Annual Report for 2006 - National Centre for Medical Genetics
advertisement

National Centre for Medical Genetics
Ionad Náisiúnta Gineolaíocht Leighis
Director: Professor Andrew J Green, MB, PhD, FRCPI, FFPath(RCPI)
National Centre for
Medical Genetics
Annual Report
2006
Foreword by Director
I am delighted to introduce the 2006 annual report from the National Centre for Medical Genetics
(NCMG). Despite the increasing pressures due to major increases in the numbers of samples received for
genetic testing, our hard working and committed Laboratory, Clinical, and Administrative staff, have
continued to make great strides in developing the service for the benefit of all the families in Ireland who
are affected by genetic disease.
However, we remain disappointed that we are not yet in a position to provide a truly national laboratory
genetics service. A privately funded genetics laboratory at NUI Galway , which had formerly carried out
5,000 genetics tests annually, closed in 2005. The NCMG applied to the HSE (then ERHA) for €1.5 million
to fund the costs of undertaking these tests. However, only half this amount was made available, and so
the NCMG has not been able to provide an equitable laboratory service for the whole country. This
inequitable laboratory service primarily affects the West and North West of Ireland. The NCMG also has
concerns over the outsourcing of these genetic tests abroad, in the absence of a national service, to some
laboratories where there may be quality issues. We hope the balance of funds requested will be made
available, to enable a truly national service, and we continue to work with the Health Service Executive
(HSE) and The Department of Health & Children (DoHC) to meet this aim.
In 2006, we consolidated the Clinical and Laboratory staff who were appointed from a major expansion
in 2005 — this expansion was primarily due to the transfer of services from the aforementioned closure of
the NUI Galway Genetics Laboratory. We were also delighted that the NCMG, along with University
College Dublin and Trinity College Dublin, obtained a €5 million grant from the Health Research Board
to fund work on the Autism Genome Project; a worldwide collaboration of 16 research centres working to
define the genetic basis of Autism.
The NCMG also has a major deficit in the number of Clinical staff compared to sister units abroad. The
UK Royal College of Physicians recommends 2 general Consultant Geneticists per million population,
and therefore the NCMG should have a minimum of 8 Consultants, rather than the 3 currently in place.
The NCMG has also had great difficulty in filling a permanent 4th consultant post, with an interest in
cancer genetics.
The NCMG continues to work closely with the management of Our Lady’s Children’s Hospital Crumlin
(OLCHC), the HSE, and the DoHC, to develop our services, aiming to provide a service comparable with
our sister genetic services across Europe.
I hope that in 2007, many of the deficits and concerns over the level of service which the NCMG can
supply will be addressed by our funding agencies. We are also working towards external accreditation
of our laboratories, which will independently establish the NCMG as a centre of quality for genetic tests.
Finally, I am deeply grateful to the many NCMG staff who contributed to this annual report, especially
Damien Moyles, NCMG General Manager.
________________________________
Prof. Andrew Green
NCMG Director
Page I
Table of Contents
Introduction ........................................................................................................................................................1
Clinical Genetics Division.................................................................................................................................2
Clinical Links With Other Genetic Departments .................................................................................3
Clinical Activity........................................................................................................................................4
Cytogenetics Division........................................................................................................................................5
Cytogenetics Activity ..............................................................................................................................6
Molecular Genetics Division ............................................................................................................................8
Molecular Genetics Activity ...................................................................................................................9
Service downgraded as Samples are sent Abroad for Testing.........................................................11
Clinical/Laboratory Liaison Meetings...........................................................................................................12
Research.............................................................................................................................................................13
Amyotrophic Lateral Sclerosis .............................................................................................................13
Autism .....................................................................................................................................................13
Vesicoureteral Reflux.............................................................................................................................14
SNiP2CHIP..............................................................................................................................................15
EuroGentest ............................................................................................................................................16
Rare Single Gene Disorders ..................................................................................................................16
NCMG Multidisciplinary Committees .........................................................................................................17
Management/Accreditation ..................................................................................................................17
Health & Safety.......................................................................................................................................17
Training & Education ............................................................................................................................18
Quality .....................................................................................................................................................18
Administration Team ......................................................................................................................................19
Training .............................................................................................................................................................20
In-house Training Courses run by NCMG .........................................................................................20
External Courses Attended...................................................................................................................20
NCMG Publications.........................................................................................................................................21
Audits ................................................................................................................................................................22
Meetings Attended ..........................................................................................................................................23
Presentations.....................................................................................................................................................24
Poster Presentations.........................................................................................................................................25
External Quality Assessment Scheme—Assessors & Organisers..............................................................26
Teaching ............................................................................................................................................................27
Administrative Research Activities .....................................................................................................27
NCMG Staff Photo ...........................................................................................................................................28
Page II
Annual Report 2006
Introduction
The National Centre for Medical Genetics (NCMG) was set up in late 1994 in Our Lady’s Children’s
Hospital Crumlin, with the objective of providing a clinical and laboratory genetic service for those
affected by or at risk of a genetic disorder. Initially the NCMG had 18 staff, and provided a limited
service for the Greater Dublin area, and the Eastern seaboard. In 2006 this number was 68.6 whole
time equivalent (WTE) staff employed in the NCMG, in addition to a number of research staff.
There are three division in the NCMG, each is individually distinct and unique.
These three
divisions are:.
Clinical Genetics
Cytogenetics
Molecular Genetics
The framework, within which this annual report is set, is the Harper report of 1998, commissioned
and subsequently accepted by the Department of Health and Children. The Harper report states that
the National Centre for Medical Genetics should follow the model of service delivery for other
European countries.
It recommended that a single integrated genetic service provides for a
population of 4 million people. The report recommends that there should be a centralised laboratory
service which analyses samples from the whole country, and a clinical service which provides clinics
on the basis of need on a "hub and spoke" model, with a central administrative base at the National
Centre for Medical Genetics.
This comprehensive Annual Report was produced by the staff of the National Centre for Medical
Genetics, and endorsed and adopted by the Director and Laboratory Heads of the National Centre
for Medical Genetics. In reading this report the large increases in workload of all three divisions in
the NCMG, since 2000, should be taken into account.
Page 1
Clinical Genetics Division
The National Centre for Medical Genetics offers genetic clinics and counselling to all residents of the
Republic of Ireland. As a national service, the clinics are free. The NCMG holds clinics in two major
paediatric hospitals in Dublin; Our Lady’s Children’s Hospital Crumlin, where the centre is based,
and The Children’s University Hospital, Temple Street. Peripheral clinics in Cork, Galway and
Limerick are held regularly throughout the year.
