Glucose and lipid metabolism in human skeletal muscle
advertisement

University of Helsinki
Faculty of Medicine
Department of Medicine
Division of Cardiology
Minerva Foundation Institute
for Medical Research
Helsinki, Finland
Glucose and lipid metabolism in human
skeletal muscle
Paulina Skrobuk
ACADEMIC DISSERTATION
To be presented, with the permission of the Faculty of Medicine, University of
Helsinki, for public examination in the Auditorium 2 of Biomedicum Helsinki
on Friday September 7th 2012, at 12 noon.
Helsinki 2012
SUPERVISED BY
Adjunct Professor Heikki Koistinen, M.D., Ph.D.
Minerva Foundation Institute for Medical Research
Department of Medicine, Division of Cardiology
Helsinki University Central Hospital
Helsinki, Finland
REVIEWED BY
Professor Jussi Pihlajamäki, M.D., Ph.D.
Department of Clinical Nutrition
University of Eastern Finland
Kuopio, Finland
Adjunct Professor Antti Virkamäki, M.D., Ph.D.
Helsinki University
Helsinki, Finland
OPPONENT
Associate Professor Michael Gaster M.D., Ph.D., D.MSc
Laboratory of Molecular Physiology
Department of Pathology
Odense University Hospital
Odense, Denmark
ISBN 978-952-10-8233-7 (paperback)
ISBN 978-952-10-8234-4 (PDF, ethesis.helsinki.fi)
Helsinki University Printing House
Helsinki 2012
“I am among those who think that science has great beauty. A
scientist in his laboratory is not only a technician: he is also a child
placed before natural phenomena which impress him like a fairy tale.”
Maria Sklodowska-Curie
Abstract
Insulin resistance is characterized by a blunted biological response to insulin, and it is the
hallmark of obesity and type 2 diabetes. Since skeletal muscle is among the major
metabolic organs in the body, a better understanding of the molecular pathways regulating
metabolic responses in muscle will help to develop novel strategies to improve glucose
and lipid metabolism. Here, two different models of human skeletal muscle, intact skeletal
muscle strips and primary human myotubes, were used to study acute regulation of
metabolism. Globular adiponectin modestly increased glucose transport in type 2 diabetic,
but not in nondiabetic muscle strips, without any effects on proximal insulin signaling.
Insulin sensitizing drug rosiglitazone did not affect glucose transport or proximal insulin
signaling events in intact human muscle strips, but it transiently activated AMPKsignaling pathway. Polyphenolic compound resveratrol inhibited fatty acid oxidation,
glucose metabolism and insulin signaling in human myotubes. Moreover, resveratrol
increased ER stress and directly inhibited AMPK activity. Palmitate impaired glucose
metabolism and increased ER stress in primary human myotubes and also in intact skeletal
muscle strips from overweight, but not lean men. Thus, the role of ER stress in the
pathogenesis of fatty acid induced insulin resistance and T2D warrants further studies.
Acknowledgements
This study was carried during 2007-2012 in the Minerva Foundation Institute for Medical
Research and Department of Medicine, Division of Cardiology Helsinki University
Central Hospital.
I wish to express my gratitude to all the people who have helped and supported me during
this study and especially I wish to thank you:
My supervisor, Heikki Koistinen for personal guidance, giving me the “free hand” and
explaining to me what science means. Despite your busy schedule you always managed to
be available when I needed your help by phone or e-mail. It was a pleasure to work with
you.
The head of the Minerva Institute Docent Vesa Olkonen as well as the previous head
Professor Dan Lindholm for the excellent research environment.
Professor Juleen Zierath for the collaboration and giving me the opportunity to visit and
work with her excellent team at Karolinska Institute. I also would like to thank Dr. Lubna
Al-Khalili from Karolinska Institute for answering my numerous questions regarding
muscle primary cells.
Professor Sirkka-Liisa Karonen and Dr. Tuula Huitti for helping to solve all the problems
concerning radiochemistry.
Professor Jussi Pihlajamäki and Adjunct Professor Antti Virkamäki for their constructive
criticism and advises during the review of this thesis.
In addition, I would like to thank Ritta Päivärinta and Eeva Jääskeläinen for the help in the
laboratory and being my friends. Moreover, Eeva and Noora for an unforgettable trip and
the time we shared outside the lab. Carita Kortman and Cia Olsson for the administration
help. The special thanks go to all my collaborators Maria Semenova, Anna Zitting, Heidi
Kuoppamaa Maarit Makkonen, Dr. Anne Hiukka, Professor Alexander Chambelin and
Stephanie von Kraemer. Steffi you were the best gradu student and it was a pleasure to
work with you. I wish to warmly thank you all my friends and colleagues in Minerva
Institute. You all created a pleasant atmosphere and it was fun to work next to you.
I would like to thank all my friends in Helsinki. Without you I would have never survived
in cold Finland. Anna thank you for the friendship and all your support. Annika for being
my “sister in science”, for all you advices and sharing football games with me. Marion and
Veronica for all the support and lunch disscussions. Special thanks go to Marion for the
help with articles and prepositions. I own my warm thanks to my friends in Tampere,
Gosia, Anna and Lukasz. I will never forget the moments we had in Finland. I am grateful
to Gosia for all the encouragement, support and “talks on the balcony”(you know what I
mean). I warmly would like to thank my great Finnish friends Janica and Jarkko. I would
have never stayed in Finland without your help and support. I could always count on you
guys and I will never forget that. The special thanks go to my best friend Kinga. You were
always on my side. Thank you for all the Skype talks during the last 5 years,
encouragement, warm welcome at home and everlasting friendship.
I am very grateful to all the volunteers that participated in this study.
This thesis was finically supported by the Finnish Academy of Science, the Finnish
Cultural Foundation, the Finnish Diabetes Research Foundation, the Finnish Foundation
for Cardiovascular Research, the Finnish Medical Foundation, the Liv och Hälsa
Foundation, the Novo Nordisk Foundation, the Sigrid Juselius Foundation, the Finska
Läkaresällskapet, the University of Helsinki and Paulo Foundation, all of which I
gratefully acknowledge.
All above, I would like to thank to my family, especially my parents for all the support,
love and care I got during my PhD studies and simply for beliving in me. I would not be
where I am now without you: ”Dziekuje Kochani. Kocham Was”. My deepest gratefulness
goes to my brother for sharing the passion to speedway, for all the travels we made
together and for always being there when I needed help. Finally, the special thanks to
Nicolas for joining me on bord of my plane.
Helsinki, August 2012
Paulina Skrobuk
Table of Contents
Abstract.......................................................................................................................... 3
Acknowledgements ....................................................................................................... 5
List of original publications ......................................................................................... 9
Abbreviations .............................................................................................................. 10
1 Introduction.............................................................................................................. 13
2 Review of the literature ........................................................................................... 15
2.1 Insulin signaling in skeletal muscle ..............................................................................15
2.1.1 Insulin receptor .........................................................................................................15
2.1.1 The PI 3-kinase pathway ..........................................................................................16
2.1.2 MAPK pathways ......................................................................................................19
2.1.3 CAP/Cbl/TC10 pathway...........................................................................................19
2.1.4 Defects in insulin signaling and metabolism in human skeletal muscle ..................20
2.2 AMP –activated protein kinase pathway.....................................................................24
2.2.1 The structure and regulation of AMPK ....................................................................24
2.2.2 Downstream targets of AMPK in skeletal muscle ...................................................25
2.2.3 AMPK activators ......................................................................................................28
2.3 Fatty acid-induced insulin resistance in skeletal muscle ............................................31
2.3.1 Intramuscular lipid metabolites ................................................................................32
2.3.2 Mitochondrial β-oxidation of fatty acids..................................................................34
2.3.3 Inflammation ............................................................................................................37
2.3.4 Endoplasmic reticulum stress ...................................................................................40
2.4 Insulin resistance in other tissues .................................................................................44
2.4.1 Liver .........................................................................................................................45
2.4.2 Adipose tissue...........................................................................................................46
2.4.3 The effect of insulin resistance on β-cell failure ......................................................47
3 Aims of the study...................................................................................................... 48
4 Methods..................................................................................................................... 49
4.1 Subjects ...........................................................................................................................49
4.2 Open muscle biopsy (Studies I-III)...............................................................................49
4.3 Human primary muscle cells (study III)......................................................................50
4.4 Immunocytochemistry (study III) ................................................................................50
4.5 L6 cell line (study III) ....................................................................................................50
4.6 Metabolic assays of intact muscle strips ......................................................................51
4.6.1 Glucose transport (studies I,II) .................................................................................51
4.6.2 Glycogen synthesis ...................................................................................................51
4.7 Metabolic assays in cell cultures (study III) ................................................................51
4.7.1 Glucose uptake .........................................................................................................51
7
4.7.2 Glycogen synthesis ...................................................................................................52
4.7.3 Palmitate oxidation ...................................................................................................52
4.8 Western blotting (studies I-III).....................................................................................52
4.8.1 Tissue processing (studies I,II).................................................................................52
4.8.2 Cell lysates (study III) ..............................................................................................53
4.8.3 Immunoprecipitation (study III) ...............................................................................53
4.9 Cell viability (study III) .................................................................................................53
4.10 AMPK activity (study III) ...........................................................................................54
4.11 Muscle ATP and PCr concentrations.........................................................................54
4.12 Statistics ........................................................................................................................54
4.12.1 Statistics used for intact skeletal muscle strips (studies I,II)..................................54
4.12.2 Statistics used in cell culture models (study III) ....................................................54
5 Results and discussion ............................................................................................. 55
5.1 Characteristics of the models used in the study. .........................................................55
5.1.1 Viability of the human muscle strips........................................................................55
5.1.2 Human primary muscle cells (study III)...................................................................55
5.2 The effect of adiponectin on glucose transport in human skeletal muscle (study I)56
5.3 The effect of adiponectin on canonical insulin signaling pathway (study I).............57
5.4 The expression of adiponectin receptors in skeletal muscle from type 2 diabetic and
healthy men (study I) .................................................................................................................58
5.5 The effect of adiponectin on AMPK signaling (study I).............................................59
5.6 The effect of rosiglitazone on insulin action and glucose transport in human
skeletal muscle (study II) ...........................................................................................................59
5.7 The effect of rosiglitazone on the AMPK signaling pathway (study II) ...................61
5.8 The effect of resveratol on glucose and fatty acid metabolism in human skeletal
muscle (study III) ......................................................................................................................61
5.9 The effect of RSV on insulin signaling (study III) ......................................................63
5.10 The inhibitory effect of RSV on AMPK signaling in human myotubes (study III)
......................................................................................................................................................64
5.11 The effect of acute exposure to RSV on ER stress (study III) .................................65
5.12 The effect of palmitate on glucose metabolism and insulin signaling in isolated
human skeletal muscle strips (Unpublished data) ..................................................................65
5.13 Palmitate and ER stress ..............................................................................................70
6 Summary .................................................................................................................. 72
7 Conclusions and future perspectives...................................................................... 73
8 References................................................................................................................. 75
8
List of original publications
This thesis is based on the following publications:
I.
Kuoppamaa H, Skrobuk P, Sihvo M, Hiukka A, Chibalin AV, Zierath JR, Koistinen
HA: Globular adiponectin stimulates glucose transport in type 2 diabetic muscle.
Diabetes/Metabolism Research and Reviews. 2008 Oct;24:554-62.
II.
Skrobuk P, Kuoppamaa H, Hiukka A, Koistinen HA: Acute exposure to rosiglitazone
does not affect glucose transport in intact human skeletal muscle. Metabolism Clinical
and Experimental. 2010 Feb;59(2):224-30.
III.
Skrobuk P, von Kraemer S, Semenova MM, Zitting A, Koistinen HA: Acute exposure
to resveratrol inhibits AMPK activity in human skeletal muscle cells. Diabetologia
2012 in press.
The publications are referred to in the text by their Roman numerals. In addition,
unpublished data are presented.
The original publications are printed here with the permission of the copyright holders.
9
Abbreviations
4-PBA
4-Phenyl butyrate
ACC
Acetyl-CoA carboxylase
AICAR
5-aminoimidazole-4-carboxamide-1-β-D-ribonucleoside
AKT/PKB
Protein kinase B
AMP
Adenosine monophosphate
AMPK
AMP-activated protein kinase
aPKC
Atypical protein kinase C
AS160
AKT substrate 160
ASM
Acid soluble metabolites
ATF4
Activating transcription factor 4
ATF6
Activating transcription factor 6
ATP
Adenosine triphosphate
BiP/GRP78
Glucose related protein 78
CaMKKβ
Calcium/calmodulin dependent protein kinase beta
CAP
Cbl-associated protein
CAT
Carnitine acetyl transferase
CHOP
CCAATT/enhancer binding protein homologous protein
CPT-1
Carnitine palmitoyltransferase 1
CT
Carnitine translocase
DAG
Diacylglycerol
DGKδ
Diacylglycerol kinase δ
DMEM
Dulbecco’s modified Eagle Medium
eIF2α
Eukaryotic translation initiation factor 2 alpha
ER
Endoplasmic reticulum
ERK
Extracellular signal-regulated kinase
ETC
Electron transport chain
FA
Fatty acid
FAD
Flavin adenine dinucleotide
FBS
Fetal bovine serum
10
FFA
Free fatty acids
gAd
Globular adiponectin
GLUT
Glucose transporter
GRB2
Growth factor receptor-bound protein 2
GSK-3
Glycogen synthase kinase-3
GS
Glycogen synthase
HFD
High fat diet
HS
Horse serum
IκBα
Inhibitor of the nuclear factor κB
IKKβ
Inhibitor of the nuclear factor κB kinase-β
IGT
Impaired glucose tolerance
IL-6
Interleukin 6
IR
Insulin receptor
IRE1
Inositol requiring enzyme-1
IRS
Insulin receptor substrate
JNK
c-Jun N-terminal kinase
KHB
Krebs-Henseleit buffer
LKB1
Liver kinase B1
LPS
Lipopolysacharide
MAPK
Mitogen-activated protein kinase
MCP-1
Monocyte chemotactic protein 1
mSOS
Murine son of sevenless
MTT
3-(4,5-Dimethylthiazol-2-yl)-2,5-diphenyl tetrazolium bromide
NAD
Nicotinamide adenine dinucleotide
NF-κB
Nuclear factor kappa-light-chain-enhancer of activated B cells
PCr
Phosphocreatine
PERK
PKR-like endoplasmic reticulum kinase
PGC-1α
PPARγ co-activator 1-alpha
PIP
Phosphatidyinositol phosphate
PI3K
Phosphatidyl inositol 3-kinase
PKC
Protein kinase C
PKD
Protein kinase D
11
PP2A
Protein phophatase 2 A
PPARs
Peroxisome proliferator-activated receptors
ROS
Reactive oxygen species
RSV
Resveratrol
S6K
Ribosomal protein S6 kinase
Shc
Src homology 2 domain containing transforming protein
Sir2
C.elegans homologue of SIRT1
Sirt1
Silent information regulator (sirtuin); NAD-dependent deacetylase
SPT
Serine palmitoyl transferase
SR
Sarcoplasmic reticulum
SREBP-1c
Sterol regulatory element-binding protein-1c
T2D, T2DM
Type 2 diabetes mellitus
TAK1
Mammalian transforming growth factor beta-activated kinase
TCA cycle
Tricarboxylic acid cycle; citric acid cycle; Krebs cycle
TG
Triacylglycerol
TLR
Toll-like receptor
TNF-α
Tumour necrosis factor alpha
TUDCA
Tauroursodeoxycholic acid
TZD
Thiazolidinediones
UPR
Unfolded protein response
XBP-1
X-box binding protein-1
ZMP
5-aminoimidazole-4-carboxamide-1-β-D-ribofuranosyl
5’monophosphate
12
1 Introduction
Type 2 diabetes mellitus (T2DM) accounts for 90 % of diabetes cases around the world. It
is a life-long condition that can lead to severe medical complications, which include
cardiovascular disease, renal failure, blindness, neuropathy, and suspectibility to infections
which together with compromised circulation in lower extremities may lead to gangrene
and leg amputations. Both genetic and environmental factors contribute to the
development of type 2 diabetes. Obesity, sedentary lifestyle, and diet with excessive
saturated fatty acid content are the main nongenetic reasons for type 2 diabetes pandemic.
Insulin resistance is the hallmark of common metabolic diseases such as obesity and type
2 diabetes and is associated with defects in whole body glucose and lipid metabolism.
Thus, it is important to identify the molecular mechanism underlying insulin resistance.
This information will help to prevent the development of type 2 diabetes and to improve
glucose and lipid homeostasis in afflicted patients.
The skeletal muscle is the main tissue responsible for whole body glucose metabolism and
therefore plays an important role in the development of insulin resistance. Increased
intramuscular fat content has been hypothesized to induce insulin resistance via generation
of active fatty acid-derived metabolites, which can interfere with insulin signal
transduction. Moreover, inflammatory state that is present in obesity, and increased
production of proinflammatory cytokines may also negatively affect insulin action in
skeletal muscle. Recently, endoplasmic reticulum stress has been introduced as one of the
central mechanisms leading to insulin resistance.
AMP-activated protein kinase (AMPK) is a cellular energy sensor that acts as a master
regulator of energy balance. Many hormones, such as leptin and adiponectin regulate
metabolism via AMPK. Until recently, TZD:s were commonly used drugs to treat type 2
diabetes. However, their molecular mechanism of action in skeletal muscle is unclear. It
has been hypothesized that they may directly affect AMPK activity. In addition,
polyphenols, such as resveratrol that is present in grapes and red wine, have been proposed
to improve insulin sensitivity via activation of AMPK signaling cascade. Finally, AMPK
is known to stimulate glucose metabolism independent of the insulin signaling pathway.
13
These data highlight AMPK activation as an attractive pharmacological target to treat
insulin resistance.
The aim of this thesis has been to examine the regulation of glucose and fatty acid
metabolism in human skeletal muscle. More specifically, the acute direct effects of the
adipokine adiponectin and the antihyperglycaemic drug rosiglitazone, two insulin
sensitizing compounds, on glucose transport and metabolic signaling pathways have been
examined in intact human skeletal muscle. In addition, the effects of the polyphenolic
compound resveratrol on glucose and lipid metabolism and its potential effect on AMPK
activity have been studied in human skeletal muscle cells.
14
2 Review of the literature
2.1 Insulin signaling in skeletal muscle
Whole body glucose homeostasis is regulated by the hormone insulin, which is secreted
by β-cells in the pancreatic islets of Langerhans in response to a rise in plasma glucose
concentration. Insulin promotes glucose transport and oxidation and regulates protein,
glycogen and triacylglycerol metabolism in target tissues such as skeletal muscle and
adipose tissue. Skeletal muscle is responsible for ~80 % of whole body glucose uptake in
insulin-stimulated conditions and thus it is an important tissue to study the mechanism of
defects in insulin signaling and action (DeFronzo, Jacot et al. 1981; Ferrannini, Simonson
et al. 1988).
2.1.1 Insulin receptor
Insulin signaling events are initiated by binding of insulin to its receptor (IR). This results
in rapid autophoshorylation of the receptor (White and Kahn 1994). The insulin receptor is
a transmembrane heterotetrameric glycoprotein, which belongs to the tyrosine kinase
receptor family. IR consists of two extracellular α-subunits, which possess the ability to
bind insulin, and two intracellular β-subunits that contain the tyrosine kinase domain
(White and Kahn 1994). Insulin binding to its receptor leads to conformational changes in
α-subunits and subsequent activation of the tyrosine kinase in the β-subunit. The IR is
autophosphorylated in at least six residues, where Tyr960 plays the most important role in
the regulation of glucose homeostasis (White and Kahn 1994). Tyr960 is located in the
juxtamembrane region of the insulin receptor. This site is recognized by the insulin
receptor substrate (IRS) proteins (1-6 isoforms) (Cai, Dhe-Paganon et al. 2003), Gab-1
(Holgado-Madruga, Emlet et al. 1996) and Shc (Craparo, O'Neill et al. 1995; Gustafson,
He et al. 1995). These proteins are critical mediators of downstream insulin signaling
events in skeletal muscle. IRS-1 and its homologue IRS-2 are the most important insulin
receptor substrates in the regulation of glucose and lipid homeostasis. IRS molecules
consist of pleckstrin homology domain (PH), which is followed by phosphotyrosinebinding (PTB) domain that is critical for the interaction with the insulin receptor. The
15
carboxy-terminal tail of IRS contains several tyrosine phosphorylation sites that are
responsible for recruiting effector proteins such as the phosphatidyl inositol 3-kinase
(PI3K) and the phosphatase SHP2 (White 2003).
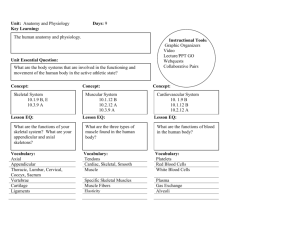
Figure 1. Insulin signaling cascades.
2.1.1 The PI 3-kinase pathway
The phosphatidylinositol 3-kinases (PI3Ks) are involved in the regulation of a wide range
of physiological processes, including insulin-mediated glucose transport in skeletal muscle
in rodents (Lund, Holman et al. 1995) as well as in humans (Shepherd, Nave et al. 1997).
Depending on its sequence homology and substrate affinity, PI3Ks are divided into three
classes (I-III) (Engelman, Luo et al. 2006). Class I PI3K is a heterodimeric protein
consisting of a p85 regulatory/adapter subunit and a p110 catalytic subunit. Class I PI3K
plays an important role in terms of insulin signaling and glucose homeostasis (Rameh and
16
Cantley 1999; Engelman, Luo et al. 2006). The role of the class II and III PI3Ks is still
poorly understood.
After insulin stimulation tyrosine phosphorylated IRS proteins bind to the regulatory
subunit (p85) of the class I PI3K. This activates the catalytic subunit p110 and leads to the
phosphorylation of membrane phospholipids and phosphatidylinositol- 4, 5- bisphosphate
(PIP2) on the 3’ position (Vollenweider 2003; Engelman, Luo et al. 2006) (Figure 1). The
formation of phosphatidylinositol- 3, 4, 5- trisphosphate leads to the activation of 3phosphoinositide dependent protein kinase (PKD- 1 and PKD- 2). PKD regulates
downstream phosphorylation of Akt/protein kinase B (PKB) and atypical isoforms of
protein kinase C (aPKC), which are dependent neither on diacylglycerol (DAG) nor Ca2+
(Cantley 2002; Saltiel and Pessin 2002; Vollenweider 2003; Engelman, Luo et al. 2006).
AKT/protein kinase B (PKB)
The serine/threonine kinase AKT possesses a N-terminal PH domain that is followed by a
catalytic kinase domain and a C-terminal tail. There are three isoforms of AKT: AKT1,
AKT2 and AKT3 (AKTα, AKTβ, AKTγ, respectively), which are expressed ubiquitously
(Bjornholm and Zierath 2005; Kim and Novak 2007). AKT1 is the major isoform
expressed in muscle, whereas AKT2 expression has been shown to be predominant in
adipocytes (Walker, Deak et al. 1998). AKT3 has been shown to be expressed mainly in
the brain and it is not activated in muscle or adipose tissue in response to insulin (Konishi,
Kuroda et al. 1995; Walker, Deak et al. 1998). The activation of AKT requires
phosphorylation at two specific sites, Thr308 that is localized in the kinase domain (for
AKT1 isoform) and Ser473 in the C-terminal domain (for AKT1 isoform). PDK1 has been
identified as the kinase responsible for the phosphorylation at the Thr308 site. The
mechanism that leads to the phosphorylation of AKT at Ser473 is not well understood;
PDK1 and PDK2, as well as autophosphorylation of AKT may be involved (Hajduch,
Litherland et al. 2001; Vollenweider 2003).
