Anatomy Larynx (2) -Larynx is a box of cartilage
advertisement
 -Larynx is a box of cartilage")
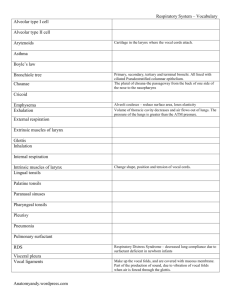
Anatomy Larynx (2) -Larynx is a box of cartilage -Structures of the larynx include: inlet, vocal cords false and true -Boundaries of the inlet: Above anterior: epiglottis On each side: aryepiglottic fold with aryepeglottic muscle within. Below and behind: transverse arytenoid muscle -Larynx from inside has 3 parts: 1) Vestibule (like the nose comes in the beginning) Above the false vocal cords below the inlet 2) Middle compartment :between the false and true vocal cords The opening between the false and true cords is called the sinus/ventricle of the larynx While inside we have the saccule: a pocket that contains the mucosa-rich glands. These glands secrete seromucous fluid. This saccule comes deep and below the false vocal cords, which means that it secretion will go downwards proving continuous lubrication of the true vocal cords. 3) Lower/ inferior compartment: the infra-glottic compartment. It continues as the trachea: extends below the true vocal cords. This compartment is important in the build-up of the air column; which with the adduction of the vocal cords is critical for speech and coughing. -The characteristics of the true vocal cords: 1) Attachment: vocal process of arytenoids cartilage pst. Inner angle of the thyroid cartilage ant. (this angle is acute in males obtuse in females) 2) Structures: 1) vocal ligament: free edge of conus elasticus 2) The mucus membrane covering the ligament is stratified squamous epithelium nonkeratinised (cause it is susceptible to injury: fast mitosis is crucial) 3) vocalis muscle : parallel to the ligament and part of the thyroaryetinoid muscle. The vocalis muscle relaxes the cords. 4) no submucosa: the larynx along with all the rest of respiratory tract is made up of mucosa, submucosa, supporting layer and connective tissue. However the true vocal cords lack submucosa. This is important so that no fluid accumulates in the submucosa causing edema and obstruction of the tract. 5) no blood vessels: normally the submucosa and lamina propria are rich in blood vessels. Since there is no submucosa in the true vocal cords, the blood vessels are also scarce and these cords are supplied by diffusion. This is not opposite to the false cords that are rich in blood vessels Muscles of the larynx: The space between the vestibular folds is called rima vestibule. The space between the true cords is the rima glottidis. This gap is the narrowest part of the larynx important in intubation of the patient. The muscles of the larynx are two groups: 1) Extrinsic 2) Intrinsic: all internal but cricothyroid is external The extrinsic muscles are: they affect the hyoid bone and since both the hyoid bone and larynx are covered with pretracheal fascia both are effected by these muscles. (along with the thyroid : thyrohyoid membrane. This is used for testing the thyroid by asking the patient to swallow and observe the movement) The extrinsic muscles are either: elevators of larynx: 1) digastric muscles :pst + ant bellies attached to the hyoid bone 2) stylohyoid muscles: from styloid process to hyoid bone. 3) myelohyoid muscles: from myelohyoid line of mandible. 4) geniohyoid muscles: inferior genial tubercle of mandible. These muscles are assisted by: salpingopharyngeus, palatopharyngeus and stylopharyngeus muscles. Intrinsic muscles: These muscles are divided into groups: 1) a group that controls the inlet of the larynx. 2) a group that controls the movement of the true cords. 1) A) oblique aryetinoid muscle: a continuation of aryepiglottic muscle. Between the arytenoids and the epiglottis. Effecting the fold attached to epiglottis. Origin: muscular process of arytinoid cartilage. Insertion: the apex of the opposite aryetinoid cartilage. (from one to another, hence oblique!) Nerve supply (N.S): recurrent laryngeal nerve Function: narrowing the inlet. B) thyroepiglottic muscle: medial surface of thyroid cartilage to the lateral margin of epiglottis. N.S: recurrent laryngeal nerve Function: widening in aryepiglottic folds (inlet) 2) (effecting the length): a) cricothyroid muscle: from side of cricoids cartilage to the lower border (inferior cornu) of thyroid cartilage. N.S: recurrent laryngeal nerve. Function: tenses the true cords (shortening) b) thyroaryetinoid muscle: (part of which is the vocalis muscle) from the inner surface of thyroid cartilage to the aryetinoid cartilage. N.S: recurrent laryngeal nerve. Function: relaxes the true cords (elongation): the aryetinoid cartilage goes forward causing the relaxation. (effecting the space in between) a) lateral cricoaryetinoid muscle: from the upper border of cricoids cartilage to the muscular process of the aryetinoid cartilage. N.S: recurrent laryngeal nerve. Function: adduction of the vocal cords: by the rotation of the aryetinoid cartilage above the upper border of the lamina of cricoids cartilage (rotatory movement) The muscular process goes anteriorly + medially. (inwards) b) posterior cricoaryetinoid muscle: from the back of the cricoids cartilage lamina to the muscular process of the aryetinoid cartilage. N.S: recurrent laryngeal nerve. Function: abduction of the vocal cords. The muscular process goes laterally and backwards. c) Transverse aryetinoid muscle: from the back and medial surface of aryetinoid cartilage to the back and medial surface of the opposite aryetinoid cartilage. It is located posteriorly. N.S: recurrent laryngeal nerve. Function: closes the posterior aspect of rima glottidis (related to the epiglottis) the aryepiglottic muscle within the aryepiglottic fold, continues as oblique aryetinoid muscle and transverse aryetinoid muscle. All these muscles are innervated by the recurrent laryngeal nerve except the cricothyroid muscle by external laryngeal nerve. (all from vagus) Blood supply of the larynx: 1) Superior laryngeal artery from the superior thyroid artery of the external carotid. It supplies part of the larynx above true vocal cords. This artery is accompanied with the internal laryngeal nerve of the superior laryngeal nerve of vagus: this nerve gives sensory branches to the mucosa above the true vocal cords. 