Senior Design Paper - Department of Electrical and Systems
advertisement

Washington University in St. Louis
School of Engineering and Applied Science
Electrical and Systems Engineering Department
ESE 498
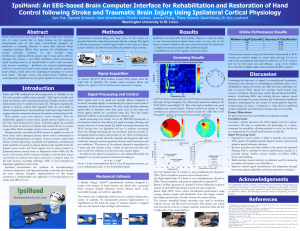
An EEG-based Brain Computer Interface for
Rehabilitation and Restoration of Hand
Control following Stroke Using Ipsilateral
Cortical Physiology
By
Sam B. Fok, Raphael Schwartz, Charles D. Holmes
Supervisor
Eric Leuthardt, David Bundy, Robert Morley
Submitted in Partial Fulfillment of the Requirement for the BSEE Degree,
Electrical and Systems Engineering Department,
School of Engineering and Applied Science,
Washington University in St. Louis
Student Statement
The authors of this report have observed and upheld all codes and ethics, including the
University’s Honor System, and have maintained the integrity of this course in the design and
implementation of this project.
2
Abstract
Stroke and traumatic brain injury (TBI) cause long-term, unilateral loss of motor control due to
brain damage on the opposing (contralateral) side of the body. Conventional neurological
therapies have been found ineffective in rehabilitating upper-limb function after stroke. Brain
computer interfaces (BCIs), devices that tap directly into brain signals, show promise in
providing rehabilitation but remain in research. Also, BCIs cannot work if the target signals have
been eliminated due to injury. Therefore we present a novel BCI, the IpsiHand, which combines
advances in neurophysiology, electronics, and rehabilitation. Recent studies show that during
hand movement, the cortical hemisphere on the same (ipsilateral) side of the body as the hand
also activates. IpsiHand uses electroencephalography (EEG) to record these signals and control a
powered hand orthosis. The undamaged hemisphere can then control both hands, and through
neural plasticity IpsiHand will strengthen ipsilateral neural pathways to enhance ipsilateral motor
control.
Acknowledgements
We would like to especially thank Mark Wronkiewicz, Jessica Zhang, Thane Somers, and
Nathan Brodell who were a part of our design team. We would like to thank Dr. Eric Leuthardt,
our faculty mentor, and David Bundy, our graduate student mentor, for their guidance. We would
also like to thank Joanne Rasch and the Rehabilitation Institute of St. Louis for providing
consumer feedback and expert opinion on current rehabilitation, and Professors Robert Morley
and Joseph Klaesner for instruction during senior design. This work is supported in part by The
National Collegiate Inventors and Innovators Alliance, the Washington University School of
Engineering, and Emotiv Systems.
3
Table of Contents
Student Statement ......................................................................................................................................... 2
Abstract ......................................................................................................................................................... 3
Acknowledgements ....................................................................................................................................... 3
List of Figures ................................................................................................................................................ 5
List of Tables ................................................................................................................................................. 5
Problem Formulation .................................................................................................................................... 6
Problem Statement ................................................................................................................................... 6
Problem Formulation ................................................................................................................................ 6
Project Specifications.................................................................................................................................... 7
Signal Acquisition .................................................................................................................................. 7
Signal Processing ................................................................................................................................... 7
Mechanical Output ............................................................................................................................... 7
System Operation ................................................................................................................................. 7
Concept Synthesis ......................................................................................................................................... 8
Literature Review ...................................................................................................................................... 8
Concept Generation .................................................................................................................................. 9
Concept Reduction.................................................................................................................................. 11
Detailed Engineering Analysis and Design Presentation ............................................................................ 12
Signal Acquisition .................................................................................................................................... 12
Screening Procedure and Signal Processing ........................................................................................... 13
Control Signal Conditioning and Output ................................................................................................. 14
Least Mean Squares Adaptive Filter ....................................................................................................... 15
Performance Analysis ............................................................................................................................. 16
Computational Analysis .......................................................................................................................... 20
Mechanical Orthosis ............................................................................................................................... 21
Cost Analysis ........................................................................................................................................... 22
Lifetime Operation Cost .......................................................................................................................... 23
Hazards and Failure Analysis................................................................................................................... 23
Conclusion .................................................................................................................................................. 24
4
Works Cited................................................................................................................................................. 25
List of Figures
Figure 1 – Differences in power spectrum during A) contralateral movements and B) ipsilateral
movements during movement and rest. Note that contralateral movement shows a decrease in power
at frequencies less than 35Hz and an increase in power between 60 and 120Hz whereas ipsilateral
movements show a decrease in power only at frequencies below 50Hz [9]. .............................................. 8
Figure 2 – Concept of a BCI using ipsilateral signals to restore motor function in hemiplegic stroke
survivors [10]. ............................................................................................................................................... 9
Figure 3 – Orthosis design options.............................................................................................................. 10
Figure 4 - Data acquisition Design Options ................................................................................................. 11
Figure 5 - Structure and data flow of IpsiHand. Processing occurs in three steps: signal acquisition, signal
processing, and mechanical actuation........................................................................................................ 12
Figure 6 - Spatial location of electrodes of Emotiv EPOC headset relative to head ................................... 13
Figure 7 - between left hand movemnet and rest across bins of electrode channel and frequency... 17
Figure 8 - Frequency spectrum of the F3 EEG electrode location during conditions of left hand movement
(red curve) and conditions of rest (blue curve). ......................................................................................... 17
Figure 9 - Topographical color maps of values for 12 Hz and 22 Hz. .................................................... 18
Figure 10 - ROC curves shows classification performance using varying window lengths and thresholds.
