EXAMINATION OF THE SENSORY & MOTOR SYSTEMS
advertisement

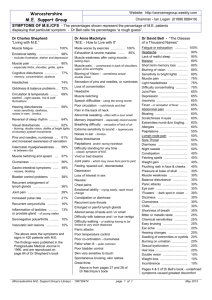
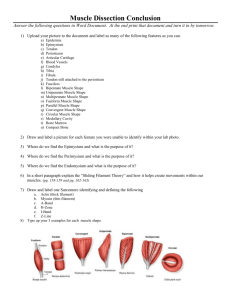
Practical No : 21 EXAMINATION OF THE SENSORY & MOTOR SYSTEMS Examination of the Sensory System Objectives : At the end of the practical the student should be able to, 1. List the different sensory modalities and state the instruments / equipment used to test each of them. 2. Accurately test for the above sensory modalities 3. Illustrate the dermatomal nerve distribution in the body. 4. Describe the physiological basis of testing to detect the sensory level of a lesion. The Sensory Modalities Sensation can be divided into Exteroception (Eg. Touch, Pain, Temperature) Proprioception (Eg. Muscle, joint position) Interoception (Eg. Visceral sensation) Distance reception (Eg. Smell, Sound, Taste) The purpose of testing these modalities is, To demonstrate clearly, the areas of abnormal sensation To define which modalities are involved within these limits. To compare the findings with known patterns of abnormal sensation. Each sensory modality requires specific equipment in order to test them accurately. Light Touch Pain Temperature Proprioception Vibration Cortical localization Two point discrimination Steriognosis Graphaesthesia Point localizations Sensory extinction Tested with cotton wool Tested with either a toothpick or a pin Tested using warm / cool water filled into small glass tubes. Tested by changing joint positions. Tested with a vibrating tuning fork Tested with a divider or two toothpicks applied simultaneously - Tested by giving an easily identifiable object like a key. - Tested by tracing numbers or letters on the skin - Tested with cotton wool, pin prick Testing the sensory nervous system Instruments / equipment Swabs of cotton wool Toothpicks Pins Tuning fork Two point discriminator / Divider Tubes of warm / cold water Key, coin, pencil Method - - General : The patient should be relaxed and aware of what he is being examined for. The patient should be shown each piece of equipment used for testing. He should be made aware of each sensation prior to testing. In the process of examination, avoid rhythmicity. All dermatomes on both sides of the body should be examined. The sensations should be compared on both sides of the body as well as adjacent dermatomes. Touch : The swab of cotton wool is twisted into a small point. This point is applied to the patient's forehead and chest to demonstrate the sensation. The patient is then told to close his eyes and count each time he feels the examiner touching the cotton wool to the various dermatomes. The cotton should not be dragged along the skin - Pain : Using the pin or toothpick, the patient is lightly pricked on the forehead or chest, to familiarize him with the sensation of both the sharp and blunt ends. As above, the patient closes his eyes and counts when he perceives the sensation. The examiner should use both sharp and blunt ends and as the patient to differentiate. He should also report areas of diminished pain sensation. - Temperature : The hot and cold tubes should first be placed on the patient's forehead to identify. They are then applied at a random sequence to the skin. The patient with eyes closed, then attempts to distinguish them. - Deep pain : Tested by firmly squeezing over muscles and tendons. The patient is asked to indicate when the pressure becomes painful. The examiner gauges if the force applied will be painful in normal people. - - Proprioception : Usually tested at the proximal interphalangeal joint of the big toe. The proximal phalanx is fixed by grasping it firmly in the finger and thumb of the examiner's left hand. The thumb and forefinger of the right hand grip the terminal phalanx on its lateral borders. Avoid contact with the second toe. Then the terminal phalanx is moved upward or downward by the examiner. The patient is initially shown the upward and downward movement and told that they are 'up' or 'down'. He is then asked to close his eyes and to indicate whether the joint is flexed or extended by saying 'down' or 'up' respectively. - Vibration : A tuning fork with a frequency of 128 cycles / sec. is vibrated and the handle then