A pacemaker primer - American Nurse Today
advertisement

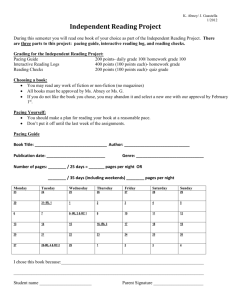
beat The goes on: A pacemaker primer Whether temporary or permanent, single- or dual-chamber, pacemakers optimize cardiac output and improve quality of life. By Nicolette C. Mininni, MEd, RN, CCRN NEARLY 400,000 cardiac pacemakers and cardioverter-defibrillators are implanted annually in the United States. In some cases, pacemakers are used as a temporary intervention to support a patient through an acute episode. In other situations, as for patients with permanent conditions that require cardiac pacing, pacemakers are implanted surgically. Whether temporary or permanent, a pacemaker generates an electrical impulse that travels via one or more leadwires, or leads, which in turn stimulate the myocardium to depolarize and initiate a contraction. A pacemaker’s primary function is to keep the ventricles beating at a rate that maintains sufficient blood pressure and perfuses all organs adequately. Pacemaker components The main parts of a pacemaker are the pulse generator, which contains the power source (typically a lithiumiodide battery and a small electronic circuit), leads, and electrodes at the terminal ends of the leads. Electrodes may be unipolar or bipolar. • Bipolar electrodes are located on the same lead. Once the electrode is implanted in the myocardium, the impulse travels to the negative electrode at the tip of the lead, where it stimulates the myocardium. Then the current flows back to the positive electrode to complete the circuit. Compared to unipolar electrodes, bipolar electrodes are less easily affected by outside electrical ac26 American Nurse Today tivity, including skeletal muscle contractions and magnetic fields. • With a unipolar electrode, a negative electrode is located at the distal tip of the lead and the positive electrode is located at the pulse generator. Unipolar electrodes are more sensitive to myocardial electrical activity. CE 1.6 contact hours L EARNING O BJECTIVES 1. Differentiate temporary and permanent pacemakers. 2. Describe how to interpret rhythm strips of a patient with a pacemaker. 3. Identify a system for pacemaker codes. The author and planners of this CNE activity have disclosed no relevant financial relationships with any commercial companies pertaining to this activity. See the last page of the article to learn how to earn CE credit. Volume 7, Number 3 Single-chamber vs. dualchamber pacemakers Single-chamber pacemakers are used primarily to pace the ventricle when the patient’s underlying rhythm is atrial fibrillation or another atrial arrhythmia. Temporary single-chamber pacemakers most commonly are used in emergencies when temporary pacing is required. If the patient has an atrial arrhythmia, the lead for a single-chamber pacemaker is placed in the right ventricle. If the patient has intact atrioventricular (AV) conduction with a slow heart rate, the lead is placed in the right atrium. Dual-chamber pacemakers—the most commonly implanted pacemaker type—have two leads. The pulse generator is implanted in the chest wall; one lead is implanted in the right atrium and the other in the right ventricle. The pacemaker then maintains synchrony between the atria and ventricles. Dual-chamber pacemakers are used to treat AV node dysfunction, acquired AV blocks, and advanced second- and third-degree heart blocks in adults, as well as chronic bifascicular blocks. Pacemaker codes Many clinicians use the North American Society for Pacing and Electrophysiology/British Pacing and Electrophysiology Group (NASPE/BPEG) generic code for Antibradycardia, Adaptive-Rate Pacing, and Multisite Pacing. This system describes pacemaker and automatic implantable cardioverter-defibrillator settings. www.AmericanNurseToday.com NASPE/BPEG generic code for pacemakers (See NASPE/BPEG generic code for pacemakers.) Temporary pacemakers Temporary pacing is indicated when the heart rate must be increased urgently or as a preventive measure— for instance, in postoperative cardiac surgery patients. Right coronary artery myocardial infarction (MI) commonly causes bradycardic arrhythmias due to lack of blood flow to the sinoatrial node. In a large percentage of individuals, the right coronary artery also perfuses the AV node. Many drugs, including diltiazem, digitalis, and beta blockers, slow the heart rate and in toxic doses may cause symptomatic bradycardia. These conditions may call for temporary pacing. Normally, all types of temporary pacing are demand pacing, in which the pacemaker delivers electrical current only when the heart’s intrinsic rate falls below the preset rate. The three