.................................................................................................................................................................... 19
Figure 11 – prefabricated hand orthotic fitted with linear actuator for control of finger position ........... 21
List of Tables
Table 1 - Classification accuracy using best threshold as determined by ROC analysis per window length
.................................................................................................................................................................... 20
Table 2 - Bill of Materials ............................................................................................................................ 22
5
Problem Formulation
Problem Statement
In the United States, stroke, traumatic brain injury (TBI), and spinal cord injury (SCI) are the
leading causes of disability affecting over a million individuals annually [1] [2] [3]. About
900,000 individuals have reported severe trouble with hand function [4], and conventional
physical therapy produces little significant improvement after 3 months post injury [5]. Loss of
hand function causes a severe decrease in quality of life for affected individuals [6]. In addition,
lasting disabilities result in a typical lifetime cost between $100k and $2M per patient, including
inpatient care, rehabilitation, and follow-up [1] [7] [8]. The most effective therapies have patients
actively controlling their limb, which is not an option in cases of severe paralysis. While BCIs
promise new hope for treatment, they remain in the research stage. In addition, conventional
BCIs cannot be applied to cases of brain injury since the classical motor signals in cortex
contralateral to the target limb needed would be gone with the injury.
Problem Formulation
We addressed the problem of applying BCI technology to rehabilitation following stroke and
TBI. To do this we developed a device for rehabilitation that synthesizes recent developments in
neurophysiology, electronics, and physical therapy into a BCI hand orthosis. A recent study
found signals associated with hand movements in cortex ipsilateral to the hand. These signals
were present in cortex anterior to ipsilateral primary motor cortex and at frequencies below 40Hz
[9], which are accessible via EEG. With this knowledge, these intent-to-move signals can be
recorded from the cortex to control an orthosis which opens and closes a patient’s hand. Tactile
and proprioceptive feedback provided from this device will facilitate neural plasticity,
strengthening existing and developing new neural pathways ipsilateral to the affected hand that
will ultimately restore motor control. Allowing the patient to regain hand control with their
thoughts alone should also provide tremendous encouragement in the rehabilitation process.
Our objective is to directly recouple the intent-to-move a hand with hand motion in order to
improve outcomes of recovery, reduce the lifetime cost of brain injury, and improve quality of
life for those affected by stroke or TBI.
6
Project Specifications
Our design will provide the following:
Signal Acquisition
EEG signal recordings at locations corresponding to the International 10-20 EEG
standard, specifically with locations over the motor and premotor cortex.
Spectral information up to 60 Hz.
Signal Processing
Identification of signal features correlated with intent to open or close the hand.
Extraction of the control signal from the identified electrode location and frequency
band.
Spatial filtering to reduce noise common to the electrode of interest and reference
electrode(s).
Normalization of a control signal from identified features.
Communication with a linear actuator for mechanical output.
An adaptive filter which adjusts the gain of the mechanical output to counteract
changes in the strength of the control signal.
Mechanical Output
Enough force to overcome spasticity and tone imbalance in a patient’s hand (up to
110 N).
Graded extension and flexion of the hand.
System Operation
Real time operation, with latency less than 3 seconds.
Signal classification with an accuracy of at least 70%.
7
Concept Synthesis
Literature Review
Previous study by Wineski, et. al., discovered differences in cortical signals during contralateral
and ipsilateral movement conditions (Figure 1). Note that this study was conducted with the
electrocorticography (ECoG) technique, in which electrodes are placed directly onto the surface
of the brain. The spatial and temporal resolution afforded by ECoG will be unavailable with the
EEG technique, which is generally limited to less than 60Hz and greater than 2cm temporal and
spatial resolution, respectively [10]. Figure 2 from the same lab illustrates the concept of using
ipsilateral signals in a BCI application to restore limb control. Understanding of this literature
was supported by courses discussing signal processing at Washington University, such as ESE
351, Signals and Systems, ESE 482, Digital Signal Processing, and ESE 488, Signals and
Systems Laboratory.
