reconstructive - Shifa International Hospital
advertisement

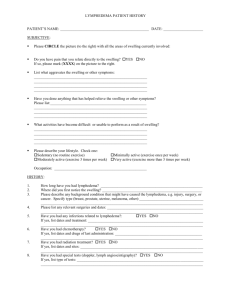
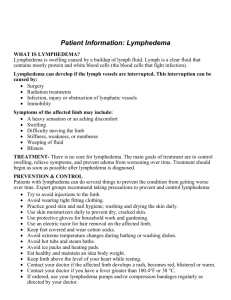
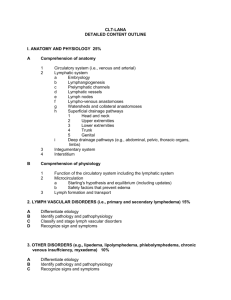
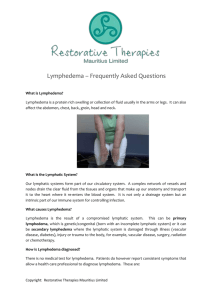
RECONSTRUCTIVE Differential Diagnosis of Lower Extremity Enlargement in Pediatric Patients Referred with a Diagnosis of Lymphedema Carolyn C. Schook, B.A. John B. Mulliken, M.D. Steven J. Fishman, M.D. Ahmad I. Alomari, M.D. Frederick D. Grant, M.D. Arin K. Greene, M.D., M.M.Sc. Boston, Mass. Background: There are many causes for a large lower limb in the pediatric age group. These children are often mislabeled as having lymphedema, and incorrect diagnosis can lead to improper treatment. The purpose of this study was to determine the differential diagnosis in pediatric patients referred for lower extremity “lymphedema” and to clarify management. Methods: The authors’ Vascular Anomalies Center database was reviewed between 1999 and 2010 for patients referred with a diagnosis of lymphedema of the lower extremity. Records were studied to determine the correct cause for the enlarged extremity. Alternative diagnoses, sex, age of onset, and imaging studies were also analyzed. Results: A referral diagnosis of lower extremity lymphedema was given to 170 children; however, the condition was confirmed in only 72.9 percent of patients. Forty-six children (27.1 percent) had another disorder: microcystic/macrocystic lymphatic malformation (19.6 percent), noneponymous combined vascular malformation (13.0 percent), capillary malformation (10.9 percent), KlippelTrenaunay syndrome (10.9 percent), hemihypertrophy (8.7 percent), posttraumatic swelling (8.7 percent), Parkes Weber syndrome (6.5 percent), lipedema (6.5 percent), venous malformation (4.3 percent), rheumatologic disorder (4.3 percent), infantile hemangioma (2.2 percent), kaposiform hemangioendothelioma (2.2 percent), or lipofibromatosis (2.2 percent). Age of onset in children with lymphedema was older than in patients with another diagnosis (p ⫽ 0.027). Conclusions: “Lymphedema” is not a generic term. Approximately one-fourth of pediatric patients with a large lower extremity are misdiagnosed as having lymphedema; the most commonly confused causes are other types of vascular anomalies. History, physical examination, and often radiographic studies are required to differentiate lymphedema from other conditions to ensure the child is managed appropriately. (Plast. Reconstr. Surg. 127: 1571, 2011.) L ymphedema is the chronic, progressive swelling of tissue caused by inadequate lymphatic function. Lymphedema may result from anomalous development (primary) or injury (secondary) to lymph nodes or lymphatic vessels. Although lymphedema is a specific condition, children with a large lower limb are often labeled as having lymphedema, regardless of the underlying cause. Because lymphedema is much more prevalent in the general population than other potenFrom the Departments of Plastic and Oral Surgery, Surgery, and Radiology, Vascular Anomalies Center, Children’s Hospital Boston, Harvard Medical School. Received for publication July 22, 2010; accepted October 11, 2010. Copyright ©2011 by the American Society of Plastic Surgeons DOI: 10.1097/PRS.0b013e31820a64f3 tial causes of congenital lower extremity overgrowth, referring physicians likely are most familiar with the term “lymphedema.” Lymphedema, however, is typically an adult disease caused by lymphadenectomy and/or irradiation to the axilla or groin. Primary pediatric lymphedema is rare; a child erroneously diagnosed with lymphedema may undergo unnecessary tests and be given incorrect treatment. The purposes of this study were to determine the accuracy of the term “lymphedema” for pediatric lower limb enlargement and to document other causes with which it is frequently confused. Disclosure: The authors have no financial interest to declare in relation to the content of this article. www.PRSJournal.com 1571 Plastic and Reconstructive Surgery • April 2011 PATIENTS AND METHODS After approval from the Committee on Clinical Investigation at Children’s Hospital Boston, our Vascular Anomalies Center database was reviewed for patients sent between 1999 and 