EMS - Heart of Texas Regional Advisory Council
advertisement

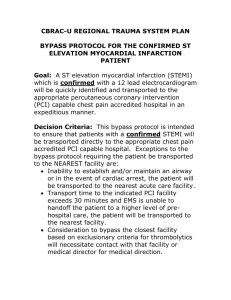
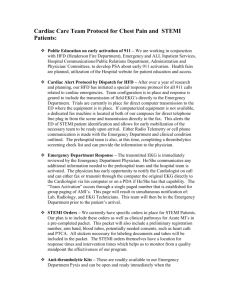
Heart of Texas Regional Advisory Council (HOTRAC) Trauma Service Area (TSA) - M Regional STEMI Plan Heart of Texas Regional Advisory Council (HOTRAC) 405 Londonderry, Suite 201 Waco, Texas 76712 Email: info@heartoftexasrac.org For the service delivery area including Bosque, Falls, Hill, Limestone, and McLennan Counties. Phone: (254) 761-7890 Fax: (254) 761-7895 HOTRAC Regional STEMI Plan March 2011 Page 1 Table of Contents Introduction Organization Service Area/ Facilities Regional Plan TSA M – EMS Providers (Ground) TSA M – Air Medical Providers TSA M – Acute Care Facilities System Participation System Access Communications Regional Pre-hospital Medical Oversight & Control Pre-hospital Triage Helicopter Activation Facility Diversion Facility Bypass Facility Triage Criteria Inter-hospital Transfers Regional STEMI Form System Performance Improvement Statement of Confidentiality HOTRAC Regional STEMI Plan March 2011 3 3 3 4 5 9 18 19 20 20 27 28 28 29 29 30 30 33 34 36 Page 2 Introduction Organization and Service Area Organization The Heart of Texas Regional Advisory Council (HOTRAC) is comprised of the Central Texas counties of Bosque, Falls, Hill, Limestone, and McLennan. The HOTRAC was organized and completed the incorporation process in 1994, and became an approved 501 (c) (3) organization in 1995. The HOTRAC Vision Statement is be a lead Regional Advisory Council in the State of Texas that achieves improved quality of life by reducing morbidity/mortality for emergency healthcare conditions within our Trauma Service Area. The mission is to reduce death/disability related to acute illness and injury by providing infrastructure and leadership necessary to sustain an inclusive acute care, trauma, emergency medical, and disaster system in all phases within our Trauma Service Area. Service Area/Facilities The HOTRAC Service Area is comprised of four rural counties (Bosque, Falls, Hill, and Limestone) and one suburban county (McLennan). The terrain in this region is primarily Black-land prairie with rolling hills located in the Bosque county area. Interstate 35, a heavily traveled transportation artery, transects McLennan and Hill Counties and is the source of many multi-vehicular crashes annually. Also heavily traveled State Highway 6 traverses McLennan, Falls and Bosque counties, while Limestone counties transportation primarily occurs via farm-to-market roads. Bosque County encompasses 989.3 square miles and has a population of 17,631 lives. Goodall-Witcher Healthcare Foundation is a 40-bed acute care facility located in Clifton, Texas. Goodall-Witcher has surgical capability. One EMS service provides 9-1-1 service in Bosque County. Falls County is located in the southern most part of this Region and encompasses 769 square miles. The county population is 16,782. Falls Community Hospital in Marlin is a 44 bed facility and is centrally located. There is one EMS service that provides 9-1-1 service in Falls County. Hill County is located in the northern portion of the region and encompasses 962 square miles. The county population is 35,840 persons. Hill Regional Hospital is a 92-bed acute care facility with surgical capability. A second facility is Lake Whitney Medical Center which is located in the western portion of the county. Lake Whitney Medical Center is a 49-bed acute care facility. Three EMS providers provide 9-1-1 services in Hill County. Located in the eastern-most portion of the region, Limestone County includes 909 square miles of primarily farm and ranch land. The population in Limestone County is 22,287 persons. Parkview Regional Hospital is a 77-bed acute care facility with surgical capability. Limestone Medical Center is a 20-bed acute care facility (which does not have surgical capability). Three EMS providers provide 9-1-1 service in Limestone County. McLennan County is the only suburban county in the region and covers 1041.9 square miles of Central Texas and has a total population of 233,378 persons. Waco is the largest city in the county (population approximately 121,496) and contains two acute care hospitals: Hillcrest Baptist Medical Center and Providence Health Center. Both facilities are capable of providing Percutaneous Coronary Intervention (PCI) care. Providence Health Center is a 230-bed acute care facility with surgical capability. Hillcrest Baptist Medical Center is a 393-bed acute care facility with surgical capability. The other hospitals located in Waco are psychiatric facilities. These facilities are Central Texas Veterans Healthcare System – Waco Campus and Waco Center for Youth. There are five EMS services that provide 9-1-1 services in McLennan County. HOTRAC Regional STEMI Plan March 2011 Page 3 Regional Plan This Plan has been developed in accordance with generally accepted STEMI guidelines and procedures for implementation of a comprehensive Emergency Medical Services (EMS) and STEMI System plan. This plan does not establish a legal standard of care, but rather is intended as an aid to decision-making in general patient care scenarios. It is not intended to supersede the physician’s prerogative to order treatment. Due to the rural areas in this Region, the HOTRAC promotes and supports First Responder Organizations (FRO) and Volunteer Fire Departments (VFD) in order to help ensure expedited pre-hospital emergency care for its residents. STEMI Patient The classification of STEMI patients is based on a standard definition of “the STEMI patient” which is applied in a consistent manner in both the pre-hospital and hospital setting. The STEMI Patient - In TSA-M, the STEMI patient is defined as any patient presenting with symptoms of an acute myocardial infarction and/or left bundle branch blockage and/or 1mm of ST-elevation in two contiguous EKG leads. HOTRAC Regional STEMI Plan March 2011 Page 4 HOTRAC – TSA M EMS 9-1-1 PROVIDERS (Ground) (see attached map on page 8 of this document for service areas) CareFlite Jan Cody – ( Fax – Dispatch – Level of Service – Medical Director – Number of Vehicles – Central Texas EMS Jason Haisler - Manager Marlin, TX (254) Fax – (254) Dispatch – Level of Service – Medical Director – Dr. Steven Ellerbe Number of Vehicles - 3 