The waiting times for these clinics are
approximately three to four months for most clinics. Some peripheral clinics have longer waiting
times. Patients can be seen privately if requested.
The NCMG see families with all types of genetic disorders ranging from single gene disorders such
as Cystic Fibrosis, Huntington disease, Duchenne muscular dystrophy, and neurofibromatosis,
through to families with a history of breast or bowel cancer. The NCMG are also asked to see
children with birth defects such as cleft lip/palate, cardiac defects, kidney problems and limb
anomalies. In addition, a large part of the workload includes seeing children with developmental
delay of unknown cause. The remit is to see whether the NCMG can make a diagnosis in these
difficult cases. Clinical Genetics, as a speciality, involves dealing with both children and adults.
Over 50% of our referrals are adults. Historically, Clinical Genetics arose from paediatrics and is still
thought of as a paediatric speciality. However, the service had changed and adult genetics disorders
such as Huntington disease, Charcot-Marie-Tooth, Spino-cerebellar ataxias, and cancer genetics,
forms an important part of our remit.
In 2006 there were three Consultant Geneticists, six Genetic Counsellors (two of which are parttime), and five clinical administrative staff employed in the clinical section. Ms Marie Meany, a
Genetic Counsellor, joined NCMG from Northwick Park, London in June 2006.
Like many other sectors of the Irish health service, the Clinical Division of NCMG is seriously under
resourced. The United Kingdom’s Royal College of Physicians recommends there should be at least 2
whole time-equivalent Consultants per million of population, for both cancer and general Genetics,
with two genetic counsellors per Consultant.
In order to meet these United Kingdom
recommendations the NCMG requires a further 5-6 extra full-time consultants and a further 13
counsellors. {From RCP consultant physicians working with patients latest version (page 83) http://
www.rcplondon.ac.uk/pubs/books/cpwp/ConsPhys2.clingenetic.pdf }.
Page 2
Annual Report 2006
In Northern Ireland, where there are 1.69 (UK 2001
census) million residents, there are five full time
consultants and 6.5 counsellors. In the Republic,
there are three full-time consultants and 4.3
counsellors for 4.5 million residents, and this
inevitably leads to a compromise in the service.
The NCMG cannot offer joint specialist clinics, or
even specialist clinics within Genetics, unlike our
European counterparts.
Other activity that is
affected by this staff shortage includes allowing
time for staff to undertake clinical audit and/or research.
Clinical Links With Other Genetic Departments
The NCMG had two joint meetings with the Clinical Genetics Team from Belfast in 2006. The first
one was hosted by the Belfast group on 18th January 2006, the second meeting was hosted by NCMG
in Dublin on 14th June 2006. NCMG presented audits on Trisomy 13 & 18 from both centres and also
had a case discussion at the end of the day. Dr Alan Irvine, Consultant Dermatologist at Our Lady’s
Children’s Hospital Crumlin, was the invited speaker and spoke on a number of Genetic skin
disorders.
The NCMG had an away day at the Conway institute on the 4th October 2006. The main aim was to
update the centres protocols and procedures. The centre was fortunate to have Dr Nuala Murphy,
Consultant Paediatric Endocrinologist, talk about Disorders of Sexual Development, Dr Eileen
Treacy spoke on new treatments for inherited metabolic disease, and Dr Raveen Shahdadpuri spoke
on the management of children with Sickle cell anaemia.
Multidisciplinary Meetings
The NCMG held its first Neurology/Radiology/Genetics multidisciplinary meeting on 26th January
2006. This involved case discussion plus a presentation on ataxia telangectasia by Dr N Ni Shuibne.
The centre held a joint Genetics/Dermatology meeting on 14th June 2006.
This involved case
discussion. Staff from the NCMG attended a number of multidisciplinary endocrine meetings on 16th
March, 15th June & 28th Sept 2006. These meetings were organised by the paediatric endocrine teams
in both Our Lady’s Children’s Hospital Crumlin and the Children’s University Hospital Temple
Street.
Page 3
Clinical Activity
In 2006 the NCMG sent out 2,627 public appointments; 2,017 (76.7%) families attended with the
remainder 596 (23.3%) either cancelling their appointment 333 (12.3%)or failing to attend/unspecified
263 (10%). Of the 2,017 families who attended 872 (43.2%) were seen by genetic counsellors. The
remainder 1,346 (56,8%) were seen by one of the three Consultants, sometimes in conjunction with
the paediatric registrar. These 2,017 public individual and family appointments equated to 4,225
public patients seen in 2006. An additional 137 families (253 patients) elected to be seen privately – 5
of these did not attend and 21 private patients cancelled.
In 2006 42% of NCMG clinics (1,127 appointments sent: 1,922 patients attended) were held offsite;
this is a similar percentage as 2005.
The highest number of patients seen offsite was in The
Children’s University Hospital Temple Street (584 offered appointments and 948 patients attended).
In addition to this there were 543 appointments offered in outreach peripheral clinics, where 974
attended. These included Limerick Regional Hospital 190 appointments (12 did not attend, 34
cancelled, 368 patients were seen), University College Hospital Galway 171 appointments (9 did not
attend, 32 cancelled, 301 patients seen), St. Finbarr’s Hospital Cork 182 appointments (16 did not
attend, 20 cancelled, 291 patients were seen) and Letterkenny General Hospital 10 appointments,
with 14 patients seen.
In addition, there were 340 ward referrals in total, all were seen by one of the consultants: 215 in our
Lady’s Children’s Hospital Crumlin, 52 ward referrals in The Children’s University Hospital Temple
Street, 13 in the Rotunda Hospital, 13 in the Coombe Hospital, and 36 in the National Maternity
Hospital. These referrals amounted to 668 patients seen.
The tables below provides a summary of this activity:
No. Appointments & Referrals
Total
Attended
2,017
Cancelled
333
Not attended
202
Not specified
51
Total Appointments
2,627
Total Numbers of Patients Seen
4,225
Page 4
Annual Report 2006
Cytogenetics Division
Cytogenetics is the study of chromosomes and disorders which form a major category of genetic
disease. The incidence of chromosome abnormalities is relatively common in the population. In a
clinical setting chromosome abnormalities account for a large proportion of cases involving
spontaneous miscarriages, individuals with congenital malformations, mental retardation, or
infertility. Additionally, the field of Cytogenetics is now important in the workup of patients with
Haematologic/Oncologic disorders. Cytogenetics is a labour intensive process which involves the
culture, harvest, and analysis of the genetic make up of a cell. Currently, the NCMG Cytogenetics
Laboratory provides a broad range of services incorporating prenatal & postnatal diagnosis, and
haematologic/oncologic disorders. These studies include both traditional Cytogenetic techniques as
well as Molecular Cytogenetics by Fluorescent In-Situ Hybridisation (FISH).