2) Inferior laryngeal artery from the inferior thyroid artery from the thyrocervical trunk of subclavian artery. This artery is accompanied by the recurrent laryngeal nerve. Venous drainage: On each side of the larynx we have: - carotid sheath and contents (common carotid artery+ internal jugular vein +vagus in between). - The lobes of the thyroid gland. Posteriorly we have: the pharynx and the recurrent laryngeal nerve in between. Inferiorly we have: skin, superficial fascia (+contents) and the 4 infrahyoid muscles. Back to the venous drainage: 1) superior laryngeal vein from the superior thyroid vein from internal jugular vein. 2) inferior laryngeal vein from inferior thyroid vein( usually one vein) from the left brachiocephalic vein (longer than the right>>1-3 inches only the right) Lymphatics: Above the vocal cords: lymph vessels go with the superior laryngeal artery to the deep cervical L.N (associated with the bifurcation of the common carotid artery) Below the vocal cords: with inferior laryngeal artery to the paratracheal L.N around the trachea. Nerve supply: All from vagus nerve: there are two ganglia in the course of vagal nerve: superior and inferior vagal ganglia. The inferior ganglion gives the superior and inferior laryngeal nerves>>the superior laryngeal nerve gives the external and internal laryngeal nerves. External laryngeal nerve (accompanied with the superior thyroid artery) supplies the cricothyroid muscle. In the thyroidectomy operation (especially when there is a tumor in the thyroid and the anatomy is not clear), there is a high risk to ligate and cut the external laryngeal nerve with the superior thyroid artery. This will cause the cricothyroid muscle to lose function. This causes hoarseness of the voice (weakness of voice)>>other causes of hoarseness of voice include inflammation and post-drinking cold water. Internal laryngeal nerve pierces the thyrohyoid membrane with the superior laryngeal artery. (no risk considered in thyroidectomy>>>far from being cut) The recurrent laryngeal nerve: the vagus descends in the carotid sheath between the artery and vein : - at the root of the neck (right side)>>the right recurrent laryngeal arises deep to the right subclavian artery. - at the thorax below the arch of aorta>> the left recurrent laryngeal arises deep to ligamentum arteriosus (former ductus arteriosus, between the pulmonary artery and the arch of aorta)>>so it is a branch from vagus in the thorax. The left recurrent ascends between the trachea and the esophagus in the left side, then both (right and left) ascend between the larynx and the pharynx. These nerves supply all muscles of larynx/ cricothyroid muscle. Also, they give sensory branches to the mucosa below the true vocal cords. Injury to the recurrent laryngeal nerve: 4 cases: 1) Unilateral complete injury: Respiration: one vocal cord in the mid line balanced between abduction and adduction and another vocal cord normal: slight effect on breathing>>partial obstruction. Speech: not greatly affected, other cord compensates. 2) Unilateral partial injury: in this case only the superficial fibres of the nerve are damaged>>this is mostly due to manipulation: tough retraction by surgeon (the superficial fibres mostly supply the posterior cricoaryetinoid muscle(abduction)) So partial injury causes the adduction of the corresponding muscle. So: we will have hoarseness of voice and difficulty in breathing. 3) Bilateral complete injury: Both cords in mid position. Breathing impaired due to partial closure of rima glottidis (dyspnea) Speech is lost. 4) Bilateral partial injury: Both cords are adducted. Lost of voice. Suffocation>>no breathing. This case will require tracheostomy: (opening in the rings of trachea) The lobes of the thyroid gland are lateral to the larynx while the isthmus comes anterior to the 2,3,4 rings of trachea. So rings available for tracheostomy are: 1) First ring: mostly used in operations, when both the recurrent laryngeal are damaged while operating. This is called high tracheostomy. 2) Lower rings below the isthmus: these are used mainly in emergencies: Put your finger in the supra-sternal notch and you can feel the rings of trachea (5,6..rings), now with a sharp object make an opening so the patient can start breathing. This will prevent the brain death in the patient if done in less than 2-5 minutes of obstruction. However, it will cause bleeding due to the presence of : anterior jugular vein, inferior thyroid vein and thyroidea ima artery>>this bleeding will stop in 2 minutes and is considered a minor disadvantage.. ---------------------------------------------------the end----------------------------------------------