Crawford EMS Marilyn Judy – President P.O. Box 341 Crawford, Texas 76638 (254) 486-2101 Fax – (254) 486-2198 Dispatch – McGregor Police Department (254) 840-2855 Level of Service - BLS Medical Director – Dr. George Smith Number of Vehicles - 1 Hillsboro Fire Dept. & EMS Chief Tony Cain – Director of Public Safety P.O. Box 568 Hillsboro, Texas 76645 (254) 582-2401 Fax – (254) 582-9155 Dispatch – City of Hillsboro (254) 582-2141 Level of Service – BLS with ALS capabilities Medical Director – Dr. Richard Jackson Number of Vehicles – 2 HOTRAC Regional STEMI Plan March 2011 Page 5 ETMC – EMS Dale Yates – Regional Director 1501 Hogan Lane, Ste. H Waco, TX 76705 (254) 799-7718 Fax – (254) 799-2363 Dispatch – EMTC Tyler (800) 255-2011 Level of Service – MICU Medical Director – Dr. William Moore Number of vehicles – 13 Lake Whitney Medical Center EMS Jimmy Hoskins – Director 103 N. Colorado Street Whitney, Texas 76692 (254) 694-9706 Fax – (254) 694-9708 Dispatch – Level of Service - BLS with MICU capabilities Medical Director – Dr. Richard Jackson Number of Vehicles - 3 Limestone Medical Center EMS Shelton Chapman - Director 701 McClintic Dr. Groesbeck, Texas 76642 (254) 729-3097 Fax – (254) 729-3532 Dispatch – Limestone County Sheriff’s Office (254) 729-3278 Level of Service – BLS with MICU capabilities Medical Director – Dr. Mark Hoeschele Number of Vehicles - 3 McGregor EMS William Heath – President PO Box 237 McGregor, Texas 76657 (254) 840-2528 Fax – (254) 840-2528 Dispatch – McGregor Police Department (254) 840-2855 Level of Service – BLS with MICU capabilities Medical Director – Dr. Jon Daniell Number of Vehicles - 2 Mart EMS James Fullner – President P.O. Box 335 Mart, Texas 76664 (254) 876-3322 HOTRAC Regional STEMI Plan March 2011 Page 6 Fax – (254) 876-3332 Dispatch – McLennan County Sheriff’s Office (254) 757-5222 Level of Service - MICU Medical Director – Dr. Jon Daniell Number of Vehicles - 2 Mexia Fire Dept & EMS Mike Clements – EMS Director P.O. Box 207 Mexia, Texas 76667 (254) 562-4188 Fax – (254) 562-2569 Dispatch – Mexia Fire Department (254) 562-4150 Level of Service – BLS with MICU capabilities Medical Director – Dr. Yong Chin Number of Vehicles – 3 Ambulances North Bosque EMS Linda Catena – EMS Director P.O. Box 119 Meridian, Texas 76665 (254) 435-2070 Fax – (254) 435-2560 Dispatch – Bosque County Sheriff’s Office (254) 435-2362 Level of Service – BLS with MICU capabilities Medical Director – Dr. Kevin Blanton Number of Vehicles – 3 Scott & White EMS 2401 S. 31st Street Temple, TX 76508 (254) 724-8080 Fax – (254) 724-0019 Dispatch – via MedCom Level of Service – BLS with MICU capabilities Medical Director – Dr. Robert Greenberg Number of vehicles- 16 (total) West Volunteer Ambulance Service Tom Marek – Supervisor P.O. Box 461 West, Texas 76691 (254) 826-3779 Fax – (254) 826-3231 Dispatch – (254) 826-3778 Level of Service – BLS with MICU capabilities Medical Director – Dr. George Smith Number of Vehicles - 3 HOTRAC Regional STEMI Plan March 2011 Page 7 HOTRAC – TSA M EMS 9-1-1 PROVIDERS (Ground) HOTRAC Regional STEMI Plan March 2011 Page 8 HOTRAC – TSA M EMS 9-1-1 PROVIDERS (Air) (see maps on next pages of this document for service areas) Air Evac LifeTeam – West (AEL 51) Steven Clinkscales, Regional Manager Cell (417) 293-2626 405 Meadow Drive West, TX 76691 Base – (254) 826-0521 Fax – (254) 826-0520 Dispatch – 800-247-8322 Medical Director – Dr. Brian Price Air Evac LifeTeam – Killeen (AEL ) 2407 S. Creek Clear Road Killeen, TX 76549 Base – (254) 628-1275 Fax – (254) 628-2710 Dispatch – (800) 247-3822 or (800)568-6806 Medical Director – Dr. Philip Chapa Air Evac LifeTeam – Fairfield (AEL 53) 160 S IH 45 Fairfield, TX 75840 Base – (903) 389-7266 Fax – (903) 389-7352 Dispatch – 800-247-8322 Medical Director – Dr. Brian Price Air Evac LifeTeam – Ennis (AEL 74) 3004 West Ennis Ave. Ennis, TX 75119 Base – (972) 875-8216 Fax – (972) 875-6963 Dispatch – 800-247-8322 Medical Director – Dr. Frank Chappa Cell – (417) 274-8722 Base – (817) 579-2031 Fax – (817) 579-2034 Dispatch – (800) 247-3822 or (800)568-6806 Medical Director – Dr. Philip Chapa PHI STAT Air 1 – Killen Skylark Field Brittany Misercola, Business Relations Supervisor Jeff Brown, Base Supervisor Base - (254) 680-3644 Fax – (254) 680-3573 Dispatch – 800-456-7477 Medical Director – Dr. Jeff Jarvis PHI Air Medical 6 – Corsicana Lora Murphy, Flight Nurse (214) 395-6033 9000 Old Navarro Road Corsicana, TX 75109 Fax – (903) 872-0201 Dispatch – 877-435-9744 Medical Director – Dr. Roy Yamada PHI Air Medical 12 – Bryan Billy Rice, Base Supervisor Base (936) Fax – Dispatch – Medical Director – Dr. Air Evac LifeTeam – Granbury (AEL 69) Martha Headrick, Base Manager HOTRAC Regional STEMI Plan March 2011 Page 9 Air Evac LifeTeam – 51 (West) HOTRAC Regional STEMI Plan March 2011 Page 10 Air Evac LifeTeam – HOTRAC Regional STEMI Plan March 2011 (Killeen) Page 11 Air Evac LifeTeam – 53 (Fairfield) HOTRAC Regional STEMI Plan March 2011 Page 12 Air Evac LifeTeam – 74 (Ennis) HOTRAC Regional STEMI Plan March 2011 Page 13 Air Evac LifeTeam – 69 (Granbury) HOTRAC Regional STEMI Plan March 2011 Page 14 PHI STAT Air 1 (Killeen Skylark Airfield) *divide the air miles by 2 for approximate ETA in minutes (i.e., 30 miles = 15 min ETA). HOTRAC Regional STEMI Plan March 2011 Page 15 PHI Air Medical 6 (Corsicana) *divide the air miles by 2 for approximate ETA in minutes (i.e., 30 miles = 15 min ETA). HOTRAC Regional STEMI Plan March 2011 Page 16 PHI Air Medical 12 (Bryan) *divide the air miles by 2 for approximate ETA in minutes (i.e., 30 miles = 15 min ETA). HOTRAC Regional STEMI Plan March 2011 Page 17 Heart of Texas Regional Advisory Council – TSA M TSA-M Acute Care Facilities Facility Falls Community Hospital (254) 803-3561 Fax (254) 803-6066 Goodall-Witcher Healthcare Foundation (254) 675-8322 FAX- (254) 675-8964 Hill Regional Hospital (254) 582-8500 FAX- (254) 582-2144 Hillcrest Baptist Medical Center (254) 202-2000 FAX-(254) 202-6605 Lake Whitney Medical Center (254) 694-3165 FAX-(254) 694-3299 Limestone Medical Center (254) 729-3281 FAX-(254) 729-3080 Parkview Regional Hospital (254) 562-5332 FAX-(254) 562-9279 Providence Health Center (254) 751-4000 Fax: (254) 751-4769 HOTRAC Regional STEMI Plan March 2011 Location PO Box 60 Marlin, TX 76661 Falls County 44 beds PO Box 549 101 South