Figure 1 – Differences in power spectrum during A) contralateral movements and B) ipsilateral movements during movement
and rest. Note that contralateral movement shows a decrease in power at frequencies less than 35Hz and an increase in
power between 60 and 120Hz whereas ipsilateral movements show a decrease in power only at frequencies below 50Hz [9].
8
Figure 2 – Concept of a BCI using ipsilateral signals to restore motor function in hemiplegic stroke survivors [10].
Device-based therapies for rehabilitation exist for both BCI and non-BCI techniques. Patent
application 11/857,881 describes a Nuero-robotic System developed by Myomo, which uses
weak EMG signals of a partially paralyzed stroke patient to coordinate elbow movement with a
motor-driven orthosis [11]. Patent application 12/758,706 describes the system for
“neuromuscular reeducation” developed for Hand Mentor [12]. In using EMG rather than EEG,
both Myomo and Hand Mentor can only be used by patients with significant residual motor
control. From BrainGate, patent application 9/991,498 describes a system that uses neurological
signals to control a device, and application 11/201,283 describes associated biological interface
systems and methods [13] [14]. We differentiate our device from BrainGate by using EEG rather
than invasive single/multiunit recordings and by focusing on intent-to-move signals in the
undamaged ipsilateral cortex.
Concept Generation
There are three major physical components that were considered in the design of Ipsihand: 1) the
mechanical orthosis, 2) the data acquisition, and 3) the linear actuator. There is a fourth
component which is the signal processor, but for this prototype there was nothing considered
other than a laptop. However, it should be noted that there are considerations for the future signal
processing platforms, such as microcomputers and microprocessors.
For the orthosis itself, there were many options to choose from. Options for the orthosis
are illustrated in Figure 3. An initially attractive option was to purchase and modify an existing
9
device. There exist many orthotic splints that have capabilities of joint movement or aide of joint
movement. Particularly, we looked at wrist-driven orthotics. With these devices, it would be very
easy to uncouple the wrist to the hand movement and replace it with a linear actuator. Other
options that came about included already functional actuating orthotics, including devices
implementing functional electrical stimulation. Functional electrical stimulation involves
applying electrical currents to activate nerves and induce muscle contraction. Devices like this
were considered primarily because they would involve less direct connections to the hand and
not require the addition of a linear actuator.
Orthosis
Modify Existing
Device
Wrist-Driven
Orthosis
Dynamic Splint
Continuous Passive
Motion Machine
Use Existing Device
Haptic Feedback
Build from Scratch
Functional Electrical
Stimulation
Figure 3 – Orthosis design options.
For the data acquisiton, there were many commerical options for EEG headsets and
headcaps. Single electrode headsets, such as the Neurosky Mindwave, were inexpensive and
simple. Most had an accesible SDK so development would be relativaley simple. However, a
downside to the simple single elctrode set up is the lack of channels. For this reason, more
expensive, multiple-electrode headsets were also considers. Their advantages included the ability
to do spatial filtering and accesibilty to more than one location of brain. Figure 4 shows an
illustration of all of the options for data acquistion devices.
10
Data Acquistion
Neurosky
Mindwave
Single Electrode
EEG Headset
Star Wars Force
Trainer
MindSet
Multiple Electrode
EEG Headset
Standard Medical
Headcap
Emotiv EPOC
Figure 4 - Data acquisition Design Options
Finally, for the linear actuator, there were a multitude of options online for purchase. All
devices performed essentially the same. The big differences from option to option were the size,
power, and cost of the actuator.
Concept Reduction
In the choice of the orthotic itself, price became a big decision factor. Devices that already hand
motor driven actuation cost well over $1500. In addition, overriding the control of the actuation
would be more complex than programming a separate linear actuator. For these reasons, the
wrist-driven orthosis was chosen. This orthosis, the Becker Oregon Talon
TM
, would eventually
have the bar coupling finger movement to wrist movement removed. This bar would be replaced
by the linear actuator, the Firgelli L16, which would be fastened to the back end of the orthotic.
The L16 was chosen primarily because of its ease of use and its value.
Finally, the Emotiv EPOC was chosen as the data acquisition device. This was for a number of
reasons. The device was a low cost consumer headset, yet it had multiple electrodes, so there was
11
more capability for feature extraction. Additionally, the device came with an easy to use SDK
which had been adapted to work with BCI2000 in a BCI2000 module.
