surgical debulking can improve symptoms and appearance. © 2014 Elsevier Inc. All rights reserveed. Lymphedema is chronic swelling of tissue owing to poor lymphatic function from either anomalous lymphatic development of (primary) or injury to (secondary) lymphatic nodes or vessels. Affected tissue initially swells from accumulation of subcutaneous lymph; resultant inflammation stimulates adipose deposition and fibrosis causing further enlargement over time [1]. Primary lymphedema is uncommon; it affects 1.2 per 100,000 persons less than 20 years of age [2]. Secondary lymphedema affects the majority (90%) of patients, principally the lower extremities of adults, owing to infection or treatment for malignancy [3]. In developing countries, filarial infestation is the most common cause of genital lymphedema [3]. The prevalence of primary genital lymphedema is unknown. Complications of lymphedema include infection, functional disability, and chronic cutaneous changes. Disfigurement from lymphedema, particularly of the genitalia, can cause considerable psychosocial distress. ☆ Statement of financial interest: No financial support or benefits were given to the authors from any source that is related to the scientific work reported in this article. ☆☆ Lists of products used: No products or devices were used in this article. ⁎ Corresponding author at: Department of Surgery, Boston Children's Hospital, 300 Longwood Ave. Boston, MA 02115. Tel.: +1 617 355 3040; fax: +1 617 730 0752. E-mail address: steven.fishman@childrens.harvard.edu (S.J. Fishman). http://dx.doi.org/10.1016/j.jpedsurg.2014.05.031 0022-3468/© 2014 Elsevier Inc. All rights reserveed. Genital lymphedema in the pediatric population is not only infrequent but also poorly understood. Previous reports on genital lymphedema have been limited by small numbers of patients [4–12] and/or are comprised largely of adults [13–19]. Conflicting opinions on the utility of compression therapy [10,14,16,20] and timing of operative interventions (early versus post-pubertal) exist [4,7,10,14,16]. The purpose of this study was to determine the epidemiology, morbidity, and treatment outcome for males with genital lymphedema in an effort to improve patient counseling and offer management options for practitioners. 1. Materials and methods After approval by the Committee on Clinical Investigation at Boston Children's Hospital, the Vascular Anomalies Center database was queried for all male patients with “lymphedema” of the penis and/or scrotum who presented to our center between January 1995 and January 2011. Records were retrospectively reviewed for referring diagnosis, age at presentation and intervention, anatomic location, morbidity, treatment modalities, and outcome. Diagnosis was made by clinical history, physical examination, and/or imaging studies. Age-of-onset was categorized based on physiological age: 1648 C.C. Schook et al. / Journal of Pediatric Surgery 49 (2014) 1647–1651 infancy (b 12 months), childhood (1–9), and adolescence (10–21 years) [21–23]. Data are presented as mean ± standard deviation. Excisional debulking is utilized in our center for lymphedema of the penis and scrotum. The procedures were performed by two surgeons in the following manner. The genitalia are prepared and draped widely and a urinary catheter of the largest size that can be easily inserted is placed. For penile lymphedema, a circumferential incision is made in the penile skin several millimeters proximal to the corona of the glans penis, using the scar from previous circumcision, if relevant. The skin of the shaft of the penis is then dissected just below the dermis circumferentially to the base. The entirety of the shaft skin is unfurled proximally using blunt, sharp, and/or cautery dissection. The underlying lymphedematous adipose tissue is then dissected off Buck's fascia circumferentially. Care is taken to avoid injury to the skin, neurovascular bundles, or urethra. Once the lymphedematous tissue is removed, the redundant skin is advanced back down the penile shaft. Excess circumference of skin is resected to leave just enough to comfortably wrap the penile shaft. When possible, the least abnormal skin is saved for penile coverage, discarding as much of the skin containing vesicles, dimples, or fibrosis. The skin is approximated to create a longitudinal scar at the ventral midline. The excess length of skin is excised to facilitate reapproximation at the distal precoronal incisional location. A small round closed-suction drain is placed under the skin