Ave. T Clifton, TX 76634 Bosque County 40 Beds 101 Circle Drive Hillsboro, Texas 76645 Hill County 92 Beds 100 Hillcrest Blvd Waco, Texas 76706 McLennan County 393 Beds PO Box 468 Whitney, Texas 76692 Hill County 49 Beds 701 McClintic Groesbeck, TX 76642 Limestone County 20 Beds 600 S Bonham Mexia, Texas 76667 Limestone County 59 Beds 6901 Medical Parkway Waco, TX 76712 McLennan County 230 beds AVERAGE DAILY CENSUS HOSPITAL-BASED EMS SERVICE ED DIRECTOR Administrator 15-20 No Tammy Samford, RN Willis Reese CEO 12-15 No Joyce McDowell, RN Clarence Fields President & CEO 30 No Annie Tucker, RN Jan McClure CEO 175 No Tamra Acierni, RN Glenn A. Robinson President & CEO 10-15 Yes 10-12 Yes George Black, RN Penny Gray CEO 30 No Marcy McFarland, RN, BSN vacant CEO 175 No Eileen Bohannon, RN Kent Keahey President & CEO Ruth Ann Crow Administration Page 18 System Participation All HOTRAC General Assembly meetings are open to any interested persons. Meeting notices and reminders are emailed to the membership well in advance of all meetings, and meeting notices are posted on the HOTRAC website. Minutes of all meetings are emailed and provided at each meeting, along with a meeting agenda. Active Participation in the RAC is defined as the following: A. EMS Provider Agencies 1. 2. 3. 4. 5. 6. 7. B. Hospital Members 1. 2. 3. 4. 5. 6. 7. 8. 9. C. Will have representation at 75% of General Assembly Meetings. Will participate in a minimum of one (1) standing committee and will have representation at 75% of that committee meetings. Will submit information into the Trauma Registry and attend any meeting when the agency has a referral on the agenda. Will demonstrate participation in at least one HOTRAC sanctioned prevention activity annually and submit documentation of such. Will submit required Performance Improvement data upon request. Will have physician representation at 75% of the Physician Advisory Committee meetings. Will participate in one community disaster preparedness drill per year. Will have representation at 75% of General Assembly Meetings. Will participate in a minimum of one (1) standing committee and will have representation at 75% of that committee meetings. If applicable, will have Trauma Coordinator attend at least 75% of the Hospital Care & Management Committee as well as participate in the Trauma System Plan development. If applicable, will have Stroke Coordinator attend at least 75% of the Stroke Committee as well as participate in the Stroke System Plan development. Will have physician representation at 75% of Physician Advisory Committee Meetings. Will demonstrate participation in at least one HOTRAC sanctioned prevention activity annually and submit documentation of such. Will submit information into the Trauma Registry and attend any meeting when the agency has a referral on the agenda. Will participate in 75% of scheduled preparedness activities. In the event of emergency healthcare activations, will participate as required by the Health & Medical Annex of the County Emergency Operations Plans and/or the Health & Medical Appendix of the Regional Response Plan. Non-EMS/Hospital Entities 1. 2. 3. Will have representation at 75% of General Assembly Meetings. Will participate in a minimum of one (1) standing committee and will have representation at 75% of that committee meetings. Will participate in at least one (1) scheduled regional preparedness activity. Meeting attendance may be met in person, via conference call, or via webinar. D. Each member entity will complete an annual Regional Needs Assessment by the 1st of March of each year. HOTRAC Regional STEMI Plan March 2011 Page 19 E. Membership Dues must be paid in full by each member by the 1 st of March of each year. Membership dues is charged as follows: Hospitals - $500.00 9-1-1 EMS Providers (including Air Medical) - $250.00 Other Members (i.e., FROs, Emergency Management, etc.) - $50.00 Individuals - $25.00 Participation from each organization is encouraged. The Bylaws are reviewed each year and revised as appropriate. Each component of the Regional STEMI Plan is presented, discussed, and approved by the HOTRAC General Assembly, Board of Directors, and Physicians Advisory Committee. All revisions are reviewed and approved through the same process. Once approved, complete copies of the Regional Trauma Plan will be distributed to the HOTRAC membership. System Access via 9-1-1 Goal The Goal for System Access within TSA-M is two-fold. First, rapid access to notification of the need for emergency cardiac care at any location within TSA-M must be available to all persons in the Region. Second, Emergency Medical Services (EMS) must be rapidly available to provide quality health care to injured or ill persons in each HOTRAC Community. In portions of this Region, First Responder Organizations (FRO) may provide initial treatment pending EMS arrival. Objectives 1. To ensure that all persons located in Trauma Service Area M will have the availability to access Emergency Dispatch for EMS services. 2. To ensure emergency healthcare providers have communication equipment available. 3. To strive to maintain an adequate number of first responders and EMS providers that have the knowledge, skills, and equipment needed to provide emergency care to persons requesting assistance within the Region. Discussion The 9-1-1 communications system provides a dedicated phone line allowing direct routing of emergency calls through a telephone company central office to a Public Safety Answering Point (PSAP). Routing is based on the specific telephone exchange area rather than municipal boundaries. Enhanced 9-1-1 includes Automatic Number Identification (ANI) and/or Automatic Location Identification (ALI). Enhanced 9-1-1 also automatically routes emergency calls to a pre-selected answering point based upon the geographical location from which the call originated. Each of the five HOTRAC counties has enhanced 9-1-1 with ANI/ALI capability. The 9-1-1 Advisory Committee of the Heart of Texas Council of Governments is responsible for the development, performance evaluation, and administration of the 9-1-1 system in rural HOTRAC counties. Representatives from each county meet on a regular basis to discuss system problems, plan educational activities, and work cooperatively to develop and implement the 