Detailed Engineering Analysis and Design Presentation
Electrical fields produced by synchronous firings of neurons over large areas of the brain are
recorded on the scalp. These signals are then sent to a laptop for processing. The signal is filtered
to generate an output signal, which is then sent to a linear actuator. An orthosis controls the
patient’s finger closure with this linear actuator, so that brainwaves can control the opening and
closing of the hand using a signal route that bypasses damage nerves.
Figure 5 - Structure and data flow of IpsiHand. Processing occurs in three steps: signal acquisition, signal processing, and
mechanical actuation.
Signal Acquisition
EEG signals were acquired from the subject’s scalp using a dry-electrode Emotiv EPOC
(Emotiv; Australia) headset with 14 electrodes located over 10-20 international system positions
AF3, F7, F3, FC5, T7, P7, O1, O2, P8, T8, FC6, F4, F8, and AF4 using 2 reference electrodes
(Figure 6). The headset aligns, bandpass filters, and digitizes the signal at 128 Hz and transmits
wirelessly to a laptop.
12
Figure 6 - Spatial location of electrodes of Emotiv EPOC headset relative to head
Screening Procedure and Signal Processing
On the laptop, signal processing was carried out in the BCI2000 framework, a development
platform written primarily in C++ and MATLAB that allows rapid recording, filtering, and
feature selection of brain signals [15]. Initial screening in which signals are recorded while the
subject makes hand movements is used to determine the EEG features that our algorithm will use
to contrast movement from rest. During this screening procedure the user alternates between
periods of attempted hand movement and periods of rest. After several trials, we identify the
specific electrode channels and frequency bins which consistently changed in power between
hand movement and rest conditions
A bipolar reference scheme, in which a signal is generated by taking the difference between the
signals recorded at pairs of adjacent electrodes [16], at 6-9cm distance is used to attenuate noise
and artifacts on the scalp common to pairwise electrodes. It is also used to detecting signals from
a region consistent in size with the diffuse spatial characteristics of EEG signals [16]. This
reference technique also makes the system resilient to variation in electrode placement, which
happens simply because it is impossible to place the headset in the exact same spot for each
experiment. Five electrodes are available above the frontal lobe and premotor area of the
contralesional hemisphere, the location of our signal of interest. Using these 5 electrodes, all
combinations of spatial reference choices can be evaluated. The coefficient of determination is used as a measure of spatial reference performance, where indicates the proportion of
variability in the signal attributable to the user’s hand movement. The bipolar derivation is
defined,
13
= − (1)
where i = 1…5, j=1…5 refer to the electrode locations of interest and and are the voltage
measurement signals from the electrode i and j respectively. Therefore, is bipolar derivation
of i referenced to j. We evaluate each combination and select for the highest ,
= arg max( { })
(2)
Once the bipolar reference has been selected, the frequency bin of width 2 Hz with the
highest is then selected as the control spectrum. The bipolar spatial filtered recording is then
converted to actuator control signal by BCI2000 and normalized to have a mean of zero and a
unit variance. This normalized control signal is then sent to LabVIEW via a UDP port.
Control Signal Conditioning and Output
For each cycle, a LabVIEW (National Instruments; Austin, TX) program detected whether the
control signal exceeded a threshold. This is determined by:
0
|′| < !
= ′
"#$"
(1)
where ′ is the control signal from BCI2000, ! is the threshold of the system and is termed the
condition control signal. The system is designed such that a positive signal corresponds to the
hand closing and a negative signal corresponds to the hand opening. The signal is condition in
this way so that a user can keep the device stationary by maintaining the signal below threshold.
This conditioned control signal is then used to adjust the position of the linear actuator,
and thus open or close the hand. There are two main approaches to the implementation of this: 1)
the control signal reflects position or 2) the control signal reflects velocity. With the first option,
the control signal would be multiplied by a gain and the product would be the position the linear
actuator would go to. With the second option, the control signal would be multiplied by a gain
and the product would be added to the current position.
14
The second option is implemented because it does not show radical changes in the
position as a result of the stochastic nature of the control signal. This, in turn, makes for
smoother movements of the hand. This velocity based approach can be expressed by
% ′ = %&' + )
(2)
0
% ′ < 0
% = *%+,- % ′ > %+,% ′
"#$"
(3)
where % is the extension length of the linear actuator for iteration /, %+,- is the maximum length
of the linear actuator, ) is the gain, and is the conditioned control signal for iteration /. From
equation (3) we can see that the there is a limit in both directions to how much the linear actuator
can open or close. Though the actuator physically cannot extend past these values, this equation
is included in calculations to avoid bugs.
