Poster - Washington University in St. Louis
advertisement

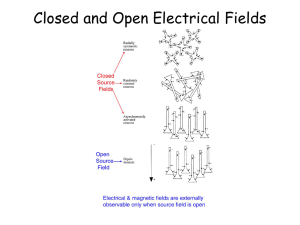
IpsiHand: An EEG-based Brain Computer Interface for Rehabilitation and Restoration of Hand Control following Stroke and Traumatic Brain Injury Using Ipsilateral Cortical Physiology Sam Fok, Raphael Schwartz, Mark Wronkiewicz, Charles Holmes, Jessica Zhang, Thane Somers, David Bundy, Dr. Eric Leuthardt Washington University in St. Louis Abstract Methods Results Stroke and traumatic brain injury (TBI) cause long-term, unilateral loss of motor control due to brain damage on the opposing (contralateral) side of the body. Conventional therapies are ineffective at restoring function in about half affected. Brain computer interfaces (BCIs) show promise for rehabilitation but remain primarily restricted to the research stage. Furthermore, traditional BCIs cannot work if areas such as M1 are damaged. We present a novel BCI, IpsiHand, which circumvents signal sourcing issues in an injured brain as well as risk associated with invasive recordings. IpsiHand uses electroencephalography (EEG) to record novel motor intent signals and control a powered hand orthosis, which allows the undamaged hemisphere to control both hands. Through sensory and proprioceptive feedback and neural plasticity, IpsiHand can strengthen ipsilateral neural pathways. Synchronous neuronal firing over large areas of the cortex are recorded from the scalp and processed onboard a laptop. The signal is filtered to generate a control signal, which is then sent to a linear actuator fitted to an orthosis controlling the patient’s finger closure. IpsiHand was tested with three healthy subjects to verify the ability to use non-conventional signals from cortex on one side of the brain to control a hand on the same side of the body. We found that: 1. Hand movement correlates with ipsilateral signals. 2. IpsiHand can use EEG signals to move the hand. Introduction Stroke and TBI combined are the leading cause of disability in the US, with around a million cases annually. Half report trouble with hand movement, and conventional physical therapy produces little improvement after 3 months post injury [1]. Therapies requiring the patient to actively control their impaired limb are most likely to induce reorganization of neural pathways and improving control but require intensive interaction between the patient and practitioner [2]. BCIs promise new, more effective motor therapies. They are traditionally applied in cases where central nervous signals are cut off from their destination by injury. Electrical signals are recorded from the brain to circumvent injuries and control devices to actuate a target limb, which recouples intent to move and movement [3]. Despite promise, conventional BCIs cannot be applied to cases of brain injury where damaged primary motor cortex contralateral to the affected limb produces no signals. However, recent study found distinct cortical physiology associated with ipsilateral, contralesional hand and limb movement in regions distinct and separable from the primary motor cortex [4]. These signals exist in cortex anterior to ipsilateral primary motor cortex at frequencies below 40Hz [5]. We used a non-invasive EEG consumer headset to record from cortex and control an orthosis that opens and closes a subject’s hand. As the least invasive recording technique, EEG is most practical for immediate application in the clinic. IpsiHand demonstrates the synthesis of neurophysiology, consumer electronics, and signal processing to develop new devices for more effective therapies. Implementation of this design constitutes a fundamentally new approach to restoring function in stroke and TBI survivors. Online Performance Results An Emotiv EPOCTM EEG headset records EEG signals from the scalp with 14 channels. The headset aligns, bandpass filters, and digitizes the signal at 128 Hz and transmits wirelessly to a laptop. Signal Processing and Control A Becker Oregon TalonTM prefabricated orthosis, designed to couple wrist motion to hand closure, was fitted with a powered linear actuator (Firgelli Miniature Linear Motion Series L16), controlled through our LabView algorithm. The orthosis size is adjustable, which is key in a clinical setting with a variety of patients. To mechanically prevent hyperextension or hyperflexion of the hand, the range of actuator motion is mapped only onto the natural range of finger joint rotation. 96.2% 92.3% 86.5% 80.8% Discussion Signal Acquisition Mechanical Orthosis 2.60 2.0 1.0 0.5 Classification accuracy using best threshold as determined by ROC analysis per window length. In actual trials, through 10 sets of trials with non-impaired individuals we achieved an 81.3% success rate for the 1D cursor task and orthosis using a 0.5s window. Note that this is slightly higher than predicted by ROC analysis. Screening Results EEG signals tend to be small and spatially diffuse compared to invasively recorded signals, so maximizing the signal-to-noise ratio is imperative to device performance. We used a large bi-polar reference spatial filter to attenuate noise from wide areas of the scalp and detect signals specific to a particular brain area. This also makes IpsiHand resilient to electrode placement variations [6]. Signal processing was carried out in the BCI2000 framework, a development platform that allows for rapid recording, filtering, and feature selection of brain signals [2]. Initial screenings determine the