17
Targets of AKT
AKT has been demonstrated to act as an anti-apoptotic kinase, which has a crucial role in
cell survival. AKT regulates the activity of proteins that are involved in apoptosis
including BAD, members of the forkhead family of transcription factors and transcription
factor NF-κB. Importantly, AKT is involved in the regulation of metabolic events such as
glucose metabolism in skeletal muscle and adipocytes (Hajduch, Litherland et al. 2001;
Vollenweider 2003). Glycogen synthase kinase -3 (GSK-3), which controls glycogen and
protein synthesis among many other cellular processes, was one of the first described
physiological targets of AKT (Cross, Alessi et al. 1995). GSK-3 possesses two isoforms,
GSK-3α and GSK-3β, which remain active in the basal, unstimulated state. Upon insulin
stimulation, the activity of GSK-3 is inhibited via phosphorylation at Ser21 or Ser9 (GSK3α and GSK-3β, respectively). This event is mediated through the PI3K-AKT signaling
pathway. Moreover, insulin-stimulated inhibition of GSK promotes dephosphorylation
and theryby activation of the glycogen synthase (GS), which leads to stimulation of
glycogen synthesis (Grimes and Jope 2001).
Glucose uptake is another important process that is regulated by insulin via the PI3K-AKT
pathway in skeletal muscle (Hajduch, Alessi et al. 1998; Wang, Somwar et al. 1999;
Karlsson, Ahlsen et al. 2006) and adipocytes (Kohn, Summers et al. 1996; Foran, Fletcher
et al. 1999; Bai, Wang et al. 2007). AKT promotes translocation of the insulin dependent
glucose transporter GLUT4 from the intracellular space to the plasma membrane. Several
studies have indicated that this process is mediated by the downstream target of AKT,
AKT substrate 160 (AS160), which is phosphorylated at five crucial residues (Ser318,
Ser570, Ser588, Thr642, and Thr751) in response to insulin (Sano, Kane et al. 2003; Zeigerer,
McBrayer et al. 2004).
aPKC
Protein kinase C isoforms are important intracellular molecules that control many cellular
events such as cell growth, cell differentiation, glucose and lipid metabolism. PKCs are
divided into three classes according to their domain structure and regulation: conventional
(cPKC), novel (nPKC) and atypical (aPKC) (Bertram and Ley 2011; Turban and Hajduch
18
2011). Conventional and novel PKCs are usually activated by diacylglycerol (DAG) and
have been shown to have a negative impact on insulin signaling. Their role in the
regulation of insulin signaling will be discussed later (Hotamisligil 2006). The aPKCs
(aPKCλ/ζ), which lack the structural domains that bind lipids and Ca2+, are regulated by
PDK1, the downstream target of PI3K. In skeletal muscle (Etgen, Valasek et al. 1999)
and adipocytes (Kotani, Ogawa et al. 1998) the overexpression of aPKC leads to an
increase in both basal and insulin-stimulated glucose transport. In addition, muscle
specific deletion of both isoforms of aPKCs affects insulin-stimulated glucose transport,
as well as GLUT4 translocation (Farese, Sajan et al. 2007). Thus, these data suggest that
aPKCs are also involved in the direct stimulation of GLUT4 transporter, independent from
AKT.
2.1.2 MAPK pathways
Apart from the PI3K pathway insulin controls another well-characterized signaling
cascade, which is known as the Ras/ERK (or mitogen activated protein kinase - MAPK)
pathway (Figure 1). The MAPK pathway is activated in response to insulin and growth
factors, such as IGF1, but also in response to cellular stress (Widegren, Ryder et al. 2001).
Recruitment of the signaling target Shc as well as IRS to the insulin receptor (IR),
activates the Ras/ERK cascade. Both Shc and IRS proteins bind to the adaptor GRB2
protein that is in complex with the mSOS protein (Weng, Smith et al. 2001). The mSOS
protein, a p21ras guanine nucleotide exchange factor (ras-GNRF), facilitates the conversion
of inactive Ras-GDP to active Ras-GTP (Downward 1996). This leads to the
phosphorylation of Raf and downstream activation of ERK 1 and ERK 2 (MAPK 1 and
MAPK 2, respectively (Blenis 1993; Widegren, Ryder et al. 2001). Activated ERKs
regulate a number of transcription events that are involved in DNA synthesis and cell
cycle progression. For instance, ERKs phoshorylate Elk-1, a transcription activator which
mediates the expression of immediate early genes including c-fos (Blenis 1993).
2.1.3 CAP/Cbl/TC10 pathway
A decade ago a novel signaling pathway, CAP/Cbl/TC10 pathway, that mediates insulin
signaling independent of the PI3K-AKT pathway, was described (Baumann, Ribon et al.
19
2000; Chiang, Baumann et al. 2001). The CAP/TC10 pathway is involved in the
regulation of glucose transport in adipocytes (Baumann, Ribon et al. 2000; Chiang,
Baumann et al. 2001). The CAP protein (Cbl-associated protein), which is expressed
mostly in insulin sensitive tissues, functions as an adaptor protein for Cbl. Cbl
phosphorylation leads to dissociation of the CAP/Cbl-complex from the IR, its
translocation to caveolae compartments of the cell membrane and activation of TC10, a
small GTP binding protein belonging to the Rho-family. TC10 regulates the translocation
of the GLUT 4 transporter synergistically with PI3K (Chiang, Baumann et al. 2001).
However, the role of the CAP/Cbl/TC10 pathway in metabolic regulation in skeletal
muscle is not yet well understood.
2.1.4 Defects in insulin signaling and metabolism in human skeletal muscle
Skeletal muscle insulin resistance is an early defect in Type 2 diabetes (DeFronzo, Jacot et
al. 1981; DeFronzo and Tripathy 2009). Therefore, a deeper understanding of the
mechanisms which lead to dysregulation of insulin action in muscle may play a significant
role in drug development. Several techniques have been employed to study molecular
events that occur in skeletal muscle in insulin resistant states. A widely used in vivo
method to measure insulin action is the euglycaemic hyperinsulinemic clamp. This
technique is the golden standard to study whole body insulin action, and it can be
combined with muscle biopsies, which further allow to study molecular events involved in
insulin resistance (DeFronzo and Tripathy 2009). However, to gain more insight into the
events underlying insulin resistance, independent of systemic factors such as ambient
glycaemia, hyperlipidemia or circulating cytokines, direct in vitro techniques to study
glucose metabolism and insulin action are necessary. In 1988, the method employing in
vitro muscle preparation was described for the first time by Dohm et al. (Dohm, Tapscott
et al. 1988). Human primary muscle cells provide another widely used experimental tool
to investigate impairments in metabolic regulation and insulin signaling pathway. Primary
human muscle cells possess the features of mature muscle tissue and importantly their
diabetic phenotype is sustained in culture (Gaster, Petersen et al. 2002).
20
Defects in the early insulin signaling
The data regarding phosphorylation of IR in obese and type 2 diabetic subjects remain
contradictory. There is a correlation between the expression of IR and obesity (Goodyear,
Giorgino et al. 1995). Moreover, the IR autophosphorylation was impaired in abdominal
skeletal muscle obtained from lean diabetic subjects (Maegawa, Shigeta et al. 1991). The
results from euglycaemic clamp studies showed a modest impairment in IR kinase activity
in nondiabetic obese, whereas obese type 2 diabetic patients demonstrated a significant
decrease in comparison to healthy lean or nondiabetic obese people (Nolan, Freidenberg et
al. 1994). On the other hand, Krook et al. reported no impairment in the IR
autophosphorylation in overweight type 2 diabetic men in comparison to healthy lean men
(Krook, Bjornholm et al. 2000). Furthermore, subsequent studies reported no changes in
the IR activation (Meyer, Levin et al. 2002; Kim, Kotani et al. 2003). Thus, it appears that
major defects in the insulin signaling cascade occur downstream of IR.
IRS-1 and IRS-2, the major downstream targets of IR, are the predominant IRS isoforms
that are expressed in skeletal muscle. Reduced insulin-stimulated phosphorylation of IRS1 has been demonstrated in muscles from type 2 diabetic subjects during
hyperinsulinaemic clamps in vivo, as well as in vitro in the muscle strip preparation (Cusi,
Maezono et al. 2000; Krook, Bjornholm et al. 2000; Kim, Kotani et al. 2003). The human
IRS-1 protein possesses over 20 potential tyrosine phosphorylation sites and more than 30
serine/threonine phosphorylation sites, which play a crucial role in the regulation of the
IRS activity (Bjornholm and Zierath 2005; Frojdo, Vidal et al. 2009). The phosphorylation
of the IRS-1 at Ser312 (Ser309 in rats) has been implicated in the negative regulation of the
insulin signaling cascade in cell and animal models, as well as in type 2 diabetic patients
(Aguirre, Uchida et al. 2000; Bandyopadhyay, Yu et al. 2005; Taniguchi, Emanuelli et al.
2006). The phosphorylation of IRS at this serine residue leads to decreased IRS tyrosine
phosphorylation, with consequent impaired activation of PI3K (Bandyopadhyay, Yu et al.
2005). A number of serine/threonine kinases, including c-Jun N-terminal kinase (JNK), an
inhibitor of NFκB kinase (IKK) and protein kinase C, which have been demonstrated to
have increased activity in obesity and type 2 diabetes, have been reported to diminish
insulin action by serine phosphorylation of IRS-1 (Hotamisligil 2006).
21
The involvement of IRS-2 in the regulation of insulin action is poorly understood. In
contrast to IRS-1, which is centrally involved in the regulation of glucose metabolism,
IRS-2 regulates lipid metabolism and the MAPK signaling pathway in primary human
skeletal muscle cells (Bouzakri, Zachrisson et al. 2006). A decrease in IRS-2-associated
PI3K activity has been reported in human skeletal muscle obtained from diabetic subjects
(Kim, Nikoulina et al. 1999). Further studies are needed to investigate the metabolic role
of IRS-2 in human skeletal muscle.
Defects in the PI3K pathway
The phosphatidyl inositol-3 kinase (PI3K) plays a crucial role in insulin-mediated signal
transduction, and controls glucose uptake and GLUT4 translocation. Alterations in PI3K
activity in human skeletal muscle from type 2 diabetic subjects have been described in a
number of independent in vivo and in vitro studies (Bjornholm, Kawano et al. 1997; Kim,
Nikoulina et al. 1999; Krook, Bjornholm et al. 2000; Bandyopadhyay, Yu et al. 2005).
Data regarding defects in AKT activity in obese and type 2 diabetic patients have been
controversial. Significant defects in the phosphorylation of AKT at Ser473 or Thr308 in
skeletal muscle obtained from type 2 diabetic patients have been described (Krook, Roth
et al. 1998; Meyer, Levin et al. 2002; Karlsson, Zierath et al. 2005; Cozzone, Frojdo et al.
2008). However, other investigators have found no changes in the phosphorylation or
activity of AKT in type 2 diabetic people (Kim, Nikoulina et al. 1999; Krook, Bjornholm
et al. 2000). Any impairment in the AKT phosphorylation at the level of the specific
phosphorylation site is also unclear. It has been reported that the phosphorylation of
AKT473 is unaltered, while the phosphorylation of AKT308 is significantly decreased in
skeletal muscle from type 2 diabetic subjects (Karlsson, Zierath et al. 2005). On the other
hand, Cozzane et al. reported a decrease in insulin-stimulated phosphorylation at Ser473,
but not at Thr308 in skeletal muscle of Type 2 diabetic subjects during hyperinsulinaemiceuglycaemic clamp (Cozzone, Frojdo et al. 2008). The differences in the activity of AKT
might be explained by isoform-specific defects, as most of the studies mentioned above
have measured the global phosphorylation of AKT. Isoform specific impairments of
AKT2 and AKT3, but not AKT1 in response to insulin have been observed in skeletal
22
muscle obtained from morbidly obese insulin resistant subjects (Brozinick, Roberts et al.
2003). In addition, a decrease in the phosphorylation of AKT2 at Ser473 and AKT1 at
Thr308 has been reported in human primary muscle cells from Type 2 diabetic patients
(Cozzone, Frojdo et al. 2008). The variability of AKT activation can also be due to
different experimental models (muscle biopsy, muscle strips and primary cells) and
experimental conditions (normoglycaemia and hyperglycaemia), but can also be due to
subject characteristics, which has not been comparable in most studies.
AS160 is a downstream target of AKT, and links PI3K/AKT signaling to GLUT4
translocation. The insulin-stimulated phosphorylation of AS160 is significantly decreased
in skeletal muscle from type 2 diabetic subjects (Karlsson, Zierath et al. 2005). Infusion of
TNF-α, a well-known cytokine to induce insulin resistance, was also positively correlated
with impaired AS160 phosphorylation in healthy subjects (Plomgaard, Bouzakri et al.
2005). Several studies have reported defects in GLUT4 translocation from the intracellular
pool to the cellular membrane in human skeletal muscle from T2D patients (Ryder, Yang
et al. 2000; Koistinen, Galuska et al. 2003). Recently, the hypothesis of involvement of
AS160 in GLUT4 translocation has been proven in 3T3-L1 adipocytes (Eguez, Lee et al.
2005) and L6 cells (Thong, Bilan et al. 2007). Additionally, impairments in glucose
transport correlated with decrease in phosphorylation of AS160 in skeletal muscle from
type 2 diabetic men (Karlsson, Ahlsen et al. 2006).
GLUT4 translocation and subsequent increases in glucose transport are also stimulated in
an insulin-dependent manner by aPKCs, which operate downstream of PI3K and its lipid
product PIP3. However, the data regarding the role of aPKCs in human skeletal muscle are
limited. In subjects with impaired glucose tolerance (IGT), which is considered a
prediabetic state, and in subjects with type 2 diabetes, aPKC activation during the
hyperinsulinaemic euglycaemic clamp is markedly decreased (Beeson, Sajan et al. 2003).
In cultured myotubes from IGT subjects, there is a significant reduction of aPKC activity
in response to insulin. This is also associated with impaired glucose uptake (Vollenweider,
Menard et al. 2002).
23
Defects in glucose transport and glycogen synthesis
During the euglycaemic hyperinsulinaemic clamp, 20-25 % of glucose is utilized in
skeletal muscle to produce energy in glycolytic processes, where glucose is oxidized to
CO2 and H2O via the citric acid cycle, ultimately leading to generation of ATP. However,
the major part, ~75-80 % of glucose disposal is accounted for by nonoxidative glucose
metabolism where glucose is converted into glycogen and stored for later energy
utilization (DeFronzo and Tripathy 2009). Impaired glycogen synthesis and reduced
glycogen synthase activity are considered among the earliest detectable metabolic defects
in type 2 diabetes (Bogardus, Lillioja et al. 1984; Shulman, Rothman et al. 1990).
However, impaired insulin stimulated glucose transport is the key rate-limiting step in the
reduced glycogen synthesis and glucose uptake in the insulin resistant state (Cline,
Petersen et al. 1999).
Glucose is a hydrophilic molecule and has to diffuse into the cell via a lipid bilayer. This
is mediated by membrane transporter proteins, such as GLUTs that facilitate glucose
uptake. To date, at least 14 GLUTs have been described (GLUT 1-14) (Vollenweider
2003). In skeletal muscle, GLUT1 is responsible for mediating basal glucose transport,
whereas GLUT4 controls the major part of the insulin-stimulated glucose transport
(Tordjman, Leingang et al. 1989). Insulin-stimulated glucose transport is reduced in
skeletal muscle obtained from type 2 diabetic subjects. While the total protein content of
GLUT 4 is unchanged in these subjects, the protein content at the cell surface is markedly
reduced (Bouzakri, Koistinen et al. 2005).
2.2 AMP –activated protein kinase pathway
2.2.1 The structure and regulation of AMPK
AMP-activated protein kinase (AMPK) plays a major role in the regulation of whole body
energy balance and constitutes an alternative, noninsulin-dependent pathway to improve
glucose and lipid metabolism. In skeletal muscle and adipose tissue, AMPK is activated
by the action of various adipokines, such as leptin and adiponectin, as well as by changes
24
in the AMP/ATP ratio (for example during glucose deprivation or hypoxia) and cellular
concentration of Ca2+, which are linked to energy deprivation (Zhang, Zhou et al. 2009).
AMPK is a heterotrimeric enzyme composed of the catalytic subunit α1 or α2, and two
regulatory subunits (β1 or β2, and γ1, γ2 or γ3). AMPK is activated via the
phosphorylation at Thr172 at the catalytical α subunit (Zhang, Zhou et al. 2009). This
critical step is needed for the maximal activation of the enzyme and is limited by upstream
kinases like LKB1, calcium/calmodulin dependent protein kinase β (CaMKKβ) and
mammalian transforming growth factor β-activated kinase (TAK1) (Hawley, Pan et al.
2005; Hurley, Anderson et al. 2005; Momcilovic, Hong et al. 2006). The role of the
different kinases involved in the activation of AMPK is still unresolved. Nevertheless,
there is compelling evidence that LKB1 is required for the regulation of AMPK in
response to changes in AMP/ATP ratio. The γ-subunit of AMPK possesses four CBS
(cystathionine-β-synthase) domains, which are involved in AMP binding. Binding of
AMP to AMPK activates the enzyme allosterically, as well as inhibits the
dephosphorylation of AMPK at Thr172. In addition, constitutively active LKB1 leads to
increases in phosphorylation at Thr172, since the dephosphorylation is inhibited (Sanders,
Grondin et al. 2007).
2.2.2 Downstream targets of AMPK in skeletal muscle
In skeletal muscle, the activation of AMPK occurs mainly in response to contraction and it
is linked with increased energy demand and ATP turnover. AMPK regulates a number of
metabolic processes in skeletal muscle, including fatty acid oxidation, glucose transport,
and glycogen synthesis as well as mitochondrial biogenesis.
Fatty acid oxidation
AMPK regulates fatty acid (FA) oxidation in skeletal muscle via the malonyl-CoA
signaling network (Figure 2). Malonyl-CoA is an allosteric inhibitor of carnitine
palmitoyltransferase 1 (CPT-1), the enzyme that controls the transfer of long-chain fatty
acids into the mitochondria (Koh, Brandauer et al. 2008).
25
Activation of AMPK leads to an increases in fatty acid oxidation via phosphorylation and
inactivation of ACC2 isoform, which is involved in the production of malonyl-CoA
(Winder and Hardie 1996; Dean, Daugaard et al. 2000). During exercise, AMPK inhibits
ACC and the production of malonyl-CoA and thereby activates downstream CPT-1. This
promotes fatty acid uptake into the mitochondria and hence FA oxidation (Hardie 2011).
In addition, AMPK stimulates FA oxidation through the activation of malonyl-CoA
decarboxylase, which catalyzes decarboxylation and degradation of malonyl-CoA (Saha,
Schwarsin et al. 2000). Activation of AMPK reduces elevated free fatty acids and
intramuscular triglycerol content in skeletal muscle. Thefore, AMPK plays an important
regulatory role in insulin sensitivity.
Regulation of glucose transport
Apart from FA oxidation (Figure 2), AMPK is involved in the stimulation of glucose
transport that is independent of insulin, but has an additive effect to insulin action. Studies
have shown that physical activity or pharmacological compounds that mimic exercise can
increase GLUT 4 translocation and glucose transport in skeletal muscle from rodents and
humans (Kurth-Kraczek, Hirshman et al. 1999; Fryer, Foufelle et al. 2002; Koistinen,
Galuska et al. 2003). The mechanisms that lead to stimulation of glucose transport by
AMPK are incompletely understood. It has been proposed that AMPK phosphorylates
AS160 (TBC1D1) in human skeletal muscle. However, recent studies have introduced
TBC1D4 as the main target of AMPK that links the activation of the enzyme to glucose
transport. Importantly, AMPK can also promote glucose transport by increasing the
activity of the GLUT1 transporter in muscle cells (Fryer, Foufelle et al. 2002). In addition,
chronic activation of AMPK promotes gene transcription of the GLUT4 transporter
(Zheng, MacLean et al. 2001).
Glycogen synthesis
Glycogen synthase (GS), the enzyme that controls the last step of glycogen synthesis, is
one of the targets of AMPK. GS activity is reduced through phosphorylation at Ser7,
which is mediated by AMPK. This leads to a decrease in glycogen synthesis (Jorgensen,
Nielsen et al. 2004). Interestingly, the β-subunit of AMPK possesses the ability to bind
26
glycogen (Hudson, Pan et al. 2003; Polekhina, Gupta et al. 2003) and it has been
suggested that glycogen itself can inhibit AMPK activity (McBride, Ghilagaber et al.
2009). However, the mechanism of glycogen regulation on AMPK activity is still poorly
understood.
Figure 2. AMPK signaling pathway.
Mitochondrial biogenesis
AMPK has also been shown to upregulate the expression of the transcriptional coactivator PPARγ co-activator-1α (PGC-1α), which promotes the expression of genes
involved in mitochondrial biogenesis (Hardie 2011). Although it has been reported that
AMPK has a direct effect on PGC-1α phosphorylation in skeletal muscle (Jager,
Handschin et al. 2007), the mechanism may involve deacetylation of PGC-1α by Sirt1,
which acts downstream of AMPK (Canto, Gerhart-Hines et al. 2009; Canto, Jiang et al.
2010).
27
2.2.3 AMPK activators
2.2.3.1 Physiological activators
Leptin
Leptin is secreted by adipocytes and this hormone is involved in the regulation of
numerous metabolic processes including glucose and lipid metabolism, as well as food
intake. Leptin has been shown to activate AMPK in skeletal muscle, which is linked with
the stimulatory effect of leptin on glucose transport and lipid oxidation (Minokoshi, Kim
et al. 2002). Moreover, leptin has a positive impact on insulin sensitivity by preventing
lipid accumulation in peripheral tissues such as skeletal muscle. Chronic treatment with
leptin decreases the triacyglycerol content in skeletal muscle from rodents on high fat diet
and this is associated with improvements in insulin-stimulated glucose uptake and
glycogen synthesis (Yaspelkis, Singh et al. 2004). However, obesity is a leptin resistant
state, as indicated by high levels of circulating leptin in obese humans and rodents
(Maffei, Halaas et al. 1995; Considine, Sinha et al. 1996). Treatment of obese patients
with leptin does not have an effect on weight loss (Heymsfield, Greenberg et al. 1999).
Taken together, these data suggest that obese humans are resistant to both endogenous and
exogenous leptin.
Adiponectin
Adiponectin is a 30 kDa adipokine that activates AMPK. Adiponectin enhances insulin
sensitivity in skeletal muscle and liver from animals by affecting glucose and lipid
metabolism (Tomas, Tsao et al. 2002; Yamauchi, Kamon et al. 2002). Under physiological
conditions plasma concentrations of adiponectin account for 0.01 % of total proteins in
humans (Dyck, Heigenhauser et al. 2006). Several lines of evidence indicate that lower
levels of circulating adiponectin are associated with obesity and type 2 diabetes in rodents
and humans (Hu, Liang et al. 1996; Arita, Kihara et al. 1999; Hotta, Funahashi et al. 2001;
Ryo, Nakamura et al. 2004). In skeletal muscle, globular adiponectin (gAd) regulates fatty
acid oxidation via increased phosphorylation of AMPK and its downstream target ACC
(Yamauchi, Kamon et al. 2002; Ceddia, Somwar et al. 2005). Moreover, adiponectin
enhances GLUT4 translocation and glucose transport independently from the insulin
28
signaling cascade, suggesting that other pathways, such as AMPK, are involved in the
mechanism of gAd action (Ceddia, Somwar et al. 2005). To date, there have been only a
few studies that have addressed the effect of gAd on metabolism in human skeletal
muscle. In cultured myotubes obtained from obese subjects, the phosphorylation of
AMPK and FA oxidation are blunted at low gAd concentration. In myotubes from diabetic
subjects high adiponectin concentrations are able to activate AMPK, but there are no
changes in the phosphorylation of ACC or FA oxidation (Chen, McAinch et al. 2005). In
human skeletal muscle strips from obese individuals, fatty acid oxidation is not affected
by exposure to globular adiponectin. Although there is no difference in the glucose
transport rate between obese and lean women in response to gAd, the additive effect of
gAd on insulin action is impaired in obese individuals (Bruce, Mertz et al. 2005). In
summary, these data suggest the presence of adiponectin resistance in obesity and type 2
diabetes. The mechanism of adiponectin resistance remains unknown. However, it is
unlikely to be dependent on changes in the AdipoR1 receptor expression (Thrush,
Heigenhauser et al. 2008; Mullen, Pritchard et al. 2009).