flap, positioned dorsally away from the urethra and brought out in a suprapubic position. Interrupted intradermal absorbable sutures followed by a running subcuticular suture are used for closure. A penile block with 0.25% bupivacaine is performed prior to dressing the wound. The penis is gently wrapped with circumferential gauze, leaving the urinary catheter in place for 24 hours. For scrotal lymphedema, a lenticular incision is made vertically encompassing the median raphe or transversely at the most dependent portion of the scrotum. The testes and spermatic cord structures are identified and protected. A full thickness wedge of scrotal tissue, encompassing skin, adipose tissue and dartos is excised. If hydroceles are present, the tunica vaginalis is similarly excised. The excess scrotal septum is resected and the testes are secured with nonabsorbable sutures to the reduced septum. Scrotoplasty is performed to create a new midline raphe or transverse closure parallel to the rugae. In cases of extreme scrotal enlargement, additional redundant tissue is resected from the lateral aspect of each hemi-scrotum and closed in a V-Y advancement fashion. Closure is accomplished with multiple layers of absorbable suture in the tunica vaginalis, dartos, subcutaneous tissue, and skin. Post-operative scrotal elevation is employed for 1 week and patients are encouraged to wear a compressive undergarment thereafter. 2. Results Of the 3889 male patients with a vascular anomaly, 25 (0.6%) had lymphedema of the genitalia. Primary lymphedema occurred in 92.0% (23/25) of patients and six children (24.0%) had syndromic or familial lymphedema [Noonan syndrome (n = 2), lymphedema–distichiasis (n = 2), and Milroy disease (n = 2)] (Table 1). Two patients (8.0%) Table 1 Characteristics of genital lymphedema in 25 male pediatric patients. Etiology Age of onset Location Primary Familial/syndromic Secondary Infancy Childhood Adolescence Genital Combined penile and scrotal Isolated scrotal Isolated penile Associated lower extremity involvement 92.0% 24.0% 8.0% 60.9% 13.0% 26.1% (23/25) (6/25) (2/25) (14/23) (3/23) (6/23) 72.0% 24.0% 4.0% 76.0% (18/25) (6/25) (1/25) (19/25) had secondary lymphedema from operative intervention for undescended testes (n = 1) or non-infectious granulomatous disease (n = 1). Average age of onset was 4.5 ± 6.3 years (range: 0 to 15). Fourteen (60.9%) patients presented in infancy. Childhood onset occurred in 13.0% (3/23) of patients; the remaining 26.1% (6/23) presented during adolescence. The referring diagnosis was accurate in 64.0% (16/25) of patients; the most common erroneous diagnosis was capillary-lymphatico-venous malformation (Klippel-Trenaunay syndrome). Diagnosis was made by history and physical examination in almost all patients. No adjunctive imaging studies were performed in 8.0% (2/25) of children. MRI [72.0% (18/25)] and/or lymphoscintigraphy [36.0% (9/25)] were reviewed when available; of these studies, most were obtained at prior institutions or primarily for evaluation of non-genital anomalies. Pathologic specimens were reviewed in addition to imaging and clinical evaluation in nine (36.0%) children. Penoscrotal lymphedema was identified in 72.0% (n = 18) of patients. Isolated scrotal and penile disease was found in 24.0% (n = 6) and 4.0% (n = 1) of patients, respectively. Concomitant involvement of the lower extremities occurred in 76.0% (n = 19) of children. Genitourinary symptoms were observed in 60.0% (n = 15) of patients and included hematuria [12% (n = 3)], altered urinary mechanics [8.0% (n = 2)], and phimosis [8.0% (n = 2)] (Table 2). Additional morbidities included cellulitis [24.0% (n = 6)], lymphorrhea [24.0% (n = 6)], and skin changes [12% (n = 3)]. Treatment was administered to 72.0% (18/25) of patients; seven (28.0%) children were observed (Table 3). Compression therapy was prescribed to 12 patients (48.0%). Of the patients receiving compression therapy, four (33.3%) later received surgical debulking. Contouring to improve symptoms and/or the appearance of the genitalia was performed in 44.0% (n = 11) of patients with a mean of 1.5 ± 1.0 procedures per patient. One patient underwent concomitant debulking of a lymphedematous lower extremity. Initial operative intervention occurred at average 13.9 ± 8.0 years of age. Post-operative complications (n = 2) included the appearance of granulomatous tissue along a penile shaft suture line that improved with time and a superficial wound infection treated with antibiotics. Post-operative follow-up was available for 54.5% (6/11) of patients with surgical procedures at a median of 4.2 years (range: 0.3–11.0). All patients with operative treatment and follow-up had sustained improvement. 