lab report 2 - Sites at Penn State
advertisement

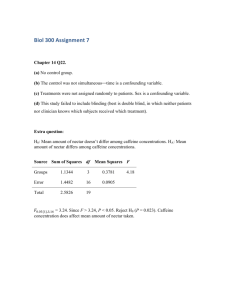
Martin 1 Effects of caffeine on the heart by analyzing heart rates of men and women after physical activity Gina Martin Bio230W Section 002 Sashi Gollapudi April 8, 2013 Martin 2 Introduction: According to the National Vital Statistics Reports, the leading cause of death in the United States is heart disease.1 Heart disease can be induced by many different factors such as, high cholesterol, stress, poor diet, smoking and family history. Heart disease is defined as a condition that impairs heart function or circulation of the blood by the heart. One of the most common types of heart disease is coronary heart disease, which is when the arteries of the heart harden, blocking blood supply back to the heart for further circulation.2 Coronary artery disease can often induce a heart attack in patients due to the hardening of the arteries. Other heart diseases include: angina pectoris, auricular fibrillation, and coronary thrombosis. Heart disease can be reduced by changes in diet, increase in exercise, and less stressful environment. The heart pumps nutrients to all parts of the body through a system of veins and arteries in the body.3 The heart is made up of four chambers which pump blood in and out of this muscular organ. The muscles of the heart are classified as cardiac muscles, which are unique when compared to other muscles because they can contract without control of the central nervous system. The chambers of the heart are separated into two major sections called the superior atrial chambers and inferior ventricular chambers. The heart is also further divided into right and left atriums. The right portion of the heart collects deoxygenated blood from other parts of the body and pumps it into the pulmonary artery where it goes to the lungs to become oxygenated again. Once the blood is oxygenated by the lungs it then circulates back up to the heart and enters the left atrium. Diastolic contraction is when the oxygenated blood moves from the left atrium to the left ventricle. Systolic contraction Martin 3 is when the oxygenated blood is pumped through the semilunar aortic valve into the aorta which eventually will enter systemic circulation. These diastolic and systolic contraction are the systems used to measure blood pressure. Blood pressure measures the opening and closing of the valves during diastolic and systolic contraction.4 High blood pressure can indicate how blocked arteries are in a person’s body. The instrument used to measure blood pressure is called an sphygmomanometer. A sphygmomanometer is a cuff with pump that shows the blood pressure. A stethoscope is also needed in order to differentiate between the diastolic and systolic pressure. Caffeine is one of the most widely consumed drugs in the world. About 80% of adults consume at least 3-5 cups of coffee a day.5 Caffeine can be found in many different substances such as, coffee, tea, chocolate, and energy drinks. Researchers are uncertain as to whether or not caffeine has a positive or negative effect on the body. A study done by Bennett, Rodrigues, and Kline found that caffeine caused and increase in systolic blood pressure in both men and women who had a family history of cardiovascular disease.6 Another study done Astorino, Martin, and Schachtsiek, compared the effects of caffeine in men with hypertension and without hypertension while exercising. 7 The results showed that caffeine resulted in an increase in resting, exercise, and recovery systolic blood pressure, but there was no change in diastolic pressure and heart rate. Caffeine use was also found to cause an increase in muscle pain and heart rate during exercise, in a study done by Duncan, M.J. and Hankey, J. 8 Thus, it is believed that caffeine consumption may increase the risk for cardiovascular diseases. During this laboratory experiment, participants blood pressures and pulse counts were taken before and after exercise in order to compare the effects of caffeine on the heart.9 The Martin 4 objectives of this laboratory experiment were to collect data from each participant in order for their resting pulse count and blood pressure to be compared with their values post exercise. Participants were asked to give their personal history in order to indicate