Results generated by Cytogenetic techniques continue to play a major role in clinical decisions at
both the constitutional and oncology level. Indeed the further increase in sample numbers
compared to 2005 is witness to this. Unfortunately, this increase in workload has had to be
undertaken by the same staffing levels. As previously identified in 2005 there remained the situation
in 2006 whereby the Cytogenetic Division was unable to meet the demand from Hospitals,
Consultants, and General Practitioners, to provide a national Cytogenetic service. The Oncology
section, while now offering a service to all hospitals, still provided an incomplete service as only
selected disease types or tests could be analysed. The primary reason for this continued to be the
inadequate staffing levels in the laboratory.
A further major factor in 2006 was the absence of a Chief Cytogeneticist, due to the appointed
applicant ultimately not taking the job and the need to re-advertise at the end of the year. Indeed the
position remained unfilled until August 2007. The inadequate staffing levels of the laboratory and
the absence of a Chief Cytogeneticist had the further knock on effect that development of new tests
or improvements in existing tests was limited in 2006. With a further increase in sample numbers
projected for 2007, there will continue to exist an unsatisfactory state of affairs whereby the National
Centre cannot offer a full range of Cytogenetic tests for the whole of the country. Therefore, some
hospitals continue to have to send their samples abroad with the inherent costs this entails.
Despite being unable to take on new hospitals the department processed 6,194 samples, an increase
of 15% compared to 2005. The majority of the extra samples were either constitutional bloods or
bone marrows. Increases were seen with other sample types, although the number of amniocentesis
and CVS remained stable.
________________________________
Mr David Betts
Chief Cytogeneticist
Page 5
Cytogenetics Activity
As previously outlined; the Cyotgenetics Division processed 6,194 samples in 2006, this was an
increase of 15% compared to 2005. The breakdown of this activity is show in the following table:
Sample type
2005
2006
Blood (Constitutional)
3,074
3,430
Amnio
212
217
CVS
95
92
Tissue
127
141
Fixed cells
89
122
1,681
2182
Other Neoplasia
1
7
Others
3
3
5,282
6,194
Haematology (Bone marrow or blood)
Total
Increases in the number of fluorescent in situ
hybridisation (FISH) tests continued, mirroring a
theme that is faced by most cytogenetic laboratories
worldwide with the increasing number of available
commercial probes. This is seen particularly in
oncology where there has been an explosion in the
availability of clinically relevant probes.
A
breakdown of number of FISH tests performed by
section is show in the following table:
FISH Tests
Total Constitutional
Page 6
Number of tests
619
Total Oncology
1,141
Total FISH tests
1,760
Annual Report 2006
The majority of FISH analyses for constitutional defects were for known microdeletion syndromes,
of which approximately 4% were found to be abnormal. In addition 49 subtel screens were
performed of which 2 were abnormal. A breakdown of this is shown in the following table:
Microdeletion
Total tests (abnormal)
22q
366 (12)
Prader Willi
65 (2)
Williams
29 (2)
Miller-Dieker
5 (0)
Smith-Magenis
12 (0)
Wolf
10 (1)
1p36
19 (1)
Angelman
15 (1)
Kallman
8 (1)
Cri du Chat
5 (1)
Steriod sul.
3 (2)
2q
10 (0)
Total
547 (23)
The FISH analyses in oncology is more diverse and multiple tests may be performed on the same
patient both at initial diagnosis and through the course of their disease. BCR/ABL remained the
most widely employed probe (112 tests) due to the need to test in both chronic myeloid leukaemia
(CML) and acute leukaemias. The X/Y probe was the next most frequent (61 tests) and it is expected
that the use of this probe will continue to increase as more stem cell transplantations occur and the
frequent need for continuous follow up in these patient.
Quality Issues
The laboratory participated in the UKNEQAS EQA
scheme with full compliance and satisfactory
performance in all areas of prenatal, postnatal and
oncology assessment.
Sample Projection for 2007
It is projected there will be 7,000 samples in 2007;
this is based on previous increases and early 2007
figures.
This number is likely to include an
estimated 4,000 blood samples and 2,500 haematological samples.
Page 7
Molecular Genetics
Molecular Genetics uses DNA testing to answer clinical questions about the diagnosis of inherited
disorders, or the carrier status of family members. At the NCMG, we have assembled a highlyskilled team of Clinical Scientists each of whom takes on responsibility for the testing of one or more
inherited disorders.
The Clinical Scientists are supported by Genetic Technologists, Medical
Laboratory Assistants and Administrators, all working within a well-developed quality system.
Scientists from the Molecular Genetics Division are active in quality assurance networks in the UK
and Europe, to ensure that genetic testing laboratories throughout Europe and the UK meet the
highest quality standards.
In 2006, the Molecular Genetics division of the NCMG offered molecular testing for eleven genetic
conditions: cystic fibrosis, Duchenne muscular dystrophy, Huntington chorea, spinal muscular
atrophy, fragile X syndrome, haemochromatosis, Angelman syndrome, Prader-Willi syndrome,
Friedreich ataxia, uniparental disomy and torsion dystonia (DYT1).
Requests for molecular analysis have increased exponentially since our inception. Sample numbers
have more than doubled since 2000. This increased demand for Molecular Genetics (DNA) testing
continued in 2006 with annual sample numbers up 11%. All of the most commonly-requested tests
increased significantly, hereditary haemochromatosis leading the field with an increase of 25%.
In addition, we extract DNA and act as a send-out service for genetic testing to other laboratories
worldwide. We exported 1,503 DNA samples for molecular testing in 2006 to over 50 laboratories
worldwide – an increase of 50% on the number sent abroad in 2005. Samples were sent abroad for
testing for over 175 different inherited disorders.
As of December 2006, staff comprised of a Head of Department (Dr David Barton), one Principal
Scientist (Dr Shirley McQuaid), 2.5 Senior Clinical Scientists, 7.3 Basic Grade Clinical Scientists, 8
Genetic Technologists and 3 Medical Laboratory Assistants. The staff expansion started in late 2005
was completed in 2006 – excellent news for the Division, but bringing with it a huge training
workload. Trainers and trainees alike are to be congratulated on a great year’s work. New staff will
enable the Division to cope with ever-increasing test numbers, bring in new technologies and expand
the test repertoire of the Laboratory.