2010 labeled with lower extremity “lymphedema.” Individuals with disease onset after 21 years of age were excluded to ensure that only a pediatric cohort was studied. The correct diagnosis was determined by history, physical examination, photographs, imaging studies, and/or histopathology. Alternative conditions, sex, and age-of-onset were recorded. The Mann-Whitney U test was used to differentiate age of onset between patients with lymphedema and children with other disorders. Age of onset was defined in years and, if present before 12 months of age, was recorded as 0. Results are presented as median with interquartile range (25th to 75th percentile). A two-tailed value of p ⬍ 0.05 was considered significant. Statistical analysis was performed using the SPSS software package (version 16.0; SPSS, Inc., Chicago, Ill.). RESULTS A referral diagnosis of lower extremity lymphedema was identified in 170 children of 9477 patients in the database (1.8 percent). Lymphedema was confirmed in 124 patients (72.9 percent). The remaining 27.1 percent (46 of 170) of patients referred with lymphedema had a different diagnosis (Table 1). Seventy percent (32 of 46) had another type of vascular anomaly: microcystic/macrocystic lymphatic malformation (19.6 percent), noneponymous combined vascular malformation (13.0 percent), diffuse capillary malformation with overgrowth (10.9 percent), Klippel-Trenaunay syndrome (10.9 percent), Parkes Table 1. Causes of an Enlarged Lower Extremity Referred with an Incorrect Diagnosis of Lymphedema No. (%) Microcystic/macrocystic lymphatic malformation Noneponymous combined vascular malformation Klippel-Trenaunay syndrome Capillary malformation Hemihypertrophy Posttraumatic swelling Parkes Weber syndrome Lipedema Venous malformation Rheumatologic disease Infantile hemangioma Kaposiform hemangioendothelioma Lipofibromatosis Total 1572 9 (19.6) 6 (13.0) 5 (10.9) 5 (10.9) 4 (8.7) 4 (8.7) 3 (6.5) 3 (6.5) 2 (4.3) 2 (4.3) 1 (2.2) 1 (2.2) 1 (2.2) 46 (100) Weber syndrome (6.5 percent), venous malformation (4.3 percent), infantile hemangioma (2.2 percent), or kaposiform hemangioendothelioma (2.2 percent). Other conditions confused with lymphedema were hemihypertrophy (8.7 percent), posttraumatic swelling (8.7 percent), lipedema (6.5 percent), rheumatologic disease (4.3 percent), and lipofibromatosis (2.2 percent). Female patients constituted 62.1 percent of patients (77 of 124) with lymphedema and 58.7 percent (27 of 46) of children without the disorder (p ⫽ 0.68). Median age of onset in children with lymphedema was older [4 years (range, 0 to 12 years)] than in patients with another diagnosis [0 years (range, 0 to 4 years)] (p ⫽ 0.027). At least one imaging study was obtained in 84.7 percent (144 of 170) of children: magnetic resonance imaging in 93 (54.1 percent), ultrasonography in 78 (45.9 percent), plain film radiography in 53 (31.2 percent), lymphoscintigraphy in 35 (20.6 percent), computed tomography in 27 (15.9 percent), echocardiography in 13 (7.6 percent), and/or angiography in 12 patients (7.1 percent). DISCUSSION Lymphedema is an often loosely used label for an enlarged lower extremity in children, regardless of the cause. Lymphedema is a precise term that defines chronic, progressive swelling of subcutaneous tissue caused by abnormal development or injury to the lymphatic vasculature. Primary lymphedema most commonly affects the lower extremity (Fig. 1). Patients have a significant risk of infection, and limb enlargement occurs over time from adipose deposition and fibrosis. Lymphedema can be differentiated from other causes of extremity overgrowth by history and physical examination in approximately 90 percent of patients. The foot is always involved and swelling proceeds proximally. Edema becomes less pitting over time as adipose and fibrous tissue are deposited.1 Definitive diagnosis of lymphedema requires lymphoscintigraphy, which is 92 percent sensitive and 100 percent specific for the disorder.2 Compromised lymphatic function is illustrated by delayed transit and/or cutaneous accumulation (dermal backflow) of radiolabeled colloid injected into the feet. Management of lymphedema requires daily washing and moisturizing of the extremity