the amount of exercise, caffeine, and other habits that may affect cardiovascular health that they experienced in a weeks time, in order for their cardiovascular health to be examined. It is believed that participants who regularly ingest large amounts of caffeine during a week will have higher blood pressure and pulse counts, when compared to participants who had moderate to no consumption of caffeine. Materials and Methods: Personal History: This laboratory experiment began with collecting personal history from each participant in the study. The personal data collected was the following information: age, sex, weight (lbs.), height (inches), smoking (number of cigarettes a day), caffeine (average servings a day), alcohol (average servings a week), and exercise (average numbers of days a week). The data was charted on a computer, so it could later be charted with additional data for comparison. Resting Pulse Count and Blood Pressure: Next, each individual collected their own resting heart rate by placing their index and middle fingers on the neck or wrist and counting the amount of pulse counts in thirty seconds. This was repeated three times for each individual to get an average thirty second pulse count. The average pulse count was then multiplied by two to get the resting heart rate in beats per minute. The resting blood pressure was also collected for each individual using a sphygmomanometer and a stethoscope. To measure resting blood pressure the brachial artery on Martin 5 the arm is located in order to determine where to attach the sphygmomanometer. The cuff was then wrapped around the individuals arm so it is above the elbow crease, making sure that the valve on the bulb remains closed. The upper arm must be level with the heart in order to get a accurate reading. The stethoscope was then placed under the cuff where the artery is located and the bulb was then squeezed to apply pressure to 200mm. The valve was then released slowly until a fait thump was heard, which was the systolic pressure. When the sound disappears completely the diastolic pressure has been found. Both these values are recorded as systolic over diastolic. Exercise Pulse Count and Blood Pressure: For participants shorter than 5 feet 6 inches a box that was 33cm high was used. If participants were taller than 5 feet 6 inches then a 40 cm high box was used for the exercise. A single exercise consisted of taking one step with one leg onto the box, another step with the other leg so the whole body was on the box. Then stepping down off the box with one leg, and finally stepping down with the other. This exercise was done at two different speeds 15 steps per minute and 30 steps per minute for one minute each time. After the participants completed the exercise they sat down and after 15 seconds began taking their own pulse. Their blood pressure was taken after the 15 seconds had passed. This was repeated for everyone in the group at both speeds. Data Collection: After the class had finished the exercise portion of the experiment, the data was then placed on a chart so it could be combined with additional data. One category of data was chosen for analysis. For this study, pulse count and blood pressure of participants that drank caffeine were compared with participants who did not drink any caffeine. Martin 6 Results: The resting levels values in Table 1(see below) and in the Resting Level Values graph(see below) showed no significant difference in pulse rate between the caffeine and no caffeine groups. The average systolic blood pressure in the caffeine group was 125.19 mm Hg, while the value for the caffeine-less group was 121.912 mm Hg. The values for average diastolic blood pressure was 76.234 mm Hg, while the caffeine-free group was 72.5455 mmHg. The p-values for these results was 0.445 for the pulse count data, 0.137 for the systolic blood pressure data, and 0.162 for the diastolic blood pressure data. The normalized average change in pulse count after exercise was depicted in Table 2 and Graph 2. The average pulse count for the caffeine group was 12.75 beats per minute during the 15-step exercise and 43.72 beats per minute during the 30-step exercise. The average pulse count for the no caffeine group during the 15-step exercise was 21.27 beats per minute and 48.77 beats per minute for the 