types of temporary pacing are transcutaneous, transvenous, and epicardial. Transcutaneous pacing Transcutaneous pacing is used in the most urgent situations. The American Heart Association’s Advanced Cardiac Life Support Guidelines recommend noninvasive transcutaneous pacing (NTP) for hemodynamically unstable bradycardia. When used for symptomatic bradycardia, NTP is a Class I recommendation—always acceptable, unquestionably safe, and definitely useful. NTP also is recommended to ready a patient for pacing if needed. For example, if a patient has the potential to develop a heart block (as after an MI), transcutaneous pacing pads are placed on the patient so pacing can begin if symptomatic bradycardia develops. Today, most defibrillators have a temporary pacing function. With NTP, one large pacing pad is placed on the patient’s chest wall and another on the back; both are attached to the defibrillator set in the pacing mode. (See www.AmericanNurseToday.com The North American Society for Pacing and Electrophysiology/British Pacing and Electrophysiology Group (NASPE/BPEG) generic code for Antibradycardia, AdaptiveRate Pacing, and Multisite Pacing has five letters (positions), indicated by Roman numerals in the table below. • The first letter of the code identifies which heart chamber is being paced. • The second letter identifies the chamber where intrinsic electrical activity is being sensed. • The third letter indicates the pacemaker’s response to what it senses. A VVI pacemaker, for instance, paces and senses the ventricle; when it senses ventricular activity, it inhibits firing. • The fourth letter tells whether the pacemaker’s rate is modulated. A rate-modulated pacemaker increases the pacing rate to ensure the heart rate can meet the greater cardiac output demanded by increased activity. • The fifth letter refers to the pacemaker’s multisite pacing settings or biventricular pacing setting. I II III IV V Chamber(s) paced Chamber(s) sensed Response to sensing Rate modulation Multisite pacing O = None O = None O = None O = None O = None A = Atrium A = Atrium T = Triggered R = Rate modulation A = Atrium V = Ventricle V = Ventricle I = Inhibited V = Ventricle D = Dual (A+V) D = Dual (A+V) D = Dual (T+I) D = Dual (A+V) Bernstein AD, Daubert JC, Fletcher RD et al. The Revised NASPE/BPEG generic code for antibradycardia, adaptive-rate, and multisite pacing. North American Society of Pacing and Electrophysiology/British Pacing and Electrophysiology Group. Pacing Clin Electrophysiol. 2002 (Feb);25(2):260-4. NASPE/BPEG implanted cardioverter-defibrillator code The short form of the NASPE/BPEG generic pacemaker code describes the response of an implanted cardioverter-defibrillator (ICD) to sensing. ICD-S: ICD with shock capability only ICD-B: ICD with bradycardia pacing as well as shock capability ICD-T: ICD with tachycardia and bradycardia pacing, plus shock capability Pad placement for temporary transcutaneous pacing.) When the patient’s heart rate falls below the programmed rate, the NTP fires or paces the myocardium through the chest wall. The amount of milliamperes (mA) required to stimulate the myocardium through the chest wall is higher than when an electrode is placed directly on the myocardium; for NTP, up to 200 mA may be used. Because NTP may be uncomfortable for patients who are awake, sedation and analgesia should be used if possible. With NTP, electrocardiograph (ECG) leads are attached to the patient to sense a QRS complex, which represents ventricular depolarization. Like other ventricular demand pace- makers (which may be temporary or permanent), an NTP fires only when the intrinsic heart rate falls below a set rate. When it senses a QRS complex, it inhibits firing. (See Evaluating pacemaker rhythm strips.) Transvenous pacing Transvenous pacing is used after the recommended 12 hours of continuous or 24 hours of intermittent transcutaneous pacing have elapsed. It’s also used as a bridge to permanent pacemaker implantation. A leadwire is guided through the vascular system to the myocardium and attached to a cable that connects to the pulse generator. Transvenous pacing is relatively March 2012 American Nurse Today 27 Pad placement for temporary transcutaneous pacing Front Back around the tips of the pacing wires, affecting capture and sensing. When this happens, the mA setting may have to be raised to achieve capture and the sensitivity setting may have to be lowered to achieve sensing. The patient’s fluid and electrolyte status also influences the ability to pace and sense properly. Pacing of both the atria and ventricles (dualchamber pacing) maintains cardiac synchrony and