to minimize desiccation, skin breakdown, and subsequent cellulitis. Patients should wear protective clothing to prevent incidental trauma, which also can lead to infection. Compression therapy using a custom-fitted garment and a pneumatic pump Volume 127, Number 4 • Pediatric Lower Limb Enlargement Fig. 1. Images demonstrating primary lymphedema in a 2-year-old boy with left lower extremity swelling that had been present since birth (left). (Above, right) Lymphoscintigraphy demonstrates dermal backflow and absent inguinal node drainage 21⁄2 hours after injection. (Below, right) Axial T2-weighted magnetic resonance imaging with fat saturation shows a hyperintense reticular network of dilated subcutaneous channels between the dermis and fascial plane. helps to reduce the volume of the extremity and slow progression. Patients with significant morbidity who have failed conservative treatment may be considered for contour resection. We prefer suction-assisted lipectomy for moderately enlarged extremities and staged skin/subcutaneous resection for patients with major overgrowth and skin excess.3– 6 Approximately one-fourth of patients labeled with lymphedema referred to our center had another condition. The most commonly confused diagnoses were other vascular anomalies: single-vessel forms (capillary malformation, lymphatic malformation, venous malformation), combined malformations (capillary-venous, lymphatic-venous), and eponymous syndromes (Klippel-Trenaunay, Parkes Weber). It is important to separate these conditions from lymphedema because their natural history, prognosis, and treatment are very different. Like lymphedema, vascular anomalies are diagnosed by history and physical examination in at least 90 percent of patients. Although primary lymphedema can present at birth, it also may develop later in childhood or in adolescence. In contrast, most vascular anomalies are obvious during infancy. Girls are not more likely to have lymphedema than boys; therefore, sex should not be considered when differentiating lymphedema from other conditions. If the diagnosis remains equivocal following history and physical examination, lymphoscintigraphy will rule out lymphedema, and magnetic resonance imaging can confirm the diagnosis of another vascular anomaly. Diffuse capillary malformation with overgrowth can cause soft-tissue and skeletal enlargement of a limb (Fig. 2). Patients are not at increased risk for infection, and the progression of overgrowth is slow. The cutaneous stain is treated by pulsed-dye laser. The circumferential overgrowth may be improved with suction-assisted lipectomy; occasionally, axial enlargement can cause a leg-length discrepancy. Venous and noneponymous combined malformations (e.g., capillary-venous, lymphatic-venous) are localized in more than 90 percent of patients; 50 percent affect deep structures (e.g., muscle, bone, joints, viscera) (Figs. 2 and 3).7,8 One-half of sporadic venous malformations have a somatic mutation in the TIE2 receptor.8 Venous malformations of the lower limb typically involve the skin and/or muscles. If all tissues, including 1573 Plastic and Reconstructive Surgery • April 2011 Fig. 2. Examples of patients with single-vessel type vascular malformations with a referring diagnosis of lymphedema. (Above, left) A 9-year-old boy with a diffuse capillary malformation and overgrowth of the left lower extremity; capillary malformation is not a component of lymphedema. (Below, left) Coronal T1-weighted magnetic resonance imaging shows thickening of the subcutaneous fat with normal blood channels. (Above, center) An 8-year-old girl with a venous malformation of the right lower extremity (lymphedema does not have cutaneous varicosities). (Below, center) Coronal T2-weighted magnetic resonance imaging scan showing deep intramuscular and cutaneous venous anomalies. (Above, right) A 12-month-old boy with a lymphatic malformation of the right lower limb. Although history and physical examination were consistent with lymphedema, macrocystic lymphatic malformation was diagnosed based on magnetic resonance imaging findings. (Below, right) Sagittal T2-weighted magnetic resonance imaging scan with fat saturation demonstrates fluid-filled lymphatic macrocysts within the intermuscular space. bone, are affected, the disorder is called phlebectasia of Bockenheimer.9 Extremity venous malformation can cause leg-length discrepancy, hypoplasia resulting from disuse atrophy, fibrosis, pain, pathologic fracture, hemarthrosis, and degenerative arthritis.10,11 A large venous malformation involving the deep venous system is at risk for thrombosis and pulmonary embolism. Stagnation within a lesion can cause localized intravascular coagulopathy and painful phlebothromboses. 