2.2.3.2 Pharmaceutical activators
TZDs
Thiazolidinediones (TZDs), such as rosiglitazone or pioglitazone, were widely used
therapeutic agents to treat type 2 diabetes before the concerns regarding cardiovascular
risks led to withdrawal of rosiglitazone (Quinn, Hamilton et al. 2008). TZDs are known to
enhance insulin sensitivity by improving glucose disposal and inhibiting gluconeogenesis.
TZDs improve insulin action via activation of proliferator-activated receptor- γ (PPAR- γ),
a transcription factor that is highly expressed in adipocytes. The activation of PPAR-γ in
adipose tissue leads to increased differentiation of adipocytes and formation of smaller
adipocytes that are more sensitive to insulin. However, it has been suggested that TZDs
may have direct metabolic effects on skeletal muscle independent of the activation of
PPAR- γ. Treatment of transgenic mice with no adipose tissue or with muscle specific
PPAR- γ deletion with TZD promotes insulin sensitivity (Burant, Sreenan et al. 1997;
Norris, Chen et al. 2003). In addition, in intact skeletal muscle from rat TZDs activate
AMPK and stimulate glucose uptake and lipid oxidation (LeBrasseur, Kelly et al. 2006).
In human primary muscle cells obtained form type 2 diabetic subjects treatment with
29
different TZDs improves fatty acid metabolism and decreases the activation of ACC, a
downstream target of AMPK (Cha, Ciaraldi et al. 2005).
AICAR
The pharmacological compound AICAR (5-aminoimidazole-4-carboxamide-1-β-Dribonucleoside) is the precursor of ZMP, which mimics AMP and thus activates AMPK in
a similar fashion as for example an increase in AMP to ATP-ratio during exercise.
Treatment with AICAR improves metabolic disturbances in animal models of insulin
resistance (Bergeron, Previs et al. 2001; Song, Fiedler et al. 2002; Pold, Jensen et al.
2005). In skeletal muscle from rodents, AICAR enhances glucose transport and GLUT4
translocation via insulin-independent pathway (Hayashi, Hirshman et al. 1998). Moreover,
AICAR significantly increases glucose uptake in isolated human skeletal muscle strips
from subjects with type 2 diabetes. This is associated with increased cell-surface content
of GLUT4 (Koistinen, Galuska et al. 2003). Chronic treatment with AICAR leads to
increased mitochondrial biogenesis in rat skeletal muscle (Winder, Holmes et al. 2000).
Thus, AICAR, as an exercise mimetic, is an excellent research tool to study the effects of
AMPK on glucose and lipid metabolism in metabolic disorders.
Metformin
Metformin is a commonly used antidiabetic agent that mainly acts as a suppressor of
glucose production in liver. It also enhances glucose transport in skeletal muscle. A
decade ago, it was shown that metformin activates the AMPK pathway in rat hepatocytes
and abolishes lipogenic gene expression via reduced expression of SREBP-1c, a key
lipogenic transcription factor (Zhou, Myers et al. 2001). In addition, AMPK activation by
metformin in rat skeletal muscle leads to an increase in glucose transport (Zhou, Myers et
al. 2001). Metformin has been shown to increase phosphorylation of AMPK also in
skeletal muscle of type 2 diabetic subjects (Musi, Hirshman et al. 2002).
30
2.2.3.3 Natural activators
Resveratrol
Resveratrol (RSV), a natural polyphenol that is found in the skin of grapes and peanuts,
has recently been shown to have antidiabetic properties. In vivo animal studies have
reported a beneficial effect of RSV on weight loss, lipid and DAG accumulation in muscle
(Um, Park et al. 2010). In addition, treatment with RSV increases mitochondrial
biogenesis and physical endurance in rodents (Lagouge, Argmann et al. 2006; Um, Park et
al. 2010). Although the compound has been discovered already a few decades ago, the
mechanism of its action on metabolism is not yet clear. Resveratrol has been reported to
increase the activity of SIRT1, a member of the sirtuin gene family, which shares
homology with the yeast Sir2 protein (Howitz, Bitterman et al. 2003). Sirt1 is a
histone/protein deacetylase that controls nicotinamide adenine dinucleotide (NAD+)dependent deacetylation of target substrates, such as PGC-1α (Lagouge, Argmann et al.
2006; Canto and Auwerx 2009). In addition to being involved in the regulation of
processes like life span extension and apoptosis, Sirt1 may play an important role in
glucose metabolism (Lagouge, Argmann et al. 2006; Canto and Auwerx 2009). Recent
studies have proposed that resveratrol acts via direct activation of AMPK, which is well
correlated with the stimulation of glucose uptake in rodent models (Breen, Sanli et al.
2008; Canto, Jiang et al. 2010; Um, Park et al. 2010). In addition, the activation of SIRT1
and deacetylation of PGC-1α by resveratrol may be dependent on AMPK activity (Canto,
Jiang et al. 2010).
2.3 Fatty acid-induced insulin resistance in skeletal muscle
Elevated free fatty acid concentrations and reduced fatty acid oxidation in muscle are
considered among the major causes of insulin resistance in obesity and type 2 diabetes.
Several clinical studies have reported an association with elevated plasma FFA levels and
impaired insulin sensitivity (Opie and Walfish 1963; McGarry 1992; Boden 2011). Acute
elevation of FFA in plasma by lipid infusion leads to insulin resistance (Boden 2011),
31
whereas lowering chronically elevated plasma FFA levels improves insulin sensitivity in
rodents and humans (Ahren 2001; Qvigstad, Mostad et al. 2003). Several mechanisms
have been suggested to explain how increased intramuscular fat may affect insulin
sensitivity. One theory is that generation of active fatty acid-derived metabolites, such as
diacylglycerol (DAG), long-chain fatty acyl-CoA:s and ceramides alter insulin action and
consequently lead to defects in glucose utilization and insulin resistance (Bajaj,
Suraamornkul et al. 2005; Holland, Brozinick et al. 2007; Kraegen and Cooney 2008).
Another concept suggests low-grade chronic inflammatory state, induced by adiposetissue derived cytokines, negatively affects insulin signaling (Hotamisligil 2006). Recent
studies have suggested endoplasmic reticulum (ER) stress as one of the major mechanisms
involved in the free fatty acid- induced insulin resistance (Ozcan, Cao et al. 2004). Finally,
an alternative theory based on the concept of mitochondrial overload and incomplete βoxidation has been proposed to explain the negative effects of free fatty acids in the
pathogenesis of insulin resistance (Koves, Ussher et al. 2008).
2.3.1 Intramuscular lipid metabolites
The metabolic fate of free fatty acids depends on their composition and energy needs of
the cell. Once entering the cell fatty acids are esterified into fatty acyl-CoA:s and at the
next step they can either be directed to β-oxidation in the mitochondria or to glycerolipid
synthesis such as formation of triacylglycerols (TG), diacylglycerols (DAG) or
sphingolipids (Holland, Knotts et al. 2007). Increased fatty acid uptake in relation to the
rate of β-oxidation, may lead to the accumulation of intramuscular active lipid
metabolites, such as DAG:s, long-chain fatty acyl-CoA:s and ceramides, which negatively
modulate insulin action (Holland, Knotts et al. 2007). The role of these lipid metabolites in
insulin resistance is discussed below.
2.3.1.1 Long chain fatty acyl-CoA:s
Acyl-CoA esters of long chain fatty acids have been introduced as a marker of insulin
resistance (Ellis, Poynten et al. 2000). High fat diet or lipid infusion increases the
accumulation of long chain fatty acyl CoA:s in skeletal muscle of rats and humans, and
this coincides with insulin resistance (Chalkley, Hettiarachchi et al. 1998; Ellis, Poynten et
al. 2000). Moreover, pharmacological inhibition of lipolysis with acipimox significantly
32
improves whole-body glucose disposal with a parallel reduction of intramuscular long
chain fatty acyl-CoA:s (Bajaj, Suraamornkul et al. 2005). The mechanism by which long
chain fatty acyl-CoA:s interfere with insulin signaling remains unclear. It is possible that
long chain fatty acyl-CoA:s may activate PKC isozymes (Yu, Chen et al. 2002).
2.3.1.2 Ceramides
Ceramides belong to the family of lipids and comprise the fundamental structure of all
sphingolipid molecules. These are composed of two FA chains covalently linked to
sphingosine. Previously it was assumed that ceramides are merely structural elements that
make up sphingomyelin, a major lipid in the cell membrane bilayer. Nowadays, it is wellestablished that ceramides act as signaling molecules and their synthesis is induced in
response to stress stimuli (e.g., UV radiation, or inflammatory mediators) (Bikman and
Summers 2011). There are two major pathways of ceramide synthesis – de novo synthesis
from saturated long chain fatty acids such as palmitate, which is a complex biosynthetic
pathway; and sphingomyelin hydrolysis, a process controlled by the enzyme
sphingomyelinase (Bikman and Summers 2011) (Figure 3).
In human skeletal muscle, the ceramide content is positively correlated with the fasting
plasma FFA concentrations (Adams, Pratipanawatr et al. 2004). Increased ceramide
accumulation was reported in skeletal muscle of insulin resistants rodents (Turinsky,
O'Sullivan et al. 1990), in intralipid/heparin infusion-induced insulin resistance
(Straczkowski, Kowalska et al. 2004), in obese insulin resistant humans (Adams,
Pratipanawatr et al. 2004), as well as in lean offspring of type 2 diabetic patients
(Straczkowski, Kowalska et al. 2007). Exposure to ceramide analogues alters the
activation of AKT/PKB and as a consequence leads to defects in GLUT4 translocation and
insulin-stimulated glucose uptake in muscle cells (Summers, Garza et al. 1998; Hajduch,
Balendran et al. 2001). Ceramides promote the inhibition of AKT/PKB via activation of
protein phosphatase 2 A (PP2A), which is the primary phosphatase responsible for the
dephosphorylation of AKT/PKB. In addition, ceramides inhibit translocation of AKT/PKB
from the cytoplasm to the plasma membrane (Bikman and Summers 2011). Myriocin is an
inhibitor of the enzyme serine palmitoyl transferase (SPT), which regulates the initial ratelimiting step of de novo ceramide synthetic pathway. Myriocin treatment lowers ceramide
concentration in muscle and improves glucose tolerance and insulin action at the level of
33
AKT/PKB in rodent models of obesity and diabetes (Holland, Brozinick et al. 2007).
Ceramides have also been linked to inflammatory response and activation of the toll-like
receptor 4 (TLR4), which is an essential mediator in the synthesis and secretion of
inflammatory cytokines (Bikman and Summers 2011). Recent data suggest that activation
of TLR4 via its agonists such as LPS or saturated free fatty acids, increases ceramide
production and transcription of genes encoding enzymes that are involved in de novo
ceramide synthesis (Holland, Bikman et al. 2011).
2.3.1.3 Diacylglycerol
DAG is a lipid metabolite that plays an important role as a second messenger in
intracellular signaling. DAG can be generated by esterification of two long chain fatty
acyl-CoA:s to glycerol-3-phosphate or by breakdown of phospholipids by the enzyme
phospholipase C or phosphatidylcholine by phospholipase D (Timmers, Schrauwen et al.
2008). Increased DAG content has been reported in skeletal muscle of insulin resistant
rodents (Heydrick, Ruderman et al. 1991; Avignon, Yamada et al. 1996) and humans
(Itani, Ruderman et al. 2002), as well as in skeletal muscle following lipid infusion (Yu,
Chen et al. 2002). In animal models, lipid infusion resulted in elevated levels of
intracellular DAG, which was associated with the activation of PKCθ, which is known to
inhibit insulin signaling via serine phosphorylation of the IRS-1(Itani, Ruderman et al.
2002; Yu, Chen et al. 2002). The accumulation of DAG has also been positively correlated
with increased activity of PKCθ in skeletal muscle of obese humans (Itani, Ruderman et
al. 2002).
It has been hypothesised that an increase in fatty acid oxidation can lower the level of
intramuscular lipid metabolites and thus protect the cells from fatty acid-induced insulin
resistance. In L6 muscle cells, overexpresion of CPT-1 protects the cells from palmitateinduced insulin resistance by reducing DAG and ceramide levels with a concommitant
decrease in the activation of PKCθ (Sebastian, Herrero et al. 2007).
2.3.2 Mitochondrial β-oxidation of fatty acids
A few decades ago, Randle et al introduced a link between muscle glucose and lipid
metabolism. They postulated that when β-oxidation of fatty acids is increased glucose
oxidation is decreased, a phenomenon that is called “Randle Cycle” (Randle, Garland et
34
al. 1963). The existence of the Randle Cycle would suggest that substrate preference
contributes to the development of insulin resistance. However, as mentioned above,
enhancing β-oxidation of fatty acids has been proposed as a protective mechanism to
combat insulin resistance. Additionally, a number of studies have shown that insulin
resistant subjects have a decrease in fatty acid oxidation capacity and an impaired
mitochondrial function (Sebastian, Herrero et al. 2007; Schenk, Saberi et al. 2008). Taken
together, free fatty acids may affect insulin stimulated glucose transport by a mechanism
different to the one proposed by Randle. Recent observations in skeletal muscle have
introduced a new intresting concept, which is based on the incomplete β-oxidation and an
increase in fatty acid oxidation in insulin resistant states.
Mitochondrial β-oxidation
Before long chain fatty acyl-CoA:s undergo β-oxidation, they must be transported across
the mitochondrial outer and inner membranes, as they cannot diffuse freely without a
transporter molecule. Transport is facilitated by a carnitine-dependent transport system,
which consists of carnitine palmitoyl transferase-1 (CPT-1), carnitine translocase (CT),
and carnitine palmitoyl transferase-2 (CPT-2). CPT-1 is the key and rate-limiting enzyme
that catalyses the reaction where long chain fatty acyl-CoA is covalently bound to
carnitine and forms an acylcarnitine. Acylcarnitine is then transported into the
mitochondria by CT. Once in the mitochondrial matrix, acylcarnitine is converted back to
long chain fatty acid and carnitine by CPT-2 (Mingrone 2004). Subsequently, the long
chain fatty acyl-CoA enters the β-oxidation cycle, where the length of the molecule is
reduced by two carbons per cycle producing acetyl-CoA, NADH and FADH2. The acetylCoA molecules are the end products of β-oxidation and enter the TCA cycle, which
produces NADH and FADH2. NADH and FADH2 are then used to produce ATP in the
electron transport chain (ETC) (Berg, Tymoczko et al. 2007). If acetyl-CoA molecules do
not enter the TCA cycle, they are synthetised into acylcarnitines by the enzyme carnitine
acetyl transferase (CAT), which is located inside the mitochondria (Adams, Hoppel et al.
2009).
35
Figure 3. Schematic representation of the two major pathways involved in the ceramide
synthesis.
2.3.2.1 Incomplete β- oxidation
The novel concept of incomplete β- oxidation suggests that lipid oversupply promotes βoxidation by activation of peroxisome proliferator-activated receptor (PPAR) genes and by
increased substrate supply, but without activation of TCA cycle and ETC. This results in
the failure of the muscle to completely oxidize fatty acids resulting in an accumulation of
acid soluble metabolites (ASM), such as acylcarnitines (Koves, Ussher et al. 2008). This
hypothesis is supported by animal studies where the markers of incomplete β-oxidation
accumulate in insulin resistant muscle. Conversely, reduction of the products of
incomplete β-oxidation improves insulin sensitivity (Koves, Ussher et al. 2008). Elevated
plasma acylcarnitine concentrations have been reported in type 2 diabetic patients
compared to non-diabetic people (Adams, Hoppel et al. 2009). In addition, increased
36
levels of urinary acylcarnitines have been observed in type 2 diabetic subjects, which
supports the existence of incomplete β-oxidation in insulin resistance (Moder, Kiessling et
al. 2003).
The mechanism by which incomplete β-oxidation affects insulin signaling and leads to
insulin resistance is unknown. Acylcarnitines may alter the function of the mitochondrial
proteins by acylation and acetylation (Kim, Sprung et al. 2006; Muoio and Koves 2007).
Additionally, incomplete β-oxidation can lead to the formation of reactive oxygen species
(ROS), which can lead to the formation of lipid peroxides and damage of the
mitochondrial enzymes and DNA (Andreyev, Kushnareva et al. 2005). Moreover, ROS
are know to activate inflammatory proteins, such as JNK and IKKβ (Bloch-Damti and
Bashan 2005).
2.3.3 Inflammation
Obesity and insulin resistance are inflammatory states, characterized by increased
production of proinflammatory cytokines and activation of inflammatory signaling
pathways (Hotamisligil 2006). Adipose tissue is an important initiator of the inflammatory
response. In addition to its role in storage of energy as fat, it is well established that
adipose tissue also functions as an endocrine and paracrine organ. A variety of cytokines
and chemokines, such as tumour necrosis factor-α (TNF-α), IL-6 or monocyte chemotactic
protein 1 (MCP-1) are secreted in abundance from obese insulin-resistant subjects
(Goossens 2008). Thus, adipose tissue may affect inflammatory signaling and insulin
resistance in skeletal muscle via circulating cytokines. In addition, plasma FA levels
derived from excess adipose tissue can activate inflammatory responses and affect insulin
sensitivity by the accumulation of lipids or via activation of Toll-like receptors.
2.3.3.1 Toll-like receptors
Toll-like receptors (TLR) play an essential role in the activation of inflammatory signaling
associated with innate immunity. Recently, it has been suggested that TLR2 and TLR4
receptors are involved in skeletal muscle insulin resistance. TLR4 is the best-described
TLR and known target for saturated fatty acids and LPS. In TLR4-knockout mice infusion
of lipids does not induce insulin resistance in skeletal muscle in comparison to wild type
37
mice, suggesting an important role of TLR4 in acute lipid-induced insulin resistance (Shi,
Kokoeva et al. 2006). Moreover, a loss-of-function mutation in TLR4 protects mice
against development of diet-induced insulin resistance (Tsukumo, Carvalho-Filho et al.
2007). In isolated intact soleus muscle from these animals, exposure to palmitate does not
affect insulin signaling, glucose uptake or glycogen synthesis. TLR4 is also involved in
ceramide biosynthesis (Holland, Bikman et al. 2011). The data regarding TLR2 are sparse
and the role of TLR2 in insulin resistance is less known. It has been demonstrated that
blocking the activity of TLR2 in C2C12 muscle cell line protects these cells against
palmitate induced insulin resistance (Senn 2006). Thus, both TLR2 and –4 appear to
contribute to lipid-induced insulin resistance.
2.3.3.2 Macrophages
Obese adipose tissue is infiltrated with an increased number of macrophages. These cells
are the source of proinflammatory cytokine secretion that may cause insulin resistance
(Olefsky and Glass 2010). Adipose tissue macrophage infiltration is positively correlated
with body mass index, adipocyte size and insulin resistant state (Goossens 2008). Recent
studies have shown the presence of macrophages also in skeletal muscle. Increased
macrophage content has been reported in skeletal muscle from obese mice (Weisberg,
McCann et al. 2003), as well as in HFD fed mice (Nguyen, Favelyukis et al. 2007).
Increased macrophage infiltration has also been observed in vastus lateralis biopsies from
obese humans (Varma, Yao-Borengasser et al. 2009). Co-culture of human myotubes with
macrophages in the presence of palmitic acid results in impairments in insulin signaling at
the level of AKT and increased activation of JNK and IκBα (Varma, Yao-Borengasser et
al. 2009). IKK-β deletion of myeloid cells in mice on HFD improves skeletal muscle and
whole body insulin resistance (Arkan, Hevener et al. 2005). Collectively, these studies
provide evidence that cytokines derived from macrophages either in adipose tissue or
skeletal muscle may contribute to the skeletal muscle insulin resistance.
2.3.3.3 Stress Kinases
Activation of cytokine receptors, intracellular lipid accumulation and activation of TLRs
lead to activation of stress kinases, such as c-Jun N-terminal kinase (JNK), inhibitor of
NF-κB kinase (IKK) and protein kinase C (PKC), which are central mediators of insulin
resistance.
38
NF-κB pathway
In the basal state NF-κB is bound to its inhibitory protein IκBα in the cytoplasm. IKKβ
phosphorylates IκBα, which subsequently targets IκBα to proteosomal degradation. This
results in nuclear translocation of NFκB and transcriptional activation of several
proinflammatory genes. In human skeletal muscle, fatty acid-induced insulin resistance is
closely associated with DAG accumulation and reduction of IκBα (Itani, Ruderman et al.
2002). Acute hyperlipidemia and HFD have also been reported to decrease IκBα levels in
rodent skeletal muscle (Bhatt, Dube et al. 2006). Targetting the IKKβ/NFκB signaling
pathway with high doses of salicylate, an inhibitor of IKKβ, prevents insulin resistance in
skeletal muscle from rodents (Kim, Kim et al. 2001) and humans (Kim, Kim et al. 2001).
IKKβ has also been shown to negatively affect insulin signaling by directly
phosphorylating IRS-1 at serine residues (Gao, Hwang et al. 2002). On the other hand,
muscle specific IKKβ knockdown mice are not protected against diet-induced insulin
resistance (Rohl, Pasparakis et al. 2004). Pharmacological or genetic modification of
NFκB does not protect C2C12 myotubes from insulin resistance induced by palmitate
(Hommelberg, Plat et al. 2011). The pharmacological approaches, such as treatment with
salicylate may actually be IKK-independent. It is known that salicylate is able to inhibit
serine kinases, such as JNK and S6K, which interfere with insulin signaling through IRS-1
phosphorylation (Gao, Zuberi et al. 2003). Therefore, IKKβ/NFκB pathway may not play
a central role in FFA-induced insulin resistance in skeletal muscle.
JNK
JNK activity is significantly increased in insulin resistant skeletal muscle of obese rats and
humans (Hirosumi, Tuncman et al. 2002; Bandyopadhyay, Yu et al. 2005; Todd, Watt et
al. 2007). Moreover, when challenged with HFD, mice with muscle specific JNK-1
deficiency are protected from serine phosphorylation of IRS-1 and muscle insulin
resistance (Sabio, Kennedy et al. 2010). The palmitate-induced insulin resistance is also
diminished in JNK-depleted C2C12 muscle cells (Vijayvargia, Mann et al. 2010). Taken
together, JNK activity plays an important role in obesity and diabetes and its inhibition
may be a potential target to treat insulin resistance in humans.
39
PKC
Conventional (c) and novel (n) PKC:s have a negative impact on the insulin signaling
pathway. These serine kinases can be activated by DAG and they induce insulin resistance
by phosphorylating defined residues of IRS-1 (Yu, Chen et al. 2002; Ragheb, Shanab et al.