30-step exercise. The p-value for the 15-step exercise was 0.065, while the pvalue for the 30-step exercise was 0.494. Table 3 and Graph 3 depicted a normalized average change in systolic blood pressure after exercise. The average percentage difference for the systolic blood pressure in the caffeine users was 131.44 mm Hg for the 15-step exercise and 144.74 mm Hg for the 30-step exercise. While the average percentage difference in systolic pressure for the no caffeine group was 132.03 mm Hg for the 15-step exercise trial and 144.697 mm Hg for the 30-step exercise. The pvalue for the 15-step exercise was 0.882 and the p-value for the 30-step exercise was 0.97. Lastly Table 4 and Graph 4 showed the average percentage difference for diastolic blood pressure. The average percentage difference for the diastolic blood pressure for the caffeine Martin 7 group was 74.89 mm Hg for the 15-step exercise and 76.744 mm Hg for the 30-step exercise. The average percentage difference for the caffeine-free group was 75.27 mm Hg for the 15-step exercise and 77.57 mm Hg for the 30-step exercise. The p-value for the 15-step exercise was 0.874 and the p-value for the 30-step exercise was 0.162. Table 1: Resting level values: Average caffeine no caf Pulse count 36.2166 35.38697 Sys.BP 125.1915 121.9118 Dias.BP 76.23404 72.54546 SE caf 0.740089 1.907102 1.880376 SD no caf caf 0.788588 5.0737908 1.691007 13.074433 1.809639 12.891205 no caf 4.53009 9.71409 10.3956 Graph 1: Resting Level Values Resting Level Values 130 98 65 33 0 Pulse count caffeine Sys. BP Dias. BP no caffeine The results of Table 1 and Graph 1 showed that there was no significant increase or decrease in average pulse count in the caffeine and no caffeine groups. The average systolic pressure for the caffeine group was slightly higher than what was experienced in the no caffeine group. The average diastolic pressure was also slightly higher in the caffein group than in the no caffeine group. Martin 8 Graph 2: Normalized Average Change in Pulse Count/ 30sec After Exercise Pulse Count 60 45 30 15 0 Caffeine 15-Steps No Caffeine 30-Steps Exercise Data: Table 2: Normalized average change in pulse count/30sec after exercise av. % diff SE sd no caf caffeine no caf caf no caf Pulse count caffeine 15-steps 12.753 21.276 3.0638 3.372 21.004 19.369 30-steps 43.723 48.77 4.4303 5.8603 30.372 33.665 Table 2 and Graph 2 examined the results for the average change in pulse count after exercise. The no caffeine group experienced a larger increase in pulse count after exercise than the caffeine group. Martin 9 Graph 3: Normalized Average Change in Systolic BP After Exercise Systolic BP (mm Hg) 150 143 135 128 120 Caffeine 15-Steps No Caffeine 30-Steps Exercise Data: Table 3: Normalized average change in systolic BP after exercise av. % diff SE sd Sys.BP caffeine no caf caf no caf caf no caf 15-steps 131.446 132.03 2.288 3.19 15.683 18.35 30-steps 144.74 144.697 2.299 2.971 15.764 17.069 Table 3 and Graph 3 showed no significant differences between the caffeine and the no caffeine groups. The average percentage difference for the 30-step exercise was actually the same number. Martin 10 Graph 4: Normalized Average Change in Diastolic BP After Exercise Diastolic BP (mm Hg) 80 78 77 75 73 Caffeine 15-Step No Caffeine 30-Step Table 4: Normalized average change in diastolic BP after exercise av. % diff SE SD Dias.BP caffeine no caf caf no caf CAF NO caf 15-steps 74.894 75.273 1.624 1.7338 11.134 9.96 30-steps 76.745 77.576 1.577 1.834 10.810 10.539 Table 4 and Graph 4 shows the average change in diastolic blood pressure after exercise. The difference between the average blood pressures were so close they were proven insignificant. The standard error for the diastolic blood pressure was also too large to prove any significance. Martin 11 Discussion: The results of the analysis of the data collected from the analysis of caffeine’s affects of the heart are unclear. The average resting level values in table 1 showed no significant difference in the average pulse rate, but did show a difference in the systolic blood pressure and the diastolic blood pressure. The systolic blood pressure in the caffeine group was 125.19 mm Hg while it was only 121.912 mm Hg for the caffeine free group. The diastolic blood pressure was 76.23 mm Hg for the caffeine group