1574 Treatment of lower extremity venous malformation includes compression garments, sclerotherapy, and/or resection. Primary lymphedema differs from microcystic, macrocystic, and combined lymphatic malformations because it is not cystic and involves only the subcutaneous layer. Microcystic/macrocystic lymphatic malformation can affect all structures of the extremity, including muscle and bone (Fig. 2). Several germ-line mutations cause Volume 127, Number 4 • Pediatric Lower Limb Enlargement Fig. 3. Example of a noneponymous combined vascular malformation with a referring diagnosis of lymphedema. (Left) A 15-year-old girl with a capillary-venous malformation of the right lower limb; a lymphedematous lower extremity typically has normal overlying skin. (Right) Axial T2-weighted magnetic resonance imaging scan shows dilated veins within the subcutaneous fat underlying the capillary stain. primary lymphedema (VEGFR3, FOXC2, SOX18, and CCBE1).12–15 In contrast, microcystic/macrocystic lymphatic malformations are thought to result from paradominant inheritance; an individual with a predisposed inherited mutation develops a somatic second hit in the same gene that causes expression of the lesion.16 Symptomatic microcystic/macrocystic lymphatic malformations of the lower extremity are managed by compression, sclerotherapy, and/or resection. The eponymous vascular malformations, KlippelTrenaunay and Parkes Weber syndrome, usually are more problematic than lymphedema (Fig. 4). Klippel-Trenaunay syndrome is a capillary-lymphatic-venous malformation of the lower extremity with overgrowth. Patients are at risk for infections, deep venous thrombosis, pulmonary embolism, leg-length discrepancy, and difficulty with ambulation. Large embryonal veins are removed to prevent venous thrombosis. A shoe lift or epiphysiodesis may be necessary to correct leg-length discrepancy. Occasionally, selective amputation is required to permit footwear and to facilitate ambulation. Soft-tissue overgrowth can be improved with staged skin/subcutaneous resection. Parkes Weber syndrome is a capillary-arteriovenous or capillary-lymphatic-arteriovenous malformation of the lower extremity with overgrowth. Parkes Weber syndrome can be caused by a mutation in RASA1, and patients with multiple capillary malformations are likely on the spectrum of capillary malformation-arteriovenous malformation.17 Patients are at risk for congestive heart failure because of extensive arteriovenous shunting. Genetic counseling is required for children with capillary malformation-arteriovenous malformation because it is an autosomal dominant condition. Symptomatic patients are managed by embolization; epiphysiodesis or amputation may be necessary. Lipedema is commonly misdiagnosed as lymphedema (Fig. 5). It is characterized by bilateral, fatty hypertrophy of the lower extremities in disproportion to the rest of the body.18 Pubertal female patients are primarily affected, and a positive family history may be reported. Unlike lymphedema, the foot is not involved, pain is common, and patients are not at an increased risk for infection. Lipedema can be differentiated from lymphedema by history and physical examination. Magnetic resonance imaging shows increased subcutaneous adipose tissue without stranding or thickened skin; lymphoscintigraphy is normal. The size of the limb can be reduced by suctionassisted lipectomy. 