________________________________
Dr David E Barton
Chief Molecular Genetics Scientist
Page 8
Annual Report 2006
Molecular Genetics Activity
Total Sample Numbers:
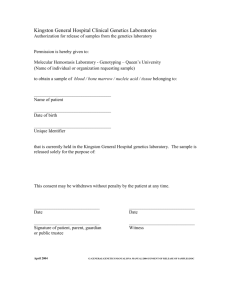
Requests for molecular analysis have increased exponentially since the centre’s inception. Sample
numbers have more than doubled since 2000. This increased demand for Molecular Genetics (DNA)
testing continued in 2006 with annual sample numbers up 11%. All of the most commonly-requested
tests increased significantly, hereditary haemochromatosis leading the field with an increase of 25%.
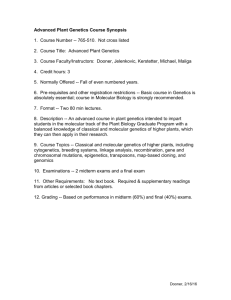
Trends and responses
The dramatic increase in sample numbers observed between 2001 and 2006 is illustrated below:
Molecular Genetics
6000
Samples Received
5000
4000
3000
2000
1000
0
2000
2001
2002
2003
Year
Molecular Genetics Sample Increases 2000-2006
In addition, the Molecular division extracted DNA and
acted as a send-out service for genetic testing to other
laboratories worldwide. The division exported 1,501 DNA
samples for molecular testing in 2006 to over 50
laboratories worldwide – an increase of 50% on the
number sent abroad in 2005. Samples were sent abroad
for testing for over 175 different inherited disorders.
Page 9
2004
2005
2006
The breakdown of samples received, extracted, sent out, and analysed in-house, in 2006, is shown in
the following table :
Received
Extracted
Sent Out
Analysed in house
5,869
5,144
1,501
3,607
Reports Issued:
The Molecular Genetics Division achieved a 10% increase in reports issued in 2006 over 2005, despite
the huge training programme undertaken during the year. These figures are outlined in the table
below:
Disease Name
2005
2006
Angelman Syndrome
Becker Muscular Dystrophy
Breast Cancer
Cystic fibrosis
27
1
23
520
31
2
27
646
Duchenne Muscular Dystrophy
17
28
Dystonia, Autosomal Dominant Torsion
Fragile X syndrome
Friedreich Ataxia
Hereditary Haemochromatosis
Huntington disease
Prader-Willi Syndrome
Russell-Silver Syndrome
13
699
52
747
54
118
1
6
561
19
1,021
47
93
8
Spinal Muscular Atrophy
20
22
Uniparental Disomy
6
10
2,298
2,521
TOTAL
The table below shows the Molecular Genetics Top in-house tests 2006:
Disease Name
Page 10
2005
2006
Hereditary Haemochromatosis
Cystic fibrosis
Fragile X syndrome
Breast Cancer
897
659
683
441
1,126
754
615
494
Hereditary non-Polyposis Colon Cancer
Prader-Willi Syndrome
Friedreich Ataxia
Duchenne Muscular Dystrophy
Familial Adenomatous Polyposis Coli
Huntington disease
Angelman Syndrome
Spinal Muscular Atrophy
Uniparental Disomy
169
127
58
58
38
60
44
36
15
150
110
70
60
51
51
45
37
18
Annual Report 2006
SERVICE DOWNGRADED AS SAMPLES ARE SENT
ABROAD FOR TESTING
The Molecular Division had to drop tests for several genetic disorders from the in-house service
repertoire in 2001 and 2002 due to lack of resources
necessary to maintain these, and this situation has
continued into 2006.
More than a third of the testing
repertoire has now been dropped. These samples are now
being sent to UK laboratories, leading to a loss of hard-won
expertise from the Laboratory and making the NCMG very
much less of a National Centre. It is certain that these tests
could be performed more cheaply in-house, if the money
was used to hire staff instead of paying for testing abroad.
In the past the NCMG used to offer testing for myotonic dystrophy, Familial polyposis coli, X
inactivation, zygosity testing, UPD for chromosome 11 (one cause of Beckwith–Wiedemann
syndrome), hereditary motor and sensory neuropathy, spino-cerebellar ataxias, dentatorubralpallidoluysian atrophy (DRPLA), spinal bulbar muscular atrophy and breast-ovarian cancer (on a
research basis).
Page 11
Clinical/Laboratory Liaison Meetings
Clinical/Laboratory liaison meetings were initiated in 2005 and have proved extremely successful.
The aim of these meetings is to facilitate the formal presentation and discussion of ongoing audits, or
research & developmental projects, within all divisions of the NCMG.
These meetings are
enthusiastically received by all staff members as they give a forum for discussion across the different
disciplines.
The structure involves one member of each of the sections presenting an interesting
topic for 15 minutes.
NCMG have tried to have a common theme at most meetings. These
presentations have stimulated interesting debate and also encouraged staff to start similar projects
within their own division. The titles of the talks given at these meetings in 2006 are listed below:
January 2006
Dr Caitriona King: Report back on NOWGEN Communication Workshop for Geneticists
Dr Rod Howell: Ataxia Telangectasia
Dr Sally Ann Lynch: Ataxia Telangectasia
May 2006
Johanna Kelly: Haematological cytogenetics at NCMG
Dr Solvig Roring: HNPCC diagnostic testing
October 2006
Dr David Barton: The testing of children for adult onset genetic disorders
Cliona deBaroid: HNPCC, a Clinical Perspective
Prof. Andrew Green: The use of free fetal DNA in maternal blood: non-invasive prenatal diagnosis
December 2006
Adam Dunlop: Cytogenetic Prenatals – Audit
Emma Ryan & Bronagh Oh’Ici: MLPA as a molecular genetic diagnostic tool
Dr Raveen Shahdadpuri: Sickle Cell Disease – Clinical perspective
Page 12
Annual Report 2006
Research
The National Centre for Medical Genetics undertakes and participates in a wide variety of Irish and
international Genetic Research projects of significant medical importance for the diagnosis and
treatment of patients. The main research projects in 2006, which the NCMG undertook, or had a
high priority role, are outlined in the following section.
Amyotrophic Lateral Sclerosis
The NCMG has had a long standing collaboration with Dr Orla Hardiman, Department of
Neurology, Beaumont Hospital, Dublin, into the genetics of Amyotrophic Lateral Sclerosis. A PhD
student, Dr Matt Greenway, is funded from 2005-2007 by the Health Research Board to work jointly
between the Royal College of Surgeons in Ireland, and the NCMG. Dr Greenway, with Dr Sean
Ennis and Prof. Andrew Green from the NCMG published a landmark paper in Nature Genetics in
2006, describing mutations in a previously unidentified gene, ANG in patients with Amyotrophic
Lateral Sclerosis. Much of this work was done in the NCMG laboratory.
Autism
Over the last few years, the NCMG has developed a collaboration with Prof. Michael Gill and Dr
Louise Gallagher of the Department of Psychiatry, Trinity College, Dublin. Dr. Sean Ennis and Prof.