3. Discussion Genital lymphedema is an uncommon but troubling cause of deformity of the male genitalia. The epidemiology and morbidity are unclear in part owing to the rarity of the condition. Furthermore, diagnostic criteria, timing of therapies, and surgical techniques have been debated. To our knowledge, this is the largest series of male pediatric patients with genital lymphedema. The etiology of genital lymphedema in children in the United States is predominately idiopathic. While most patients develop symptoms in infancy or early childhood, the diagnosis is often delayed for several years. Lymphedema is most commonly confused with other vascular anomalies, particularly if the lower extremities are also affected. An accurate diagnosis is imperative in providing appropriate Table 2 Complications of genital lymphedema in 25 male pediatric patients. Cellulitis Lymphorrhea Skin changes Hematuria Pain Bleeding Altered urinary mechanics Chylous reflux Phimosis Dysuria 24.0% 24.0% 12.0% 12.0% 8.0% 8.0% 8.0% 8.0% 8.0% 4.0% (6/25) (6/25) (3/25) (3/25) (2/25) (2/25) (2/25) (2/25) (2/25) (1/25) C.C. Schook et al. / Journal of Pediatric Surgery 49 (2014) 1647–1651 Table 3 Treatment of genital lymphedema in 25 male pediatric patients. Observation only Compression therapy Contouring/debulking Mean number of procedures Mean age at first intervention Follow-up available Median years of follow-up Sustained improvement Other Hydrocele repair/aspiration Orchidopexy Circumcision Urethral meatotomy 28.0% (7/25) 48.0% (12/25) 44.0% (11/25) 1.5 ± 1.0 13.9 ± 8.0 years 54.5% (6/11) 4.2 (range: 0.3–11.0) years 100.0% (6/6) 56.0% (14/25) 36.0% (9/25) 16.0% (4/25) 8.0% (2/25) 4.0% (1/25) counseling and treatment. History and physical examination are the primary mode of diagnosis, followed by imaging in limited cases. Initial evaluation of male genital lymphedema includes a precise history to rule-out secondary causes such as trauma, infection, prior radiation therapy, or surgery. Non-infectious granulomatous disease has been linked with lymphedema in children, affecting one patient in our series, and is likely related to an inflammatory process (e.g. Crohn's disease) [24,25]. Family history and extraneous physical findings should be evaluated as lymphedema occasionally can be syndromic or inherited. Milroy disease is lower extremity lymphedema at birth with a family history of the condition; Meige disease is similar but presents in adolescence [26,27]. Lymphedema in both Milroy and Meige disease can extend to the genitalia. Noonan syndrome, diagnosed either by clinical evaluation or genetic testing, consists of short stature, webbed neck, low-set ears, and cardiac anomalies; lymphedema is a secondary finding [28]. Lymphedema can also occur with distichiasis (an extra row of eyelashes arising from the meibomian glands) [29]. To our knowledge, no syndromic or familial form of lymphedema has been linked uniquely to the genitalia. In all forms of lymphedema, the lower extremities are often concurrently involved, although isolated genital disease does occur. The scrotum is involved in almost all patients. Combined penoscrotal disease is the most common presentation. Isolated penile enlargement is rare although disease limited to the scrotum is more common. Pitting edema and minimal cutaneous changes are present in early disease; non-pitting overgrowth will occur over time from adipose deposition and fibrosis. History and physical examination are rarely equivocal. Nevertheless, some of our patients had confirmatory lymphoscintigraphy prior to referral. Delayed transport and/or dermal backflow of radiolabeled colloid indicate lymphatic dysfunction with 92% sensitivity and 100% specificity [30]. Lymphoscintigraphy can be performed either by scrotal injection when isolated genital disease occurs or injection of the foot if the lower limbs are involved. If lateralization of labeled colloid is less clear 1649 with an extremity lymphoscintigram, a dedicated genital examination may be indicated. Ultrasonography is less specific and CT entails radiation to the testes. MRI can be particularly useful to distinguish other vascular anomalies, such as venous or lymphatic malformation, from lymphedema, and can also be of value in operative planning. Biopsy should be utilized only if malignancy or other conditions, such as non-infectious granulomatous