9-1-1 Strategic Plan. In McLennan County, the McLennan County 9-1-1 District provides the same services to the entire McLennan County area. There is free public access to 9-1-1 throughout TSA-M. Public education programs such as the Red E. Fox program are used to educate consumers. Training sessions are provided at community health fairs, schools, auxiliaries, hospitals, Sheriff’s departments, and EMS providers. HOTRAC Regional STEMI Plan March 2011 Page 20 Communications Goal The Goal for Communications within TSA-M is to ensure communication capability between EMS providers, medical control, receiving facilities; and other First Responders entities. Rapid dispatch and notification of the need for emergency cardiac care at any location within TSA-M must be available to all persons in the region. Objectives 1. To facilitate regional communications, all EMS & first responder units as well as hospital emergency personnel will have a list of the communication devices & operating frequencies of the EMS and emergency care providers operating in the HOTRAC region. 2. To ensure that all EMS providers, First Responders, and hospital facilities in the HOTRAC region have functional communications equipment in order to communicate information related to the patient’s condition, the need for medical, EMS, or helicopter back-up, and to receive and communicate information related to patient care and disposition. 3. To ensure that emergency dispatch within the HOTRAC region is accomplished by persons who have the knowledge, skills, and equipment necessary to rapidly mobilize the appropriate level of emergency care to persons requesting assistance throughout the region. Discussion The communications network in TSA-M is comprised of UHF, VHF, and 800 MHz radio devices combined with telephone links, both cellular and base site. In some instances individual EMS providers utilize UHF, VHF, 800 MHz, and cellular phones to ensure communications capability. The use of multiple communications systems ensures regional communications are maintained between public and private EMS agencies, police, fire, and hospital entities. Dispatch - Emergency dispatch in each of the five HOTRAC counties is accomplished through various methods (i.e., sheriff’s office, local police department, or county 911 services). Pre-hospital Care Providers – Most of the EMS Providers utilize the VHF frequency while ETMC-EMS in McLennan County utilizes 800 MHz. Hospital Care Providers - All HOTRAC hospital facilities maintain communications capability with pre-hospital care providers through the use of UHF emergency radios, cellular phones, or standard phone lines. Cellular phones are the primary means of communications between EMS Providers and Hospitals. HOTRAC purchased each facility a HAM radio that is programmed as follows: HAM Radio Frequencies: CH Location Type Service 0 Alpha/Numeric W5BEC - ???? 147.140 147.740 123.0 Bell Amateur 1 W5BCR - Clifton 147.180 147.780 123.0 Bosque Amateur 2 KC5QHO - Comanche 146.680 146.080 110.9 Comanche Amateur 3 N5DDR - Gatesville 146.960 146.360 Coryell Amateur 4 WD5DDH - Waxahachie 145.410 144.810 Ellis Amateur 5 KB5TPP - Stephenville 147.360 147.960 110.9 Erath Amateur 6 WB5YJL - Fairfield 145.110 144.510 146.2 Freestone Amateur 7 WM5L - Hillsboro 146.780 146.180 123.0 Hill Amateur 8 WD5GIC - Granbury 147.080 147.680 110.9 Hood Amateur 9 KC5PGV - Cleburne 145.490 144.890 88.5 Johnson Amateur HOTRAC Regional STEMI Plan March 2011 Out In Tone Page 21 10 W5ZMI - Mexia 145.390 144.790 146.2 Limestone Amateur 11 W5ZDN - Hewitt 146.890 146.290 123.0 McLennan Amateur 12 W5ZDN - Moody 145.150 144.550 123.0 McLennan Amateur 13 AA5RT - Waco 146.660 146.060 123.0 McLennan Amateur 14 W5ZDN - Waco 146.880 146.280 123.0 McLennan Amateur 15 WA5BU - Waco 147.160 147.760 McLennan Amateur 16 AA5RT - Waco 147.360 147.960 123.0 McLennan Amateur 17 N5DDC -Corsicana 145.290 144.690 146.2 Navarro Amateur 18 WD5GND - Glen Rose 145.270 144.670 110.9 Somervell Amateur 19 WD5GIC - Glen Rose 147.020 147.620 110.9 Somervell Amateur 25 Simplex Point to Point 146.400 Amateur 26 Simplex Point to Point 146.410 Amateur 27 Simplex Point to Point 146.420 Amateur 28 Simplex Point to Point 146.430 Amateur 29 Simplex Point to Point 146.440 Amateur 30 Simplex Point to Point 146.450 Amateur 31 Simplex Point to Point 146.460 Amateur 32 Simplex Point to Point 146.470 Amateur 33 Simplex Point to Point 147.480 Amateur 34 Simplex Point to Point 146.490 Amateur 35 Simplex Point to Point 146.500 Amateur 36 Simplex Point to Point 146.510 Amateur 37 National Calling Frequency 146.520 Amateur 38 Simplex Point to Point 146.530 Amateur 39 Simplex Point to Point 146.540 Amateur 40 Simplex Point to Point 146.550 Amateur 41 Simplex Point to Point 146.560 Amateur 42 Simplex Point to Point 146.570 Amateur 43 Simplex Point to Point 146.580 Amateur CH Alpha/Numeric 20 24 Out In Tone Location Type Service 49 50 Simplex Point to Point 147.420 Amateur 51 Simplex Point to Point 147.430 Amateur 52 Simplex Point to Point 147.440 Amateur 53 Simplex Point to Point 147.450 Amateur 54 Simplex Point to Point 147.460 Amateur 55 Simplex Point to Point 147.470 Amateur 56 Simplex Point to Point 147.480 Amateur 57 Simplex Point to Point 147.490 Amateur 58 Simplex Point to Point 147.500 Amateur 59 Simplex Point to Point 147.510 Amateur 60 Simplex Point to Point 147.520 Amateur 61 Simplex Point to Point 147.530 Amateur 62 Simplex Point to Point 147.540 Amateur 63 Simplex Point to Point 147.550 Amateur 64 Simplex Point to Point 147.560 Amateur 65 Simplex Point to Point 147.570 Amateur 66 85 86 TX Fire 3 HOTRAC Regional STEMI Plan March 2011 154.2950 NOTE: Receive only Public Service Page 22 87 TX Fire 2 154.2650 88 TX Fire 1 154.2800 on Public Service Bands Public Service 89 TX Air 2 151.3850 90 TX Med 1 155.3400 Public Service 91 TX Law 3 155.4750 Public Service 92 TX Law 2 155.3700 Public Service 93 TX Law 1 154.9500 Public Service 94 Freestone EOC 155.7975 Public Service 95 Limestone EOC 155.9325 Public Service 96 Falls EOC 154.0025 Public Service 97 McLennan EOC 158.7750 Public Service 98 Hill EOC 155.6925 Public Service 99 Bosque EOC 155.8875 Public Service Public Service 127.3 Public Service HOTRAC is an active participant in the interoperability planning efforts being address by the Heart of Texas Council of Governments. HOTRAC strives to remain at Level 4 interoperability. HOTRAC follows the HOTCOG Regional Communications Plan. Please see that specific plan for additional detailed information regarding communications in the Region. Regional Pre-hospital Medical Oversight & Control Goal The goal for Regional Medical Control in TSA-M is multifaceted. - To ensure strong physician leadership and supervision for pre-hospital care providers in both on-line and off-line functions. - To secure medical involvement in regional planning and educational program development. - Provide for the development and implementation of regional treatment guidelines and system plan components, as well as in systems evaluation. . Objectives 1. To evaluate regional cardiac care from a systems perspective, under the direction of representatives of HOTRAC medical staff throughout the Region. 