2009). Among the several isoforms of novel/conventional PKCs, the PKCθ and PKCε are
mainly associated with DAG-induced skeletal muscle insulin resistance in rodents and
humans (Idris, Gray et al. 2001; Samuel, Petersen et al. 2010). Moreover, PKCθ knockout
mice are prevented from muscle insulin resistance during lipid infusion (Kim, Fillmore et
al. 2004). Increasing DAG content via inhibition of diacylglycerol kinase δ (DGKδ)
results in activation of n/c PKCs and increases phosphorylation of IRS-1 at Ser307 in intact
skeletal muscle from rat (Chibalin, Leng et al. 2008). Besides direct inhibitory
phosphorylation of IRS-1, PKCs can act upstream of the stress kinases JNK and IKKβ and
thereby influence insulin signaling by serine phosphorylation of IRS-1. PKCε has also
been shown to interfere with insulin signaling by directly associating with and inhibiting
the tyrosine kinase activity of the insulin receptor in skeletal muscle of diabetic animals
(Ikeda, Olsen et al. 2001). Finally, PKCζ has been shown to mediate ceramide-induced
insulin resistance, as discussed in section 2.3.1.2.
2.3.4 Endoplasmic reticulum stress
The ER stress response has strongly been implicated in obesity and the pathogenesis of
diabetes. ER stress affects insulin action in liver and adipose tissue as well as the function
and mass of the pancreatic beta cells (for review (Hotamisligil 2010; Cnop, Foufelle et al.
2012)). The role of ER stress in skeletal muscle in fatty acid-induced insulin resistance is
controversial and is discussed in more detail below.
2.3.4.1 UPR pathway
ER is an intracellular organelle and the principal site of protein folding and
posttranslational modification, lipid synthesis and calcium storage. Under conditions such
as high intracellular lipids, glucose deprivation or calcium imbalance, ER homeostasis is
disturbed and thus the organelle has developed an adaptive response system known as the
unfolded protein response (UPR) (Hotamisligil 2010). The canonical UPR pathway
40
consist of three different mediators: inositol requiring enzyme-1 (IRE1), PKR-like
endoplasmic reticulum kinase (PERK) and activating transcription factor 6 (ATF6) that
work to restore ER homeostasis (Figure 4). In “stress-free” cell, these three proteins are
bound to the chaperone-binding protein/glucose-regulated protein 78 (BiP/GRP78) and
remain inactive. Accumulation of misfolded proteins leads to the activation of these three
signaling arms by the dissociation of their proximal effectors from BiP (Bertolotti, Zhang
et al. 2000; Shen, Chen et al. 2002). Activation of PERK and IRE1 occurs via
transautophosphorylation, whereas the activation of ATF6 into an active transcription
factor occurs by cleavage in the Golgi apparatus by two proteases: serine protease site-1
(S1P) and the metalloprotease site-2 (S2P) (Chen, Shen et al. 2002; Flamment, Kammoun
et al. 2010). Active PERK phosphorylates the eukaryotic translation initiation factor 2
(eIF2α) at Ser 51 leading to the suppression of global protein translation (Harding, Zhang
et al. 1999). Moreover, phosphorylation of eIF2α induces downstream translation of
ATF4, which controls the gene expression of the CCAAT/enhancer binding protein
homologous protein (CHOP) (Ma, Brewer et al. 2002). However, eIF2α can also be
phosphorylated by other kinases like the double-stranded RNA-activated protein kinase
(PKR) and the general control non-derepressible kinase 2 (GCN2). The role of these
kinases in ER stress is unclear and thus eIF2α phosphorylation status alone cannot be used
to confirm the presence or absence of ER stress (Ron and Walter 2007). The release of
IRE1 from the BiP complex results in the activation of the endonuclease activity of IRE1
and results in splicing of the transcription factor X-box binding protein-1 (XBP-1)
(Sidrauski and Walter 1997). The spliced form of XBP-1 (XBP-1s) regulates
independently or in co-operation with ATF6 the production of chaperone proteins
(including BiP), ER-associated protein degradation (ERAD) and phospholipid synthesis,
to improve the folding capacity of ER and to alleviate the ER stress (Lee, Iwakoshi et al.
2003).
41
Figure 4. UPR pathway and its crosstalk with insulin signaling.
2.3.4.2 UPR pathway and the link to insulin signaling
ER stress and activation of the UPR have been linked to the insulin signaling pathway.
First, XBP-1 deficiency leads to the development of insulin resistance and type 2 diabetes
in mice on HFD (Ozcan, Cao et al. 2004). In addition, the activation of the IRE-1 arm
inhibits insulin action via the activation of JNK, which phosphorylates IRS-1 at specific
inhibitory serine residues. Recently, two independent studies demonstrated that XBP-1s
interacts with the p85 regulatory subunit of PI3K and that this association facilitates the
nuclear translocation of XBP-1s and induction of the UPR target genes (Park, Zhou et al.
2010; Winnay, Boucher et al. 2010). Park et al. demonstrated that in the liver of ob/ob
mice on HFD, this interaction is diminished and thereby the animals cannot cope with ER
stress. Moreover, overexpression of the p85 subunit in liver of these mice restores XBP-1s
translocation to the nucleus, enhances transcription of XBP-1s– regulated genes, and most
42
importantly, improves glucose tolerance (Park, Zhou et al. 2010). Although this novel
insulin regulated pathway may provide new approaches to treat diabetes and insulin
resistance, further studies on p85-XBP1s interaction are required to validate this
interaction in clinical context as well as in extrahepatic tissues.
2.3.4.3 ER stress in skeletal muscle
The link between ER stress and insulin resistance in skeletal muscle is less understood.
Presently, only a few studies have reported the presence of ER stress in skeletal muscle of
obese and type 2 diabetic animal models. In mice, ER stress markers are elevated after 6
and 20 weeks of HFD (Deldicque, Cani et al. 2010). Palmitic acid has been shown to
induce ER stress in C2C12 and L6 muscle cells (Peng, Li et al. 2011; Hage Hassan,
Hainault et al. 2012; Rieusset, Chauvin et al. 2012). However, the mechanism of ER stress
and its effect on insulin sensitivity has been divergent in these studies. Peng et al. have
demonstrated that treatment with 4-phenyl butyric acid (4-PBA), a chemical chaperone,
alleviates palmitate-induced ER stress in C2C12 and L6 cell lines and improves insulin
signaling and glucose uptake. Interestingly, the addition of oleate to the medium has a
similar effect as 4-PBA and protects the cells from palmitate-induced ER stress and
insulin resistance. On the other hand, in two other studies the prevention of palmitateinduced ER stress with the chemical chaperones 4-PBA or tauroursodeoxycholic acid
(TUDCA), a taurine-conjucated derivative of bile acids, does not prevent palmitateinduced insulin resistance. In addition, although overexpression of the chaperon protein
BiP reduces ER stress in C2C12 cells, this does not improve reduced insulin action
induced by palmitate (Rieusset, Chauvin et al. 2012). When muscle cells are treated with
tunicamycin (an inhibitor of protein glycosylation that induces ER stress) and with
chemical chaperones, the gene expression of the UPR pathway is decreased. The negative
effect of tunicamycin on insulin action is also prevented (Rieusset, Chauvin et al. 2012).
Similar effect of chaperones is also seen on glucosamine (GlcN)-induced insulin
resistance (Raciti, Iadicicco et al. 2010).
Less is known about the presence of ER stress in insulin resistant human skeletal muscle.
Induction of ER stress has been observed in human primary myotubes treated with
palmitate (Peter, Weigert et al. 2009). In human in vivo studies, treatment with the
43
chemical chaperone TUDCA for one month increases insulin sensitivity in liver and
muscle of obese men by approximately 30 % in comparison to the placebo group.
However, in this study the impairment in insulin signaling does not coincide with changes
in ER stress markers in skeletal muscle (Kars, Yang et al. 2010). Moreover, six weeks of
HFD resulted in small increases in blood glucose during oral glucose tolerance test, but
not in the activation of ER stress in skeletal muscle from physically active lean men
(Deldicque, Van Proeyen et al. 2011).
Taken together, there may be a dissociation between palmitiate-induced ER stress and
insulin resistance. ER stress plays an important role in glucosamine-induced insulin
resistance, whereas palmitate may impair insulin action via mechanisms different from ER
stress signaling.
2.3.4.4 ER stress and exercise
Skeletal muscle possess smooth ER called sarcoplasmic reticulum (SR), which is highly
specialized to maintain calcium concentration and has a minor role in protein secretion.
Thus, SR plays an important role in the regulation of muscle contraction. It has been
hypothesised that skeletal muscle adapts to exercise training via activation of the UPR
pathway that protects from further stress. Indeed, acute exercise activated ER stress
markers in skeletal muscle from mice. Moreover, a 4-week training activated a different
pattern of UPR markers in comparison to sedentary mice, who are trained only once (Wu,
Ruas et al. 2011). PGC-1α has been shown to regulate UPR pathway in response to
exercise through coactivation with ATF6 (Wu, Ruas et al. 2011). ER stress has also been
shown to be activated in human skeletal muscle after a 200 km run. This is accompanied
with a reduced activity of the proteasome, which suggests compensatory mechanisms to
protect against cellular stress (Kim, Jamart et al. 2011).
2.4 Insulin resistance in other tissues
In addition to skeletal muscle, liver and adipose tissue are additional main targets of
insulin action and insulin resistance in these organs accounts for the core defects in type 2
diabetes. Moreover, β-cell failure plays an important role in the progression of the
pathophysiological events leading to T2DM. Thus, deep understanding of the contribution
44
of these organs to whole body insulin resistance and the cross-talk between these tissues is
essential in attempts to prevent the development of T2DM and to effectively control
metabolic balance in diabetic patients.
2.4.1 Liver
Liver is one of the major secretory organs and has a pivotal role in carbohydrate and lipid
metabolism. Increased glucose production due to enhanced gluconeogenesis and
glycogenolysis is a metabolic hallmark of insulin resistance in type 2 diabetes mellitus
(Consoli, Nurjhan et al. 1990; Magnusson, Rothman et al. 1992). After an overnight fast,
the liver of healthy individuals produces glucose at the rate of ~2 mg/ kg per min, whereas
in diabetic state the production is increased up to ~2.5 mg/kg per min. Moreover, the
insulin-induced suppression of hepatic glucose production is impaired in Type 2 diabetes.
Increased hepatic glucose production in T2DM is in good correlation with the increased
fasting plasma glucose and fasting plasma insulin levels, and accounts for fasting
hyperglycaemia (DeFronzo, Ferrannini et al. 1989; Defronzo 2009). Increased hepatic
glucose production in T2DM is also related to increased circulating glucagon levels and
hepatic sensitivity to glucagon, lipotoxicity as well as glucose toxicity (Defronzo 2009).
Liver is the main site of de novo lipogenesis, which allows the synthesis of fatty acids
from excess carbohydrates in the diet. Newly synthesized fatty acids are esterified to
triacylglycerols that can later be secreted as lipoproteins such as VLDL. In physiological
conditions, there are also other sources of fatty acids that can be delivered for TG
synthesis in the liver. Among them the most important are non-esterified fatty acids
originating from the hydrolysis of TGs stored in adipose tissue. Imbalances in the rate of
fatty acid uptake and oxidation in the liver, hepatic de novo fatty acid synthesis, and
secretion of TG lead to ectopic lipid accumulation and insulin resistance in the liver
(Fabbrini, Sullivan et al. 2010). Recent evidence suggests that skeletal muscle insulin
resistance may be an early event responsible for eventual non-alcoholic fatty liver disease,
a predictor of metabolic syndrome and T2DM. Studies using magnetic resonance
spectroscopy have revealed that glycogen synthesis in skeletal muscle is decreased,
whereas hepatic de novo lipogenesis is increased after a carbohydrate meal in young
insulin resistant individuals. This results in an increase in liver triglyceride synthesis and
increased plasma triglyceride concentration (Petersen, Dufour et al. 2007). Importantly,
45
one bout of acute exercise increases postprandial glycogen synthesis in skeletal muscle
and decreases hepatic triglyceride synthesis (Rabol, Petersen et al. 2011). Thus, insulin
resistance in skeletal muscle is an early target to treat and prevent the development of nonalcoholic fatty liver disease.
2.4.2 Adipose tissue
The main function of the adipose tissue is to store excess energy in the form of TG.
During energy deprivation fat stored as TG undergoes lipolysis. Free fatty acids (FFA) are
then delivered to other tissues for energy production. Insulin is the main regulator of fatty
acid metabolism in adipose tissue, and insulin promotes fat storage by its antilipolytic
effect as well as by enhancing synthesis of TG:s. Adipose tissue is composed not only of
adipocytes (70 % of total mass) but also of stromal vascular fraction that contains immune
cells such as macrophages. Macrophages have a pivotal role in inflammatory responses
(Bays, Gonzalez-Campoy et al. 2008).
In T2DM, metabolic defects in adipose tissue can impact other tissues such as skeletal
muscle and liver via different mechanisms (Bays, Gonzalez-Campoy et al. 2008). First,
adipocytes are resistant to the antilipolytic effect of insulin, and studies using insulin
clamp technique have shown that lean type 2 diabetic and obese nondiabetic patients have
impaired antilipolytic effect of insulin (Groop, Bonadonna et al. 1989). This leads to an
elevation in plasma FFA concentrations, which may induce insulin resistance in other
tissues (Opie and Walfish 1963; Boden 2011). Moreover, adipose tissue secretes a large
number of different hormones, cytokines, chemokines and other peptides that influence
insulin action in an autocrine, paracrine and endocrine fashion. In obesity adipose tissue
macrophage content is increased. Inflamed adipose tissue has been suggested to contribute
to insulin resistance in other tissues such as skeletal muscle and liver by increased
secretion of several cytokines and proinflammatory mediators, such as TNF-α, IL-6 or
MPC-1. These cytokines also contribute to increased lipolysis (Hotamisligil 2006; Bays,
Gonzalez-Campoy et al. 2008). Adipose tissue also secretes adiponectin, an insulin
sensitizing adipokine. In insulin resistance, adiponectin secretion is markedly
compromised (Bays, Gonzalez-Campoy et al. 2008). Finally, in insulin resistance
adipocytes have a decreased capacity to store fat. Taken together, these aspects enable an
46
overflow of fatty acids to other tissues such as liver and skeletal muscle, and contribute to
development of insulin resistance (Bays, Gonzalez-Campoy et al. 2008).
2.4.3 The effect of insulin resistance on β-cell failure
Although insulin resistance plays an important role in the pathogenesis of T2DM, β-cell
failure is also essential factor and responsible for the progression of impaired glucose
tolerance (IGT) to T2DM. Multiple factors including age, genetic factors, and acquired
factors like glucotoxicity, lipotoxicity and insulin resistance contribute to β-cell failure
(DeFronzo and Abdul-Ghani 2011). Initially, plasma insulin concentrations are increased
in the insulin resistance state, which is viewed as a compensatory mechanism. However,
as β-cell failure progesses, first phase insulin secretion is blunted and β-cell mass
decreases. It is estimated that 50% of the β-cells are already lost at the detection of
hyperglycaemia. Finally, there may be a further deterioration of insulin secretion in T2DM
which leads to a need for insulin-based therapy, as in T1DM. Early prevention of
development of T2DM should protect against the loss of β-cells mass and function.
Weight gain and physical inactivity lead to insulin resistance and create pressure for βcells to hypersecrete insulin. This plays a role in progressive β-cell failure. Intrestingly,
exercise and weight loss can improve insulin sensitivity and glucose tolerance as well as
augment insulin secretion (Henry, Wallace et al. 1986; Koivisto, Yki-Jarvinen et al. 1986;
Kitabchi, Temprosa et al. 2005). In addition, treatment with TZDs, but surprisingly not
with metformin, can also preserve β-cell function besides their effect on insulin sensitivity
(DeFronzo and Abdul-Ghani 2011). Thus, the ideal intervention to prevent development
of T2DM and to improve glycaemic control in established diabetes would impact insulin
sensitivity and protect against the loss of β-cell mass and function.
47
3 Aims of the study
The specific aims of the study are:
1. To study if globular adiponectin (gACRP) impacts glucose transport in type 2
diabetic human skeletal muscle (study I).
2. To study the effect of rosiglitazone on glucose transport and metabolic signaling in
human skeletal muscle (study II)
3. To study acute metabolic effects of the polyphenol resveratrol, and to examine if
resveratrol could combat palmitate-induced insulin resistance in human skeletal
muscle (study III).
48
4 Methods
The methods used in this thesis are described briefly below. A more detailed description
of the methods can be found in the individual publications, which are marked with the
Roman numerals.
4.1 Subjects
The clinical characteristics of the subjects are presented in Table I.
Study group
No. of
subjects
Age
BMI
2
(kg/m )
Fasting
glucose
(mmol/l)
2h glucose
(mmol/l)
Study I
Nondiabetic
men
Type 2
diabetic men
15
59±1
28±1
5.6±0.1
5.4±0.4
12
56±1
30.5±1.1
6.7±0.3
ND
5.3±0.1
5.3±0.4
5.5±0.1
5.3±0.5
Study II
Healthy men
15
50±3
26.9±1.1
Study III
Healthy men
6
54±3
25±1.7
Table 1. Subject characteristics. Glucose concentration was determined from whole blood
(I,II) or from plasma (III). The volunteers were recruited separately for each study.
4.2 Open muscle biopsy (Studies I-III)
A muscle biopsy was taken surgically from vastus lateralis muscle under local anesthesia.
Muscle was placed in oxygenated Krebs-Henseleit buffer (KHB). Smaller muscle strips
(25 mg) were dissected, mounted on Plexiglass clamps, and incubated for 60-240 min at
35°C in KHB under basal conditions with or without palmitate, or with or without insulin,
49
or were exposed to gACRP, AICAR or rosiglitazone (Koistinen, Galuska et al. 2003).
4.3 Human primary muscle cells (study III)
A skeletal muscle biopsy was trypsin digested to isolate satellite cells. These were grown
to 80% confluent myoblasts in the proliferating medium (Dulbecco’s modified Eagle
Medium: Nutrient Mixture F–12 (DMEM/F12) medium supplemented with 20 % foetal
bovine serum (FBS), 1% penicillin, 1% streptomycin, 1% Fungizone). Subsequently,
myoblast were purified using magnetic cell separation with CD56 antibody.
Differentiation of the myoblast was started by switching proliferating medium to
differentiation medium (DMEM/F12 containing 2% FBS, 1% penicillin, 1% streptomycin,
1% Fungizone). The myotubes differentiated for 7 days were serum-starved for 2 h before
each experiment in low glucose-DMEM supplemented with 0.5 % FFA free BSA (AlKhalili, Kramer et al. 2004).
4.4 Immunocytochemistry (study III)
To assess the formation and purity of myotubes immunocytochemistry was used for the
visualisation of myogenin expresion. Briefly, myoblast were proliferated on glass
coverslips until they reached 80 % confluence and subsequently differentiation was started
The samples for the visualisation of myogenin were collected between 0-7 days. The
pictures were taken using AXIOVERT 200M microscope (Carl Zeiss AG, Germany).
4.5 L6 cell line (study III)
L6 myoblasts were obtained from American Type Culture Collection (ATCC). The cells
were proliferating in DMEM medium supplemented with 10 % FBS, 1% penicillin, 1%
streptomycin, and 1% Fungizone. At 80% confluence medium was switched to
differentiation medium (DMEM, 2 % horse serum (HS)).
All experiments were
performed using L6 myotubes differentiated for 7 days with 2 h starvation in low-glucose
DMEM supplemented with 0.5 % FFA-free BSA prior to the experiment.
50
4.6 Metabolic assays of intact muscle strips
4.6.1 Glucose transport (studies I,II)
Muscle strips were incubated in Krebs-Henseleit buffer supplemented with 5 mM glucose
and 0.1 % BSA or 4% FFA-free BSA depending on the study protocol. Intact skeletal
muscle strips were rinsed for 10 min in KHB containing 20 mM mannitol and 0.1 % BSA
or 4 % FFA-free BSA. For the last 20 min, muscle strips were transferred to KHB buffer
supplemented 5 mM 3-0-methyl [3H] glucose (800 µCi/mmol) and 15 mM [14C] mannitol
(53 µCi/mmol). Glucose transport was analyzed by measuring the accumulation of
intracellular of 3-0-methyl [3H] glucose in the scintillation counter (Koistinen, Galuska et
al. 2003; Glund, Deshmukh et al. 2007).
4.6.2 Glycogen synthesis
Human skeletal muscle strips were incubated in KHB (containing 4 % FFA free BSA and
5 mM glucose) with or without 1 mM palmitate and with or without 1.2 nM insulin for 4
h. Thereafter, muscles were transferred to KHB supplemented with 5 mM [14C]-glucose
(0.3 µCi/mmol) for 1 h to assess glucose incorporation rate into glycogen. Muscles were
frozen in liquid nitrogen and stored at -80oC. Glucose incorporation into glycogen was
analyzed by precipitation of glycogen and measuring radioactivity by liquid scintillation
counting (Glund, Deshmukh et al. 2007).
4.7 Metabolic assays in cell cultures (study III)
4.7.1 Glucose uptake
Human primary myotubes were pre-exposed to resveratrol (RSV) or other compounds for
4 h, followed by incubation with or without 100 nM insulin for 1 hour. Subsequently, the
cells were incubated in zero-glucose DMEM (0.5 % FFA free BSA, 10 µM 2-DeoxyGlucose, [3H]-2-Deoxy-D-Glucose (100 mCi/mmol) for 15 min to assess glucose uptake.
The concentrations of RSV and other compounds were maintained unchanged until the
end of the experiment. The radioactivity was measured in the β-counter (Al-Khalili,
Bouzakri et al. 2006).
51
4.7.2 Glycogen synthesis
After 4 h pre-exposure to compounds of interest, the cells were stimulated with insulin
(100 nM) for 2 h and labeled D-[U-14C]-glucose (1µCi/ml; final specific activity 0.18
µCi/µl) was added for the last 90 min. The glycogen was precipitated and the glucose
incorporation into glycogen was determined by measuring radioactivity by liquid
scintillation counting (Al-Khalili, Bouzakri et al. 2006).
4.7.3 Palmitate oxidation
The cells were exposed to RSV or other compounds of interest for 4 h with the addition of
[9,10-3H]-palmitic acid (5 µCi/ml of medium). The 3H labeled water was extracted from
the incubation medium with charcoal. The radioactivity of the samples was determined by
scintillation counting (Salehzadeh, Rune et al. 2011).
4.8 Western blotting (studies I-III)
4.8.1 Tissue processing (studies I,II)
Human muscle strips were homogenized in ice-cold buffer (20 mM Tris (pH 7.8), 137
mM NaCl, 2.7 mM KCl, 1 mM MgCl2, 1% Triton X-100, 10 % (w/v) glycerol, 10 mM
NaF, 0.5 mM Na3VO4, 1 µg/ml leupeptin, 1 µg/ml aprotinin, 0.2 mM PMSF, 1 mM DTT,
1 mM EDTA). The samples were put on rotor for 60 min at +4 oC and centrifuged for 10
min (12 000 g, +4 oC). Protein concentration was determined with BCA kit. Muscle
extracts were mixed with Laemmli buffer and heated (56 oC) for 20 min. Samples (30 µg)
were separated by SDS-PAGE (6-12 %). Proteins were transferred to PVDF membranes
and blocked in 5 % or 7.5 % milk or 5 % BSA. Membranes were incubated with primary
antibodies. Thereafter, membranes were incubated with secondary HRP-conjugated
antibodies. Immunoreactive proteins were detected by enhanced chemiluminescence (ECL
plus) and quantified by densitometry using the ImageJ software.