disease, are suspected. Once the diagnosis of lymphedema is made, symptomatic treatment should be initiated. Lymphedema can adversely influence a patient's quality of life both functionally and emotionally. Our study indicated that forty-percent of patients will have no symptoms beyond enlargement of the genitalia; however, the psychosocial consequences of disfigurement should not be trivialized particularly in a developing child. Emotional health should be screened in all patients; a formal psychiatric assessment may be indicated in some children. For those patients with additional somatic symptoms, cellulitis, lymphorrhea, and skin changes were most common. Cellulitis is a potentially life-threatening consequence of lymphedema. It was observed in a quarter of our patients. The presence of cellulitis mandates prompt treatment with oral or intravenous antibiotics depending upon severity. A patient experiencing three or more episodes of cellulitis per year may benefit from a prophylactic lowdose regimen of antibiotics. Infection prevention includes daily washing of the genitalia and application of a moisturizing agent to prevent desiccation and breakdown of the skin. The primary goal of conservative lymphedema treatment is to minimize stagnant lymph accumulation to prevent progression and improve contour. Pharmacologic treatment has thus far been limited. Preliminary investigations, suggest that angiogenesis and vasculogenesis play no role in the expansion of lymphedema; therefore, angiogenic inhibitors are not indicated [31]. Compression therapy with stockings or fitted garments is the mainstay of non-operative treatment in patients with lower extremity lymphedema [32]. Because of the shape and location of genital lymphedema, wrapping and stocking material can be difficult to apply and may require ingenuity on behalf of the patient and family. Applying fitted compression stockings to a growing infant is often impractical. Many patients utilize over-the-counter elastic shorts. Some patients also place a wedge under the pelvis to elevate the genitalia at night to improve lymphatic return. The merits of compression and elevation therapy in genital lymphedema are mixed and should be weighed against inconvenience to the patient [4,7]. However, in our experience, as well as others, compression therapy is a useful tool to maintain and even reduce genital size when tolerated [16]. Postoperatively, penile wrapping is particularly effective at minimizing recurrent swelling. Surgical treatment of genital lymphedema is indicated for patients with significant morbidity who have failed non-operative management. In our center, operative indications include excessive size, Fig. 1. Operative debulking of male genital lymphedema. (Left) Patient at 12 years of age with swelling of the penis and scrotum. Patient has had lymphedema since birth; surgical intervention was delayed until puberty was completed. (Middle) Intraoperative appearance of debulking procedure. (Right) Three month follow-up demonstrates an improved contour. 1650 C.C. Schook et al. / Journal of Pediatric Surgery 49 (2014) 1647–1651 Fig. 2. Surgical debulking of male scrotal lyphedema. He had previously undergone contour resection of the penile shaft. The scrotum is large and pendulous. (Left) Pre-operative appearance of scrotum with area of resection marked. (Middle) Intraoperative appearance of debulking procedure. (Right) Follow-up appearance of scrotum. functional impairment, and/or disfigurement (Fig. 1). The optimal operative technique and timing remain controversial. There are two surgical approaches to lymphedema: physiological or excisional. Physiologic procedures, which include local flap transfers and lymphaticovenous anastomoses, have shown inconsistent benefits in the treatment of extremity lymphedema. In the genitalia, these procedures mostly have been abandoned owing to inefficacy. Excisional procedures remove lymphedematous tissue with or without excision of the overlying skin. We favor excisional intervention at our center for both penile and scrotal debulking (Fig. 2). There are alternative surgical techniques for debulking the penis and scrotum largely related to placement of the incisions, such as a transverse incision at the base of the penis or scrotum [33]. That approach has the advantage of avoiding scars on the penile shaft. However, with that incision, excess skin circumference cannot be removed from the penis. We prefer to remove as much redundant skin as possible to minimize re-enlargement. The small