2. To involve HOTRAC medical staff in all phases and at all levels of the leadership and planning activities of regional development. 3. To ensure appropriate medical oversight of all pre-hospital care providers through a Performance Improvement (PI) process and other administrative processes. 4. To identify and educate regional medical control resources, standardize treatment protocols, and analyze accessibility of medical control resources. 5. To identify and educate HOTRAC EMS providers and sources of on-line and off-line medical control. Discussion The HOTRAC Region includes both rural and suburban hospital and emergency care providers with varying levels of medical capability. There is not a single EMS medical director for all EMS providers in the HOTRAC Region. All EMS medical directors are members of the HOTRAC Physician Advisory Committee, which meets on a quarterly basis. Physician Involvement in Regional Plan Development - The Physician Advisory Committee meets on a quarterly basis to conduct its usual business and to review and approve regional planning components, policies, and treatment guidelines HOTRAC Regional STEMI Plan March 2011 Page 23 related to medical care. Each EMS medical director and at least one physician from each HOTRAC hospital has representation on this standing committee. Any interested HOTRAC physician is invited to attend committee meetings. Medical Direction of Pre-hospital Care Providers - In accordance with DSHS guidelines, all HOTRAC pre-hospital care providers function under medical control. Regional EMS treatment guidelines are printed and distributed to all EMS providers for incorporation into local protocols. Periodic reviews and updates are completed and upon approval are distributed as necessary. These treatment guidelines serve as a baseline and individual Medical Directors may adapt for their local community. Regional Performance Improvement - The Physician Advisory Committee meets quarterly to conduct its usual business and to carry out regional performance improvement (PI) activities. The ED Directors/EMS Providers meet in conjunction with the Physician Advisory Committee to review patient care and evaluate outcomes from a systems perspective. PI indicators include a review of all STEMI patients. (Please see System PI section for more details). Pre-hospital Triage Goal Patients will be identified, rapidly and accurately assessed, and based on identification of their actual or suspected onset of symptoms, will be transported to the nearest appropriate TSA-M facility. Purpose In order to ensure the prompt availability of medical resources needed for optimal patient care, each patient will be assessed for the presence of abnormal vital signs; concurrent disease/predisposing factors; and abnormal EKG or 12-lead if available. System Triage If a provider is unable to complete an EKG or 12-lead, suspected cardiac patient should be taken to the nearest acute care facility within TSA M. If a provider suspects a STEMI (confirm by 12-lead), the patient should be taken directly to a PCI Facility within TSA M. If a provider is unable to provide MICU care to the suspected cardiac patient, paramedic intercept should be considered. Paramedic intercept may be by ground or air. If transport by ground to the nearest appropriate facility is more than 20 minutes, consider helicopter activation. Helicopter Activation Goal TSA-M regional air transport resources will be appropriately utilized in order to reduce delays in providing optimal cardiac care. Decision Criteria HOTRAC Regional STEMI Plan March 2011 Page 24 1. Helicopter activation/scene response should be considered when it can reduce transportation time for patients with: Pulmonary edema Altered Mental Status Hypotension OR A PCI Facility is more than 20 minutes away by ground. Should there be any question whether or not to activate TSA-M regional air transport resources, on-line medical control should be consulted for the final decision. 2. Patients transported via helicopter should be taken to the nearest PCI Facility within TSA M. Facility Diversion Goal TSA-M facilities will communicate “facility diversion” status promptly and clearly to regional EMS and other facilities through EMSystem in order to ensure that STEMI patients are transported to the nearest appropriate facility. System Objectives 1. To ensure that STEMI patients will be transported to the nearest appropriate TSA-M facility. 2. To develop system treatment guidelines for regional facility and STEMI diversion status (see EMSystem guidelines and protocols): Situations which would require the facility to go on diversion Notification/activation of facility diversion status Procedure for termination of diversion status 3. Regional cardiac care problems associated with facility diversion will be assessed through the Physician Advisory Committee PI process. 4. All facilities and pre-hospital providers will use EMSystem to notify and track diversion status. Facility Bypass Goal Suspected STEMI patients will be safely and rapidly transported to the nearest appropriate facility within TSA M. Decision Criteria Regional transport treatment guidelines ensure that patients who meet the triage criteria for activation of the TSA-M Regional STEMI Plan will be transported directly to the nearest appropriate PCI Facility rather than to the nearest hospital except under the following circumstances: HOTRAC Regional STEMI Plan March 2011 Page 25 1. If unable to establish and/or maintain an adequate airway, the patient should be taken to the nearest acute care facility for stabilization. 