1575 Plastic and Reconstructive Surgery • April 2011 Fig. 4. Examples of children with eponymous combined vascular anomalies with a referring diagnosis of lymphedema. (Above, left) An 18-year-old female patient with KlippelTrenaunay syndrome of the left lower extremity. The capillary malformation, venous varicosities, and cutaneous lymphatic vesicles were not consistent with lymphedema. (Below, left) Axial T2-weighted magnetic resonance imaging scan with fat saturation demonstrates a marginal venous system and subcutaneous lymphatic malformation with subfascial involvement. (Above, right) A 6-month-old with Parkes Weber syndrome. A cutaneous stain and warm extremity indicated a fast-flow malformation. Diagnosis was confirmed by magnetic resonance angiography (below, right), demonstrating enlargement of the arteries and early opacification of the dilated veins. Hemihypertrophy, the idiopathic enlargement of an area compared with the contralateral side, may be confused with lymphedema (Fig. 6).19 Hemihypertrophy is usually a diagnosis of exclusion. Lymphoscintigraphy is normal and magnetic resonance imaging demonstrates enlargement of all components of the extremity (i.e., adipose, muscle, bone) without pathologic findings. Unlike lymphedema, there is overgrowth of the tissues below the muscle fascia. Occasionally, symmetry may be improved with suction-assisted lipectomy of the subcutaneous compartment. In contrast to other causes of extremity overgrowth, children with hemihypertrophy are at risk for Wilms tumor and require screening.20 A lower extremity tumor can be mistaken for lymphedema (Fig. 7). Infantile hemangioma, the 1576 most common tumor of infancy, is usually localized and easily distinguished from lymphedema. A diffuse, reticular form may involve the lower extremity and present with hypertrophy.21 Reticular hemangioma is differentiated from lymphedema because it appears shortly after birth, proliferates, and then involutes. The tumor is infiltrative and can involve fascia or muscle. In addition, reticular hemangioma often ulcerates and is associated with ventral-caudal malformative anomalies.21 Management may require corticosteroid treatment for recalcitrant ulceration or congestive heart failure; imaging is necessary to rule out underlying structural disorders. Kaposiform hemangioendothelioma is a rare vascular neoplasm that is locally aggressive but does not metastasize.22,23 Although one-half of le- Volume 127, Number 4 • Pediatric Lower Limb Enlargement Fig. 5. Example of a patient with lipedema referred with a mistaken diagnosis of lymphedema. (Left) The patient was a 34-year-old woman who had had enlarged lower extremities since adolescence. Because the feet were not involved, lipedema was diagnosed by physical examination and confirmed with imaging. The lymphoscintigram was normal (prompt tracer uptake into abdominal nodes bilaterally) (above, right), and coronal T1-weighted magnetic resonance imaging showed circumferential overgrowth of the subcutaneous fat (below, right). sions are present at birth, onset can occur in infancy or childhood.24 The tumor is often diffuse, and an extremity is affected in approximately onethird of patients.24,25 The skin is reddish purple and pain is common. In addition, 50 percent of patients have Kasabach-Merritt phenomenon [thrombocytopenia (⬍25,000/mm3), petechiae, bleeding].22,26,27 Kaposiform hemangioendothelioma enlarges in early childhood and then partially regresses after 2 years of age into mid childhood. Usually, there is residual tumor and fibrosis that causes chronic pain and stiffness.28 Kaposiform hemangioendothelioma also has a lymphatic component, which stains positive for the lymphatic marker D2-40.25 First-line treatment is vincristine to control Kasabach-Merritt phenomenon and pain; resection is rarely possible because the tumor involves multiple tissue planes and important structures.29 Lipofibromatosis is a rare, slow-growing neoplasm that, when diffuse, can cause enlargement of the lower limb.30,31 It is not aggressive and does not metastasize. The leg usually is enlarged at birth or by early childhood; subcutaneous fatty over- growth is the predominant finding. Lipofibromatosis can involve the subfacial compartments and cause bony overgrowth; the foot may be spared. Diagnosis is confirmed by histopathologic examination showing abundant adipose tissue, spindled fibroblasts, focal fascicular growth, and limited mitotic activity.30,31 Suction-assisted lipectomy can