52
4.8.2 Cell lysates (study III)
Human primary myotubes or L6 myotubes were washed and extracted in ice-cold lysing
buffer (50 mM Tris-HCl, 150 mM NaCl, 1% NP-40, 0.5 mM Na3VO4, 1 µg/ml leupeptin,
1 µg/ml aprotinin, 0.2 mM PMSF). The samples were centrifuged (12 000 g) at +4 oC for
10 min. Protein concentration was determined with BCA kit. The supernatant was
resuspended in Laemmli Buffer and the protein samples were heated for 20 min at 56 oC.
The proteins (20 µg) were separated by SDS-PAGE, followed by transfer to the PVDF
membrane. Membranes were blocked in 5 % milk or 5% BSA and incubated with primary
antibodies. Next, membranes were washed and incubated with secondary antibodies for 1
hour at room temperature. The proteins were detected using enhanced chemiluminescence
and quantified by densitometry using the ImigeJ Software.
4.8.3 Immunoprecipitation (study III)
Human primary myotubes were lysed in ice-cold IP lysing buffer (50 mM Tris pH 7.5,
150 mM NaCl, 1 % NP-40, 0.5 % sodium deoxycholate) and lysates were pre-cleaned
with Protein A-Agarose and Protein G-Agarose. Anti-PGC-1α antibody was added and the
lysates were incubated overnight. Next, Protein-A agarose beads were added and
incubated for 4 h. The agarose-immunocomplex was washed with IP washing buffer (50
mM Tris pH 7.5, 250 mM NaCl, 0.1 % NP-40, 0.05 % sodium deoxycholate). The pellet
was suspended in Laemmli Buffer and boiled. For the detection samples were separated by
8 % SDS-PAGE and western blotting protocol.
4.9 Cell viability (study III)
The toxicity of acute exposure to RSV was measured in human primary myotubes or L6
myotubes using the compound 3- (4,5- Dimethylthiazol- 2- yl)- 2,5- diphenyl tetrazolium
bromide (MTT). The MTT test measures the formation of formazan by the mitochondrial
dehydrogenases, and therefore it has also been used as a test of mitochondrial function
(Morino, Petersen et al. 2012). Absorbance of the purple formazone (the reduced MTT
which is formed in the living cells) was measured at the wavelength of 560 nm, with
background substraction at 650 nm.
53
4.10 AMPK activity (study III)
The activity of AMPK isoform complexes α1/β2/γ1 and α2/β2/γ1 was measured to assess
the effect of RSV. AMPK (300 ng per reaction) was incubated with the SAMS synthetic
peptide substrate (HMRSAMSGLHLVKRR) (250 µg/ml), AMP (125 mM) and the
compound of interest for 2 h at 30 oC. The reaction was initiated by adding 250 µM [33P]ATP Assay Cocktail (50 µM ATP, 5 Ci/nmol [33P]-ATP per reaction). The reaction was
terminated on P81 paper strips, followed by washing with 1% phosphoric acid and
measurement of the radioactivity in the β-counter.
4.11 Muscle ATP and PCr concentrations
To confirm the viability of the muscle strips in study IV ATP and PCr concentrations were
measured. Intact muscle strips were incubated up to 360 min in KHB at 35oC with or
without 1 mM palmitate. ATP and PCr concentrations were assessed by Lowry’s
fluorometric method with modification (Lowery 1972).
4.12 Statistics
4.12.1 Statistics used for intact skeletal muscle strips (studies I,II)
All data are presented as mean ± SEM. Paired and unpaired Student´s t-tests were used to
analyse paired and unpaired data, respectively. All statistical analysis were performed with
SPSS statistical package (Version 13.0) (studies I,II) or with Prism statistical software
(study IV). P < 0.05 was considered significant.
4.12.2 Statistics used in cell culture models (study III)
All data are presented as mean ± SEM from at least three independent experiments. The
data were analyzed with one-way ANOVA with repeated measurements followed by
Tukey´s post hoc test. P < 0.05 was considered significant.
54
5 Results and discussion
5.1 Characteristics of the models used in the study.
In the current study, two models of skeletal muscle were used: human muscle strips and
human primary muscle cells. These models enable the use of strictly controlled incubation
conditions. However, as isolated human muscle strips maintain the composition of intact
and mature muscle tissue, this model more closely simulates physiological in vivo
conditions. This is an advantage over human primary muscle cells. On the other hand, the
viability of the human muscle strips is severely compromised after prolonged incubations
(Zierath 1995). Thus, this model can only be used in acute experiments. Human primary
muscle cells are more suitable to study the effect of chronic perturbations, and the amount
of available material usually does not create experimental limits. As human primary
muscle cells express all the insulin signaling components (Al-Khalili, Kramer et al. 2004)
and are able to sustain their diabetic phenotype in culture (Gaster, Petersen et al. 2002),
they are an important additional research tool to study muscle metabolism.
5.1.1 Viability of the human muscle strips
ATP and PCr concentrations at the beginning of the incubation (0 h) were 20.23±1.14
µM/g dry wt and 62.81± 5.19 µM/g dry wt, respectively; and decreased slightly after 6 h
incubation to 15.32 ±1.19 µM/g dry wt and 57.57± 2.72 µM/g dry wt, respectively (n=5)
(Figure 5, Skrobuk et al. unpublished). Incubation with palmitate for 6 h did not affect
ATP and PCr concentrations (14.53± 1.28 µM/g dry and 56.15± 3.45 µM/g dry,
respectively n=3). These data confirm that the muscle strips were viable within the timeframe and experimental set-up of our experiment.
5.1.2 Human primary muscle cells (study III)
To confirm the formation of myotubes we analysed the expression of the muscle specific
transcription factor myogenin using immunocytochemistry. Moreover, we also assessed
the expression of desmin, a structural protein specific for muscle cells, and the expression
of myogenin using western blotting technique. Myogenin expression was transiently
55
increased with a maximum at 3 d and return to basal at 7 d (Fig 6A and Fig 6B). Desmin
expression increased gradually during the differentiation period, with the maximum
reached at day 7 (Figure 6 B). Thus, we chose to differentiate muscle cells for 7 days in
our studies.
Figure 5. ATP and PCr concentrations over time in isolated human muscle strips
(Skrobuk et al. unpublished). Muscle strips from 5 men were incubated in KHB for 0, 2
(n=1), or 6 h, and ATP and PCr concentrations were determined as described in the Methods
(4.11).
5.2 The effect of adiponectin on glucose transport in human
skeletal muscle (study I)
A decrease in circulating levels of adiponectin has been shown in insulin resistant states
such as obesity and type 2 diabetes (Hotta, Funahashi et al. 2000). Interestingly,
therapeutic approaches to improve insulin sensitivity, such as TZDs, are associated with
increased adiponectin concentrations (Yu, Javorschi et al. 2002). Exposure to the globular
head of adiponectin increases 2-deoxyglucose uptake in isolated EDL muscle from rat
(Tomas, Tsao et al. 2002). These data are in good agreement with our study. We observed
that globular adiponectin increased glucose transport by 1.3-fold in isolated skeletal
muscle strips from type 2 diabetic men. A similar effect of globular adiponectin has been
reported in skeletal muscle from lean and obese women. In the study by Bruce et al.
identical concentrations of insulin (120 nM) and globular adiponectin (2.5 µg/ml) to our
study were used (Bruce, Mertz et al. 2005). A combination of globular adiponectin and
insulin had an additive effect on glucose transport in skeletal muscle obtained from lean
56
and obese women. However, this effect was reduced in skeletal muscle from obese
subjects, suggesting existence of adiponectin resistance (Bruce, Mertz et al. 2005). We did
not detect any further changes in glucose transport in muscle strips exposed to globular
adiponectin and insulin, beyond that observed with insulin alone. Glucose transport may
Figure 6. Analysis of the muscle specific markers expressed in primary human
muscle cells during the differentiation period. A. Immunocytochemistry of the myogenin
expression. B. Representative western blot of myogenin and desmin expression.
already have been maximally stimulated in our subjects in response to pharmacological
insulin concentration (120 nM). On the other hand, exposure to AICAR enhanced insulin
action on glucose transport in skeletal muscle from type 2 diabetic men by 52 % and in
healthy men by 31 %, which is in good agreement with previous report where exposure to
AICAR improved insulin-stimulated glucose transport in type 2 diabetic skeletal muscle
(Koistinen, Galuska et al. 2003). Gender affects adiponectin concentrations, with higher
levels observed in women (Fernandez-Real, Lopez-Bermejo et al. 2003). We recruited
only men, whereas Bruce et al. studied women. Thus, the lack of insulin-sensitizing action
of globular adiponectin in our population may have been related to gender. Finally,
57
considering that only a 30 % increase in glucose transport was observed in our study and
by Bruce et al. (Bruce, Mertz et al. 2005), an acute elevation of adiponectin concentration
may play a minor role in the regulation of glucose metabolism in human skeletal muscle.
5.3 The effect of adiponectin on canonical insulin signaling
pathway (study I)
Adiponectin increases insulin-mediated activation of AKT via APPL1 in C2C12 cells
(Mao, Kikani et al. 2006). To explore the role of adiponectin in human skeletal muscle, we
tested if globular adiponectin stimulates phosphorylation of AKT at Ser
473
and Thr308.
Globular adiponectin did not affect AKT phosphorylation at either residue in either of our
study groups, which is in line with data from C2C12 cells (Mao, Kikani et al. 2006).
Insulin stimulation increased phosphorylation of AKT at Ser473 and Thr308 similarly in type
2 diabetic and nondiabetic muscle. Globular adiponectin did not have any further effect
on insulin-stimulated AKT phosphorylation. Our data are opposite to those reported in
C2C12 myotubes, where adiponectin had an additive effect on the insulin-stimulated
phosphorylation of AKT at Thr308. Taken together, adiponectin might have different
effects depending on the study model used. Our signaling data are in line with the glucose
transport results: adiponectin did not have any further effect on insulin action on glucose
metabolism. Considering the lack of adiponectin on AKT phosphorylation in the basal
state, globular adiponectin appears to stimulate glucose transport in type 2 diabetic muscle
via signaling pathways distinct from AKT.
5.4 The expression of adiponectin receptors in skeletal
muscle from type 2 diabetic and healthy men (study I)
Adiponectin receptors, AdipoR1 and R2, are both abundantly expressed in skeletal
muscle. AdipoR1 plays the main role in adiponectin action in skeletal muscle (Chen,
McAinch et al. 2005; Yamauchi, Nio et al. 2007). AdipoR1 mediates adiponectin
signaling via AMPK, whereas AdipoR2 signals via PPARα (Yamauchi, Nio et al. 2007).
Studies examining adiponectin receptor expression in human skeletal muscle are
controversial. mRNA expression for both adiponectin receptors has been reported to be
similar in obese type 2 diabetic and lean nondiabetic subjects in skeletal muscle (Debard,
Laville et al. 2004) or in cultured myotubes (Chen, McAinch et al. 2005). Blüher et al.
58
have reported higher skeletal muscle adiponectin receptor 1 and 2 mRNA expression in
obese type 2 diabetic and IGT subjects than lean normoglycaemic people (Bluher, Bullen
et al. 2006). In our study, we examined the protein expression of adiponectin receptors in
type 2 diabetic and non-diabetic muscle. The expression of AdipoR1 and AdipoR2 was
similar between both groups. Thus, changes in AdipoR expression do not account for
differences in metabolic responses to globular adiponectin between the two study groups.
5.5 The effect of adiponectin on AMPK signaling (study I)
Globular adiponectin activates the AMPK signaling pathway and stimulates glucose
uptake in C2C12 cells (Yamauchi, Kamon et al. 2002). In addition, effect of adiponectin
on AMPK activity was observed in human primary muscle cells (Chen, McAinch et al.
2005). Therefore, to identify a possible molecular mechanism of adiponectin action in
human skeletal muscle, we next analyzed the effect of globular adiponectin on
phosphorylation of AMPK. Phosphorylation of AMPK was unchanged after a 60 min
exposure to globular adiponectin in type 2 diabetic. In nondiabetic muscle AMPK
phosphorylation was slightly decreased following exposure to globular adiponectin.
AICAR increased phosphorylation of AMPK by 11 % in non-diabetic muscle, as
expected. Activation of AMPK in C2C12 myotubes was reported after 15 min incubation
with globular adiponectin (Yamauchi, Kamon et al. 2002). In rat skeletal mucle activation
of AMPK in response to globular adiponectin was transient and returned to basal after 60
min exposure to adiponectin (Tomas, Tsao et al. 2002). Thus, phosphorylation of AMPK
could possibly have occurred at an earlier time point in our study.
5.6 The effect of rosiglitazone on insulin action and glucose
transport in human skeletal muscle (study II)
Despite clinical safety concerns and withdrawal of rosiglitazone from the pharmaceutical
market, TZDs remain an excellent research tool to develop novel and improved
therapeutical strategies to treat insulin resistance. The molecular mechanisms whereby
TZDs improve insulin sensitivity are still incompletely understood. TZDs are high affinity
ligands for PPARγ, a transcription factor highly expressed in adipocytes and also to some
extent in other tissues such as skeletal muscle (Vidal-Puig, Considine et al. 1997).
However, the effects of TZDs on PPARγ and adipocytes do not exclude the possibility
59
that TZDs may also act via different signaling mechanisms in other tissues. Acute
exposure of rat EDL muscle to troglitazone increases 2-deoxyglucose uptake and
palmitate oxidation, as well as activates AMPK (LeBrasseur, Kelly et al. 2006). Since
chronic treatment with TZDs improves insulin action in humans (Tiikkainen, Hakkinen et
al. 2004; Skov, Glintborg et al. 2008), we examined whether TZDs had an acute effect
directly in intact human skeletal muscle. Exposure for 60 min to rosiglitazone did not
modify basal or insulin-stimulated glucose transport. Although we observed a tendency to
improve glucose transport rate in response to higher rosiglitazone concentration (10 µM),
this was not statistically significant (p = 0.182). Furthermore, we analysed if the clinical
characteristics of the study cohort would affect responses to rosiglitazone. Rosiglitazone
did not modify glucose transport in the absence or presence of abnormal glucose
metabolism, overweight or compromised physical fitness. We used 60 min exposure time
to study the effect of rosiglitazone on glucose transport. Thus, it cannot be excluded that a
longer incubation time would have been needed to see an effect in human skeletal muscle.
On the other hand, exposure of isolated mouse muscle for 5 h to a TZD does not modify
insulin-stimulated 2-deoxyglucose uptake (Zierath, Ryder et al. 1998). Moreover, our
study is in line with the lack of an acute stimulation of 3-O-methyl glucose transport by
troglitazone in L6GLUT4myc cell line (Konrad, Rudich et al. 2005). Interestingly, 2deoxyglucose uptake was increased in response to troglitazone due to stimulation of 2deoxyglucose phosphorylation in L6GLUT4myc myotubes, suggesting that metabolic flux
via hexokinase was increased (Konrad, Rudich et al. 2005). We used 3-O-methylglucose
in our study. Therefore, we could only measure the glucose transport step, because
hexokinase is not able to phosphorylate 3-O-methylglucose. In contrast, 2-deoxyglucose
uptake reflects both glucose transport and phosphorylation steps. Thus, we cannot exclude
that rosiglitazone might acutely stimulate glucose fluxes downstream of the glucose
transport step in human skeletal muscle. To study the effect of rosiglitazone on insulin
sensitivity we tested if exposure to rosiglitazone affected proximal insulin signaling
events. As reflected by unchanged basal or insulin-stimulated phosphorylation of AKT at
Ser 473 and Thr308, rosiglitazone did not affect insulin signaling events in our study.
60
5.7 The effect of rosiglitazone on the AMPK signaling
pathway (study II)
Emerging evidence suggests that one of the mechanisms whereby TZDs stimulate glucose
uptake and lipid metabolism is via the AMPK signaling cascade. TZDs have been shown
to activate AMPK in H-2Kb muscle cells (Fryer, Parbu-Patel et al. 2002) and
L6GLUT4myc myotubes (Konrad, Rudich et al. 2005). Moreover, a decrease in the
expression of AMPK using siRNA inhibits the stimulation of 2-deoxyglucose uptake by
troglitazone (Konrad, Rudich et al. 2005). Increased glucose uptake and palmitate
oxidation in response to TZDs was demonstrated in intact skeletal muscle from rat and it
coincided with rapid activation of AMPK (LeBrasseur, Kelly et al. 2006). We analyzed
whether rosiglitazone directly activates AMPK in intact human skeletal muscle. Exposure
to 10 µM rosiglitazone transiently increased ACC phosphorylation in nondiabetic muscle.
Phosphorylation reached a peak at 15 min (p = 0.051, n = 5), suggesting AMPK activation
by acute exposure to rosiglitazone. The time course results observed in our studies were
similar to rodent muscle, where a peak in AMPK activity and ACC phosphorylation
following exposure to 5 µM troglitazone occurs between 5 and 15 min, with a return to
baseline within 60 min (LeBrasseur, Kelly et al. 2006). Acute AMPK activation by
rosiglitazone did not coincide with stimulation of glucose transport in our study. However,
it is possible that rosiglitazone might acutely modify lipid metabolism via the AMPKACC signaling pathway in intact human skeletal muscle.
5.8 The effect of resveratol on glucose and fatty acid
metabolism in human skeletal muscle (study III)
The natural polyphenolic compound resveratrol has recently attracted considerable
scientific interest due to its antidiabetic properties. There is evidence for RSV to improve
insulin action and whole body glucose homeostasis in animal models (Lagouge, Argmann
et al. 2006; Um, Park et al. 2010). Treatment with RSV has also been linked with the
reduction of fat content and body weight in rodents (Su, Hung et al. 2006; Um, Park et al.
2010). However, the molecular mechanisms of RSV action on glucose and lipid
metabolism in human skeletal muscle have not been established. Therefore, we examined
the metabolic effects of RSV in human primary muscle cells. In the basal state, glucose
61
uptake was unaffected by the presence of 100 µM RSV. However, the insulin-stimulated
glucose uptake was decreased by 34 %. To further explore the effects of RSV on glucose
metabolism, we measured glucose incorporation into glycogen. Exposure to RSV
significantly reduced basal as well as insulin-stimulated glycogen synthesis. Our data were
surprising, because RSV stimulates glucose uptake in L6 muscle cells in a dose-dependent
fashion, with the maximum response seen at 100 µM (Breen, Sanli et al. 2008; Minakawa,
Kawano et al. 2011). Since our data differed from those obtained in L6 muscle cells, we
examined if the effects of 4h exposure to RSV are concentration- or species dependent. In
human myotubes, basal glucose uptake was increased with lower RSV concentrations (1
and 10 µM). Moreover, we observed an inhibition of basal and insulin- stimulated glucose
uptake by higher RSV concentrations (100-200 µM). We also performed dose-response
experiments using 0.1-100 µM RSV in L6 myotubes. RSV at 0.1-100 µM did not affect,
while 200 µM RSV inhibited basal glucose uptake. Similar to human myotubes there was
an inhibition of insulin-stimulated glucose uptake at 100-200 µM. The reason for different
findings between our study and studies by Breen et. al. or Minakawa et al. is unclear, but
cannot be explained by different concentrations of RSV or duration of RSV exposure.
Possible species differences may also be excluded, since we observed similar inhibitory
effect of higher doses of RSV on glucose uptake in both human and L6 myotubes. It is
worth noticing that lower concentrations of RSV enhanced basal glucose uptake in human
myotubes, while higher concentrations had the opposite effect. Thus, our data fit well with
the concept of hormesis, with lower concentrations of RSV having a positive and higher
ones a negative biological effect (Hawley, Burke et al. 2011).
RSV exerts beneficial effects such as weight reduction and reduced fat accumulation.
Moreover, RSV has been shown to increase mitochondrial biogenesis as well as physical
endurance in rodents (Lagouge, Argmann et al. 2006; Um, Park et al. 2010). These data
suggest that RSV impacts lipid metabolism. Thefore, we examinated if acute exposure to
RSV affects lipid metabolism in human skeletal muscle. First, we determined fatty acid
oxidation, using only a trace amount of radioactive palmitate in the media (without any
cold palmitate). Curiously, insulin increased palmitate oxidation. This most likely was
due to stimulatory effect of insulin on palmitate uptake (Bouzakri, Austin et al. 2008). As
expected, acute exposure of human myotubes to AICAR increased palmitate oxidation,
62
whereas presence of AMPK inhibitor compound C significantly decreased palmitate
oxidation. In the presence of resveratrol, palmitate oxidation was reduced by 40 %. We
also performed fatty acid oxidation experiments using physiological palmitate
concentration (0.2 mM). Also in this experimental set-up, acute exposure of human
muscle cells to RSV led to a decrease in palmitate oxidation. Taken together, our data on
both glucose and lipid metabolism suggest that RSV may act as a metabolic inhibitor in
human skeletal muscle cells.
5.9 The effect of RSV on insulin signaling (study III)
Resveratrol reversed palmitate-induced insulin resistance in C2C12 cells (Sun, Zhang et
al. 2007). Initially, we hypothesised that exposure to RSV could counteract palmitateinduced insulin resistance in human muscle cells. However, we observed an impairment in
glucose and lipid metabolism in the presence of RSV. To gain more insight into the
mechanisms of RSV action, we investigated if RSV affects insulin signaling. We observed
a decrease in insulin-stimulated phosphorylation of AKT, an effect sustained for 24 h.
These data were consistent with the negative effects of RSV on glucose uptake and
glycogen synthesis. The inhibitory effect of RSV on glucose uptake or insulin signaling
has previously been reported. RSV has been shown to be a direct inhibitor of class IA PI3kinase in primary human myotubes (Frojdo, Cozzone et al. 2007). RSV reduced insulinstimulated AKT Ser473 phosphorylation in rat L6 and human rhabdomyosarcoma CCL
muscle-derived cells in a dose-dependent fashion. Insulin-stimulated glucose uptake was
decreased by 82.7% also in 3T3-L1 adipocytes by 100 µM RSV (Frojdo, Cozzone et al.
2007). Dose-dependent inhibition of basal glucose uptake by RSV was reported in two
myelocytic cell lines, U937 and HL-60 cells. Finally, RSV was reported to act as an
inhibitor of insulin stimulated AKT phosphorylation in H4IIE cells (a rat hepatoma cell
line), HepG2 cells (a human hepatoma cell line) and primary rat hepatocytes (Zang, Xu et
al. 2006). Taken together, RSV inhibits glucose metabolism and insulin signaling in
several different cell models.
63
5.10 The inhibitory effect of RSV on AMPK signaling in
human myotubes (study III)
Several lines of evidence suggest activation of AMPK by RSV (Zang, Xu et al. 2006;
Frojdo, Cozzone et al. 2007; Breen, Sanli et al. 2008; Um, Park et al. 2010). Therefore, we
investigated if RSV activates the AMPK pathway in human primary muscle cells. Acute
exposure to 100 µM RSV reduced phosphorylation of AMPK and ACC, suggesting a
inhibition of AMPK signaling. The inhibitory effect of RSV on the AMPK signaling
cascade was maintained for 12 h with a return to basal levels by 24 h. The inhibition of
AMPK signaling is in line with the inhibitory effect of RSV on palmitate oxidation in our
study. We also have investigated the dose-dependent effect of RSV on AMPK signaling
in human myotubes and L6 cell line. We observed that RSV decreased AMPK
phosphorylation already at the concentration of 1 µM in human muscle cells.