The actuator position is then changed by writing to the actuator microcontroller via a
USB port. The microcontroller then adjusts the position of the actuator via pulse-width
modulation.
Least Mean Squares Adaptive Filter
The brain is a very mutable object. Patterns that the Ipsihand observes change from trial to trail
and from subject to subject. Because of this, magnitudes of the band of interest can change from
trial to trial.
To counteract this, the Ipsihand implements a Least Mean Squares (LMS) adaptive filter.
The LMS algorithm linearly scales the selected bipolar channel by adjusting the gain. The gain is
adjusted after each trial to values which would have yielded better results in the previous trial.
This is expressed as
)0 = (1 − 2))0&' + 2
(Δ%)
4̅
(1)
15
where )0 is the gain for the kth trial, (Δ%) defines the desired movement for that trial, 4̅ is the
mean value for the input signal 4 in a given trial, and 2, the adaptability constant, determines the
rate of adaption.
Given a gain for trial k-1 and data from the trial, the gain for trial k will be a weighted
average of gain from trial k-1 and a gain that would have resulted in the least amount of error for
trial k-1. The weights are determined by the adaptability constant 2. If 2 is 0, then there is no
change from trial to trial. If 2 is 1, the gain changes without memory of the previous gain values.
Performance Analysis
Our design was tested with three healthy subjects to verify the ability to use non-conventional
signals from the contralesional cortex to control a hand on the same side of the body. We found :
1. Hand
movement
correlates
with
EEG
signals
from
the
contralesional hemisphere.
2. Our design was successful in using these signals to coordinate a
motor-driven orthosis.
Results of the screening procedure described above are shown in Figure 7 for a healthy subject.
The correlation between the left hand movement condition and rest condition are evaluated using
values per electrode channel (y axis) and per frequency bin (x axis). Electrodes over the left
hemisphere are on the lower half of the y axis and electrodes over the right hemisphere are on the
upper half of the y axis. Channels names are shown according to the 10-20 EEG system [17].
Bins with high values indicate significant power difference between movement and rest
conditions and as such are good candidates for control signals. Clusters (dotted red circles) of
high correlation are noted around the 12Hz bins in F3 through P7 and also in channel F3 around
the 22Hz bin.
16
Channel
R2 Values Between Left Hand Movement and Rest
R2
AF4
F8
F4
FC6
T8
P8
O2
O1
P7
T7
FC5
F3
F7
AF3
0.5
0.4
0.3
0.2
0.1
0
20
40
0
60
Frequency (Hz)
Figure 7 - between left hand movemnet and rest across bins of electrode channel and frequency
Power of the F3 electrode during conditions of left hand movement and conditions of rest is
shown in Figure 8. Movement produces even related desynchronization (ERD) in frequency bins
around 12Hz and 22Hz as physiologically expected [9].
Frequency Spectrum at Electrode F3
500
Move Left Hand
Rest
450
400
Amplitude
350
300
Decreased Amplitude
around 12Hz
250
200
150
Decreased Amplitude
around 22Hz
100
50
0
10
20
30
40
50
60
Frequency (Hz)
Figure 8 - Frequency spectrum of the F3 EEG electrode location during conditions of left hand movement (red curve) and
conditions of rest (blue curve).
17
The left hand side of Figure 5 shows a topographical color map of correlation values between
left hand movement and rest conditions for 12Hz brainwaves. Note high, bilateral correlations
are seen in the frontal cortex electrodes. On the right hand side of Figure 9, a map shows 22Hz
brainwaves. High correlations are seen unilaterally in F3 electrode. The strength of correlation at
12Hz allows for differentiation between left hand movement versus rest, and the correlation at
22Hz in electrode F3 allows for distinction of left versus right hand movement.
Figure 9 - Topographical color maps of values for 12 Hz and 22 Hz.
Using the spectral and spatial features identified from this analysis, we selected control
signals to move a cursor on a computer screen. The control signal was modulated when a subject
moved, or imagined moving his hand. The modulated signal gave the subject control of 1
dimensional cursor movement, and the subject was tasked with moving the cursor to a target that
randomly appeared on either side of a computer screen. Through 10 sets of trials with nonimpaired individuals we were able to achieve an 81.3% success rate for this task. We expect that
with optimization of our signal detection algorithms, we can achieve even better performance as
it was not uncommon to see success rates upwards of 90%.