optimizes preload and cardiac output. Permanent pacemakers Temporary transcutaneous pacing is used in emergencies. The pads can be placed quickly so pacing can begin immediately. Most defibrillators have a temporary pacing option, with multifunctional pads that can be used for temporary pacing or defibrillation. Reprinted with permission from Zoll Medical. comfortable for the patient. The pacemaker rate can be set at a low of 40 to 60 paced beats; the pacemaker fires when the rate drops below the set rate. In some models, the rate can be set for up to 110 beats/minute. Transvenous pacemakers have built-in sensing to identify ventricular depolarization. A temporary transvenous pacemaker may be set between 0 and 20 mA; the average setting is 10 mA. The pulse generator’s sensitivity settings allow the generator to “see” intrinsic myocardial activity more clearly. Sensitivity should be set so the pulse generator can “see” intrinsic P and QRS waves, which appear on the ECG and are measured in millivolts (mV). An initial ventricular sensitivity setting of 2 to 5 mV is the recommended starting point for ventricular pacing. If sensitivity is set too high, electrical activity won’t be “seen” and the pacemaker will fire—a phenomenon called undersensing or failure to sense. If sensitivity is set too low, the pacemaker may recognize electrical artifacts, such as muscle movements, and will fail to fire; this is known as oversensing. In some patients, two pacing leads may be placed—one in the atrium and the other in the ventricle. When programmed for AV sequential pacing, 28 American Nurse Today the pacemaker is used to increase cardiac output by maintaining the heart’s natural cycle (atrial contraction followed by ventricular contraction). Additional settings for AV sequential pacing include sensitivity for atrial pacing and the AV interval (the interval between atrial pacing and ventricular pacing). For atrial pacing, the average setting is 0.5 mV (which is lower than ventricular sensitivity because the P wave is smaller than the QRS complex). In a normal heart, the AV interval is about 200 milliseconds. Pacemaker AV intervals can be set to mimic the patient’s normal PR interval. Epicardial pacing Epicardial pacing is used only with cardiac surgery patients. Common postoperative complications of cardiac valve surgery and coronary artery bypass surgery include episodic sinus bradycardia, second- and thirddegree heart block, and asystole. During the intraoperative period, epicardial pacing wires are attached to the epicardium, passed through the chest wall, and attached to a cable connected to the pacemaker’s pulse generator. Epicardial pacemaker settings are similar to transvenous pacemaker settings. An endothelial sheath may form Volume 7, Number 3 Permanent pacemakers are implanted during a short surgical procedure. The pulse generator is placed in a subcutaneous pocket created in the chest wall—usually on the upper left part of the chest below the clavicle. Then the pulse generator is attached to leads, which are threaded through the vascular system to the heart and implanted into the myocardial wall. The atrial electrode is implanted in the right atrium near the coronary sinus; the ventricular electrode, near the right ventricular apex. Currently, most implanted pacemakers are dual-chamber pacemakers; about one-third have cardioversion-defibrillation settings. Implanted cardioverterdefibrillator (ICD) use is approved as a first-line treatment for patients at risk for ventricular tachycardia or ventricular fibrillation. Permanent pacemakers are used to treat various bradycardic arrhythmias. (See Permanent pacemaker indications.) Usually, patients are evaluated for bradycardia based on ECG records from 24-hour or Holter monitoring. Biventricular pacing Also called cardiac resynchronization therapy, biventricular pacing is indicated for patients with heart failure, dilated cardiomyopathy, prolonged ventricular conduction, or a reduced ejection fraction. Asynchronous activation of the heart chambers (indicated by a QRS duration greater than 0.13 seconds) is linked to worsening www.AmericanNurseToday.com Evaluating pacemaker rhythm strips When evaluating a pacemaker rhythm strip, first locate the P wave, QRS complex, and T wave. Then look for atrial and ventricular pacing spikes. These spikes may appear as a positive or negative deflection; they may be very small (less than 0.2 mV) or very large (more than 10 mV). Instead of measuring the PR interval as you would with a normal electrocardiographic waveform, measure the atrioventricular interval. Finally, assess for proper sensing. Ventricular demand