Phosphorylation of ACCβ was not affected with the lower concentration of RSV, whereas
higher RSV concentrations (100-200 µM) reduced ACCβ phosphorylation in human
myotubes. Interestingly, RSV increased phosphorylation of ACCβ in L6 myotubes at all
concentrations used, suggesting some species differences in response to RSV. PGC-1α is
deacetylated and thus activated by Sirt1 (Lagouge, Argmann et al. 2006). Since Sirt1
activation by RSV requires AMPK activity (Um, Park et al. 2010), we also analysed PGC1α acetylation. Acute exposure to 1 µM RSV significantly increased acetylation of PGC1α in human primary myotubes. These data suggest reduction of SIRT1 activity by RSV.
Since Sirt1 resides downstream of AMPK, these data would support the idea that RSV
directly inhibits AMPK activity in human primary muscle cells. To confirm or refute this
hypothesis, we next investigated the direct effect of RSV on AMPK activity by
performing in vitro kinase assays. We used α1/β2/γ1 and α2/β2/γ1 isoforms, which are the
major complexes of AMPK in skeletal muscle (Wojtaszewski, Birk et al. 2005). RSV at
lower (1 µM) concentration blocked AMPK-α1 activity by 35% and AMPK-α2 activity
by 50% (n=2), whereas higher RSV concentration (100 µM) completely inhibited the
activity of both AMPK isoform complexes. In summary, our data suggest that acute
treatment with RSV inhibits AMPK activity in human skeletal muscle cells. Since 30-day
treatment with RSV results in increased phosphorylation of AMPK in human skeletal
muscle (Timmers, Konings et al. 2011), it is possible that resveratrol has different effects
64
depending on the duration of the exposure. However, it is also possible that increased
AMPK phosphorylation following 30-d peroral RSV treatment is a secondary
phenomenon.
5.11 The effect of acute exposure to RSV on ER stress
(study III)
We examined the effect of RSV on ER stress using eIF2α phosphorylation or CHOP
expression as readouts. Interestingly, we observed increased eIF2α phosphorylation and
CHOP expression after treatment with RSV in a dose-dependent manner. These data
suggest that RSV induces ER stress in muscle cells. RSV had a similar effect on eIF2α
phosphorylation and CHOP expression in L6 myotubes. Importantly, exposure to AICAR
decreased eIF2α phosphorylation in human myotubes, suggesting that AMPK activation
alleviates ER stress. This is combatible with previous data suggesting activation of AMPK
decreases ER stress (Hwang, Chang et al. 2010). Therefore, the effects of AICAR and
other AMPK activators on ER stress should be studied in more detail, as this may reveal
novel targets for developing pharmaceutical therapies to treat insulin resistance.
5.12 The effect of palmitate on glucose metabolism and
insulin signaling in isolated human skeletal muscle strips
(Unpublished data)
Acute exposure to palmitate induced insulin resistance and activated ER stress signaling in
human myotubes (Study III). Isolated skeletal muscle strip preparation resembles intact
skeletal muscle more closely than primary cultured myotubes for example in terms of
GLUT4 expression (Sarabia, Lam et al. 1992), and therefore the use of isolated skeletal
muscle strips is an important complementary research tool in studies on muscle
metabolism. To gain more insight into the interaction of palmitate and glucose
metabolism, we next investigated the acute effects of high physiological palmitate
concentration (1 mM) on glucose metabolism and insulin signaling in isolated human
skeletal muscle strips (Skrobuk et al. unpublished). First, we studied the effect of 4 h preexposure to palmitate on glucose transport and glycogen synthesis in intact skeletal
muscle strips. Insulin at pharmacological concentration of 120 nM is often used in studies
65
in isolated muscle strips to stimulate the system maximally (Koistinen, Galuska et al.
2003; Bruce, Mertz et al. 2005; Karlsson, Ahlsen et al. 2006). However, this concentration
is 200-400-fold higher than observed postprandially for example during oral glucose
tolerance test where maximal plasma insulin concentration varies 0.2 to 0.9 nM,
depending on the degree of the insulin resistance of the subject. Insulin at extremely high
concentrations might prevent detection of subtle impairments in insulin action following
experimental perturbations such as exposure of muscles to palmitate. Thefore, here we
chose to use high physiological insulin concentration (1.2 nM), which is close to ED50 (1
nM) of the insulin receptor in human skeletal muscle (Argyraki, Wright et al. 1989).
Muscle strips were obtained from 27 nondiabetic men (age 48±2, BMI 26±0.7, fasting
glucose 5.6±0.07). Insulin increased glucose transport 1.7-fold (from 0.87±1.1 to 1.4±0.17
nmol/mg/20 min, p<0.001). In muscle strips pre-exposed to palmitate for 4 h, basal
glucose transport rate was increased (1.0±0.11 nmol/mg/20 min), insulin-stimulated
glucose transport was unchanged (1.4±0.12), and insulin action on glucose transport
(insulin-stimulated minus basal) reduced by 35 % (p = 0.086).
Palmitate (2 mM) impairs insulin-stimulated glucose transport in isolated muscle strips
from obese women, whereas it was without a significant effect in lean women (Thrush,
Heigenhauser et al. 2008). Therefore, to investigate whether the effect of palmitate is
modified by body weight, we divided our subjects into 2 groups: lean (BMI <25 kg/m2)
and overweight (BMI>25 kg/m2). The negative effects of palmitate on glucose transport
were more apparent in skeletal muscle strips from overweight compared to lean men, and
appeared to involve an increase in basal glucose transport since insulin-stimulated glucose
transport was unaffected (Figure 7a, Skrobuk et al. unpublished). Thus, these data are
consistent with the previous report and suggest that overweight/obese muscle may be
more susceptible for the ability of palmitate to evoke significant impairments in glucose
transport (Thrush, Heigenhauser et al. 2008). Formation of ceramides might play an
important role in palmitate-induced insulin resistance. Thus, we tested if blocking SPT
with myriocin could protect muscles from lipid-induced insulin resistance. Co-incubation
with myriocin protected muscle from palmitate induced insulin resistance (Figure 7b,
Skrobuk et al. unpublished).
66
Figure 7. Glucose transport. a) Glucose transport by body weight was analysed in muscle
strips from 8 lean men and 12 overweight men using 3-O-methyl [3H] glucose. * p<0.05 vs
respective control. ^ p<0.05 vs respective condition in the lean group. Data are presented as
means±SEM (Skrobuk et al. unpublished). b) The effect of SPT inhibition on glucose
transport. Glucose transport was measured in the absence or presence of 1 mM palmitate or
myriocin (10µM) or 1.2 nM insulin. Data are expressed as delta (respective insulin
stimulated condition – respective control). Data are presented as means±SEM n = 6
(Skrobuk et al. Unpublished).
67
Our data are in line with animal studies, where myriocin-treated animals were protected
against saturated fatty acid-induced insulin resistance (Holland, Brozinick et al. 2007).
However, to confirm the role of ceramides in lipid-induced insulin resistance in human
skeletal muscle, a metabolomic study would be needed to be performed. Saturated fatty
acids decrease insulin-stimulated glycogen synthesis in vitro in rat and human muscle
(Thompson, Lim-Fraser et al. 2000). These data are in good agreement with our findings,
as we observed 18 % decrease in insulin-stimulated glucose incorporation into glycogen in
muscle strips pre-exposed to palmitate (Figure 8, Skrobuk et al. unpublished).
Collectively, these data indicate that palmitate induces insulin resistance and ceramides
might play an important role in this process.
Figure 8. Glycogen synthesis. Skeletal muscle strips from 9 nondiabetic men were
incubated with or w/o 1 mM palmitate and 1.2 nM insulin for 4 h. Glucose incorporation into
glycogen was measured as the amount of [14C]-glucose incorporated into glycogen during
one hour. ** p<0.01, * p<0.05 vs respective control (Skrobuk et al. unpublished).
Insulin-stimulated AKT-Ser473 phosphorylation is unaffected in lipid-induced insulin
resistance in in vivo human studies (Storgaard, Jensen et al. 2004). These data are in
accordance with our present findings: insulin-stimulated AKT at Ser473 phosphorylation
was not impaired following exposure to palmitate (Skrobuk et al. data not shown).
68
Palmitate exposure (2 mM) reduced insulin-stimulated phosphorylation of AS160 in intact
skeletal muscle from obese but not lean women (Thrush, Heigenhauser et al. 2008).
Similarly, we observed that phosphorylation of AS160 was unaffected by 1 mM palmitate
in lean muscles, whereas in muscles from overweight men, insulin action on AS160
phosphorylation was abolished by palmitate pre-exposure (Figure 9, Skrobuk et al
unpublished). Thus, our data provide evidence that overweight muscle is more suspectible
to defects in insulin signaling when challenged with fatty acids. Interestingly, our data
agree with observations on insulin signaling in T2D muscle, where AKT-Ser473
phosphorylation is normal, while AKT-Thr308 and AS160 phosphorylations are impaired
(Karlsson, Zierath et al. 2005). These data raise the possibility that impaired AS160
phosphorylations in T2D muscle may be secondary to increased circulating FFA levels
and/or increased muscle fat content.
Figure 9. AS160 phosphorylation. AS160 phosphorylation was determined at the end of
the glucose transport protocol in muscles strips from lean (n=5) and overweight men (n=10).
AS160 phosphorylation has been expressed in relation to total AS160. The representative
blot is from one gel. * p<0.05 vs respective control (Skrobuk et al. unpublished).
69
5.13 Palmitate and ER stress
Endoplasmic reticulum (ER) stress has recently emerged as a major player in insulin
resistance (Ozcan, Cao et al. 2004). Acute exposure of human myotubes to palmitate
induced ER stress (Study III). Thus, we examined if palmitate activates ER stress in intact
human skeletal muscle. The effect of palmitate on the PERK signaling arm of the UPR
was studied by determining phosphorylation of eIF2α (Harding, Zhang et al. 1999; Ma,
Brewer et al. 2002). In skeletal muscle strips from lean men, there was no change in the
phosphorylation of eIF2α in response to palmitate. However, when muscles from
overweight men were exposed to palmitate, the phosphorylation of eIF2α was
significantly increased (Figure 10, Skrobuk et al. unpublished). After 4 h exposure to
palmitate, there was also a marked increase in chaperon protein BiP/ GRP78 levels in
muscle strips from overweight, but not from lean men. These data provide evidence that
overweight human skeletal muscle is suspectible to ER stress in response to palmitate,
while lean muscle seems to be able to cope with palmitate excess and resolve ER stress.
JNK, which is activated via IRE1(Urano, Wang et al. 2000), phosphorylates IRS at
inhibitory serine residues and thus leads to defects in the insulin-signaling pathway(Sabio,
Kennedy et al. 2010). Therefore, in the future it will be interesting to test the link between
ER stress and insulin signaling pathway in human skeletal muscle.
70
Figure 10. Phosphorylation of eIF2α and GRP78/BiP expression. Skeletal muscle
strips from 5 lean and 10 overweight men were incubated with or without 1 mM palmitate
and phosphorylation of eIF2α and GRP78/BiP levels were measured at the end of the glucose
transport protocol. Representative blots are presented. For clarity, only basal and palmitate
stimulated data are quantified. * p<0.05 vs respective condition w/o palmitate (Skrobuk et
al. unpublished).
71
6 Summary
The results of the studies can be summarised as follows:
1. Acute exposure to globular adiponectin stimulates glucose transport in skeletal
muscle from type 2 diabetic men. This is related neither to insulin nor AMPK
signaling pathways.
2. Acute exposure to rosiglitazone does not affect glucose transport or insulin
signaling in human skeletal muscle. However, rosiglitazone transiently activates
AMPK signaling.
3. Palmitate impairs glucose metabolism and increases ER stress in isolated skeletal
muscle as well as in human primary muscle cells. Acute exposure to resveratrol
inhibits glucose and lipid metabolism, and directly inhibits AMPK activity in
human skeletal muscle cells. Resveratrol does not prevent palmitate-induced
insulin resistance. Exposure to resveratrol increases and exposure to AICAR
reduces ER stress, respectively.
72
7 Conclusions and future perspectives
Insulin resistance, particularly in skeletal muscle, is the hallmark of type 2 diabetes
mellitus. Therefore, it is important to understand at molecular level what are the
mechanisms and intracellular events that impair insulin signaling and eventually
metabolism, as this may identify novel therapeutical targets to improve insulin action.
Here, we observed a stimulatory effect of globular adiponectin on glucose transport in
type 2 diabetic muscle. However, the effect was modest and therefore skeletal muscle may
not be the primary target of the insulin-sensitizing effect of adiponectin. Similarly, acute
exposure to rosiglitazone, a TZD, failed to impact on glucose transport in human skeletal
muscle. These data support the notion that the primary target of TZDs is adipose tissue,
and the increase in insulin sensitivity in skeletal muscle and liver would be secondary to
improved adipocyte function.
The polyphenolic compound resveratrol acts acutely as a metabolic inhibitor in human
skeletal muscle. Therefore, any beneficial effects of resveratrol appear to be secondary,
and further human studies on the effects of resveratrol and its mechanisms of action are
warranted. Our results add AMPK among the many intracellular kinases that are directly
inhibited by resveratrol. Acetylation/deacetylation of proteins may play an important role
in the insulin signaling pathway (Pirola, Zerzaihi et al. 2012). Thus, this concept should be
tested
in
future
studies
using
compounds
like
resveratrol,
as
protein
acetylation/deacetylation might be a promising target to design new pharmacological
compounds to treat T2DM. Palmitate induces insulin resistance and ER stress both in
primary human myotubes as well as in intact human muscle strips. AICAR reduces ER
stress in human muscle cells. Therefore targeting ER stress via the AMPK pathway may
be beneficial in treating metabolic diseases. However, more experiments with AMPK
activators would be needed to confirm this concept. In addition, to clarify the involvement
of ER stress in insulin resistance in skeletal muscle and T2DM, experiments using ER
stress alleviating chemical chaperons such as 4-PBA and TUDCA should be tested to
combat excess nutrient or cytokine induced insulin resistance.
73
Acute exposure to palmitate impairs proximal insulin signaling and affects glucose
metabolism in skeletal muscle from overweight men. This is associated with sustained ER
stress. The negative effect of palmitate is also seen in human primary muscle cells. Thus,
more signaling experiments are called for to describe mechanism of palmitate-induced
insulin resistance in skeletal muscle, as various intracellular sensors, for example stress
kinases such as JNK and inhibitory IRS1-Ser312 phosphorylation may play a role. It is
interesting to note that in contrast to overweight muscle, lean muscle seems to be able to
cope with acute exposure to excess palmitate. Identification of the molecular mechanisms
behind this adaptation may provide clues to the pathogenesis of T2DM, as well as insulin
resistance induced by excess nutrients such as obesity.
74
8 References
Adams, J. M., 2nd, T. Pratipanawatr, et al. (2004). "Ceramide content is increased in
skeletal muscle from obese insulin-resistant humans." Diabetes 53(1): 25-31.
Adams, S. H., C. L. Hoppel, et al. (2009). "Plasma acylcarnitine profiles suggest
incomplete long-chain fatty acid beta-oxidation and altered tricarboxylic acid cycle
activity in type 2 diabetic African-American women." J Nutr 139(6): 1073-1081.
Aguirre, V., T. Uchida, et al. (2000). "The c-Jun NH(2)-terminal kinase promotes insulin
resistance during association with insulin receptor substrate-1 and phosphorylation
of Ser(307)." J Biol Chem 275(12): 9047-9054.
Ahren, B. (2001). "Reducing plasma free fatty acids by acipimox improves glucose
tolerance in high-fat fed mice." Acta Physiol Scand 171(2): 161-167.
Al-Khalili, L., K. Bouzakri, et al. (2006). "Signaling specificity of interleukin-6 action on
glucose and lipid metabolism in skeletal muscle." Mol Endocrinol 20(12): 33643375.
Al-Khalili, L., D. Kramer, et al. (2004). "Human skeletal muscle cell differentiation is
associated with changes in myogenic markers and enhanced insulin-mediated
MAPK and PKB phosphorylation." Acta Physiol Scand 180(4): 395-403.
Andreyev, A. Y., Y. E. Kushnareva, et al. (2005). "Mitochondrial metabolism of reactive
oxygen species." Biochemistry (Mosc) 70(2): 200-214.
Argyraki, M., P. D. Wright, et al. (1989). "In vitro study of human skeletal muscle strips:
effect of nonesterified fatty acid supply on glucose storage." Metabolism 38(12):
1183-1187.
Arita, Y., S. Kihara, et al. (1999). "Paradoxical decrease of an adipose-specific protein,
adiponectin, in obesity." Biochem Biophys Res Commun 257(1): 79-83.
Arkan, M. C., A. L. Hevener, et al. (2005). "IKK-beta links inflammation to obesityinduced insulin resistance." Nat Med 11(2): 191-198.
Avignon, A., K. Yamada, et al. (1996). "Chronic activation of protein kinase C in soleus
muscles and other tissues of insulin-resistant type II diabetic Goto-Kakizaki (GK),
obese/aged, and obese/Zucker rats. A mechanism for inhibiting glycogen
synthesis." Diabetes 45(10): 1396-1404.
Bai, L., Y. Wang, et al. (2007). "Dissecting multiple steps of GLUT4 trafficking and
identifying the sites of insulin action." Cell Metab 5(1): 47-57.
Bajaj, M., S. Suraamornkul, et al. (2005). "Effect of a sustained reduction in plasma free
fatty acid concentration on intramuscular long-chain fatty Acyl-CoAs and insulin
action in type 2 diabetic patients." Diabetes 54(11): 3148-3153.
Bandyopadhyay, G. K., J. G. Yu, et al. (2005). "Increased p85/55/50 expression and
decreased phosphotidylinositol 3-kinase activity in insulin-resistant human skeletal
muscle." Diabetes 54(8): 2351-2359.
Baumann, C. A., V. Ribon, et al. (2000). "CAP defines a second signalling pathway
required for insulin-stimulated glucose transport." Nature 407(6801): 202-207.
Bays, H. E., J. M. Gonzalez-Campoy, et al. (2008). "Pathogenic potential of adipose tissue
and metabolic consequences of adipocyte hypertrophy and increased visceral
adiposity." Expert Rev Cardiovasc Ther 6(3): 343-368.
Beeson, M., M. P. Sajan, et al. (2003). "Activation of protein kinase C-zeta by insulin and
phosphatidylinositol-3,4,5-(PO4)3 is defective in muscle in type 2 diabetes and
impaired glucose tolerance: amelioration by rosiglitazone and exercise." Diabetes
52(8): 1926-1934.
75
Berg, J. M., J. L. Tymoczko, et al. (2007). Biochemistry. New York, W. H. Freeman.
Bergeron, R., S. F. Previs, et al. (2001). "Effect of 5-aminoimidazole-4-carboxamide-1beta-D-ribofuranoside infusion on in vivo glucose and lipid metabolism in lean and
obese Zucker rats." Diabetes 50(5): 1076-1082.
Bertolotti, A., Y. Zhang, et al. (2000). "Dynamic interaction of BiP and ER stress
transducers in the unfolded-protein response." Nat Cell Biol 2(6): 326-332.
Bertram, A. and K. Ley (2011). "Protein kinase C isoforms in neutrophil adhesion and
activation." Arch Immunol Ther Exp (Warsz) 59(2): 79-87.
Bhatt, B. A., J. J. Dube, et al. (2006). "Diet-induced obesity and acute hyperlipidemia
reduce IkappaBalpha levels in rat skeletal muscle in a fiber-type dependent
manner." Am J Physiol Regul Integr Comp Physiol 290(1): R233-240.
Bikman, B. T. and S. A. Summers (2011). "Ceramides as modulators of cellular and
whole-body metabolism." J Clin Invest 121(11): 4222-4230.
Bjornholm, M., Y. Kawano, et al. (1997). "Insulin receptor substrate-1 phosphorylation
and phosphatidylinositol 3-kinase activity in skeletal muscle from NIDDM
subjects after in vivo insulin stimulation." Diabetes 46(3): 524-527.
Bjornholm, M. and J. R. Zierath (2005). "Insulin signal transduction in human skeletal
muscle: identifying the defects in Type II diabetes." Biochem Soc Trans 33(Pt 2):
354-357.
Blenis, J. (1993). "Signal transduction via the MAP kinases: proceed at your own RSK."
Proc Natl Acad Sci U S A 90(13): 5889-5892.
Bloch-Damti, A. and N. Bashan (2005). "Proposed mechanisms for the induction of
insulin resistance by oxidative stress." Antioxid Redox Signal 7(11-12): 15531567.
Bluher, M., J. W. Bullen, Jr., et al. (2006). "Circulating adiponectin and expression of
adiponectin receptors in human skeletal muscle: associations with metabolic
parameters and insulin resistance and regulation by physical training." J Clin
Endocrinol Metab 91(6): 2310-2316.
Boden, G. (2011). "Obesity, insulin resistance and free fatty acids." Curr Opin Endocrinol
Diabetes Obes 18(2): 139-143.
Bogardus, C., S. Lillioja, et al. (1984). "Correlation between muscle glycogen synthase
activity and in vivo insulin action in man." J Clin Invest 73(4): 1185-1190.
Bouzakri, K., R. Austin, et al. (2008). "Malonyl CoenzymeA decarboxylase regulates lipid
and glucose metabolism in human skeletal muscle." Diabetes 57(6): 1508-1516.
Bouzakri, K., H. A. Koistinen, et al. (2005). "Molecular mechanisms of skeletal muscle
insulin resistance in type 2 diabetes." Curr Diabetes Rev 1(2): 167-174.
Bouzakri, K., A. Zachrisson, et al. (2006). "siRNA-based gene silencing reveals
specialized roles of IRS-1/Akt2 and IRS-2/Akt1 in glucose and lipid metabolism in
human skeletal muscle." Cell Metab 4(1): 89-96.
Breen, D. M., T. Sanli, et al. (2008). "Stimulation of muscle cell glucose uptake by
resveratrol through sirtuins and AMPK." Biochem Biophys Res Commun 374(1):
117-122.
Brozinick, J. T., Jr., B. R. Roberts, et al. (2003). "Defective signaling through Akt-2 and 3 but not Akt-1 in insulin-resistant human skeletal muscle: potential role in insulin
resistance." Diabetes 52(4): 935-941.
Bruce, C. R., V. A. Mertz, et al. (2005). "The stimulatory effect of globular adiponectin on
insulin-stimulated glucose uptake and fatty acid oxidation is impaired in skeletal
muscle from obese subjects." Diabetes 54(11): 3154-3160.
Burant, C. F., S. Sreenan, et al. (1997). "Troglitazone action is independent of adipose
tissue." J Clin Invest 100(11): 2900-2908.
76
Cai, D., S. Dhe-Paganon, et al. (2003). "Two new substrates in insulin signaling,
IRS5/DOK4 and IRS6/DOK5." J Biol Chem 278(28): 25323-25330.
Cantley, L. C. (2002). "The phosphoinositide 3-kinase pathway." Science 296(5573):
1655-1657.
Canto, C. and J. Auwerx (2009). "PGC-1alpha, SIRT1 and AMPK, an energy sensing
network that controls energy expenditure." Curr Opin Lipidol 20(2): 98-105.
Canto, C., Z. Gerhart-Hines, et al. (2009). "AMPK regulates energy expenditure by
modulating NAD+ metabolism and SIRT1 activity." Nature 458(7241): 10561060.
Canto, C., L. Q. Jiang, et al. (2010). "Interdependence of AMPK and SIRT1 for metabolic
adaptation to fasting and exercise in skeletal muscle." Cell Metab 11(3): 213-219.