placed on the patient's forehead to indicate the sensation. The patient is then asked to close his eyes and the vibrating tuning fork is placed on bony prominences, starting from the dorsum of the terminal phalanx of the big toe. He is asked to describe the sensation. The test is positive only if he perceives vibration and not touch or temperature. - Cortical sensations : - Two-point discrimination, Tests the ability to distinguish the contact of two separate points applied simultaneously. Should determine the minimum distance of separation at which two points are identified as two distinct stimuli. This distance is around 3 - 5 mm in the finger pulps and 50 - 100 mm in the legs or back. Steriognosis, Tests the ability to identify objects by palpation. Requires intact peripheral sensation as well as evocation in the cortex of the constellation of ideas and memories necessary for recognition. Is examined by giving the patient an easily identifiable object like a key ot coin. Graphaesthesia, Tests the ability to recognize numbers or letters traced by a blunt object on the palm of the hand. This is impaired in lesions of the sensory cortex. Point Localisation, Tests the ability of the patient to localize accurately, the point touched with the head of a pin or toothpick when the eyes are closed. The eyes are opened and the patient then places his finger on the exact point where the stimulus was applied. Sensory extinction This tests the perception of stimuli at corresponding sites on both sides of the body. Initially, the patient should be tested separately on both sides of the body to rule out any sensory lesions. It is necessary to demonstrate the stimulus to the patient prior to testing. Then the stimulus is simultaneously applied to corresponding sites on the opposite sides of the body. The patient, with eyes closed, should identify the side (left / right) as well as the number of stimuli (one / two) applied. The dermatomal nerve distribution C2 T2 C3 C4 C4 C5 C5 T2 3 4 5 6 3 5 4 T2 6 7 8 7 8 C6 10 12 11 T1 9 T1 9 C6 12 L1 L2 L1 C8 L2 C7 10 11 S4 C8 S2 L4 L4 C7 S3 L5 L3 S2 S1 L5 L4 S1 L5 Examination of the Motor System Objectives : At the end of the practical the student should be able to, 1. List the components tested in the examination of the motor system. 2. Evaluate muscle power according to the Medical Research Council grading system. 3. Perform a complete examination of the motor system 4. Enumerate the clinical signs observed in Upper Motor Neuron lesions and Lower Motor Neuron lesions, and state the causes for these lesions. Testing for motor function also involves the basic principles described for examination of any system. They are, Inspection Muscle bulk Fasciculation / Fibrillation Voluntary movements Involuntary movements Palpation Muscle tone Muscle power Coordination Clonus Reflexes Gait & Posture Inspection : Muscle Bulk - Is best estimated by Inspection. - A muscle may be hypertrophic or atrophic. - Differences in bulk should be observed in corresponding muscles on either side of the body. - Wasted or atrophic muscles are, Smaller, softer, more flabby than normal when contracted. If accompanied by fibrosis, are inelastic and hard. May even form contractures. - Hypertrophy can be observed in, The dominant side of the body as opposed to the non-dominant side, especially in manual labourers. Response to repeated exercise as in weight lifting and athletes. Pathological conditions such as ‘Duchenne Muscular Dystrophy’, where it is a pseudohypertrophy. Other myotonic disorders. - It may be useful to measure the corresponding muscles in both sides of the body using a tape measure, and then compare the bulk, if there is no visible difference in bulk. Fasciculation - This is often visible in wasted muscles. - It is produced by the spontaneous contraction of large groups of muscle fibres or of whole motor units. - The movements are usually of fine amplitude. - Fasciculations can be elicited by lightly tapping on the muscle concerned. - These can also be seen in normal individuals after severe exercise etc. Voluntary movements - Observe the patient’s voluntary movements and assess whether they are normal or abnormal. - Clumsy, jerky movements may