Andrew Green have been mapping a region of chromosome 2q implicated in the genesis of autism,
based on a de novo chromosome rearrangement of 2q in a patient with autism. Such mapping
studies will refine the large area of chromosome 2q implicated in autism in independent whole
genome association studies.
This successful Irish Autism Collaboration has now become part of the international Autism
Genome Project, with 14 other centres all focussing on research into the genetics of autism.
Page 13
Vesicoureteral Reflux
Vesicoureteral Reflux (VUR), the retrograde flow of urine from the bladder into the ureter and
kidney, is a common disorder, found in 1-2% of children. This reverse flow of urine can cause
kidney damage (reflux nephropathy) by itself, and the risk of damage is increased by the urinary
tract infections to which affected children are susceptible. VUR is the most common cause of endstage renal failure and of severe hypertension in children. The anatomical basis of the disorder is a
shortening of the segment of the ureter which runs through the submucosal layer of the bladder
wall.
Reflux can be corrected by an endoscopic procedure involving injecting Teflon paste beneath the
truncated ureter in the bladder wall (STING procedure), invented in the Children’s Research Centre
in 1984.
Siblings of children with VUR are at a greatly increased risk of being affected themselves, indicating
that a genetic susceptibility factor (or factors) is involved.
Professor Prem Puri at OLCHC has assembled a collection of over 250 pairs of siblings affected with
VUR and their parents. NCMG are using this resource to investigate the genetics of VUR. In 2006,
the NCMG published an analysis of the clinical features of the disease in Irish families, which
showed that the risk and severity of VUR in siblings depends on the sex of the affected child.
Brothers of index male patients have higher grade of reflux and higher rate of associated duplex
systems.
This has implications for genetic counselling and for modelling the inheritance of
vesicoureteral reflux.
In order to search for genetic loci involved in VUR, the NCMG performed a genome-wide linkage
scan using 4710 single-nucleotide polymorphisms (SNPs) in 609 individuals from 129 Irish families
with more than one affected member. Nonparametric linkage (NPL) analysis of the dataset yielded
moderately suggestive linkage at chromosome 2q37 (NPLmax = 2.67, p = 0.0001). Analysis of a
subset without any additional features, such as duplex kidneys, yielded a maximum NPL score of
4.1 (p < 0.00001), reaching levels of genome-wide statistical significance. Suggestive linkage was also
seen at 10q26 and 6q27, and there were several smaller peaks. These results have been submitted for
publication. Senior Postdoctoral Researcher Dr John Darlow is currently studying the candidate
genes under there linkage peaks to determine which are most likely to be involved in causing VUR.
This work is funded by the Children’s Medical & Research Foundation.
Page 14
Annual Report 2006
SNiP2CHIP
The requirement to screen for known SNPs (Single Nucleotide Polymorphisms) has become one of
the key challenges to be addressed to enable the exploitation of the human genome sequence, where
approximately 3 million SNPs are responsible for much of the variation within the human
population. Several methods and technologies are currently available for detection of SNPs, but no
single platform exists which can deliver 100% accuracy, in a low cost, versatile, and easy-to-use
integrated system.
The SNiP2CHIP project, coordinated by Dr Paul Galvin, at the Tyndall National Institute in Cork,
builds on the successful CF-CHIP project to work towards the development of integrated SNP
detection platforms to include modules for DNA extraction and purification from biological samples,
DNA amplification, DNA characterisation (including SNP detection), signal transduction,
interpretation and data analysis. Integration of the modules on a single platform will include a
transport mechanism based on electrowetting actuation (EWOD).
Two alternative SNP detection platforms will be developed based on optical detection and magnetic
sensing, respectively. The whole system will be packaged as a single automated functional unit with
a simplified GUI interface, based on specifications recommended by potential end-users within the
consortium, including the National Centre for Medical Genetics. The systems development will
focus on delivering a product customised for low to medium throughput, low cost, point-of-care
applications, with emphasis on providing very rapid and accurate results. Within the project, the
systems will be benchmarked for screening of SNPs in the CFTR gene that are associated with Cystic
Fibrosis (CF). CF patient samples will be used to verify the accuracy and reproducibility of the
system in a clinical diagnostics laboratory.
At NCMG, researcher Dr Mark Dobson works to keep the consortium abreast of the latest
genotyping and molecular diagnostics technologies, and is compiling a major review of technologies
for point-of-care genotyping with a view to publication.
SNiP2CHIP is funded by the European Commission’s 6th Framework contract NMP4-CT-2005016833.
Page 15
EuroGentest
EuroGentest is an EU-funded Network of Excellence (NoE) with five Units looking at all aspects of
genetic testing - Quality Management, Information Databases, Public Health, New Technologies and
Education. Through a series of initiatives, EuroGentest encourages the harmonization of standards
and practice in all these areas throughout the EU and beyond.
The NCMG is a full partner in EuroGentest, which funds researcher Dr Christine Brady to work on
the development of new reference materials for genetic testing. Reference materials are an essential
component of any quality assurance system, and the objective of Dr Bardy’s work is to encourage the
development of well-validated reference materials and to help make them available to end users:
genetic testing laboratories, diagnostic kit manufacturers and external quality assessment scheme
organisers. EuroGentest partner Dr David Barton will also explore regulatory issues around genetic
testing in general and reference material development and distribution. These aims are being
realised by a series of major international symposia on reference materials for genetic testing during
the course of the EuroGentest project, as well as smaller meetings of expert groups to focus on
specific areas. Priorities will be set for which reference materials to develop. The specific projects to
meet the high-priority needs are also being supported.
EuroGentest is funded by the European Commission’s 6th Framework, contract no.:FP6-512148
Rare Single Gene Disorders
Dr Sally Ann Lynch, Dr Sean Ennis and Professor Andrew Green were successful recipients of a
grant award totalling over €90,000 from the Children's Medical & Research Foundation in October
2006.
Their grant application aims to investigate the genetic basis of three separate genetic
conditions of Autosomal Recessive Microphthalmia, Autosomal Dominant Ptosis, and Autosomal
Recessive ACTH Resistance.
Page 16
Annual Report 2006
NCMG Multidisciplinary Committees
There are a number of multidisciplinary committees within NCMG.
These were originally
established as a mandatory requirement of the accreditation process, but have also proved hugely
beneficial in their own right.
Management/Accreditation
The remit of this group is to monitor the Centre’s growth and development. The group, which meets
monthly, is made up of senior representatives from all three divisions. The group oversees and
approves the annual Service Plan, and decides on budgetary and staffing priorities. A representative
from the other groups, (Health & Safety, Training and Education, Quality), are invited to contribute
any outstanding issues. Monthly statistics from each division are submitted and discussed.