2. Medical Control may wish to order bypass when a facility is unable to meet hospital resource criteria or when there are patients in need of specialty care. 3. If expected transport time to the nearest appropriate PCI Facility is excessive (> 20 minutes), medical control or the EMS crew on scene should consider activating air transportation resources. 4. Additionally, should the patient or their cardiologist choose to bypass a PCI Facility, their request should be followed when possible. Note: Should there be any question regarding whether or not to bypass a facility, the receiving facility should be consulted. Facility Triage Criteria Goal The goal of establishing and implementing facility triage criteria in TSA-M is to ensure that all regional hospitals use standard definitions to classify STEMI patients in order to ensure uniform patient reporting and facilitate inter-hospital transfer decisions. Objectives 1. To ensure that each STEMI patient is identified, rapidly and accurately assessed, and based on identification and classification of their actual or suspected onset of symptoms, transferred to the nearest appropriate TSA-M facility. 2. To ensure the prompt availability of medical resources needed for optimal patient care at the receiving facility. 3. To develop and implement a system of standardized STEMI patient classification definitions. Discussion After a confirmed STEMI, a patient should be transferred immediately to the nearest PCI Facility within TSA M. If a PCI Facility receives and confirms a 12-lead, the PCI Facility should activate the facility’s Code STEMI protocol. Inter-Hospital Transfers Goal The goal for establishing and implementing inter-hospital transfer criteria in TSA-M is to ensure that those STEMI patients requiring additional or specialized care and treatment beyond a facility’s capability are identified and transferred to a PCI Facility as soon as possible. HOTRAC Regional STEMI Plan March 2011 Page 26 Objectives 1. To ensure that all regional hospitals make transfer decisions based on standard definitions which classify STEMI patients according to TSA-M criteria. 2. To identify cardiac treatment and specialty facilities within and adjacent to TSA-M. 3. To establish treatment and stabilization criteria and time guidelines for TSA-M patient care facilities. Discussion The level of cardiac care resources required for STEMI patients is outlined in the TSA-M facility triage criteria and prehospital triage criteria. When a suspected STEMI patient is identified activation of a Code STEMI should be initiated. A transferring facility should state that the patient is a “Code STEMI” when calling EMS and the accepting PCI Facility within TSA M. These criterions (see attached Regional STEMI Form) are monitored through the regional PI program. Identification of STEMI Patients & STEMI Transfers - STEMI patients and their treatment requirements for optimal care are identified in the TSA-M facility triage criteria and pre-hospital triage criteria. Written transfer agreements are available between all TSA-M hospital facilities, and hospital facilities in adjacent regions. STEMI patients with special needs may be initially transferred to a PCI Facility for assessment and treatment. When resources beyond its capability are needed, transfer to another facility outside TSA M should be expedited. The TSA-M initial-receiving hospitals may also choose to transfer patients with special needs directly to these facilities, bypassing the TSA M facilities when appropriate. STEMI Patient Transport - STEMI patients in TSA-M are transported according to patient need, availability of air transport resources, and environmental conditions. Many of the EMS Providers in the HOTRAC Region are MICU capable. Additionally, this Region has several air medical services that may be utilized. HOTRAC Regional STEMI Plan March 2011 Page 27 HOTRAC Regional STEMI Alert Form Date________ Symptom Onset Time: _________ Patient Name: _____________ DOB: ____________ Regional Goal: 90 minutes or less from initial medical contact to balloon inflation. □ Male □ Female EMS to complete this section EMS Provider: ________________________ □ Patient contact time:___________ □ 12-lead administered Time: _____________ □ 12-lead transmitted to facility Time: ___________ □ O2 _____ Lpm, via _____________ □ Started IV w/ ______ gauge □ 4 chewable baby aspirin (or equivalent) PO, unless contraindicated Time: __________ □ NTG 0.4 mg SL q 5 minutes x 3, unless contraindicated Time: __________ __________ __________ □ Other Treatment: _______________________________ _____________________________________________ Medic Name (Printed): ________________________ Signature: ___________________________________ RURAL HOSPITAL to complete this section □ □ □ Patient arrived at ________________ ED Time: _________ Activate Code STEMI Time: ____________ STAT EKG & continuous cardiac monitoring. Notify ED Physician: ________________________ Time: __________ □ O2 _____ Lpm, via ____________ □ Ensure 2 IV lines □ STAT lab: CBC, CMP, PT/PTT, CK, CKMB, Troponin I □ Chest Xray completed Time: ____________ □ 4 chewable baby aspirin (or equivalent) PO, unless contraindicated Time: __________ □ NTG 0.4 mg SL q 5 minutes x 3, unless contraindicated Time: _________ __________ ___________ □ Other Treatment: _______________________________ _____________________________________________ □ IF STEMI or left bundle branch block, call for acceptance of CODE STEMI Time Called: ______ Accept rec’vd: _________ □ Hillcrest □ Providence □ Other: __________________ □ Thrombolytics given Drug/Dose:____________________ Route: __________________ Time: ________________ □ Contact EMS (ground or air) for priority transfer Provider: ____________________ Time called: ___________ □ EMS arrived Time: _______ Patient leaves ED Time: _______ □ Call Cardiologist when patient has left facility. Nurse Name (Printed): ________________________ Signature: ___________________________________ TRANSFER – TRANSPORTING AGENCY: _____________________ □ Other Treatment: _____________________________________ ___________________________________________________ □ Status