Cardiovascular 10 – Mechanical Properties of the heart II
advertisement

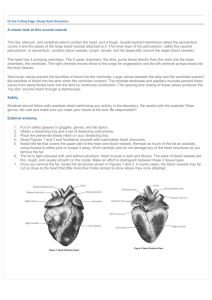
Cardio 10 – Mechanical Properties of the Heart II Anil Chopra Event 1. Describe the events of the cardiac cycle. Mechanics ECG Atrial Systole aortic, ventricle, atrial Isovolumetric Contraction aortic, ventricle, atrial Rapid Ejection aortic, ventricle, atrial Sound Atria contract to top off blood in the ventricles (some has already flown through the AV valve. Some blood is pushed back up the jugular vein. Produces P-wave as SAN depolarises atria. None, but can produce 4th heart sound in congestive heart failure, pulmonary embolism & tricuspid incompetence. The small interval where the atrio- ventricular valves are closed and the semi lunar valves are closed. There is high pressure in the ventricles QRS complex as ventricles depolarise. First “lub” as AV valves close. Ventricles contract causing the high pressure to force open the semilunar valves. No depolarisation. None. Reduced Ejection aortic, ventricle, atrial Isovolumetric Relaxation aortic, ventricle, atrial Rapid Ventricular Filling aortic, ventricle, atrial Reduced Ventricular Filling aortic, ventricle, atrial Marks the end of systole. Ventricular volume decreases. SL valves begin to close. T-wave due to ventricular depolarisation None. The beginning of diastole. Aortic and pulmonary valves are shut as blood falls back through the aorta. None. 2nd heart sound “dub” as semilunar valves close. The AV valves are open and so blood rapidly flows from veins, to atria to ventricles. This increases ventricular volume None Can produce 3rd heart sound in hypertension or mitral incompetence. Simply, the ventricles fill more slowly as atrioventricular valves are open None None. 2. Use a graph to correlate electrocardiographic events and pressure events of the atria, ventricles aorta and pulmonary artery. 3. Indicate on the graph, the phases of the cardiac cycle and the corresponding pressure changes, valve openings and closures. Pressure change patterns are the same for left and right ventricles. Aortic Valve Opens Aortic Valve Shuts Quantitatively, right pressures are lower. Mirtal Valve Shuts Mitral Valve Opens Amount of blood ejected from each ventricle is the same 4. Define and State normal values for right and left ventricular end-diastolic volume, end systolic volume, stroke volume, end diastolic pressure and peak systolic pressure. End Diastolic Volume: volume of blood in the ventricles after filling. Usually around 130ml. End systolic Volume: volume of blood in the ventricles after systole. Usually around 60ml. Stroke Volume: volume of blood ejected by ventricular contraction. Usually around 70ml. End Diastolic Volume = stroke volume + end systolic volume Left End Systolic Pressure: pressure of left ventricle systole. Usually around 120mmHg. Left End Diastolic Pressure: pressure of left ventricle diastole. Usually around 80mmHg. Mean left Atrial Pressure: Usually between 8-10mmHg. Right End Systolic Pressure: pressure of right ventricle systole. Usually around 25mmHg. Right End Diastolic Pressure: pressure of right ventricle diastole. Usually around 5mmHg. Mean right Atrial Pressure: Usually between 0-8mmHg. 5. State the origin of the heart sounds. Lub – Atrioventricular valves closing Dub – semilunar valves closing. 6. Provide the mathematical equation for ejection fraction. Define cardiac output and indicate its determinants. Ejection Fraction: % of end diastolic volume ejected. Usually around 54% Can be up to 80% in exercise or 40% during heart failure. Cardiac Output: amount of blood pumped out each ventricle per minute; calculated by heart rate x stroke volume. Usually around 5litres. 7. Construct Simple volume-pressure diagrams from the events during the cardiac cycle and annotate the graphs appropriately. 1) Ventricles full (end diastolic volume) Preload. 2) Ventricles contract and meet aortic pressure. Afterload encountered. 3) Ventricles empty (end diastolic volume) but ventricles still contracted. 4) Ventricles are relaxed and empty so pressure is low, as is volume. INCREASING PRELOAD INCREASES STROKE VOLUME (Frank – Starling relationships) These increases can be as a result of sympathetic stimulation of the heart during exercise. If the ventricles fill with more blood in diastole, the heart contracts with more force so greater stroke volume is achieved.