amount of residual subcutaneous tissue can thicken over time. Thus, removing excess skin leaves less subcutis to contribute to future girth regrowth. The key to removing excess lymphedematous tissue particularly along the penile shaft is to maintain sufficient vascular attachment both proximally and distally to avoid wound ischemia. A ventrally located incision in the scrotum has been reported to result in an unsatisfactory result. If there is re-growth of lymphedematous tissue on either side of the scar, the scrotum may assume a labia-like appearance [34,35]. We exercise care in reconstructing the scrotal septum with no tension and did not observe this outcome in our patients. Minimization and thoughtful placement of incisions are crucial as lymphedematous tissue is prone to wound break down and weeping. Because excisional procedures do not treat the underlying pathology, postoperative compression is still required after resection to prevent the re-accumulation of lymph and ongoing deposition of adipose tissue. Multiple staged serial excision procedures may be necessary over the patient's lifetime owing to recurrence. The optimal timing of the genital debulking procedures is controversial. Some argue for early intervention to minimize the physical and emotional strain on a pediatric patient [13]. In our center, we prefer to delay surgical intervention until pubertal changes to avoid overcorrection as well as to facilitate the procedure by operating on larger structures. In extreme cases, conservative early debulking can be performed with the expectation of potential additional intervention when the child is older (Fig. 3). Some patients with genital lymphedema will have a concurrent hydrocele, undescended testes, and/or chylous reflux. These conditions can be addressed at the time of the debulking. Conversely, older patients with these additional diagnoses but moderate lymphedema may desire debulking at the time of their correction when no intervention for the lymphedema would otherwise be undertaken. Like any procedure in the pediatric population, the exact timing of intervention should be weighed considering the extent of deformity, functional impairment, and psychological disturbance. All patients and their families should be properly counseled regarding their expectations. Disfigurement can be greatly improved, but the genitalia will likely never appear completely normal. There are several limitations to our study. Most important is its retrospective nature. Additionally, many patients were initially managed at outside institutions and referred to our center. This allows for gaps in the medical record and fewer surgical patients returning for follow-up. 4. Conclusions Lymphedema of the male genitalia is typically idiopathic and usually concomitantly involves the lower extremities. Most patients experience swelling in infancy and early childhood; the remaining patients present in adolescence. Psychosocial morbidity is common. Infection and lymphatic leak may occur in as many as a quarter of patients. Compression therapy may limit worsening or improve Fig. 3. Operative reconstruction of male genital lymphedema. Because of distortion of penile tissue, skin changes, and phimosis, conservative debulking with penile reconstruction by adjacent tissue advancement flap closure was performed on 17 month old patient with distichiasis–lymphedema. Right inguinal orchidopexy was also performed for undescended testis. (Left) Pre-operative penile deformity. (Middle) One week post-resection. (Right) Seven month follow-up demonstrating sustained improvement. C.C. Schook et al. / Journal of Pediatric Surgery 49 (2014) 1647–1651 swelling in early disease but can be difficult to implement. Contour resection can decrease bulk, improve appearance, and minimize psychosocial impairment. Optimally, operative intervention is postponed until after pubertal changes to the genitalia occur to avoid overcorrection and facilitate the procedure because of enlarged structures. When necessary, patients with significant overgrowth or other genitourinary symptoms can have conservative debulking in childhood. Regardless of initial age at intervention, serial excisions may be necessary for sustained improvement because of recurrence. Acknowledgments Dr. Kulungowski was supported by the Stuart and Jane Weitzman Fellowship in Vascular Anomalies. References [1] Brorson H. Adipose tissue in lymphedema: the ignorance of adipose tissue in lymphedema. Lymphology 2004;37:175–7. [2] Smeltzer DM, Stickler GB, Schirger A. Primary