EEG features that our algorithm will use to contrast movement from rest. During screening, the user alternates between periods of attempted hand movement and periods of rest. With screening data, we identified the specific electrode channels and frequency bins with consistent changes in power spectrum between hand movement and rest conditions. The power of the selected channel is normalized to 0 mean and unit variance using a buffer of previous trial data and sent to LabView software for conversion into control signal. In LabView, the signal is compared to a user defined threshold and mapped to an actuator position command according to 𝑥𝑖 = 𝑥𝑖−1 + 𝑔𝑠 ′ where xi is the commanded position of the ith program iteration, g is a user defined gain, and s’ is the thresholded signal. Window Length (Seconds) Accuracy of Classification Left: Correlation colormap between left hand movement and rest per electrode and per frequency bin. Electrodes named according to the 10-20 EEG system(Right) [7]. Bins with high correlation are good candidates for control signals. Clusters (dotted red circles) of high correlation in ipsilateral cortex noted around the 12Hz bins in F3 through P7 and also in channel F3 around the 22Hz bin. Window Length — 2.6 Seconds — 2.0 Seconds — 1.0 Seconds — 0.5 Seconds --- Random Guess Top: Left: Spatial map of L.hand vs. rest correlations per channel at 12Hz. Note correlations present across frontal cortex. Top: Right: Spatial map of L.hand vs. rest correlations per channel at 22Hz. Note correlation only present unilaterally in channel F3. Bottom: Left: Raw spectrum of channel F3 shows difference in power around 12 and 22Hz bins during L.hand and rest conditions. Bottom: Right: ROC curves shows classification performance using varying window lengths and thresholds. Note that longer window have higher performance but also increase the system latency. The features identified during screening were used to modulate orthosis closure and 1D cursor movement. The subject was tasked with moving the cursor to a target randomly located at either the left or right side of the screen (below). Combining the discovery of signals in contralesional hemisphere, electronics, and advances in rehabilitation, IpsiHand offers a new rehabilitation option for stroke and TBI survivors. IpsiHand was able to process EEG signals for real-time hand control with accuracy consistent with previous studies [8] and theoretical ROC analysis. Combining BCIs and orthotic devices induces neural plasticity and improves motor function [8]. Furthermore, IpsiHand therapy is unhampered by the severity of neural pathway injury by circumventing the injury. Compared to other devices, IpsiHand facilitates plasticity most directly, is cheaper and more portable. Future Directions: We plan improvements in portability and signal processing. Portability Goals: Currently, a laptop processes the EEG signals used for orthosis movement. We plan to miniaturize the processing to a microcomputer for portability, allowing patients to even use the device as a replacement for normal hand function in daily life. Signal Processing Goals: • Expand the system’s ability to adapt to spatially non-stationary EEG signals. Possibilities include adaptive feature selection and adaptive spatial reference selection. • Remove muscular and other artifacts with spatial and temporal filtering. This is essential for device performance outside of a research setting. Artifact sources include eye blinks, EMG, ECG, and breathing. • Build real-time feature selection to eliminate need for screening procedure and improve user friendliness. • Improve control signal normalization and adaptation through least mean squares algorithm and linear regression techniques. Acknowledgements The undergraduate authors would like to thank D. Bundy for providing technical support and manuscript comments, Dr. E. Leuthardt for advice throughout the work, and Dr. A. Nehorai for his support as well. This project supported in part by The National Collegiate Inventors and Innovators Alliance, The Washington University School of Engineering, and Emotiv Systems. References [1] HS-Jorgensen, et_al,-"Outcome and time course of recovery in stroke: Part II: Timecourse of recovery. The Copenhagen Stroke Study,"Archives of Physical Medicine and Rehabilitation, 1995. [2] G Schalk, D McFarland, T Hinterberger, N Bribaumer, and J Wolpaw, "BCI2000: a general purpose brain computer interface (BCI) system,“IEEE Transactions on Biomedical Engineering, pp. 1034-1043, 2004. [3] D Broetz and et al, "Combination of brain-computer interface training and goal-directed physical therpy in chronic stroke: A case report," J Neurorehab and Neural Repair, pp. 674-679, 2010. [4] Kimberly J Wineski et al., "Unique cortical physiology associated with ipsilateral hand movements and neuroprosthetic implications,“ Stroke, pp. 3351-3359, 2009. [5] KJ_Wineski et. al., "Unique cortical physiology associated with ipsilateral hand movements and neuroprosthetic implications,“ Stroke, 2009. [6] DJ_McFarland, et. al, "Spatial filter selection for EEG-based communication, “Electroencephalography and Clinical Neurophysiology, vol. 103, 1997. [7] Ernst Niedermeyer and Fernando Lopes da Silva, Electroencephalography: basic principles, clinical applications, and related fields.: Lippincott Williams & Wilkins, 2004. [8] DJ_McFarland, et. al, "Electroencephalographic (EEG) control of three-dimensional movement," J. Neural Eng., vol. 7, 2010.