Change(s): ____________________________________ __________________________________________________ Signature: ____________________________________________ CATH LAB to complete this section □ Patient arrives in Cath Lab:______ □ Arrival of Interventionalist: ______ □ First Lesion Access:______ □ Reperfusion time/intervention complete: ______/______ □ ICU Notified for Room:______ □ Patient leaves Cath Lab: ______ Nurse Name (Printed): ________________________ Signature: ___________________________________ HOTRAC Regional STEMI Plan March 2011 STEMI FACILITY to complete this section □ □ □ Patient arrived at _________________ ED Time: ________ Activate Code STEMI Time: ____________ STAT EKG Time: ______ & continuous cardiac monitoring. Notify Cardiologist: ________________________ Time called: _________ Time Arrived: __________ □ O2 _____ Lpm, via ___________ □ Ensure 2 IV lines □ STAT lab: CBC, CMP, PT/PTT, AMIP □ Chest Xray completed Time: ___________ □ 4 chewable baby aspirin (or equivalent) PO, unless contraindicated Time: __________ □ NTG 0.4 mg SL q 5 minutes x 3, unless contraindicated Time: _________ __________ ___________ □ Other Treatment: _______________________________ _____________________________________________ □ Thrombolytics given Drug/Dose:____________________ Route: __________________ Time: ________________ □ Prep Patient for Cath: o Remove all patient’s clothes; hospital gown only o Name/allergy bands on patient o IV x 2 with extension tubing o IV: NS at KVO rate for primary line o Clip patient’s groin bilaterally o Place radiotransparent defibrillation pads at the right subclavicular and the left axillary areas (NOT over heart) o Connect patient to the portable monitor o Portable O2 tank on stretcher o Place consent on chart; ensure patient has signed consent after explanation from cardiologist o Place label on front of chart and ensure appropriate paper is included. □ Patient leaves ED for Cath Lab. Time: _________ Nurse Name (Printed): ________________________ Signature: ___________________________________ Place patient label here Page 28 Heart of Texas Regional Advisory Council STEMI Alert Form Standard Usage Guidelines Each facility within the HOTRAC Region will maintain copies of the HOTRAC Regional STEMI Alert Form in the Emergency Department. The HOTRAC Regional STEMI Alert Form will be completed on any patient with a suspected STEMI or Left Bundle Branch Blockage. For the purposes of this program the ‘STEMI patient’ shall be defined as any patient presenting with symptoms of an acute myocardial infarction and/or left bundle branch blockage and/or 1mm of ST-elevation in two contiguous EKG leads (STEMI). The HOTRAC Regional STEMI Alert Form is intended to document required information for the regional STEMI facilities as well as serve as the tool for the regional STEMI quality improvement process. When a suspected STEMI patient presents in the ED of a HOTRAC facility, that facility will initiate the HOTRAC Regional STEMI Alert Form by completing the top portion of the STEMI Alert Form. Initial EMS Provider The EMS provider will obtain a STEMI Alert form from the facility and complete the top portion of the form titled “EMS to complete this section”. The EMS provider shall complete the section fully. The EMS provider shall attach a copy of the initial 12 lead. The 12 lead shall be noted with the patient’s name and date of birth. If additional documentation is required, a copy of the run sheet may be attached to the EMS copy and forwarded to HOTRAC. HOTRAC will forward copies of additional documentation as appropriate. The paramedic/flight nurse must sign the completed section. Upon signature, the bottom copy shall be removed by EMS provider and maintained by the provider as part of their records for QI purposes. Once the EMS copy is removed, the form shall be given to the facility. Rural HOTRAC Facility When the patient arrives at a rural HOTRAC facility, the rural facility shall complete the section titled “Rural Facility to complete this section”. If the patient presents directly at the facility by his/her own means, the facility shall mark “N/A” across the EMS Section. The attending nurse must sign the completed section. Upon signature, the bottom copy shall be removed by the rural facility; a patient label is placed at bottom of the facility’s copy, and maintained by the facility as part of their records. Once the rural facility has removed its copy, the form shall follow the patient to the PCI Facility. Transferring EMS Provider When the patient is transferred from a rural facility to a regional PCI Facility, the transferring EMS provider (ground or air medical) shall complete the section titled “Transfer-Transporting Agency”. If additional documentation is required, a copy of the run sheet shall be attached to the EMS copy and forwarded to HOTRAC to be attached to the regional copy. HOTRAC will forward copies of additional documentation as appropriate. The paramedic/flight nurse must sign the completed section. Upon signature, the bottom copy shall be removed by EMS provider and maintained by the provider as part of their records for QI purposes. Once the EMS copy is removed, the form shall be given to the PCI Facility. HOTRAC PCI Facility When the patient arrives at a regional PCI Facility, the PCI Facility shall complete the section titled “PCI Facility to complete this section”. If the patient presents directly at the facility by his/her own means, the facility shall mark “N/A” across the EMS, Rural Facility, and Transfer Section. The attending nurse must sign the completed section and place a patient label at the bottom of the form. HOTRAC Regional STEMI Plan March 2011 Page 29 Upon signature, the form shall follow the patient to the cath lab. Cath Lab Once the patient arrives in the cath lab, the section titled “Cath Lab to complete this section” shall be completed by cath lab staff. The attending nurse must sign the completed section. Upon signature, the RAC copy shall be forwarded to HOTRAC upon completion for the regional quality improvement process. The PCI Facility shall maintain the original (top) sheet as part of the facility’s record. System Performance Improvement Goal The goals for system performance improvement in TSA-M are to establish a method for monitoring and evaluating system performance over time