Health & Safety
The remit of this group is to implement health and safety procedures to ensure that there is a safe
working environment, in accordance with current safety guidelines and legislation. The group meets
monthly and is comprised of staff from all three divisions, across all grades. Health and safety issues
are discussed and procedures for all aspects of safety (e.g. fire, major spillages of dangerous
chemicals or clinical material, reporting and monitoring of accidents and incidents, risk assessments
etc) are developed and implemented.
Page 17
Training & Education
The remit of this group is to facilitate and enhance activities within the NCMG relating to both initial
staff training and ongoing education for existing staff. As Medical Genetics is a dynamic and rapidly
expanding discipline maintaining professional development activity is fundamental to ensuring a
high standard of patient care. The group meets once every 2 months and is comprised of staff from
all three divisions, across all grades.
The group considers issues arising in relation to the travel and training budget, induction & training
programmes for new staff, ongoing staff training procedures, IT training, library & journal access,
Journal Clubs, seminar programmes, research & development, access to scientific meetings, clinical/
laboratory liaison meetings, MRCPath training, continuing professional development, staff appraisal
and relationships with HR. An induction day for all new staff was rolled out in 2006 which provided
an overview of the divisions within the department, introduced new staff to issues relating to health
& safety, training & education and quality. The NCMG also plan to educate users of its service so
that accessing the service can be more effective and efficient.
Quality
The remit of this group is to establish and oversee the implementation of a quality management
system in a way that is sympathetic to attainment of CPA laboratory accreditation. The group
ensures that all procedures and practices comply with international standards and guidelines, and
that substantiating documentation exists. The group has established policies and procedures for
document preparation, review & revision, and control.
Page 18
Annual Report 2006
Administration Team
The administration staff play a vital role in supporting all three division of the NCMG. In 2006 there
were 7½ administrative staff in NCMG – this was divided between the Clinical, Molecular and
Cytogenetics divisions.
Three full time administrators support the Molecular and Cytogenetics divisions of NCMG. Their
role includes booking in samples received, entry of patient details and test requests on to the
laboratory computer systems, distribution of Laboratory reports, communications to referring
clinicians and Consultants, etc.
On the clinical side there are four and half administrators supporting the Clinical division, who are
responsible for supporting the administrative workload of a Genetic Consultants and Genetic
Counsellors. Their role includes entering and maintaining patient details on the Genetics systems,
assisting patients/parents attending the NCMG for outpatient appointments, communicating with
Consultants, General Practitioners and Patients on matters relating to tests, typing and distribution
of medical correspondences to patients, etc.
As the centre continues to expand so will the role and requirement for administrative staff to
support all three divisions.
Page 19
Training
In-house Training Courses run by NCMG:
Molecular Genetics Core Concept / Core disease Programme:
Debby Lambert (Hardy-Weinberg, Bayesian Analysis), Jan 2006;
Dr Caitriona King (Cystic Fibrosis), Mar 2006; Dr Solvig Roring (Haemochromatosis) May 2006; Dr
Shirley McQuaid & Aiveen Carey (Prenatal Analysis) Dec 2006.
Service:
Dr Caitriona King – Dealing with Complaints; August 2006
Dr Caitriona King/Helen O’Shea- Criteria & Procedure for Sample Acceptance; August 2006
Management:
Dr David Barton, Dr Shirley McQuaid, Adam Dunlop, Thomas Morris, Johanna Kelly, Dr Aileen
Butler, Aiveen Carey, Dr Trudi McDevitt, Dr Caitriona King, Anne-Marie Hegarty, Zephra
Adamson, Geri McGettrick, Rose Kelly - Irish Times Leadership Skills Course, December 2006
External Courses Attended:
Dr Aileen Butler, NOWGEN Communication Workshop for Geneticists, March 2006
John Darlow: Dublin Molecular Medicine Centre Course ‘Population Genetics and SNP Analysis’,
Institute of Molecular Medicine, Trinity Centre for Health Sciences, St James’s Hospital, Dublin, 2829 June 2006.
Miriam Russell: Dublin Molecular Medicine Centre, Unravelling Cromatin & the Role of Epigenetics
in Disease, Conway institute, April 2006
Page 20
Annual Report 2006
NCMG Publications
1.
Caitriona King and David E Barton (2006) Best practice guidelines for the molecular genetic
diagnosis of Type 1 (HFE-related) hereditary haemochromatosis. BMC Medical Genetics 2006,
7:81
2.
C. Ferec, T. Casals, N. Chuzhanova, M.Macek, T. Bienvenu, A. Holubova, C.King, T. McDevitt
et al. (2006) Gross genomic rearrangements involving deletions in the CFTR gene:
characterization of six new events from a large cohort of hitherto unidentified cystic fibrosis
chromosomes and meta analysis of the underlying mechanisms. Eur J Hum Genet 14(5): 567-576.
3.
Crawford J, Lower KM, Hennekam RC, Van Esch H, Megarbane A, Lynch SA, Turner G, Gecz J.
Mutation screening in Borjeson-Forssman-Lehmann Syndrome (BFLS): Identification of a novel,
de novo PHF6 mutation in a female patient. J Med Genet. 2006 Mar 43(3) 238-243.
4.
Murphy AM, Brenner C & Lynch SA. . Agenesis of the corpus callosum with interhemispheric
cyst, hepatic haemangioma and Trisomy 21. Clinical Dysmorphology 149-151 2006
5.
Murphy AM, Drumm B, Brenner C & Lynch SA. Diencephalic syndrome Russell’s syndrome.
Clin Dysmoph 15 (4) 253-254 2006
6.
Finn S & Lynch SA. Malpuech syndrome: facial features in the absence of clefting. Clin
Dysmorph 15 (4) 243-244 2006
7.
Crow YJ, Hayward BE, Parmar R, Robins P, Leitch A, Ali M, Black DN, van Bokhoven H,
Brunner HG, Hamel BC, Corry PC, Cowan FM, Frints SG, Klepper J, Livingston JH, Lynch SA,
et al. Mutations in the gene encoding the 3'-5' DNA exonuclease TREX1 cause Aicardi-Goutieres
syndrome at the AGS1 locus. Nat Genet. 2006 Jul 16;
8.
Kyndt F, Gueffet J-P, Probst V, Jaafer P, Legendre A, Le Bouffant F, Toquet C, Roy E, McGregor
L, Lynch SA, Newbury-Ecob R, Tran V, Young I, Trochu J-N, Le Marec H & Schott J-J.
Mutations in the gene encoding Filamin A as a cause for familial cardiac valvular dystrophy.