18
Receiver Operator Characteristic (ROC) curves evaluated the performance of a
classification scheme. They provide view of the sensitivity of a classification algorithm as a
function of its specificity. After collecting a sufficient amount of data, classification is tested
with a number of classification thresholds. The true positive rate (ratio of true positives to total
positives) and false positive rate (ratio of false positives to total negatives) are observed. True
positive rate is then plotted as a function of false positive rate so that a random guess is viewed
as a straight line curve from bottom-left to top-right and perfect classification is a right angle at
the top–left of the figure. In Figure 10 we plot ROC curves with data from 4 different lengths of
data acquisition time windows. The longer windows provide us with more power to classify our
signal, but also increase the time buffer and therefore increase the latency of our system.
ROC curves
1
True positive rate (Sensitivity)
0.9
0.8
0.7
0.6
0.5
0.4
0.3
0.2
—
—
—
—
---
2.6 Seconds
2.0 Seconds
1.0 Seconds
0.5 Seconds
Random Guess
0.1
0
0
0.2
0.4
0.6
0.8
False positive rate (1-Specificity)
1
Figure 10 - ROC curves shows classification performance using varying window lengths and thresholds.
19
We also looked at the overall classification accuracy (ratio of true classifications to total
classifications) at the best threshold for each set of data. If specificity and sensitivity are equally
important, the best threshold is the one corresponding to the point on the curve closest to the topleft corner of the figure.
Time Window (Seconds)
Accuracy of Classification
2.60
2.0
1.0
0.5
96.2%
92.3%
86.5%
80.8%
Table 1 - Classification accuracy using best threshold as determined by ROC analysis per window length
In analysis of real-time operation, through 10 sets of trials with non-impaired individuals
we achieved an 81.3% success rate for closing and opening the orthosis in response to a prompt,
when using a 0.5 second window of acquisition time. Note that this is slightly higher than that
predicted by ROC analysis for the 0.5 second time window.
Computational Analysis
We use an autoregressive technique to compute the Maximum Entropy Method (MEM) of
spectral estimation, which uses an all pole linear filter to model the spectrum. The MEM
algorithm is common in the area of EEG signal processing compared to the Fast Fourier
Transform (FFT) due to its higher spectral resolution and better fitting of sharp spectral features
for a time-limited signal [18], [19].The tradeoff is increased computational requirements. The
narrow band isolation required to evaluate mu brain waves at 11-13 Hz make the MEM a
desirable choice in this circumstance.
Choosing the MEM estimation method we can derive the computational requirements of
our system. Our signal is sampled at 128 Hz and uses buffers of data 0.5 seconds in length (as
selected by our need for near real-time operation). Our bipolar spatial reference technique
requires subtraction of the reference electrode from the electrode of interest at every sample,
translating to 64 operations per buffer. Each MEM spectral estimation requires M x N operations,
where M is the number of samples and N is the model order being used. Model order refers to
20
the number of poles used in the linear filter and is directly related to the number of peaks which
can appear across the estimated spectrum. A model order of 16 has been determined to suit EEG
applications well [18], so a total of 16 7 64 operations results. This gives us a total of 1,088
operations per 0.5 second buffer or 2,176 operations per second. This analysis is helpful for
developing requirements towards a future microprocessor choice.
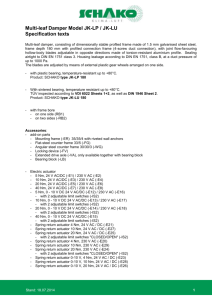
Mechanical Orthosis
The hand orthotic (Becker Oregon TAL100 Talon) was prefabricated to couple wrist motion to
the opening and closing of the hand. This coupling mechanism was replaced with a powered
linear actuator (Firgelli Miniature Linear Motion Series L16) as seen in Figure 11, shifting the
control of the device to the LabVIEW algorithm. The linear actuator operates according to pulsewidth modulation (PWM) control signals received from a microcontroller. The microcontroller
receives control signals from LabVIEW.
Figure 11 – prefabricated hand orthotic fitted with linear actuator for control of finger position
21
Cost Analysis
The IpsiHand final design has four components: the hand orthotic (Becker Oregon Talon), the
actuator to move and flex the orthotic (Firgelli model L16p), the headset (Emotiv EPOC), and
the micro-computer device to decode the brain signals (Gumstix Overo Earth COM). The Talon
by Becker Oregon has a retail price of $325, but a company representative stated that orders of
1,000 or more would cost $200-220 per orthotic. We expect to contract with Becker Oregon for
bulk manufacturing of the slightly modified version of the Talon hand that incorporates our
linear actuator. For the actuator, a representative from Firgelli reported the device costs
approximately $40 for wholesale buyers. Bulk costs of the Emotiv Epoc headset remain
undisclosed, however, a conservative estimate is $175 based on the retail price. Finally, the
Gumstix micro-computer device can be purchased for approximately $149 with bulk pricing.