Ceddia, R. B., R. Somwar, et al. (2005). "Globular adiponectin increases GLUT4
translocation and glucose uptake but reduces glycogen synthesis in rat skeletal
muscle cells." Diabetologia 48(1): 132-139.
Cha, B. S., T. P. Ciaraldi, et al. (2005). "Impaired fatty acid metabolism in type 2 diabetic
skeletal muscle cells is reversed by PPARgamma agonists." Am J Physiol
Endocrinol Metab 289(1): E151-159.
Chalkley, S. M., M. Hettiarachchi, et al. (1998). "Five-hour fatty acid elevation increases
muscle lipids and impairs glycogen synthesis in the rat." Metabolism 47(9): 11211126.
Chen, M. B., A. J. McAinch, et al. (2005). "Impaired activation of AMP-kinase and fatty
acid oxidation by globular adiponectin in cultured human skeletal muscle of obese
type 2 diabetics." J Clin Endocrinol Metab 90(6): 3665-3672.
Chen, X., J. Shen, et al. (2002). "The luminal domain of ATF6 senses endoplasmic
reticulum (ER) stress and causes translocation of ATF6 from the ER to the Golgi."
J Biol Chem 277(15): 13045-13052.
Chiang, S. H., C. A. Baumann, et al. (2001). "Insulin-stimulated GLUT4 translocation
requires the CAP-dependent activation of TC10." Nature 410(6831): 944-948.
Chibalin, A. V., Y. Leng, et al. (2008). "Downregulation of diacylglycerol kinase delta
contributes to hyperglycemia-induced insulin resistance." Cell 132(3): 375-386.
Cline, G. W., K. F. Petersen, et al. (1999). "Impaired glucose transport as a cause of
decreased insulin-stimulated muscle glycogen synthesis in type 2 diabetes." N Engl
J Med 341(4): 240-246.
Cnop, M., F. Foufelle, et al. (2012). "Endoplasmic reticulum stress, obesity and diabetes."
Trends Mol Med 18(1): 59-68.
Considine, R. V., M. K. Sinha, et al. (1996). "Serum immunoreactive-leptin
concentrations in normal-weight and obese humans." N Engl J Med 334(5): 292295.
Consoli, A., N. Nurjhan, et al. (1990). "Mechanism of increased gluconeogenesis in
noninsulin-dependent diabetes mellitus. Role of alterations in systemic, hepatic,
and muscle lactate and alanine metabolism." J Clin Invest 86(6): 2038-2045.
Cozzone, D., S. Frojdo, et al. (2008). "Isoform-specific defects of insulin stimulation of
Akt/protein kinase B (PKB) in skeletal muscle cells from type 2 diabetic patients."
Diabetologia 51(3): 512-521.
Craparo, A., T. J. O'Neill, et al. (1995). "Non-SH2 domains within insulin receptor
substrate-1 and SHC mediate their phosphotyrosine-dependent interaction with the
NPEY motif of the insulin-like growth factor I receptor." J Biol Chem 270(26):
15639-15643.
Cross, D. A., D. R. Alessi, et al. (1995). "Inhibition of glycogen synthase kinase-3 by
insulin mediated by protein kinase B." Nature 378(6559): 785-789.
77
Cusi, K., K. Maezono, et al. (2000). "Insulin resistance differentially affects the PI 3kinase- and MAP kinase-mediated signaling in human muscle." J Clin Invest
105(3): 311-320.
Dean, D., J. R. Daugaard, et al. (2000). "Exercise diminishes the activity of acetyl-CoA
carboxylase in human muscle." Diabetes 49(8): 1295-1300.
Debard, C., M. Laville, et al. (2004). "Expression of key genes of fatty acid oxidation,
including adiponectin receptors, in skeletal muscle of Type 2 diabetic patients."
Diabetologia 47(5): 917-925.
Defronzo, R. A. (2009). "Banting Lecture. From the triumvirate to the ominous octet: a
new paradigm for the treatment of type 2 diabetes mellitus." Diabetes 58(4): 773795.
DeFronzo, R. A. and M. A. Abdul-Ghani (2011). "Preservation of beta-cell function: the
key to diabetes prevention." J Clin Endocrinol Metab 96(8): 2354-2366.
DeFronzo, R. A., E. Ferrannini, et al. (1989). "Fasting hyperglycemia in non-insulindependent diabetes mellitus: contributions of excessive hepatic glucose production
and impaired tissue glucose uptake." Metabolism 38(4): 387-395.
DeFronzo, R. A., E. Jacot, et al. (1981). "The effect of insulin on the disposal of
intravenous glucose. Results from indirect calorimetry and hepatic and femoral
venous catheterization." Diabetes 30(12): 1000-1007.
DeFronzo, R. A. and D. Tripathy (2009). "Skeletal muscle insulin resistance is the primary
defect in type 2 diabetes." Diabetes Care 32 Suppl 2: S157-163.
Deldicque, L., P. D. Cani, et al. (2010). "The unfolded protein response is activated in
skeletal muscle by high-fat feeding: potential role in the downregulation of protein
synthesis." Am J Physiol Endocrinol Metab 299(5): E695-705.
Deldicque, L., K. Van Proeyen, et al. (2011). "The unfolded protein response in human
skeletal muscle is not involved in the onset of glucose tolerance impairment
induced by a fat-rich diet." Eur J Appl Physiol 111(7): 1553-1558.
Dohm, G. L., E. B. Tapscott, et al. (1988). "An in vitro human muscle preparation suitable
for metabolic studies. Decreased insulin stimulation of glucose transport in muscle
from morbidly obese and diabetic subjects." J Clin Invest 82(2): 486-494.
Downward, J. (1996). "Control of ras activation." Cancer Surv 27: 87-100.
Dyck, D. J., G. J. Heigenhauser, et al. (2006). "The role of adipokines as regulators of
skeletal muscle fatty acid metabolism and insulin sensitivity." Acta Physiol (Oxf)
186(1): 5-16.
Eguez, L., A. Lee, et al. (2005). "Full intracellular retention of GLUT4 requires AS160
Rab GTPase activating protein." Cell Metab 2(4): 263-272.
Ellis, B. A., A. Poynten, et al. (2000). "Long-chain acyl-CoA esters as indicators of lipid
metabolism and insulin sensitivity in rat and human muscle." Am J Physiol
Endocrinol Metab 279(3): E554-560.
Engelman, J. A., J. Luo, et al. (2006). "The evolution of phosphatidylinositol 3-kinases as
regulators of growth and metabolism." Nat Rev Genet 7(8): 606-619.
Etgen, G. J., K. M. Valasek, et al. (1999). "In vivo adenoviral delivery of recombinant
human protein kinase C-zeta stimulates glucose transport activity in rat skeletal
muscle." J Biol Chem 274(32): 22139-22142.
Fabbrini, E., S. Sullivan, et al. (2010). "Obesity and nonalcoholic fatty liver disease:
biochemical, metabolic, and clinical implications." Hepatology 51(2): 679-689.
Farese, R. V., M. P. Sajan, et al. (2007). "Muscle-specific knockout of PKC-lambda
impairs glucose transport and induces metabolic and diabetic syndromes." J Clin
Invest 117(8): 2289-2301.
78
Fernandez-Real, J. M., A. Lopez-Bermejo, et al. (2003). "Novel interactions of
adiponectin with the endocrine system and inflammatory parameters." J Clin
Endocrinol Metab 88(6): 2714-2718.
Ferrannini, E., D. C. Simonson, et al. (1988). "The disposal of an oral glucose load in
patients with non-insulin-dependent diabetes." Metabolism 37(1): 79-85.
Flamment, M., H. L. Kammoun, et al. (2010). "Endoplasmic reticulum stress: a new actor
in the development of hepatic steatosis." Curr Opin Lipidol 21(3): 239-246.
Foran, P. G., L. M. Fletcher, et al. (1999). "Protein kinase B stimulates the translocation of
GLUT4 but not GLUT1 or transferrin receptors in 3T3-L1 adipocytes by a
pathway involving SNAP-23, synaptobrevin-2, and/or cellubrevin." J Biol Chem
274(40): 28087-28095.
Frojdo, S., D. Cozzone, et al. (2007). "Resveratrol is a class IA phosphoinositide 3-kinase
inhibitor." Biochem J 406(3): 511-518.
Frojdo, S., H. Vidal, et al. (2009). "Alterations of insulin signaling in type 2 diabetes: a
review of the current evidence from humans." Biochim Biophys Acta 1792(2): 8392.
Fryer, L. G., F. Foufelle, et al. (2002). "Characterization of the role of the AMP-activated
protein kinase in the stimulation of glucose transport in skeletal muscle cells."
Biochem J 363(Pt 1): 167-174.
Fryer, L. G., A. Parbu-Patel, et al. (2002). "The Anti-diabetic drugs rosiglitazone and
metformin stimulate AMP-activated protein kinase through distinct signaling
pathways." J Biol Chem 277(28): 25226-25232.
Gao, Z., D. Hwang, et al. (2002). "Serine phosphorylation of insulin receptor substrate 1
by inhibitor kappa B kinase complex." J Biol Chem 277(50): 48115-48121.
Gao, Z., A. Zuberi, et al. (2003). "Aspirin inhibits serine phosphorylation of insulin
receptor substrate 1 in tumor necrosis factor-treated cells through targeting
multiple serine kinases." J Biol Chem 278(27): 24944-24950.
Gaster, M., I. Petersen, et al. (2002). "The diabetic phenotype is conserved in myotubes
established from diabetic subjects: evidence for primary defects in glucose
transport and glycogen synthase activity." Diabetes 51(4): 921-927.
Glund, S., A. Deshmukh, et al. (2007). "Interleukin-6 directly increases glucose
metabolism in resting human skeletal muscle." Diabetes 56(6): 1630-1637.
Goodyear, L. J., F. Giorgino, et al. (1995). "Insulin receptor phosphorylation, insulin
receptor substrate-1 phosphorylation, and phosphatidylinositol 3-kinase activity
are decreased in intact skeletal muscle strips from obese subjects." J Clin Invest
95(5): 2195-2204.
Goossens, G. H. (2008). "The role of adipose tissue dysfunction in the pathogenesis of
obesity-related insulin resistance." Physiol Behav 94(2): 206-218.
Grimes, C. A. and R. S. Jope (2001). "The multifaceted roles of glycogen synthase kinase
3beta in cellular signaling." Prog Neurobiol 65(4): 391-426.
Groop, L. C., R. C. Bonadonna, et al. (1989). "Glucose and free fatty acid metabolism in
non-insulin-dependent diabetes mellitus. Evidence for multiple sites of insulin
resistance." J Clin Invest 84(1): 205-213.
Gustafson, T. A., W. He, et al. (1995). "Phosphotyrosine-dependent interaction of SHC
and insulin receptor substrate 1 with the NPEY motif of the insulin receptor via a
novel non-SH2 domain." Mol Cell Biol 15(5): 2500-2508.
Hage Hassan, R., I. Hainault, et al. (2012). "Endoplasmic reticulum stress does not
mediate palmitate-induced insulin resistance in mouse and human muscle cells."
Diabetologia 55(1): 204-214.
Hajduch, E., D. R. Alessi, et al. (1998). "Constitutive activation of protein kinase B alpha
by membrane targeting promotes glucose and system A amino acid transport,
79
protein synthesis, and inactivation of glycogen synthase kinase 3 in L6 muscle
cells." Diabetes 47(7): 1006-1013.
Hajduch, E., A. Balendran, et al. (2001). "Ceramide impairs the insulin-dependent
membrane recruitment of protein kinase B leading to a loss in downstream
signalling in L6 skeletal muscle cells." Diabetologia 44(2): 173-183.
Hajduch, E., G. J. Litherland, et al. (2001). "Protein kinase B (PKB/Akt)--a key regulator
of glucose transport?" FEBS Lett 492(3): 199-203.
Hardie, D. G. (2011). "Energy sensing by the AMP-activated protein kinase and its effects
on muscle metabolism." Proc Nutr Soc 70(1): 92-99.
Harding, H. P., Y. Zhang, et al. (1999). "Protein translation and folding are coupled by an
endoplasmic-reticulum-resident kinase." Nature 397(6716): 271-274.
Hawley, J. A., L. M. Burke, et al. (2011). "Nutritional modulation of training-induced
skeletal muscle adaptations." J Appl Physiol 110(3): 834-845.
Hawley, S. A., D. A. Pan, et al. (2005). "Calmodulin-dependent protein kinase kinase-beta
is an alternative upstream kinase for AMP-activated protein kinase." Cell Metab
2(1): 9-19.
Hayashi, T., M. F. Hirshman, et al. (1998). "Evidence for 5' AMP-activated protein kinase
mediation of the effect of muscle contraction on glucose transport." Diabetes
47(8): 1369-1373.
Henry, R. R., P. Wallace, et al. (1986). "Effects of weight loss on mechanisms of
hyperglycemia in obese non-insulin-dependent diabetes mellitus." Diabetes 35(9):
990-998.
Heydrick, S. J., N. B. Ruderman, et al. (1991). "Enhanced stimulation of diacylglycerol
and lipid synthesis by insulin in denervated muscle. Altered protein kinase C
activity and possible link to insulin resistance." Diabetes 40(12): 1707-1711.
Heymsfield, S. B., A. S. Greenberg, et al. (1999). "Recombinant leptin for weight loss in
obese and lean adults: a randomized, controlled, dose-escalation trial." JAMA
282(16): 1568-1575.
Hirosumi, J., G. Tuncman, et al. (2002). "A central role for JNK in obesity and insulin
resistance." Nature 420(6913): 333-336.
Holgado-Madruga, M., D. R. Emlet, et al. (1996). "A Grb2-associated docking protein in
EGF- and insulin-receptor signalling." Nature 379(6565): 560-564.
Holland, W. L., B. T. Bikman, et al. (2011). "Lipid-induced insulin resistance mediated by
the proinflammatory receptor TLR4 requires saturated fatty acid-induced ceramide
biosynthesis in mice." J Clin Invest 121(5): 1858-1870.
Holland, W. L., J. T. Brozinick, et al. (2007). "Inhibition of ceramide synthesis
ameliorates glucocorticoid-, saturated-fat-, and obesity-induced insulin resistance."
Cell Metab 5(3): 167-179.
Holland, W. L., T. A. Knotts, et al. (2007). "Lipid mediators of insulin resistance." Nutr
Rev 65(6 Pt 2): S39-46.
Hommelberg, P. P., J. Plat, et al. (2011). "Palmitate-induced skeletal muscle insulin
resistance does not require NF-kappaB activation." Cell Mol Life Sci 68(7): 12151225.
Hotamisligil, G. S. (2006). "Inflammation and metabolic disorders." Nature 444(7121):
860-867.
Hotamisligil, G. S. (2010). "Endoplasmic reticulum stress and the inflammatory basis of
metabolic disease." Cell 140(6): 900-917.
Hotta, K., T. Funahashi, et al. (2000). "Plasma concentrations of a novel, adipose-specific
protein, adiponectin, in type 2 diabetic patients." Arterioscler Thromb Vasc Biol
20(6): 1595-1599.
80
Hotta, K., T. Funahashi, et al. (2001). "Circulating concentrations of the adipocyte protein
adiponectin are decreased in parallel with reduced insulin sensitivity during the
progression to type 2 diabetes in rhesus monkeys." Diabetes 50(5): 1126-1133.
Howitz, K. T., K. J. Bitterman, et al. (2003). "Small molecule activators of sirtuins extend
Saccharomyces cerevisiae lifespan." Nature 425(6954): 191-196.
Hu, E., P. Liang, et al. (1996). "AdipoQ is a novel adipose-specific gene dysregulated in
obesity." J Biol Chem 271(18): 10697-10703.
Hudson, E. R., D. A. Pan, et al. (2003). "A novel domain in AMP-activated protein kinase
causes glycogen storage bodies similar to those seen in hereditary cardiac
arrhythmias." Curr Biol 13(10): 861-866.
Hurley, R. L., K. A. Anderson, et al. (2005). "The Ca2+/calmodulin-dependent protein
kinase kinases are AMP-activated protein kinase kinases." J Biol Chem 280(32):
29060-29066.
Hwang, S. L., H. W. Chang, et al. (2010). "Ascofuranone prevents ER stress-induced
insulin resistance via activation of AMP-activated protein kinase in L6 myotube
cells." Biochem Biophys Res Commun 396(4): 967-972.
Idris, I., S. Gray, et al. (2001). "Protein kinase C activation: isozyme-specific effects on
metabolism and cardiovascular complications in diabetes." Diabetologia 44(6):
659-673.
Ikeda, Y., G. S. Olsen, et al. (2001). "Cellular mechanism of nutritionally induced insulin
resistance in Psammomys obesus: overexpression of protein kinase Cepsilon in
skeletal muscle precedes the onset of hyperinsulinemia and hyperglycemia."
Diabetes 50(3): 584-592.
Itani, S. I., N. B. Ruderman, et al. (2002). "Lipid-induced insulin resistance in human
muscle is associated with changes in diacylglycerol, protein kinase C, and
IkappaB-alpha." Diabetes 51(7): 2005-2011.
Jager, S., C. Handschin, et al. (2007). "AMP-activated protein kinase (AMPK) action in
skeletal muscle via direct phosphorylation of PGC-1alpha." Proc Natl Acad Sci U
S A 104(29): 12017-12022.
Jorgensen, S. B., J. N. Nielsen, et al. (2004). "The alpha2-5'AMP-activated protein kinase
is a site 2 glycogen synthase kinase in skeletal muscle and is responsive to glucose
loading." Diabetes 53(12): 3074-3081.
Karlsson, H. K., M. Ahlsen, et al. (2006). "Insulin signaling and glucose transport in
skeletal muscle from first-degree relatives of type 2 diabetic patients." Diabetes
55(5): 1283-1288.
Karlsson, H. K., J. R. Zierath, et al. (2005). "Insulin-stimulated phosphorylation of the Akt
substrate AS160 is impaired in skeletal muscle of type 2 diabetic subjects."
Diabetes 54(6): 1692-1697.
Kars, M., L. Yang, et al. (2010). "Tauroursodeoxycholic Acid may improve liver and
muscle but not adipose tissue insulin sensitivity in obese men and women."
Diabetes 59(8): 1899-1905.
Kim, H. J., C. Jamart, et al. (2011). "Endoplasmic reticulum stress markers and ubiquitinproteasome pathway activity in response to a 200-km run." Med Sci Sports Exerc
43(1): 18-25.
Kim, J. K., J. J. Fillmore, et al. (2004). "PKC-theta knockout mice are protected from fatinduced insulin resistance." J Clin Invest 114(6): 823-827.
Kim, J. K., Y. J. Kim, et al. (2001). "Prevention of fat-induced insulin resistance by
salicylate." J Clin Invest 108(3): 437-446.
Kim, S. C., R. Sprung, et al. (2006). "Substrate and functional diversity of lysine
acetylation revealed by a proteomics survey." Mol Cell 23(4): 607-618.
81
Kim, S. K. and R. F. Novak (2007). "The role of intracellular signaling in insulinmediated regulation of drug metabolizing enzyme gene and protein expression."
Pharmacol Ther 113(1): 88-120.
Kim, Y. B., K. Kotani, et al. (2003). "Insulin-stimulated protein kinase C lambda/zeta
activity is reduced in skeletal muscle of humans with obesity and type 2 diabetes:
reversal with weight reduction." Diabetes 52(8): 1935-1942.
Kim, Y. B., S. E. Nikoulina, et al. (1999). "Normal insulin-dependent activation of
Akt/protein kinase B, with diminished activation of phosphoinositide 3-kinase, in
muscle in type 2 diabetes." J Clin Invest 104(6): 733-741.
Kitabchi, A. E., M. Temprosa, et al. (2005). "Role of insulin secretion and sensitivity in
the evolution of type 2 diabetes in the diabetes prevention program: effects of
lifestyle intervention and metformin." Diabetes 54(8): 2404-2414.
Koh, H. J., J. Brandauer, et al. (2008). "LKB1 and AMPK and the regulation of skeletal
muscle metabolism." Curr Opin Clin Nutr Metab Care 11(3): 227-232.
Kohn, A. D., S. A. Summers, et al. (1996). "Expression of a constitutively active Akt
Ser/Thr kinase in 3T3-L1 adipocytes stimulates glucose uptake and glucose
transporter 4 translocation." J Biol Chem 271(49): 31372-31378.
Koistinen, H. A., D. Galuska, et al. (2003). "5-amino-imidazole carboxamide riboside
increases glucose transport and cell-surface GLUT4 content in skeletal muscle
from subjects with type 2 diabetes." Diabetes 52(5): 1066-1072.
Koivisto, V. A., H. Yki-Jarvinen, et al. (1986). "Physical training and insulin sensitivity."
Diabetes Metab Rev 1(4): 445-481.
Konishi, H., S. Kuroda, et al. (1995). "Molecular cloning and characterization of a new
member of the RAC protein kinase family: association of the pleckstrin homology
domain of three types of RAC protein kinase with protein kinase C subspecies and
beta gamma subunits of G proteins." Biochem Biophys Res Commun 216(2): 526534.
Konrad, D., A. Rudich, et al. (2005). "Troglitazone causes acute mitochondrial membrane
depolarisation and an AMPK-mediated increase in glucose phosphorylation in
muscle cells." Diabetologia 48(5): 954-966.
Kotani, K., W. Ogawa, et al. (1998). "Requirement of atypical protein kinase clambda for
insulin stimulation of glucose uptake but not for Akt activation in 3T3-L1
adipocytes." Mol Cell Biol 18(12): 6971-6982.
Koves, T. R., J. R. Ussher, et al. (2008). "Mitochondrial overload and incomplete fatty
acid oxidation contribute to skeletal muscle insulin resistance." Cell Metab 7(1):
45-56.
Kraegen, E. W. and G. J. Cooney (2008). "Free fatty acids and skeletal muscle insulin
resistance." Curr Opin Lipidol 19(3): 235-241.
Krook, A., M. Bjornholm, et al. (2000). "Characterization of signal transduction and
glucose transport in skeletal muscle from type 2 diabetic patients." Diabetes 49(2):
284-292.
Krook, A., R. A. Roth, et al. (1998). "Insulin-stimulated Akt kinase activity is reduced in
skeletal muscle from NIDDM subjects." Diabetes 47(8): 1281-1286.
Kurth-Kraczek, E. J., M. F. Hirshman, et al. (1999). "5' AMP-activated protein kinase
activation causes GLUT4 translocation in skeletal muscle." Diabetes 48(8): 16671671.
Lagouge, M., C. Argmann, et al. (2006). "Resveratrol improves mitochondrial function
and protects against metabolic disease by activating SIRT1 and PGC-1alpha." Cell
127(6): 1109-1122.
82
LeBrasseur, N. K., M. Kelly, et al. (2006). "Thiazolidinediones can rapidly activate AMPactivated protein kinase in mammalian tissues." Am J Physiol Endocrinol Metab
291(1): E175-181.
Lee, A. H., N. N. Iwakoshi, et al. (2003). "XBP-1 regulates a subset of endoplasmic
reticulum resident chaperone genes in the unfolded protein response." Mol Cell
Biol 23(21): 7448-7459.
Lowery, O. H. a. P., J.V., Ed. (1972). A flexible system of enzymatic analysis. Academic
Press. New York USA.
Lund, S., G. D. Holman, et al. (1995). "Contraction stimulates translocation of glucose
transporter GLUT4 in skeletal muscle through a mechanism distinct from that of
insulin." Proc Natl Acad Sci U S A 92(13): 5817-5821.
Ma, Y., J. W. Brewer, et al. (2002). "Two distinct stress signaling pathways converge
upon the CHOP promoter during the mammalian unfolded protein response." J
Mol Biol 318(5): 1351-1365.