improve limb contour.31 Posttraumatic swelling is erroneously labeled lymphedema in some children. Prolonged edema of the lower extremity can occur following injury, particularly after a severe sprain or fracture. Unlike lymphedema, the lymphatic function of the extremity is normal. If the diagnosis is equivocal, lymphoscintigraphy will demonstrate intact lymphatic flow. Some patients will have a ligamentous tear or small fracture that can be identified by plain film and/or magnetic resonance imaging. Rarely, rheumatologic disorders can cause chronic lower extremity swelling in children. Lymphedema and other conditions are ruled out by lymphoscintigraphy and magnetic resonance imaging. If there is no history of trauma and no other potential cause of the swelling can be 1577 Plastic and Reconstructive Surgery • April 2011 Fig. 6. Example of a child with hemihypertrophy with a referring diagnosis of lymphedema. (Left) An 11-year-old boy with right lower extremity enlargement present since birth. History and physical examination potentially were consistent with lymphedema. (Right) Axial pilot magnetic resonance imaging scan demonstrated overgrowth of the lower extremity, including subcutaneous fat, muscle, and bone. Because lymphedema affects only the skin and subcutaneous tissue, and a vascular abnormality was not present, hemihypertrophy was diagnosed. Fig. 7. Examples of patients with tumors erroneously labeled as lymphedema on referral. (Left) A 3-month-old with a reticular infantile hemangioma of the left lower extremity that appeared shortly after birth. The red appearance of the skin and rapid postnatal progression were inconsistent with lymphedema but typical for infantile hemangioma. (Center) A 3-month-old with kaposiform hemangioendothelioma diagnosed by history, physical examination, and laboratory findings. The patient suffered from diffuse discoloration of the extremity, bruising, and thrombocytopenia, which do not occur with lymphedema. (Right) A 5-year-old with lipofibromatosis. History and physical examination possibly were consistent with lymphedema. Because imaging studies were inconclusive, biopsy specimens were obtained and the diagnosis was made histopathologically. 1578 ⫾ Unilateral/bilateral ⫹ ⫾ ⫺ ⫺ ⫹ 1 Subcutaneous adipose/edema Diagnostic histopathology ⫺ Management Compression, operative Familial transmission Laterality Foot/hand involvement Cutaneous changes Abnormal blood tests Risk for Wilms tumor Lymphoscintigraphy MRI findings M, male; F, female; MRI, magnetic resonance imaging; ⫹, with; ⫺, without; ⫾, with or without; 1, increased. *Capillary malformation, lymphatic malformation, venous malformation, combined vascular malformation (e.g., lymphatic-venous malformation, Klippel-Trenaunay syndrome, Parkes Weber syndrome, CLOVES syndrome). †Infantile hemangioma, kaposiform hemangioendothelioma, lipofibromatosis. ‡Posttraumatic, rheumatologic, and systemic fluid overload (e.g., cardiac, hepatic, renal disease). M⫽F Infancy/childhood/ adolescence ⫺ ⫾ ⫺ ⫺ ⫺ Unilateral Bilateral Unilateral Unilateral Unilateral/bilateral ⫾ ⫺ ⫾ ⫾ ⫾ ⫹ ⫺ ⫹ ⫺ ⫺ ⫾ ⫺ ⫾ ⫺ ⫾ ⫺ ⫺ ⫺ ⫹ ⫺ ⫺ ⫺ ⫺ ⫺ ⫺ Abnormal vasculature 1 Subcutaneous Tumor-specific 1 Adipose/muscle/bone 1 Subcutaneous/ adipose (enhancing lesion) (normal vasculature) subfascial edema ⫹ ⫺ ⫹ ⫺ ⫺ Sclerotherapy, Operative Pharmacotherapy, Wilms tumor screening, Treat underlying embolization, operative operative condition operative M⫽F Infancy M⫽F Infancy F Adolescence Hemihypertrophy Tumor† Lipedema Vascular Malformation* M⫽F M⫽F Infancy/adolescence Infancy Male-to-female incidence Onset Fig. 8. An infant with CLOVES syndrome, an additional cause of lower extremity asymmetry in children, diagnosed by physical examination. Foot anomalies and lipomatosis of the trunk do not occur with lymphedema. Lymphedema CONCLUSIONS Approximately one-fourth of pediatric patients with a large lower extremity are misdiagnosed as having lymphedema. The most commonly confused causes are other types of vascular anomalies, lipedema, and hemihypertrophy. Although history and physical examination usually are sufficient to differentiate lymphedema from other conditions, lymphoscintigraphy and/or magnetic resonance imaging may