Overall, parts will come to roughly $574, with an estimated $50-150 for assembly, quality
assurance, and distribution of our final product (
Table 2).
Component
Supplier
Item (Item No.)
Cost for
Prototype
$325
Hand Orthotic
Becker
Oregon
TalonTM
(BO-TAL100-L)
Linear
Actuator
EEG Headset
Firgelli
L16
(L16-P)
EPOC
MicroComputer
Assembly,
Inspection,
Distribution
Total
Emotiv
Systems
Gumstix
OveroTM Water
(GUM3503W)
and
Tobi
(PKG30002)
$112
Cost for
Production
(per unit)
$210 ± $10
(Confirmed)
$500*
−
$40
(Confirmed)
$175 ± $75
(Estimated)
$149 ± $20
(Confirmed)
−
$100 ± $50
(Estimated)
$ABC
$DCA ± $EFF
http://www.beckeroregoncatalog.com/
(pp. 3.3)
http://store.firgelli.com/l16-p-linearactuat16.html
http://www.emotiv.com/store/hardware/ep
oc-bci/epoc-neuroheadset/
http://www.gumstix.com/store/catalog/pro
duct_info.php?products_id=228
http://www.gumstix.com/store/catalog/pro
duct_info.php?products_id=230
Table 2 - Bill of Materials
*
The Emotiv EPOC supplied by Emotiv Systems at no charge. The prototype cost listed is the retail price.
22
Lifetime Operation Cost
The Ipsihand is very robust. For the most part, if component were to fail, the repair cost would
be the price of the component being replaced. For our calculations of lifetime operation cost, we
will assume a lifetime of 5 years.
For the linear actuator, the lifetime is supposed to be 20,000 strokes. Assuming a bi-weekly
therapy at 2 strokes a minute for 1 hour (or 240 strokes per week) the linear actuator would last
for about 83 weeks. This is about 1.6 years. So for a single patient, the linear actuator would
have to be replaced about 3.2 times, a cost of $125.
For the EPOC headset, the headset itself should not need replacing within the five years,
however the felt pads can be damaged or lost. The gold conducting contacts can become
corroded from the saline solution that makes the felt conductive. 16 replacement felt and
conducting contact pairs can be purchased for $49.95 from Emotiv’s website. In addition, 160
felts can be bought for $79.95.
Hazards and Failure Analysis
In the early design of IpsiHand, the linear actuator back end was not set as far back as it is
currently. As a result, if the actuator was extended fully, the hand would be hyper-flexed. To
correct this, the actuator has been set such that when it is fully extended, the hand is closed fully
and not hyper-flexed, and when the actuator is fully retracted, the hand is opened fully and not
hyper-extended. It should be noted, however, that people with especially sensitive finger joints
should not use this device as it may cause them discomfort when it opens fully or closes fully.
This problem could be corrected by programming IpsiHand with changeable limits of extension
and flexion such that the hand would stop at those limits instead of moving past them.
23
Conclusion
Combining the discovery of motor related signals in the undamaged brain hemisphere,
electronics, and advances in rehabilitation, our device provides a novel method for rehabilitation
for stroke survivors. In testing, we were able to process EEG signals for real-time hand control
with accuracy consistent with previous studies [20]. Recent evidence suggests that combining
BCIs and orthotic devices induces neural plasticity and improves motor function [9].
Furthermore, the potential for recovery is unhampered by the severity of neural pathway injury
since we circumvent the entire injured pathway and uses the brain’s plasticity to generate new
ones.
Signal acquisition, signal processing, and mechanical control methods are established, but
synthesizing them with the new technique of ipsilateral cortex recording has yet to be done.
Compared to devices such as, Myomo of Neuro-robotic Systems®, the Bioness H200 from
Ness®, and Hand Mentor from Kinetic Muscles Inc., our device facilitates plasticity most
directly, is less expensive and more portable, and can be used even in cases of severe damage to
neural pathways. Allowing patients to regain hand control with their thoughts will provide
tremendous encouragement to continue with a therapy. Combined with IpsiHand’s affordability
and minimal requirements for therapist supervision, IpsiHand also makes in-home treatment a
very practical possibility.
Based on therapist discussions, numerous improvements to the design are planned. Currently, a
laptop processes the EEG signals to be used for orthosis movement. We plan to miniaturize the
processing unit onto a micro-computer to give complete portability and allow patients to go
beyond rehabilitation and use the device as a replacement of hand function in daily life.