indicate incoordination. - Muscle power may also be assessed to a certain degree, by asking the patient to perform limb movements against gravity. Involuntary movements - Careful inspection should be made of any involuntary movement the patient may have. - These are, Tremor exaggeration of physiological tremor. Eg. Alcoholics, Thyrotoxicosis, anxiety. ‘Pill rolling’ tremor in Parkinson’s disease Myoclonus Sudden, shock like, contractions Eg. Epilepsy, falling asleep Choreiform movements Irregular, jerky, semi-purposive and ill-sustained. HemiballismusSimilar to chorea, but much more forceful, and are unilateral. Athetoid spasms Palpation : Muscle tone - Is defined as the resistance to passive stretch of a muscle. - Usually, the manipulation of a limb evokes a slight elastic resistance from the adjacent muscles. - Before the examination the patient should completely relax. - Then, various limbs are manipulated by the examiner, until all muscle groups are examined. - Tone may be increased (Hypertonia) or decreased (Hypotonia). - Hypertonia o There may be spasticity or rigidity. o Spasticity is characterized by a rapid build up of resistance to stretch and as the stretch continues, there is a sudden ‘give’ followed by a lessening of resistance. Eg. Clasp-knife effect (seen in lesions of the pyramidal pathway). o Rigidity is resistance to passive movement which is sustained throughout the entire range of movement Eg. ‘Lead-Pipe’ rigidity (seen in extra-pyramidal lesions). - Hypotonia o Is the decreased resistance to passive movement. o Is harder to assess. Muscle power - Can be tested either isometrically or isotonically. - Isometric testing The patient is asked to contract a group of muscles as powerfully as possible. Then he should maintain the posture of that joint while the examiner tries to restore it to its normal position. - Isotonic testing The patient is asked to put a joint through its full range of movement using maximal power. The examiner opposes this entire range of movement, trying to prevent its accomplishment. - Assessment of muscle power is performed according to Medical Research Council grading. Grading 0 Criteria 1 No active contraction Visible or palpable contraction without active movement 2 Movement which is possible with gravity eliminated 3 Movement which is possible against gravity 4 Movement which is possible against gravity plus resistance, but which is weaker than normal Normal power 5 Coordination - This is the smooth recruitment, interaction and cooperation of separate muscles or groups of muscles in order to accomplish a specific motor act. - Loss of coordination is termed “Ataxia”. - Coordination is achieved by a combination of Proprioception from muscles and joints Cerebellar function State of muscle tone Vision (usually compensatory) - Coordination is tested with the following, o Finger pointing test (read. Cerebellar function) o Heel – shin test (read. Cerebellar function) o Draw a straight line on the floor and ask the patient to walk along it. o Romberg’s test Is not a test of cerebellar function. Is a test of sensory ataxia. The patient stands with feet close together, arms abducted and eyes closed. Patient may sway and even fall. Clonus - This is the term given to a rhythmic series of involuntary muscular contractions evoked by a sudden stretch of muscle. - A few beats of clonus maybe elicited in a nervous patient, and may not be significant. - Sustained clonus, however, reflects exaggerated tendon reflexes as a result of a UMN lesion - Two forms generally elicited, Patella Clonus The patient lies supine with legs outstretched and relaxed The examiner places one fist underneath the patient’s knee and sharply pushes the patella towards the patient’s foot. Ankle Clonus The patient lies supine with legs outstretched and relaxed The examiner raises the leg to be examined, by the knee, right off the bed. He then, firmly dorsiflexes the patient’s foot Reflexes : A neurological reflex depends on an arc which consists of, An afferent pathway triggered by stimulating a receptor An efferent system which activates an effector organ A communication between these two components and Cell body of Sensory Neuron Axon of Sensory Neuron