and to assess the impact of STEMI system development. Objectives 1. To provide a multidisciplinary forum for STEMI care providers to evaluate STEMI patient outcomes from a system perspective and to assure the optimal delivery of cardiac care. 2. To facilitate the sharing of information, knowledge, and scientific data. 3. To provide a process for medical oversight of regional STEMI and EMS operations. Discussion In order to assess the impact of regional STEMI development, system performance must be monitored and evaluated from an outcomes perspective. A plan for the evaluation of operations is needed to determine if system development is meeting its stated goals. Authority - The authority and responsibility for regional quality improvement rests with the Regional Advisory Council. This will be accomplished in a comprehensive, integrated manner through the work of the Physician Advisory, Cardiac, and Prehospital Committees. Scope & Process - The Physician Advisory Committee serves as the oversight committee for regional performance improvement. Referrals for follow-up and feedback to & from the Committee and providers ensure system-wide, multidisciplinary performance improvement. The Cardiac Committee will develop the type of data and manner of collection, set the agenda for the PI process within the regularly-scheduled meetings of the committee, and identify the events and indicators to be evaluated and monitored. Indicator identification will be based on high risk, high volume, and problem prone parameters. Indicators will be objective, measurable markers that reflect STEMI resources, procedural/patient care techniques, and or systems/process outcomes. The Physician Advisory Committee will have final approve of the PI process. Occurrences will be evaluated from a system, outcomes prospective and sentinel events will be evaluated on a case by case basis. Activities and educational offerings will be presented to address knowledge deficits and case presentations or other appropriate mediums will be designed to address systems and behavioral problems. All actions will focus on the opportunity to improve patient care and systems operation. The results from committee activities will be summarized and HOTRAC Regional STEMI Plan March 2011 Page 30 communicated to the RAC membership. Problems identified that require further action will be shared with the persons and entities involved, for follow-up and loop closure. Committee follow-up and outcome reports will be communicated on a standard format (please see attached). The functions and effectiveness of the HOTRAC Performance Improvement Process will be evaluated on an annual basis in conjunction with the annual evaluation of the HOTRAC Regional STEMI Plan. All PI activities and committee proceedings are strictly confidential. Individuals involved in performance activities will not be asked to review cases in which they are professionally involved, but will be given the opportunity to participate in the review process. Data Collection - PI data will be collected by the Cardiac Coordinator. PI forms and summary reports are submitted by each HOTRAC hospital facility and EMS provider to HOTRAC Staff. Sentinel events will be used to focus attention on specific situations/occurrences of major significance to patient care outcomes. Confidentiality - All information and materials provided and/or presented during PI meetings are strictly confidential. See attached form. HOTRAC facility and EMS provider data related to the following PI indicators are reviewed during the quarterly Physician Advisory meetings. The STEMI Alert Form is reviewed and updated annually. Reporting Quarters. HOTRAC regional PI data-reporting quarters are as follows: First Quarter: Second Quarter: Third Quarter: Fourth quarter: HOTRAC Regional STEMI Plan March 2011 Jan-Feb-Mar April-May-June July-August-Sep Oct-Nov-Dec Reporting at: Reporting at: Reporting at: Reporting at: May meeting August meeting December meeting February meeting Page 31 HOTRAC Regional Performance Improvement Statement of Confidentiality Medical Performance Improvement provides an objective mechanism to evaluate trauma and emergency care, facilitates the sharing of information, knowledge, and scientific data, and provides a forum for medical directors and other physicians to review the performance of the regional systems to assure the optimal delivery of trauma and emergency care. The direction of the committee comes from the Texas EMS Rules: Section 157.124 Regional EMS Trauma Systems: (3) (k) of the EMS Rules (effective 2/17/92) requires the development of a “performance management program that evaluates outcome from a system perspective” Committee members engaged in medical care review have protection from disclosure of proceedings, under Section 773.095 RECORDS OF PROCEEDINGS CONFIDENTIAL of the Texas Health and Safety Code as follows: (a) The proceedings and records of organized committees of hospitals, medical societies, emergency medical service providers, or first responder organizations relating to the review, evaluation, or improvement of an emergency medical services provider, a first responder organization, or emergency medical services personnel are confidential and not subject to disclosure by court subpoena or otherwise. (b) The records and proceedings may be used by the committee only in exercise of proper committee functions. (c) This section does not apply to records made or maintained in the regular course of business by an emergency medical services provider, a first responder organization, or emergency medical services personnel. Section 773.096 IMMUNITY FOR COMMITTEE MEMBERS “A member of an organized committee under Section 773.095 is not liable for damages to a person for an action taken or recommendation made within the scope of the functions of the committee if the committee member acts without malice and in the reasonable belief that the action or recommendation is warranted by the facts known to the committee member.” CONFIDENTIALITY As a participant in this HOTRAC regional performance improvement process, I understand and agree that all information and materials provided and/or presented during the meeting are strictly confidential. Meeting & Date: Physicians Advisory Meeting – HOTRAC Regional STEMI Plan March 2011 Page 32