In addition, we would like to expand the system’s ability to adapt to spatially nonstationary signals. Implementing adaptive spatial filters or an adaptive classifier that finds the
strongest correlated channel automatically and continuously would improve robustness in signal
strength for a long-term out-patient orthotic. More importantly, spatial and temporal filters that
remove artifacts from eye blinks, EMG, and breathing, are essential to the device performance
outside of a research setting.
24
Works Cited
[1] D Lloyd-Jones and et al., "Heart disease and stroke statistics--2010 update: a report from the American Heart
Association Statistics Committee and Stroke Statistics Subcommittee," Circulation, pp. e21-181, 2009.
[2] J F Kraus and D L MacArthur, "Epidemiologic aspects of brain injury," Neurologic Clinics, vol. 14, no. 2, pp. 435450, 1996.
[3] M J DeVivo, "The national spinal cord injury statistical center database," in 25th Annual SCI Model Centers
OT/PT Leadership Forum, Birmingham, 2003.
[4] US Census Bureau. (2005) Prevalence of Disability Among Individuals 15 Years and Older by Specific Measures
of Disabilities. [Online]. http://www.census.gov/hhes/www/disability/sipp/disab05/d05tb1.pdf
[5] Henrik S Jorgensen et al., "Outcome and time course of recovery in stroke. Part II: Time course of recovery.
The copenhagen stroke study," Archives of Physical Medicine and Rehabilitation, vol. 76, no. 5, pp. 406-412,
May 1995.
[6] Lorenzo Carraro, Promoting independence following a stroke: a guide for therapists and professionals working
in primary health care. Geneva: Disability and Rehabilitation team, WHO; AIFO, 1999.
[7] National Institute of Neurolgical Disorders and Stroke, "Interagency head injury task force report," National
Institute of Neurolgical Disorders and Stroke, 1989.
[8] CE Levy and et al, "Functional MRI evidence of cortical reorganization in upper-limb stroke hemiplegia treated
with constraint-induced movement therapy," Am J Phys Med Rehabil, pp. 4-12, 2001.
[9] Kimberly J Wineski et al., "Unique cortical physiology associated with ipsilateral hand movements and
neuroprosthetic implications," Stroke, pp. 3351-3359, 2009.
[10] E Leuthardt, G Schalk, D Moran, and J Ojemann, "The emerging world of motor neuroprosthetics: a
neurosurgical perspective," Neurosurgery, vol. 58, no. 1, pp. 1-14, 2006.
[11] John M McBean and Kalais N Narendran, "Powered orthotic device and method of using same," 11/857,881,
September 19, 2007.
[12] Edward J Koeneman, James B Koeneman, Donald E Herring, and Robert S Schultz, "System and method for
neuromuscular reeducation," 12/758,706, April 12, 2010.
[13] John P Donoghue, Nicholas G Hatsopoulos, Mijail D Serruya, Matthew R Fellows, and Liam Paninski,
"Neurological signal decoding," 09/991,498, November 14, 2001.
[14] J C Flaherty and John P Donoghue, "Biological interface systems with wireless connection and related
methods," 11/201,283, August 11, 2005.
25
[15] G Schalk, D McFarland, T Hinterberger, N Bribaumer, and J Wolpaw, "BCI2000: a general-purpose braincomputer interface (BCI) system," IEEE Transactions on Biomedical Engineering, pp. 1034-1043, 2004.
[16] Dennis J McFarland, Lynn M McCane, Stephen V David, and Jonathan R Wolpaw, "Spatial filter selection for
EEG-based communication," Electroencephalography and Clinical Neurophysiology, vol. 103, pp. 386-394,
1997.
[17] Ernst Niedermeyer and Fernando Lopes da Silva, Electroencephalography: basic principles, clinical
applications, and related fields.: Lippincott Williams & Wilkins, 2004.
[18] William H Press, Brian P Flanney, Saul Amo Teukolsky, and William T Vetterling, Numerical recipes Fortran 77 :
the art of scientific computing. New York: Cambridge University Press, 1992.
[19] User Reference: ARFilter. [Online]. http://www.bci2000.org/wiki/index.php/User_Reference:ARFilter
[20] Jonathan R Wolpaw and Dennis J McFarland, "Control of a two-dimensional movement signal by a noninvasive
brain-computer interface in humans," Proc. Natl. Acad. Sci, vol. 101, no. 51, pp. 17849-17854, December
2004.
[21] D Broetz and et al, "Combination of brain-computer interface training and goal-directed physical therpy in
chronic stroke: A case report," J Neurorehab and Neural Repair, pp. 674-679, 2010.
26