Dorsal Root Receptor ends of sensory neuron (neuromuscular spindles) Quadriceps tendon Synapse Cell body of motor neuron Patellar Ligament Axon of motor neuron Effector Muscle (quadriceps femoris) Tibia Ventral Root Femur Routine examination should elicit Tendon (deep) reflexes in the limbs Superficial (cutaneuos) reflexes Fibula Tendon Reflexes - Are most efficiently evoked by a tap from a tendon hammer. - The instrument should have a firm but flexible shaft and should contain most of its weight in its head, which should preferably be made of metal and well padded with soft rubber. - The patient is placed in a comfortable, relaxed position, which allows the examiner easy access to the joint where the reflex is to be elicited. - The muscle being tested should be visible. - Compare reflexes on both sides. - Reflexes commonly checked for are, Knee Jerk (L3, L4) Ankle Jerk (L5, S1) Triceps Jerk (C6, C7) Biceps Jerk (C5, C6) Supinator Jerk (C5, C6) - Quadriceps Femoris contraction Gastrocnemius, Soleus contraction Triceps contraction Biceps contraction Supination of forearm If tendon reflexes cannot be elicited, the patient should be asked to relax as well as perform reinforcing techniques simultaneous with the application of the tendon hammer. Superficial Reflexes These are muscular contractions evoked by cutaneous stimulation. The Plantar Response - The patient lies supine with his legs extended - Using the end of a car key or an orange stick, the examiner draws a line slowly along the lateral border of the foot, from the heel towards the little toe. - Observe for a ‘flexor’ response with plantar flexion of the great toe as well as the other toes. - The stimulus should not cause injury, but should be a noxious stimulus The Abdominal Reflexes - The patient should lie warm and relaxed in a supine position. - The examiner then draws the point of an orange stick lightly and quickly across the abdomen, from lateral towards the midline. - Two lines should run parallel to the costal margins and two lines parallel to the inguinal ligaments. - Observe for a brisk contraction of the underlying muscles of the anterior abdominal wall. The Cremasteric Reflex - Stroking or scratching the inner aspect of the upper part of the thigh in male patients, provokes an elevation of the testis. Gait & Posture These should be ideally observed at the very beginning of the examination, as the patient walks into the room. Various types of gait can indicate quite reliably, the condition the patient is suffering from. Spastic Gait Patient walks on a narrow base, has difficulty bending knees and drags the feet along as if glued to the floor. Stamping Gait Is the Gait seen in sensory ataxia. Patient raises his foot abnormally high and very suddenly, jerks it forward and brings it to the ground with a stamp. Drunken Gait Seen in cerebellar ataxia. Patients walk on a broad base, the feet planted widely apart and placed irregularly. Festinant Gait Characteristic of Parkinson’s disease. Patient bends forward and advances with short, shuffling steps. The arms do not swing. Waddling Gait Is likened to the gait of a duck. The body is usually tilted backwards with an increase in lumbar lordosis.. Feet are planted wide apart and the body sways from side to side. Seen in proximal myopathy. High stepping Gait Adopted to avoid tripping due to the toes dragging along the ground in foot drop. The festinant gait of Parkinson's disease Signs of Upper and Lower Motor Neuron Lesions Upper Motor Neuron Lesion Drift of upper limb Weakness with a characteristic distribution Increase in tone (spastic type) Exaggerated tendon reflexes Extensor plantar response Loss of abdominal reflexes No muscle wasting Normal electrical excitability of muscle Lower Motor Neuron Lesion Muscle weakness Muscle wasting Hypotonia Loss of reflexes Fasciculation Contractures of muscle Trophic changes in skin and nails Fibrillation potentials seen when sampled electrically Causes Causes - Spinal cord compression - Subacute combined degeneration of the cord - Syringomyelia - Cerebral infarction - Vascular disease of the cord - Bell's palsy Poliomyelitis Cervical and lumbar disc protrusion Nerve trauma or entrapment Mononeuritis multiplex