Circulation 2006 Epub 2006 Dec 26
9.
Simon C. Ramsden, Zandra Deans, David O. Robinson, Roger Mountford, Erik A. Sistermans,
Wayne W. Grody, Shirley McQuaid, Simon J. Patton, Susan A.R. Stenhouse. Monitoring
Standards for Molecular Genetic Testing in the United Kingdom, The Netherlands, and Ireland.
Genetic Testing Sep 2006, Vol. 10, No. 3: 147-156.
10. Green A & Lynch SA. Health of the world’s Roma population. Lancet 368:no.9535 575 2006
(letter).
11. F. Ni Ainle, P.J Hayden, P. Crosby, K. Murphy, D. McCarthy, J. Kelly, & M.J Neat. Concurrent
rearrangement of BCL1 and BCL6 with a single immunoglobulin locus in a case of diffuse large
B-cell lymphoma. Leukemia & Lymphoma, Volume 47, Issue 12, December 2006; Pages 26552656
Page 21
12. Pirker ME, Mohanan N, Colhoun E, Barton D, Green A, Puri P. Familial vesicoureteral reflux:
influence of sex on prevalence and expression. Journal of Urology 176(4 Pt 2):1776-80, 2006
13. ANG mutations segregate with familial and 'sporadic' amyotrophic lateral sclerosis Matthew J
Greenway, Peter M Andersen, Carsten Russ, Sean Ennis, Susan Cashman, Colette Donaghy,
Victor Patterson, Robert Swingler, Dairin Kieran, Jochen Prehn, Karen E Morrison, Andrew
Green, K Ravi Acharya, Robert H Brown Jr & Orla Hardiman Nature Genetics 2006
Apr;38(4):411-3
14. Medullary carcinoma of the pancreas in a man with hereditary non polyposis colon cancer due
to a mutation of the MSH2 mismatch repair gene. Niamh Banville, Robert Geraghty, Edward
Fox, Dermot T Leahy, Andrew Green, Denise Keegan, Justin Geoghegan, Diarmuid
O’Donoghue, John Hyland, Kieran Sheehan. Human Pathology 2006 37 1498-1502
15. Yeung J, Kempski H, Neat M, Bailey S, Smith O, Brady HJ. Characterization of the t(17;19)
translocation by gene-specific fluorescent in situ hybridization-based cytogenetics and detection
of the E2A-HLF fusion transcript and protein in patients' cells. Haematologica. 2006;91(3):422-4.
Audits
1.
Debby Lambert/Caitriona King: An Audit of Genotypes and Borderline Sweat Tests in Cystic
Fibrosis.
2.
Cliona de Baroid/Claire Gibbons: Duchenne Muscular Dystrophy.
3.
Niamh ni Shuibne, Andrew Green, Sally Ann Lynch: Trisomy 13/18 cases in Ireland over a ten
year period.
4.
R Shahdadpuri, Sally Ann Lynch: Audit of referrals with developmental delay to a genetics
clinic.
5.
Nuala Cody: Cascade screening in BRCA1/2 families in the Republic of Ireland.
Page 22
Annual Report 2006
Meetings Attended
1.
Dr David Barton: OECD Expert Group on Genetic Testing, Berlin January 2006
2.
Prof. Andrew Green: EU FP6 Public Health Genomics Unit, Bielefeld, Germany, Jan 2006
3.
Dr Trudi McDevitt, Dr Catriona King: 6th National Cystic Fibrosis Conference, Killarney,
February 2006
4.
Dr David Barton: EU Policy Forum on Genetic Testing, European Commission, Brussels,
February, 2006
5.
Dr. Trudi McDevitt: Irish Association of Cancer Research, Galway, March 2006
6.
Dr Caitriona King, Irish Paediatric Association meeting, May 26th 2006 Ardilaun Hotel, Galway.
7.
Prof. Andrew Green, Dr. Sally Ann Lynch, Irish Perinatal Society, Dublin, May 2006
8.
Dr David Barton, Dr Shirley McQuaid, Dr Aileen Butler: Clinical Molecular Genetics Society,
Glasgow, April, 2006
9.
Dr David Barton, Dr Christine Brady: European Society of Human Genetics, Amsterdam, May,
2006
10. Dr Bronagh O’hIci & Miriam Russell: New and Developing Technologies in Genetic
Diagnostics, Salisbury, July 2006
11. NCMG Staff: Irish Society of Human Genetics, Dublin, September 2006
12. Dr Willie Reardon, Dr S-A Lynch, Dr David Barton, Prof. Andrew Green, Dr Michael Sweeney,
Dr Trudi McDevitt, Dr John Darlow: British Society for Human Genetics, York, September, 2006
13. Dr John Darlow, Dublin Molecular Medicine Centre Science Day, October 2006
14. Dr David Barton, Dr Sean Ennis: American Society of Human Genetics, New Orleans, October,
2006
15. Dr David Barton: Association for Molecular Pathology, Orlando, November 2006
16. Dr David Barton: OECD Expert Group on Genetic Testing, Paris, November 2006
17. Dr David Barton: CDC Meeting on Reference Materials for Genetic Testing, November 2006
18. Dr David Barton, Dr. John Darlow: Symposium on Vesicoureteric Reflux and the Genetics of
Renal Development, UCL Institute of Child Health, London, December 2006
19. Adam Dunlop, Christine Brady: Eurogentest Workshop on Internal Audit, June 2006
20. Adam Dunlop, Thomas Morris: The Wales Genepark Workshop “Microarrays in Diagnosis”,
November 2006
21. Adam Dunlop: International Academy of Computer Training, Access Level 1, November 2006
22. Johanna Kelly: European Haematology Association, Annual meeting, June 2006
23. SA Lynch. Dysmorphology club Institute of Child Health London 8th March, 7th June & 6th Dec.
24. SA Lynch Clinical Genetics Society Spring meeting 23rd/24th March 2006 Glasgow SA Lynch
Birth Defects meeting Manchester Nov 21-24th 2006.
25. Miriam Russell: Institute of Molecular Medicine Annual Meeting, St James Hospital, November
2006.
Page 23
Presentations
Caitriona King; Genotypes & Borderline Sweat Tests: The NCMG Experience, Clinical Pathology
Conference, Our Lady’s Children’s Hospital, Crumlin, Jan 2006
N Cody, M Adams, C deBaroid, A Green & SA Lynch. Cascade screening in BRCA1/2 families in
Ireland. Association of Genetic Nurse Counsellors annual meeting, Guys Hospital, London May
11th2006
A Green, Clinical Genetics and Perinatal Medicine. Invited Lecture, Irish Perinatal Society May 2006
N ni Shuibne, A Green & SA Lynch. Audit of trisomy 13 & 18 cases over a ten year period in Ireland.