Maegawa, H., Y. Shigeta, et al. (1991). "Impaired autophosphorylation of insulin
receptors from abdominal skeletal muscles in nonobese subjects with NIDDM."
Diabetes 40(7): 815-819.
Maffei, M., J. Halaas, et al. (1995). "Leptin levels in human and rodent: measurement of
plasma leptin and ob RNA in obese and weight-reduced subjects." Nat Med 1(11):
1155-1161.
Magnusson, I., D. L. Rothman, et al. (1992). "Increased rate of gluconeogenesis in type II
diabetes mellitus. A 13C nuclear magnetic resonance study." J Clin Invest 90(4):
1323-1327.
Mao, X., C. K. Kikani, et al. (2006). "APPL1 binds to adiponectin receptors and mediates
adiponectin signalling and function." Nat Cell Biol 8(5): 516-523.
McBride, A., S. Ghilagaber, et al. (2009). "The glycogen-binding domain on the AMPK
beta subunit allows the kinase to act as a glycogen sensor." Cell Metab 9(1): 23-34.
McGarry, J. D. (1992). "What if Minkowski had been ageusic? An alternative angle on
diabetes." Science 258(5083): 766-770.
Meyer, M. M., K. Levin, et al. (2002). "Insulin signalling in skeletal muscle of subjects
with or without Type II-diabetes and first degree relatives of patients with the
disease." Diabetologia 45(6): 813-822.
Minakawa, M., A. Kawano, et al. (2011). "Hypoglycemic effect of resveratrol in type 2
diabetic model db/db mice and its actions in cultured L6 myotubes and RIN-5F
pancreatic beta-cells." J Clin Biochem Nutr 48(3): 237-244.
Mingrone, G. (2004). "Carnitine in type 2 diabetes." Ann N Y Acad Sci 1033: 99-107.
Minokoshi, Y., Y. B. Kim, et al. (2002). "Leptin stimulates fatty-acid oxidation by
activating AMP-activated protein kinase." Nature 415(6869): 339-343.
Moder, M., A. Kiessling, et al. (2003). "The pattern of urinary acylcarnitines determined
by electrospray mass spectrometry: a new tool in the diagnosis of diabetes
mellitus." Anal Bioanal Chem 375(2): 200-210.
Momcilovic, M., S. P. Hong, et al. (2006). "Mammalian TAK1 activates Snf1 protein
kinase in yeast and phosphorylates AMP-activated protein kinase in vitro." J Biol
Chem 281(35): 25336-25343.
Morino, K., K. F. Petersen, et al. (2012). "Regulation of mitochondrial biogenesis by
lipoprotein lipase in muscle of insulin-resistant offspring of parents with type 2
diabetes." Diabetes 61(4): 877-887.
Mullen, K. L., J. Pritchard, et al. (2009). "Adiponectin resistance precedes the
accumulation of skeletal muscle lipids and insulin resistance in high-fat-fed rats."
Am J Physiol Regul Integr Comp Physiol 296(2): R243-251.
83
Muoio, D. M. and T. R. Koves (2007). "Skeletal muscle adaptation to fatty acid depends
on coordinated actions of the PPARs and PGC1 alpha: implications for metabolic
disease." Appl Physiol Nutr Metab 32(5): 874-883.
Musi, N., M. F. Hirshman, et al. (2002). "Metformin increases AMP-activated protein
kinase activity in skeletal muscle of subjects with type 2 diabetes." Diabetes 51(7):
2074-2081.
Nguyen, M. T., S. Favelyukis, et al. (2007). "A subpopulation of macrophages infiltrates
hypertrophic adipose tissue and is activated by free fatty acids via Toll-like
receptors 2 and 4 and JNK-dependent pathways." J Biol Chem 282(48): 3527935292.
Nolan, J. J., G. Freidenberg, et al. (1994). "Role of human skeletal muscle insulin receptor
kinase in the in vivo insulin resistance of noninsulin-dependent diabetes mellitus
and obesity." J Clin Endocrinol Metab 78(2): 471-477.
Norris, A. W., L. Chen, et al. (2003). "Muscle-specific PPARgamma-deficient mice
develop increased adiposity and insulin resistance but respond to
thiazolidinediones." J Clin Invest 112(4): 608-618.
Olefsky, J. M. and C. K. Glass (2010). "Macrophages, inflammation, and insulin
resistance." Annu Rev Physiol 72: 219-246.
Opie, L. H. and P. G. Walfish (1963). "Plasma free fatty acid concentrations in obesity." N
Engl J Med 268: 757-760.
Ozcan, U., Q. Cao, et al. (2004). "Endoplasmic reticulum stress links obesity, insulin
action, and type 2 diabetes." Science 306(5695): 457-461.
Park, S. W., Y. Zhou, et al. (2010). "The regulatory subunits of PI3K, p85alpha and
p85beta, interact with XBP-1 and increase its nuclear translocation." Nat Med
16(4): 429-437.
Peng, G., L. Li, et al. (2011). "Oleate blocks palmitate-induced abnormal lipid
distribution, endoplasmic reticulum expansion and stress, and insulin resistance in
skeletal muscle." Endocrinology 152(6): 2206-2218.
Peter, A., C. Weigert, et al. (2009). "Individual stearoyl-coa desaturase 1 expression
modulates endoplasmic reticulum stress and inflammation in human myotubes and
is associated with skeletal muscle lipid storage and insulin sensitivity in vivo."
Diabetes 58(8): 1757-1765.
Petersen, K. F., S. Dufour, et al. (2007). "The role of skeletal muscle insulin resistance in
the pathogenesis of the metabolic syndrome." Proc Natl Acad Sci U S A 104(31):
12587-12594.
Pirola, L., O. Zerzaihi, et al. (2012). "Protein acetylation mechanisms in the regulation of
insulin and insulin-like growth factor 1 signalling." Mol Cell Endocrinol.
Plomgaard, P., K. Bouzakri, et al. (2005). "Tumor necrosis factor-alpha induces skeletal
muscle insulin resistance in healthy human subjects via inhibition of Akt substrate
160 phosphorylation." Diabetes 54(10): 2939-2945.
Pold, R., L. S. Jensen, et al. (2005). "Long-term AICAR administration and exercise
prevents diabetes in ZDF rats." Diabetes 54(4): 928-934.
Polekhina, G., A. Gupta, et al. (2003). "AMPK beta subunit targets metabolic stress
sensing to glycogen." Curr Biol 13(10): 867-871.
Quinn, C. E., P. K. Hamilton, et al. (2008). "Thiazolidinediones: effects on insulin
resistance and the cardiovascular system." Br J Pharmacol 153(4): 636-645.
Qvigstad, E., I. L. Mostad, et al. (2003). "Acute lowering of circulating fatty acids
improves insulin secretion in a subset of type 2 diabetes subjects." Am J Physiol
Endocrinol Metab 284(1): E129-137.
84
Rabol, R., K. F. Petersen, et al. (2011). "Reversal of muscle insulin resistance with
exercise reduces postprandial hepatic de novo lipogenesis in insulin resistant
individuals." Proc Natl Acad Sci U S A 108(33): 13705-13709.
Raciti, G. A., C. Iadicicco, et al. (2010). "Glucosamine-induced endoplasmic reticulum
stress affects GLUT4 expression via activating transcription factor 6 in rat and
human skeletal muscle cells." Diabetologia 53(5): 955-965.
Ragheb, R., G. M. Shanab, et al. (2009). "Free fatty acid-induced muscle insulin resistance
and glucose uptake dysfunction: evidence for PKC activation and oxidative stressactivated signaling pathways." Biochem Biophys Res Commun 389(2): 211-216.
Rameh, L. E. and L. C. Cantley (1999). "The role of phosphoinositide 3-kinase lipid
products in cell function." J Biol Chem 274(13): 8347-8350.
Randle, P. J., P. B. Garland, et al. (1963). "The glucose fatty-acid cycle. Its role in insulin
sensitivity and the metabolic disturbances of diabetes mellitus." Lancet 1(7285):
785-789.
Rieusset, J., M. A. Chauvin, et al. (2012). "Reduction of endoplasmic reticulum stress
using chemical chaperones or Grp78 overexpression does not protect muscle cells
from palmitate-induced insulin resistance." Biochem Biophys Res Commun
417(1): 439-445.
Rohl, M., M. Pasparakis, et al. (2004). "Conditional disruption of IkappaB kinase 2 fails to
prevent obesity-induced insulin resistance." J Clin Invest 113(3): 474-481.
Ron, D. and P. Walter (2007). "Signal integration in the endoplasmic reticulum unfolded
protein response." Nat Rev Mol Cell Biol 8(7): 519-529.
Ryder, J. W., J. Yang, et al. (2000). "Use of a novel impermeable biotinylated
photolabeling reagent to assess insulin- and hypoxia-stimulated cell surface
GLUT4 content in skeletal muscle from type 2 diabetic patients." Diabetes 49(4):
647-654.
Ryo, M., T. Nakamura, et al. (2004). "Adiponectin as a biomarker of the metabolic
syndrome." Circ J 68(11): 975-981.
Sabio, G., N. J. Kennedy, et al. (2010). "Role of muscle c-Jun NH2-terminal kinase 1 in
obesity-induced insulin resistance." Mol Cell Biol 30(1): 106-115.
Saha, A. K., A. J. Schwarsin, et al. (2000). "Activation of malonyl-CoA decarboxylase in
rat skeletal muscle by contraction and the AMP-activated protein kinase activator
5-aminoimidazole-4-carboxamide-1-beta -D-ribofuranoside." J Biol Chem
275(32): 24279-24283.
Salehzadeh, F., A. Rune, et al. (2011). "Testosterone or 17{beta}-estradiol exposure
reveals sex-specific effects on glucose and lipid metabolism in human myotubes."
J Endocrinol 210(2): 219-229.
Saltiel, A. R. and J. E. Pessin (2002). "Insulin signaling pathways in time and space."
Trends Cell Biol 12(2): 65-71.
Samuel, V. T., K. F. Petersen, et al. (2010). "Lipid-induced insulin resistance: unravelling
the mechanism." Lancet 375(9733): 2267-2277.
Sanders, M. J., P. O. Grondin, et al. (2007). "Investigating the mechanism for AMP
activation of the AMP-activated protein kinase cascade." Biochem J 403(1): 139148.
Sano, H., S. Kane, et al. (2003). "Insulin-stimulated phosphorylation of a Rab GTPaseactivating protein regulates GLUT4 translocation." J Biol Chem 278(17): 1459914602.
Sarabia, V., L. Lam, et al. (1992). "Glucose transport in human skeletal muscle cells in
culture. Stimulation by insulin and metformin." J Clin Invest 90(4): 1386-1395.
Schenk, S., M. Saberi, et al. (2008). "Insulin sensitivity: modulation by nutrients and
inflammation." J Clin Invest 118(9): 2992-3002.
85
Sebastian, D., L. Herrero, et al. (2007). "CPT I overexpression protects L6E9 muscle cells
from fatty acid-induced insulin resistance." Am J Physiol Endocrinol Metab
292(3): E677-686.
Senn, J. J. (2006). "Toll-like receptor-2 is essential for the development of palmitateinduced insulin resistance in myotubes." J Biol Chem 281(37): 26865-26875.
Shen, J., X. Chen, et al. (2002). "ER stress regulation of ATF6 localization by dissociation
of BiP/GRP78 binding and unmasking of Golgi localization signals." Dev Cell
3(1): 99-111.
Shepherd, P. R., B. T. Nave, et al. (1997). "Involvement of phosphoinositide 3-kinase in
insulin stimulation of MAP-kinase and phosphorylation of protein kinase-B in
human skeletal muscle: implications for glucose metabolism." Diabetologia
40(10): 1172-1177.
Shi, H., M. V. Kokoeva, et al. (2006). "TLR4 links innate immunity and fatty acidinduced insulin resistance." J Clin Invest 116(11): 3015-3025.
Shulman, G. I., D. L. Rothman, et al. (1990). "Quantitation of muscle glycogen synthesis
in normal subjects and subjects with non-insulin-dependent diabetes by 13C
nuclear magnetic resonance spectroscopy." N Engl J Med 322(4): 223-228.
Sidrauski, C. and P. Walter (1997). "The transmembrane kinase Ire1p is a site-specific
endonuclease that initiates mRNA splicing in the unfolded protein response." Cell
90(6): 1031-1039.
Skov, V., D. Glintborg, et al. (2008). "Pioglitazone enhances mitochondrial biogenesis and
ribosomal protein biosynthesis in skeletal muscle in polycystic ovary syndrome."
PLoS One 3(6): e2466.
Song, X. M., M. Fiedler, et al. (2002). "5-Aminoimidazole-4-carboxamide ribonucleoside
treatment improves glucose homeostasis in insulin-resistant diabetic (ob/ob) mice."
Diabetologia 45(1): 56-65.
Storgaard, H., C. B. Jensen, et al. (2004). "Dissociation between fat-induced in vivo
insulin resistance and proximal insulin signaling in skeletal muscle in men at risk
for type 2 diabetes." J Clin Endocrinol Metab 89(3): 1301-1311.
Straczkowski, M., I. Kowalska, et al. (2007). "Increased skeletal muscle ceramide level in
men at risk of developing type 2 diabetes." Diabetologia 50(11): 2366-2373.
Straczkowski, M., I. Kowalska, et al. (2004). "Relationship between insulin sensitivity and
sphingomyelin signaling pathway in human skeletal muscle." Diabetes 53(5):
1215-1221.
Su, H. C., L. M. Hung, et al. (2006). "Resveratrol, a red wine antioxidant, possesses an
insulin-like effect in streptozotocin-induced diabetic rats." Am J Physiol
Endocrinol Metab 290(6): E1339-1346.
Summers, S. A., L. A. Garza, et al. (1998). "Regulation of insulin-stimulated glucose
transporter GLUT4 translocation and Akt kinase activity by ceramide." Mol Cell
Biol 18(9): 5457-5464.
Sun, C., F. Zhang, et al. (2007). "SIRT1 improves insulin sensitivity under insulinresistant conditions by repressing PTP1B." Cell Metab 6(4): 307-319.
Taniguchi, C. M., B. Emanuelli, et al. (2006). "Critical nodes in signalling pathways:
insights into insulin action." Nat Rev Mol Cell Biol 7(2): 85-96.
Thompson, A. L., M. Y. Lim-Fraser, et al. (2000). "Effects of individual fatty acids on
glucose uptake and glycogen synthesis in soleus muscle in vitro." Am J Physiol
Endocrinol Metab 279(3): E577-584.
Thong, F. S., P. J. Bilan, et al. (2007). "The Rab GTPase-activating protein AS160
integrates Akt, protein kinase C, and AMP-activated protein kinase signals
regulating GLUT4 traffic." Diabetes 56(2): 414-423.
86
Thrush, A. B., G. J. Heigenhauser, et al. (2008). "Palmitate acutely induces insulin
resistance in isolated muscle from obese but not lean humans." Am J Physiol
Regul Integr Comp Physiol 294(4): R1205-1212.
Tiikkainen, M., A. M. Hakkinen, et al. (2004). "Effects of rosiglitazone and metformin on
liver fat content, hepatic insulin resistance, insulin clearance, and gene expression
in adipose tissue in patients with type 2 diabetes." Diabetes 53(8): 2169-2176.
Timmers, S., E. Konings, et al. (2011). "Calorie restriction-like effects of 30 days of
resveratrol supplementation on energy metabolism and metabolic profile in obese
humans." Cell Metab 14(5): 612-622.
Timmers, S., P. Schrauwen, et al. (2008). "Muscular diacylglycerol metabolism and
insulin resistance." Physiol Behav 94(2): 242-251.
Todd, M. K., M. J. Watt, et al. (2007). "Thiazolidinediones enhance skeletal muscle
triacylglycerol synthesis while protecting against fatty acid-induced inflammation
and insulin resistance." Am J Physiol Endocrinol Metab 292(2): E485-493.
Tomas, E., T. S. Tsao, et al. (2002). "Enhanced muscle fat oxidation and glucose transport
by ACRP30 globular domain: acetyl-CoA carboxylase inhibition and AMPactivated protein kinase activation." Proc Natl Acad Sci U S A 99(25): 1630916313.
Tordjman, K. M., K. A. Leingang, et al. (1989). "Differential regulation of two distinct
glucose transporter species expressed in 3T3-L1 adipocytes: effect of chronic
insulin and tolbutamide treatment." Proc Natl Acad Sci U S A 86(20): 7761-7765.
Tsukumo, D. M., M. A. Carvalho-Filho, et al. (2007). "Loss-of-function mutation in Tolllike receptor 4 prevents diet-induced obesity and insulin resistance." Diabetes
56(8): 1986-1998.
Turban, S. and E. Hajduch (2011). "Protein kinase C isoforms: mediators of reactive lipid
metabolites in the development of insulin resistance." FEBS Lett 585(2): 269-274.
Turinsky, J., D. M. O'Sullivan, et al. (1990). "1,2-Diacylglycerol and ceramide levels in
insulin-resistant tissues of the rat in vivo." J Biol Chem 265(28): 16880-16885.
Um, J. H., S. J. Park, et al. (2010). "AMP-activated protein kinase-deficient mice are
resistant to the metabolic effects of resveratrol." Diabetes 59(3): 554-563.
Urano, F., X. Wang, et al. (2000). "Coupling of stress in the ER to activation of JNK
protein kinases by transmembrane protein kinase IRE1." Science 287(5453): 664666.
Varma, V., A. Yao-Borengasser, et al. (2009). "Muscle inflammatory response and insulin
resistance: synergistic interaction between macrophages and fatty acids leads to
impaired insulin action." Am J Physiol Endocrinol Metab 296(6): E1300-1310.
Vidal-Puig, A. J., R. V. Considine, et al. (1997). "Peroxisome proliferator-activated
receptor gene expression in human tissues. Effects of obesity, weight loss, and
regulation by insulin and glucocorticoids." J Clin Invest 99(10): 2416-2422.
Vijayvargia, R., K. Mann, et al. (2010). "JNK deficiency enhances fatty acid utilization
and diverts glucose from oxidation to glycogen storage in cultured myotubes."
Obesity (Silver Spring) 18(9): 1701-1709.
Vollenweider, P. (2003). "Insulin resistant states and insulin signaling." Clin Chem Lab
Med 41(9): 1107-1119.
Vollenweider, P., B. Menard, et al. (2002). "Insulin resistance, defective insulin receptor
substrate 2-associated phosphatidylinositol-3' kinase activation, and impaired
atypical protein kinase C (zeta/lambda) activation in myotubes from obese patients
with impaired glucose tolerance." Diabetes 51(4): 1052-1059.
Walker, K. S., M. Deak, et al. (1998). "Activation of protein kinase B beta and gamma
isoforms by insulin in vivo and by 3-phosphoinositide-dependent protein kinase-1
in vitro: comparison with protein kinase B alpha." Biochem J 331 ( Pt 1): 299-308.
87
Wang, Q., R. Somwar, et al. (1999). "Protein kinase B/Akt participates in GLUT4
translocation by insulin in L6 myoblasts." Mol Cell Biol 19(6): 4008-4018.
Weisberg, S. P., D. McCann, et al. (2003). "Obesity is associated with macrophage
accumulation in adipose tissue." J Clin Invest 112(12): 1796-1808.
Weng, L. P., W. M. Smith, et al. (2001). "PTEN inhibits insulin-stimulated MEK/MAPK
activation and cell growth by blocking IRS-1 phosphorylation and IRS-1/Grb2/Sos complex formation in a breast cancer model." Hum Mol Genet 10(6): 605616.
White, M. F. (2003). "Insulin signaling in health and disease." Science 302(5651): 17101711.
White, M. F. and C. R. Kahn (1994). "The insulin signaling system." J Biol Chem 269(1):
1-4.
Widegren, U., J. W. Ryder, et al. (2001). "Mitogen-activated protein kinase signal
transduction in skeletal muscle: effects of exercise and muscle contraction." Acta
Physiol Scand 172(3): 227-238.
Winder, W. W. and D. G. Hardie (1996). "Inactivation of acetyl-CoA carboxylase and
activation of AMP-activated protein kinase in muscle during exercise." Am J
Physiol 270(2 Pt 1): E299-304.
Winder, W. W., B. F. Holmes, et al. (2000). "Activation of AMP-activated protein kinase
increases mitochondrial enzymes in skeletal muscle." J Appl Physiol 88(6): 22192226.
Winnay, J. N., J. Boucher, et al. (2010). "A regulatory subunit of phosphoinositide 3kinase increases the nuclear accumulation of X-box-binding protein-1 to modulate
the unfolded protein response." Nat Med 16(4): 438-445.
Wojtaszewski, J. F., J. B. Birk, et al. (2005). "5'AMP activated protein kinase expression
in human skeletal muscle: effects of strength training and type 2 diabetes." J
Physiol 564(Pt 2): 563-573.
Wu, J., J. L. Ruas, et al. (2011). "The unfolded protein response mediates adaptation to
exercise in skeletal muscle through a PGC-1alpha/ATF6alpha complex." Cell
Metab 13(2): 160-169.
Yamauchi, T., J. Kamon, et al. (2002). "Adiponectin stimulates glucose utilization and
fatty-acid oxidation by activating AMP-activated protein kinase." Nat Med 8(11):
1288-1295.
Yamauchi, T., Y. Nio, et al. (2007). "Targeted disruption of AdipoR1 and AdipoR2 causes
abrogation of adiponectin binding and metabolic actions." Nat Med 13(3): 332339.
Yaspelkis, B. B., 3rd, M. K. Singh, et al. (2004). "Chronic leptin treatment enhances
insulin-stimulated glucose disposal in skeletal muscle of high-fat fed rodents." Life
Sci 74(14): 1801-1816.
Yu, C., Y. Chen, et al. (2002). "Mechanism by which fatty acids inhibit insulin activation
of insulin receptor substrate-1 (IRS-1)-associated phosphatidylinositol 3-kinase
activity in muscle." J Biol Chem 277(52): 50230-50236.
Yu, J. G., S. Javorschi, et al. (2002). "The effect of thiazolidinediones on plasma
adiponectin levels in normal, obese, and type 2 diabetic subjects." Diabetes 51(10):
2968-2974.
Zang, M., S. Xu, et al. (2006). "Polyphenols stimulate AMP-activated protein kinase,
lower lipids, and inhibit accelerated atherosclerosis in diabetic LDL receptordeficient mice." Diabetes 55(8): 2180-2191.
Zeigerer, A., M. K. McBrayer, et al. (2004). "Insulin stimulation of GLUT4 exocytosis,
but not its inhibition of endocytosis, is dependent on RabGAP AS160." Mol Biol
Cell 15(10): 4406-4415.
88
Zhang, B. B., G. Zhou, et al. (2009). "AMPK: an emerging drug target for diabetes and the
metabolic syndrome." Cell Metab 9(5): 407-416.
Zheng, D., P. S. MacLean, et al. (2001). "Regulation of muscle GLUT-4 transcription by
AMP-activated protein kinase." J Appl Physiol 91(3): 1073-1083.
Zhou, G., R. Myers, et al. (2001). "Role of AMP-activated protein kinase in mechanism of
metformin action." J Clin Invest 108(8): 1167-1174.
Zierath, J. R. (1995). "In vitro studies of human skeletal muscle: hormonal and metabolic
regulation of glucose transport." Acta Physiol Scand Suppl 626: 1-96.
Zierath, J. R., J. W. Ryder, et al. (1998). "Role of skeletal muscle in thiazolidinedione
insulin sensitizer (PPARgamma agonist) action." Endocrinology 139(12): 50345041.
89