pacing (VVI) failure to capture. Common causes of failure to capture include a weak pulse-generator battery, loose connections, a fractured lead, and an increased pacing threshold. An increased threshold can result from fibrosis or edema at the lead implantation site, metabolic changes, and electrolyte abnormalities. The patient may experience such signs and symptoms as hypotension, syncope, light-headedness, and confusion. A VVI pacemaker paces and senses the ventricle. Note the pacing spike preceding the QRS complex; the third QRS complex isn’t preceded by a pacing spike and looks different from paced QRS complexes because it’s an intrinsic waveform. When this pacemaker senses an intrinsic QRS complex, it’s inhibited from firing (as denoted by the “I” in VVI). Failure to pace AV sequential pacing Atrioventricular (AV) sequential pacing is often called DDD pacing because it senses and paces both the atria and ventricles. The third D refers to the response to sensing; in this mode, pacemaker activity may be either inhibited or triggered. Note that the two pacing spikes are regular and consistently appear the same distance apart; this is called 100% AV sequential pacing. In this rhythm strip, you can’t assess sensing because no intrinsic activity is occurring. Failure to pace is identified by absent pacemaker activity where it should appear. Causes include a weak battery or a more serious pacemaker problem. To prepare for this situation, keep a noninvasive transcutaneous pacemaker ready. Failure to sense Failure to capture In this strip from a patient receiving ventricular pacing, pacing spikes aren’t always followed by QRS complexes, indicating heart failure and increased morbidity and mortality. A biventricular pacemaker has three leads—one for the atrium and one for each ventricle. Biventricular pacing causes synchronous contraction of both ventricles and improves cardiac output. End-of-life concerns In terminally ill patients and those www.AmericanNurseToday.com Failure to sense may result from inappropriately set sensitivity or mechanical failure, including battery failure, fractured leads, displaced electrodes, or other electrical interference. The rhythm strip shows pacing spikes after the third and fourth QRS complexes, indicating the pacemaker failed to sense and subsequently fired inappropriately. If the pacemaker fires during ventricular repolarization, life-threatening ventricular arrhythmias may arise. who’ve opted to forgo further resuscitative efforts, pacemakers with ICD functionality may interfere with the natural process of dying by continuing to function and delivering shocks. As the end of the patient’s life approaches, the patient and family should discuss with healthcare providers whether the ICD function should be discontinued. If you’re caring for a monitored hospital patient with a pacemaker, remember that the ECG will continue to show pacing spikes and possible electrical activity without a pulse. This could cause confusion in family members at the bedside, so the healthcare team should consider monitoring the patient remotely. March 2012 American Nurse Today 29 Left subclavian vein Superior vena cava pacing. North American Society of Pacing and Electrophysiology/British Pacing and Electrophysiology Group. Pacing Clin Electrophysiol. 2002 (Feb);25(2):260-4. Chow WC, Buxton AE. Implantable Cardiac Pacemakers and Defibrillators: All You Wanted to Know. Malden, MA: Blackwell Publishing, Inc; 2006. Right atrium Left ventricle Permanent pacemaker indications Patients with the following conditions may be candidates for pacemakers. • Sinus node dysfunction: persistent sinus bradycardia, atrial fibrillation with sinus node dysfunction, chronotropic incompetence, sinus arrest, tachy-brady syndrome, sick sinus syndrome • Atrioventricular (AV) node dysfunction • Acquired AV blocks in adults: post-myocardial infarction • Chronic bifascicular block • Hypersensitive carotid sinus syndrome • Neurocardiogenic syncope • Prevention of atrial arrhythmias: atrial tachyarrhythmias, prolonged QT syndrome. • • • • Special conditions that may call for pacing include: heart transplantation neuromuscular disease sleep apnea syndrome cardiac sarcoidosis. Biventricular pacing and cardiac resynchronization therapy may be indicated for patients with low ejection fraction or cardiomyopathy. Pediatric indications Pacemakers may be indicated for children and adolescents with congenital heart disease, including advanced heart block, sinus node dysfunction, atrial tachyarrhythmias, and sinus bradycardia. ECG Interpretation: An Incredibly Visual! Pocket Guide. Philadelphia, PA: Lippincott Williams & Wilkins; 2009. Epstein AE, DiMarco JP, Ellenbogen KA, et al. ACC/AHA/HRS 2008 Guidelines for DeviceBased Therapy of Cardiac Rhythm Abnormalities: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Writing Committee to Revise the ACC/AHA/NASPE 2002 Guidelines Update for Implantation of Cardiac Pacemakers and Antiarrhythmic Devices) developed in collaboration with the American Association of Thoracic Surgery and Society of Thoracic Surgeons. J Am Coll Cardiol. 