Irish perinatal society meeting, May 12th 2006, Rotunda Hospital & Temple Street Grand Rounds
May ’06.
Anne Marie Murphy, K Dunne, O Flanagan & SA Lynch. High prevalence of Cohen syndrome
amongst Irish Travellers. Irish Paediatric Meeting, 26th May 2006 Ardilaun Hotel Galway
Caitriona King; T McDevitt, D Lambert, D Barton & SA Lynch. An audit of Genotypes & Borderline
Sweat Tests in CF. Irish Paediatric Association meeting, May 26th 2006 Ardilaun Hotel, Galway.
David Barton: “Newborn screening for cystic fibrosis” Joint US-Ireland Workshop: Inflammation
and Infection in Cystic Fibrosis and Therapeutic Implications, 23 June, 2006, RCSI, Dublin
Caitriona King,T. McDevitt, M. Rogers, B. O’hIci , S. McQuaid, C. Le Maréchal, C. Férec, D. E.
Barton Update on the complex CF mutation spectrum in the Republic of Ireland (OLHSC), Irish
Society of Human Genetics, TCD Sept 2006
David Barton. Quality Control Initiatives in Europe. Association for Molecular Pathology, Orlando,
November 2006
David Barton. European developments in Reference Material production. CDC Meeting on
Reference Materials for Genetic Testing, November 2006
Michael Sweeney, E Donohue, D Barton et al Fragile X in Ireland Temple Street and Our Lady’s
Children’s Hospital Grand rounds Nov & Dec 2006.
David Barton, Prem Puri. Vesicoureteric reflux in Ireland: from the clinic to the genes. Symposium
on Vesicoureteric Reflux and the Genetics of Renal Development, UCL Institute of Child Health,
London, December 2006
Raveen Shahdadpuri Audit of referrals with developmental delay to a genetics clinic. Grand rounds,
Our Lady’s Children’s Hospital December 2006
Page 24
Annual Report 2006
Poster Presentations
C. King, T.McDevitt, D.Lambert, David Barton, S.A. Lynch, Genotypes & Borderline Sweat Tests:
The NCMG Experience; National CF Conference, Killarney, February, 2006. Awarded First Prize.
C. King, T. McDevitt, T. Yeomans, D. Barton, A Luminex-based Cystic Fibrosis Assay, National CF
Conference, Killarney, February, 2006.
T. McDevitt, C. King, B. O’hIci, S. McQuaid, C. Le Maréchal, C. Férec, D. E. Barton. Increasing
complexity of the CF mutation spectrum in the Republic of Ireland, National CF Conference,
Killarney, February, 2006.
Anne Marie Murphy, K Dunne, O Flanagan & SA Lynch. High prevalence of Cohen syndrome
amongst Irish Travellers. Eur Society of Human Genetics Meeting, Amsterdam, May 6-9th 2006
Anne Marie Murphy, C Brenner & SA Lynch. Agenesis of the corpus callosum with interhemispheric
cyst, hepatic haemangioma and Trisomy 21. Irish Paediatric Association, May 26/27th 2006 Ardilaun
Hotel, Galway.
Susan Finn, M Colreavy, Sally Ann Lynch Does Noggin cause twinning? Irish Society of Human
Genetics 9th Scientific meeting 7/9/2006.
M Sweeney and DE Barton. Detection and Accurate Sizing of Expanded Fragile X alleles using a
Multiplex Fluorescent PCR Assay. British Society for Human Genetics, York, September, 2006
C.King, T. McDevitt, M. Rogers, D. Lambert, D. Barton, S. A. Lynch. An Audit of Genotypes and
Borderline Sweat Tests in Irish CF Patients. Irish Society of Human Genetics 9th Scientific meeting
September 2006 and British Society of Human Genetics, York, September 2006
T. McDevitt, C. King, D. E. Barton. Validation of a Luminex-Based Multiplex Assay for 25 Cystic
Fibrosis Mutations. Irish Society of Human Genetics 9th Scientific meeting September 2006 and
British Society of Human Genetics, York, September 2006
Helena Kelly, Akihiro Yoneda, John M Darlow, Denis Shields, Cliona Molony, Andrew J Green, Prem
Puri, David E Barton. A Genome Scan for Genes Involved in Vesicoureteral Reflux. Irish Society of
Human Genetics 9th Scientific meeting September 2006, British Society of Human Genetics, York,
September 2006 and American Society for Human Genetics, New Orleans, October 2006
Sally Ann Lynch, M Colreavy. Does Noggin cause twinning? Birth Defects meeting, Manchester
Nov 2006
Sally Ann Lynch, Elizabeth Vandenburghe, Eibhlin Conneally, Johanna Kelly. An audit of MDS
cases submitted for cytogenetic analysis over a two year period. Cork, Nov 2006
Page 25
External Quality Assessment
Scheme—Assessors & Organisers
Dr David Barton
Scheme Organiser for European Molecular Quality Network Hereditary Friedreich Ataxia scheme
Management Group member, European Molecular Genetics Quality Network
Dr Shirley McQuaid
Scheme Organiser UK NEQAS Spinal Muscular Atrophy
Assessor for European Molecular Quality Network HNPCC scheme
Dr Caitriona King
Assessor for European Molecular Quality Network Hereditary Haemochromatosis scheme
Prof. Andrew Green
Member UK NEQAS Molecular Genetics Steering Committee
Page 26
Annual Report 2006
Teaching
Dr David Barton
UCD Pathology module for Medical Students, Genetics Tutorial
UCD Pathology module for Medical Students, Lecture on Molecular Genetics Diagnostic Tests
TCD MSc in Clinical Chemistry, Lecture on Diagnostic Molecular Genetics
Dr Caitriona King, Dr Trudi McDevitt, Dr Shirley McQuaid, Dr Alana Ward
UCD Pathology module for Medical Students, Genetics Tutorials
Prof. Andrew Green, Dr. Sean Ennis
UCD Foundation Year Module – Medical Genetics April 2006 and Oct/Nov 2006
Prof. Andrew Green
Medical Undergraduate genetic lectures for UCD, RCSI and TCD
Specialist Registrar neurology teaching, Tallaght Hospital May 2006
Administrative Research Activities
Dr David Barton
Leader of the work on Reference Materials in the EuroGentest European Network of
Excellence in Genetic Testing
Partner, European SNiP2CHIP project
Page 27
NCMG Staff Photo
Page 28
Annual Report 2006
The National Centre for Medical Genetics
Our Lady’s Children’s Hospital
Crumlin
Dublin 12
Phone: +353-1-4096739
Fax: +353-1-4560953
www.genetics.ie