be necessary if the cause is unclear (Table 2 and Fig. 9). If lymphedema is suspected, a lymphoscintigram is Table 2. Typical Characteristics of Conditions Causing Lower Extremity Enlargement in the Pediatric Age Group identified, children are referred for rheumatologic consultation. Additional conditions may cause lower extremity asymmetry in children but were excluded from this study because patients were not erroneously diagnosed with lymphedema (Fig. 8). For example, CLOVES syndrome (congenital lipomatosis overgrowth, vascular malformations, epidermal nevi, and scoliosis) represents a newly described overgrowth disorder.32,33 Rare vascular tumors, such as nonkaposiform hemangioendotheliomas can involve the lower limb. Finally, conditions that reduce the size of one lower extremity, such as hemiatrophy, may cause the contralateral limb to appear enlarged. Nonspecific Edema‡ Volume 127, Number 4 • Pediatric Lower Limb Enlargement 1579 Plastic and Reconstructive Surgery • April 2011 Fig. 9. Diagnostic algorithm for pediatric lymphedema. the first imaging test ordered. A patient thought to have a condition other than lymphedema on history and physical examination usually undergoes magnetic resonance imaging evaluation to confirm the suspected diagnosis and/or to define the extent of disease. Magnetic resonance imaging also is commonly used as a secondary imaging study if lymphoscintigraphy is negative. Correct diagnosis is important because the natural history and management of lymphedema are very different compared with other lower extremity diseases in children. Arin K. Greene M.D., M.M.Sc. Department of Plastic Surgery Vascular Anomalies Center Children’s Hospital Boston 300 Longwood Avenue Boston, Mass. 02115 arin.greene@childrens.harvard.edu ACKNOWLEDGMENT The authors thank David Zurakowski, Ph.D., for statistical expertise. REFERENCES 1. Brorson H. Adipose tissue in lymphedema: The ignorance of adipose tissue in lymphedema. Lymphology 2004;37:175–177. 2. Gloviczki P, Calcagno D, Schirger A, et al. Noninvasive evaluation of the swollen extremity: Experiences with 190 lymphoscintigraphic examinations. J Vasc Surg. 1989;9:683–689; discussion 690. 3. Miller TA, Wyatt LE, Rudkin GH. Staged skin and subcutaneous excision for lymphedema: A favorable report of longterm results. Plast Reconstr Surg. 1998;102:1486–1498; discussion 1499–1501. 1580 4. Brorson H, Svensson H. Liposuction combined with controlled compression therapy reduces arm lymphedema more effectively than controlled compression therapy alone. Plast Reconstr Surg. 1998;102:1058–1067; discussion 1068. 5. Greene AK, Slavin SA, Borud L. Treatment of lower extremity lymphedema with suction-assisted lipectomy. Plast Reconstr Surg. 2006;118:118e–121e. 6. Brorson H, Ohlin K, Olsson G, Svensson B, Svensson H. Controlled compression and liposuction treatment for lower extremity lymphedema. Lymphology 2008;41:52–63. 7. Boon LM, Mulliken JB, Enjolras O, Vikkula M. Glomuvenous malformation (glomangioma) and venous malformation: Distinct clinicopathologic and genetic entities. Arch Dermatol. 2004;140:971–976. 8. Limaye N, Wouters V, Uebelhoer M, et al. Somatic mutations in angiopoietin receptor gene TEK cause solitary and multiple sporadic venous malformations. Nat Genet. 2009; 41:118–124. 9. Kubiena HF, Liang MG, Mulliken JB. Genuine diffuse phlebectasia of Bockenheimer: Dissection of an eponym. Pediatr Dermatol. 2006;23:294–297. 10. Hein KD, Mulliken JB, Kozakewich HP, Upton J, Burrows PE. Venous malformations of skeletal muscle. Plast Reconstr Surg. 2002;110:1625–1635. 11. Upton J, Coombs CJ, Mulliken JB, Burrows PE, Pap S. Vascular malformations of the upper limb: A review of 270 patients. J Hand Surg Am. 1999;24:1019–1035. 12. Irrthum A, Karkkainen MJ, Devriendt K, Alitalo K, Vikkula M. Congenital hereditary lymphedema caused by a mutation that inactivates VEGFR3 tyrosine kinase. Am J Hum Genet. 2000;67:295–301. 13. Irrthum A, Devriendt K, Chitayat D, et al. Mutations in the transcription factor gene SOX18 underlie recessive and dominant forms of hypotrichosis-lymphedema-telangiectasia. Am J Hum Genet. 2003;72:1470–1478. 14. Finegold DN, Kimak MA, Lawrence EC, et al. Truncating mutations in FOXC2 cause multiple lymphedema syndromes. Hum Mol Genet. 