2008 May 27;51(21);e1-62. Erratum in: J Am Coll Cardiol. 2009 Apr 21;53(16):1473. J Am Coll Cardiol. 2009 Jan 6;53(1):147. Field JM, Hazinski MF, Sayre MR, et al. 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care Science. Circulation. 2010;122(suppl 3):S640-656. http:// circ.ahajournals.org/content/122/18_suppl_3 .toc. Accessed January 30, 2012. Indications for use of non-invasive transcutaneous pacing. Resuscitation Central. www .resuscitationcentral.com/pacing/indications. Accessed January 30, 2012. Cardioverter-defibrillator indications Jackson A. An overview of permanent cardiac pacing. Nurs Stand. 2010 Nov 24-30; 25(12):47-57. A permanent pacemaker with a cardioverter-defibrillator may be used for secondary prevention in sudden cardiac death survivors or for cardiomyopathy, as well as for patients with genetic arrhythmia syndromes and long QT syndrome. Runge MS, Stouffer GA, Patterson C. Netter’s Cardiology (Netter Clinical Science). 2nd ed. Philadelphia, PA: Saunders; 2010. What the future may hold Experts predict that permanent pacemakers of the future will be much smaller—about the size of a large grain of rice—and will be implanted intravascularly, not surgically. What’s more, the pulse generator will be seated directly into the myocardium without leads. For children, this means fewer surgeries to replace leads in a growing body. For adults, benefits include the possibility of fewer lead fractures and less lead displacement. 30 American Nurse Today Each year, the number of patients who receive permanent pacemakers grows. Although pacemaker technology is changing constantly, the goal of therapy remains the same—to sustain the heart rate and improve AV synchrony, thus optimizing cardiac output and improving the patient’s quality of life. ✯ Russo JE. Original research: deactivation of ICDs at the end of life: a systemic review of clinical practices and provider and patient attitudes. Am J Nurs. 2011 Oct:111(10):26-35. Scheibly K. Systematic assessment of basic pacemaker function. AACN Adv Crit Care. 2010 Jul-Sep:21(3);322-8. The eleven most implanted medical devices in America. 24/7 Wall St. Wire. July 18, 2011. http://247wallst.com/2011/07/18/the-elevenmost-implanted-medical-devices-in-america/2/. Accessed January 30, 2012. Visit www.AmericanNurseToday.com/Archives .aspx for a glossary of pacemaker terms. Selected references Bernstein AD, Daubert JC, Fletcher RD, et al. The Revised NASPE/BPEG generic code for antibradycardia, adaptive-rate, and multisite Volume 7, Number 3 Nicolette C. Mininni is an advanced practice nurse in critical care at UPMC Shadyside in Pittsburgh, Pennsylvania. www.AmericanNurseToday.com CE POST-TEST • The beat goes on: A pacemaker primer Earn contact hour credit online at www.americannursetoday.com/ContinuingEducation.aspx (ANT120101) Instructions To take the post-test for this article and earn contact hour credit, please go to www.AmericanNurseToday.com/ContinuingEducation.aspx. Simply use your Visa or MasterCard to pay the processing fee. (ANA members $15; nonmembers $20.) Once you’ve successfully passed the post-test and completed the evaluation form, you’ll be able to print out your certificate immediately. Provider accreditation The American Nurses Association Center for Continuing Education and Professional Development is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation. ANA is approved by the California Board of Registered Nursing, Provider Number 6178. Contact hours: 1.6. Expiration: 12/31/14 Post-test passing score is 75%. Please mark the correct answer online. 1. Which statement about unipolar pacemaker electrodes is correct? a. The negative electrode is located at the distal tip of the lead and the positive electrode at the pulse generator. b. The positive electrode is located at the distal tip of the lead and the negative electrode at the pulse generator. c. Unipolar electrodes are less sensitive than bipolar electrodes to myocardial electrical activity. d. Unipolar electrodes are less easily affected than bipolar electrodes by skeletal muscle contractions. 2. A single-chamber pacemaker typically is used for a patient with: a. chronic bifascicular heart block. b. acquired atrioventricular heart block. c. advanced third-degree heart block. d. an emergency need for pacing. 