lymphedema in children and adolescents: a follow-up study and review. Pediatrics 1985;76:206–18. [3] WHO ECR: Lymphatic filariasis. Fourth report of the WHO Expert Committee on Filariasis. World Health Organ Tech Rep Ser 1984;702:3–112. [4] Dijkstra JW, Bergfeld WF, Kay R. Congenital lymphedema of genitalia and extremities. Cleve Clin Q 1984;51:553–7. [5] Yormuk E, Sevin K, Emiroglu M, et al. A new surgical approach in genital lymphedema. Plast Reconstr Surg 1990;86:1194–7. [6] Steinberg J, Kim ED, McVary KT. A surgical approach to penoscrotal lymphedema. J Urol 1996;156:1770. [7] Bolt RJ, Peelen W, Nikkels PG, et al. Congenital lymphoedema of the genitalia. Eur J Pediatr 1998;157:943–6. [8] Ross JH, Kay R, Yetman RJ, et al. Primary lymphedema of the genitalia in children and adolescents. J Urol 1998;160:1485–9. [9] Shenoy VG, Jawale SA, Oak SN, et al. Primary lymphedema of the penis: surgical correction by preputial unfurling. Pediatr Surg Int 2001;17:169–70. [10] McDougal WS. Lymphedema of the external genitalia. J Urol 2003;170:711–6. [11] Hornberger BJ, Elmore JM, Roehrborn CG. Idiopathic scrotal elephantiasis. Urology 2005;65:389e14–5. [12] Kumar P, Navaneethan GP. Resection of scrotal lymphedema. Plast Reconstr Surg 2005;116:24e–7e. [13] Das S, Tuerk D, Amar AD, et al. Surgery of male genital lymphedema. J Urol 1983;129:1240–2. [14] Modolin M, Mitre AI, da Silva JC, et al. Surgical treatment of lymphedema of the penis and scrotum. Clinics (Sao Paulo) 2006;61:289–94. 1651 [15] Servelle M. Surgical treatment of lymphedema: a report on 652 cases. Surgery 1987;101:485–95. [16] Garaffa G, Christopher N, Ralph DJ. The management of genital lymphoedema. BJU Int 2008;102:480–4. [17] Halperin TJ, Slavin SA, Olumi AF, et al. Surgical management of scrotal lymphedema using local flaps. Ann Plast Surg 2007;59:67–72. [18] Apesos J, Anigian G. Reconstruction of penile and scrotal lymphedema. Ann Plast Surg 1991;27:570–3. [19] Zacharakis E, Dudderidge T, Ioannidis E. Surgical repair of idiopathic scrotal elephantiasis. South Med J 2008;101:208–10. [20] Sun GC, Zhong AG, He W, et al. Reconstruction of the external genitals and repair of skin defects of the perineal region using three types of lateral groin flap. Ann Plast Surg 1990;24:328–34. [21] Herman-Giddens ME, Slora EJ, Wasserman RC, et al. Secondary sexual characteristics and menses in young girls seen in office practice: a study from the Pediatric Research in Office Settings network. Pediatrics 1997;99:505–12. [22] Rudolph C, Rudolph A, Lister G, et al. Rudolph's pediatrics. New York, NY: McGraw-Hill; 2003. [23] Lee PA. Normal ages of pubertal events among American males and females. J Adolesc Health Care 1980;1:26–9. [24] Murphy MJ, Kogan B, Carlson JA. Granulomatous lymphangitis of the scrotum and penis. Report of a case and review of the literature of genital swelling with sarcoidal granulomatous inflammation. J Cutan Pathol 2001;28:419–24. [25] Saha M, Edmonds E, Martin J, et al. Penile lymphoedema in association with asymptomatic Crohn's disease. Clin Exp Dermatol 2009;34:88–90. [26] Feins NR, Greene AK. Primary lymphedema. In: Mulliken JB, Burrows PE, Fishman SJ, editors. Mulliken and Young's vascular anomalies: hemangioma and malformations. New York, NY: Oxford University Press; 2013. p. 1056–76. [27] Milroy W. An undescribed variety of hereditary oedema. N Y Med J 1892;56:505–17. [28] Noonan JA. Hypertelorism with Turner phenotype. A new syndrome with associated congenital heart disease. Am J Dis Child 1968;116:373–80. [29] Falls HF, Kertesz ED. A new syndrome combining pterygium colli with developmental anomalies of the eyelids and lymphatics of the lower extremities. Trans Am Ophthalmol Soc 1964;62:248–75. [30] Gloviczki P, Calcagno D, Schirger A, et al. Noninvasive evaluation of the swollen extremity: experiences with 190 lymphoscintigraphic examinations. J Vasc Surg 1989;9:683–9. [31] Cuoto RA, Kulungowski AM, Chawla AS, et al. Expression of angiogenic and vasculogenic factors in human lymphedematous tissue. Lymphat Res Biol 2011;9:143–9. [32] Moseley AL, Carati CJ, Piller NB. A systematic review of common conservative therapies for arm lymphoedema secondary to breast cancer treatment. Ann Oncol 2007;18:639–46. [33] Feins NR. An new surgical technique for lymphedema of the penis and scrotum. J Pediatr Surg 1980;15:787–9. [34] Dandapat MC, Mohapatro SK, Patro SK. Elephantiasis of the penis and scrotum: a review of 350 cases. Am J Surg 1985;149:686–90. [35] Bulkley GJ. Scrotal and penile lymphedema. J Urol 1962;87:422–9.