and 72.54 mm Hg for the caffeine-free group. Thus, the average resting heart rate was higher in individuals who had caffeine in their diet, but the pulse count was not affected. The normalized average change in pulse count(table 2) showed a increase in pulse count in participants whom did not consume caffeine. The value increased in both the 15-step and the 30-step exercises for the caffeine-free group. Thus, caffeine consumption could cause the pulse count to decrease while engaging in physical activity. The normalized average change in systolic(table 3) and diastolic (table 4) pressure after exercise showed no significant increase in the systolic group or the diastolic group from the caffeine consumers and the caffeine-free group. There was also a very large standard errors for the diastolic group, proving some statistical insignificance. The p-values for all of the data collected were above 0.05 making the data statically insignificant for the experiment. These values could have been improved by making a more strict requirements for caffeine drinkers, such as having to consume X amount of caffeine in a week. There should have also been more strict restrictions on being in the caffeine free group, such as having to consume less than X amount of caffeine a week. This would provide data on people Martin 12 who definitely fit the criteria of being in either the caffeine group or the caffeine-free group. Another improvement that would have made the data more statistically significant would have been to have taken into consideration people’s personal history for factors that would cause stress on the heart that could alter the data. In conclusion, although the p-values prove the data to be statistically insignificant the study proved the hypothesis that caffeine consumption would increase pulse rate and blood pressure to be false. Further statistically analysis needs to be done to completely accept this rejection of hypothesis because of the insignificant p-values. Improvements that need to be done to improve the results would be to use certified personnel to take the blood pressure and pulse rates so more accurate data can be received and to take into consideration family history for heart disease. According to other studies done this data is not cohesive, which intensifies the need for further research with more accurate analysis. Since there is such a large amount of the population which consumes caffeine, additional experiments need to be done with finer search criteria to provide a more accurate description of the results. Martin 13 References: 1. Kochaneck, K., Xu, J., Murphy, S., Minino, A., Kung, H. Deaths: Final Data for 2009. National Vitals Statistics Report. 60,3. December 2011. 2. Braus, Patricia. "Heart Diseases." The Gale Encyclopedia of Science. Ed. K. Lee Lerner and Brenda Wilmoth Lerner. 4th ed. Vol. 3. Detroit: Gale, 2008. 2081-2083. Gale Virtual Reference Library. Web. 3 Apr. 2013. 3. Lerner, Brenda Wilmoth, K. Lee Lerner, and Larry Blaser. "Heart." The Gale Encyclopedia of Science. Ed. K. Lee Lerner and Brenda Wilmoth Lerner. 3rd ed. Vol. 3. Detroit: Gale, 2004. 1934-1939. Gale Virtual Reference Library. Web. 3 Apr. 2013. 4. Fallon, L. Fleming. "Sphygmomanometer." The Gale Encyclopedia of Surgery. Ed. Anthony J. Senagore. Vol. 3. Detroit: Gale, 2004. 1350-1352. Gale Virtual Reference Library. Web. 4 Apr. 2013. 5. Klein, L.C. (2013). Pharmacological influences on health [Word document]. Retrieved from Lecture Notes Online Web site: https://cms.psu.edu 6. Bennett, J.M., Rodrigues, I.M., Kline, L.C. (2013). Effects of Caffeine and Stress on Biomarkers of Cardiovascular Disease in Healthy Men and Women with a Family History of Hypertension. Stress Health. 7. Astorino,T., Martin, B., Schachtsiek, L. (2011) Caffeine Ingestion and Intense Resistance Training Minimize Postexercise Hypotension in Normotensive and Prehypertensive Men. Research in Sports Medicine. 21-1, 52-65. Online. 8. Duncan, M.J., Hankey, J. (2013) The effects of a caffeinated energy drink on various psychological measures during submaximal cycling. Physio Behavior. Web. Martin 14 9. “Cardiovascular Physiology: The Relationship between Gas Exchange and Cardiac Activity.” Edited by Nelson, K. and Burpee, D. Department of Biology, The Pennsylvania State University, University Park, PA. (2013)