3. Which type of temporary pacing would most likely be chosen for a patient with hemodynamically unstable bradycardia? a. Epicardial pacing b. Endocardial pacing c. Noninvasive transcutaneous pacing (NTP) d. Biventricular pacing 4. Which type of temporary pacing usually is used for a patient having major cardiac surgery? a. Epicardial pacing b. Transvenous pacing c. NTP d. Biventricular pacing 5. For a patient with dilated cardiomyopathy, which type of pacing should you anticipate? a. Epicardial pacing b. Transvenous pacing c. NTP d. Biventricular pacing 6. The average setting for a temporary transvenous pacemaker is: a. 2 mA. b. 300 mA. c. 200 mA. d. 10 mA. www.AmericanNurseToday.com CE: 1.6 contact hours ANA Center for Continuing Education and Professional Development’s accredited provider status refers only to CNE activities and does not imply that there is real or implied endorsement of any product, service, or company referred to in this activity nor of any company subsidizing costs related to the activity. This CNE activity does not include any unannounced information about off-label use of a product for a purpose other than that for which it was approved by the Food and Drug Administration (FDA). The planners of this CNE activity have disclosed no relevant financial relationships with any commercial companies pertaining to this CNE. P URPOSE / GOAL To provide the information nurses need to deliver optimal care for patients with pacemakers L EARNING O BJECTIVES 1. Differentiate temporary and permanent pacemakers. 2. Describe how to interpret rhythm strips of a patient with a pacemaker. 3. Identify a system for pacemaker codes. 7. Up to how many milliamperes can be used with an NTP? a. 2 mA b. 300 mA c. 200 mA d. 10 mA 8. Your patient’s pacemaker is recognizing electrical artifacts, such as muscle movements, and isn’t firing. This situation is called: a. undersensing. b. underpacing. c. oversensing. d. overpacing. 9. During a short surgical procedure, the pulse generator of a permanent pacemaker is placed: a. in an intermuscular pocket created in the chest wall—usually on the upper left part of the chest below the clavicle. b. in an intermuscular pocket created in the chest wall—usually on the upper right part of the chest below the clavicle. c. in a subcutaneous pocket created in the chest wall—usually on the upper left part of the chest below the clavicle. d. in a subcutaneous pocket created in the chest wall—usually on the upper right part of the chest below the clavicle. 10. When examining the rhythm strip of a patient with a transvenous pacemaker, you see that the pacing spikes aren’t always followed by QRS complexes. You identify the situation as: a. ventricular demand pacing. b. failure to pace. c. atrioventricular sequential pacing. d. failure to capture. 11. The first letter of the five-letter North American Society for Pacing and Electrophysiology/British Pacing and Electrophysiology Group (NASPE/BPEG) generic code for Antibradycardia, Adaptive-Rate Pacing, and Multisite Pacing indicates: a. which chamber is being paced. b. the pacemaker’s response to sensing. c. rate modulation. d. multisite pacing. 12. A patient’s implanted cardioverterdefibrillator code is ICD-T, which means: a. implanted cardioverter-defibrillator (ICD) with shock capability only. b. ICD with tachycardia and bradycardia pacing, plus shock capability. c. ICD with bradycardia pacing and shock capability. d. ICD with tachycardia pacing and shock capability. 13. What does a DDI pacemaker do? a. It paces and senses the ventricles and atria; when it senses intrinsic activity, it increases firing. b. It paces and senses the atria; when it senses intrinsic activity, it inhibits firing. c. It paces and senses the ventricles and atria; when it senses intrinsic activity, it inhibits firing. d. It paces and senses the ventricles; when it senses intrinsic activity, it inhibits firing. 14. Which statement about a biventricular pacemaker is correct? a. It causes asynchronous contraction of both ventricles. b. It causes synchronous contraction of both atria. c. It has two leads. d. It has three leads. 15. If an endothelial sheath forms around the tips of epicardial pacing wires, which action may be warranted? a. The mA setting may need to be increased and the sensitivity lowered. b. Both the mA setting and sensitivity may need to be decreased. c. The mA setting may need to be decreased and the sensitivity increased. d. Both the mA setting and sensitivity may need to be increased. March 2012 American Nurse Today 31