2001;10:1185–1189. Volume 127, Number 4 • Pediatric Lower Limb Enlargement 15. Alders M, Hogan BM, Gjini E, et al. Mutations in CCBE1 cause generalized lymph vessel dysplasia in humans. Nat Genet. 2009;41:1272–1274. 16. Brouillard P, Vikkula M. Genetic causes of vascular malformations. Hum Mol Genet. 2007;16:R140–R149. 17. Revencu N, Boon LM, Mulliken JB, et al. Parkes Weber syndrome, vein of Galen aneurysmal malformation, and other fast-flow vascular anomalies are caused by RASA1 mutations. Hum Mutat. 2008;29:959–965. 18. Rudkin GH, Miller TA. Lipedema: A clinical entity distinct from lymphedema. Plast Reconstr Surg. 1994;94:841–847; discussion 848–849. 19. Ballock RT, Wiesner GL, Myers MT, Thompson BH. Hemihypertrophy: Concepts and controversies. J Bone Joint Surg Am. 1997;79:1731–1738. 20. Greene AK, Kieran M, Burrows PE, Mulliken JB, Kasser J, Fishman SJ. Wilms tumor screening is unnecessary in KlippelTrenaunay syndrome. Pediatrics 2004;113:e326–e329. 21. Mulliken JB, Marler JJ, Burrows PE, Kozakewitch HP. Reticular infantile hemangioma of the limb can be associated with ventral-caudal anomalies, refractory ulceration, and cardiac overload. Pediatr Dermatol. 2007;24:356–362. 22. Zukerberg LR, Nickoloff BJ, Weiss SW. Kaposiform hemangioendothelioma of infancy and childhood: An aggressive neoplasm associated with Kasabach-Merritt syndrome and lymphangiomatosis. Am J Surg Pathol. 1993;17:321–328. 23. Kasabach H, Merritt K. Capillary hemangioma with extensive purpura: Report of a case. Am J Dis Child. 1940;59:1063–1070. 24. Lyons LL, North PE, Mac-Moune Lai F, Stoler H, Folpe AL, Weiss SW. Kaposiform hemangioendothelioma: A study of 33 cases emphasizing its pathologic, immunophenotypic, and biologic uniqueness from juvenile hemangioma. Am J Surg Pathol. 2004;28:559–568. 25. Debelenko LV, Perez-Atayde AR, Mulliken JB, Liang MG, Archibald TH, Kozakewitch HP. D2-40 immunohistochemical 26. 27. 28. 29. 30. 31. 32. 33. analysis of pediatric vascular tumors reveals positivity in kaposiform hemangioendothelioma. Mod Pathol. 2005;18:1454–1460. Mulliken JB, Anupindi S, Ezekowitz RA, Mihm MC Jr. Case records of the Massachusetts General Hospital. Weekly clinicopathological exercises. Case 13-2004. A newborn girl with a large cutaneous lesion, thrombocytopenia, and anemia. N Engl J Med. 2004;350:1764–1775. Sarkar M, Mulliken JB, Kozakewich HP, Robertson RL, Burrows PE. Thrombocytopenic coagulopathy (Kasabach-Merritt phenomenon) is associated with Kaposiform hemangioendothelioma and not with common infantile hemangioma. Plast Reconstr Surg. 1997;100:1377–1386. Enjolras O, Mulliken JB, Wassef M, et al. Residual lesions after Kasabach-Merritt phenomenon in 41 patients. J Am Acad Dermatol. 2000;42:225–235. Karnes JC, Lee BT, Phung T, Alomari AI, Mulliken JB, Greene AK. Adult-onset kaposiform hemangioendothelioma in a posttraumatic site. Ann Plast Surg. 2009;62:456–458. Fetsch JF, Miettinen M, Laskin WB, Michal M, Enzinger FM. A clinicopathologic study of 45 pediatric soft tissue tumors with an admixture of adipose tissue and fibroblastic elements, and a proposal for classification as lipofibromatosis. Am J Surg Pathol. 2000;24:1491–1500. Greene AK, Karnes J, Padua HM, Schmidt BA, Kasser JR, Labow BI. Diffuse lipofibromatosis of the lower extremity masquerading as a vascular anomaly. Ann Plast Surg. 2009; 62:703–706. Sapp JC, Turner JT, van de Kamp JM, van Dijk FS, Lowry RB, Biesecker LG. Newly delineated syndrome of congenital lipomatous overgrowth, vascular malformations, and epidermal nevi (CLOVE syndrome) in seven patients. Am J Med Genet A. 2007;143A:2944–2958. Alomari AI. Characterization of a distinct syndrome that associates complex truncal overgrowth, vascular, and acral anomalies: A descriptive study of 18 cases of CLOVES syndrome. Clin Dysmorphol. 2009;18:1–7. Contacting the Editorial Office To reach the Editorial Office, please use the following contact information: Plastic and Reconstructive Surgery威 Rod J. Rohrich, M.D., Editor-in-Chief UT Southwestern Medical Center 5959 Harry Hines Boulevard POB1, Suite 300 Dallas, Texas 75390-8820 Tel: 214-645-7790 Fax: 847-709-7534 E-mail: rjreditor_prs@plasticsurgery.org 1581