Past Exam 1 for University of Minnesota students
advertisement

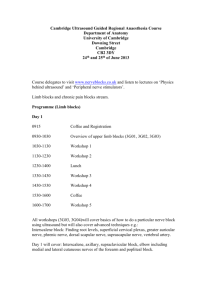
Anatomy K-Coop: 2003 Exam 1 Explained 1 of 20 Hi first years! Good luck on your first exam, I know you’ll do well. A great group of 2nd years went over the first exam from last year and explained the answers. Every person had their own style for answering the questions so the explanations and information may differ from section to section. Anything in italics is part of the explanation. Tanya Bailey bail0238@umn.edu Writers Angie Voight Tate Gisslen Paul Luikart Krista Wilhelmson Zubaid Rafique questions 1-10 and cutaneous innervation of the hand (a-e) questions 11-22 and vertebral short answer (a-e) questions 23-34 and matching #1 questions 35-44 and cross section of thigh (a-e) questions 45-54 and matching #2 ______________________________________________________________________ Examination 1: Extremities & Back Fall 2003 ______________________________________________________________________ MULTIPLE CHOICE and SHORT ANSWER: For the following multiple choice questions select the single best response for each of the following. Record your answer on the bubble sheet. There are also diagrams to be labeled. An answer sheet for the diagrams is found on the last page of the exam. Write your answers on the answer sheet page, as legibly as possible, and they will be graded by hand. Notice that the multiple choice questions are vignettes that continue for two or more questions. A short set of asterisks (****) will separate one vignette from the next. All multiple choice questions are worth 1 point. David Harleyson was riding his scooter home from his anatomy lab when he hit a curb in his parking lot and crashed. Flying from the scooter he landed on his head and shoulder. Although he had a ‘hurt bad’ feeling, he was able to get to his apartment. After much pain removing his shirt, he could not see any difference between his injured and his uninjured shoulders. However, when he pushed down on his acromion, the pain was intense. 1. What ligament did David most likely stretch or tear in this accident? A. the coracoclavicular If this ligament tore, the shoulder would fall away from the clavicle (Moore & Dalley pg 787). B. the acromioclavicular The AC joint is weak and easily injured by a direct blow (Moore & Dalley 787). C. the coracoacromial The coracoacromial arch is so strong that the humeral body or clavicle would fracture first (Moore & Dalley 790). D. the costoclavicular This is located between the first rib and the clavicle, not near the acromion where the pain is (Moore & Dalley 784). E. none of the above Anatomy K-Coop: 2003 Exam 1 Explained 2 of 20 The next morning David noticed some numbness on the lateral aspect of his forearm. Fearing his injury may be worse than he thought, he went to the doctor. The doctor, suspecting a brachial plexus injury, noticed weakness in David’s ability to flex at the elbow joint. 2. Given these symptoms, what nerve has definitely been compromised in the accident. (See Moore & Dalley pages 710-711 for the distribution of each nerve) A. the radial nerve B. the ulnar nerve C. the musculocutaneous nerve It innervates the brachialis, which flexes the forearm. It becomes cutaneous in the lateral forearm. D. the medial pectoral nerve E. the median nerve Never missing an opportunity to teach a student the value of anatomical knowledge as it relates to physical exam, she quizzes another student who was observing her exam of David on the cutaneous innervation of the forearm and hand. Supposing you were this student, name the cord of the brachial plexus which supplies the innervations to the regions of the forearm and hand labeled in the following figure of the palmar surface from Netter’s atlas. Cutaneous Innervation of Hand (Netter plates 413 and 455) A. ________lateral_______ B. ________medial_______ C. ________posterior_____ D. ___lateral and medial__ E. ________medial_______ Anatomy K-Coop: 2003 Exam 1 Explained 3 of 20 3. What kind of an injury does the physician suspect has occurred as a result of David’s fall? A. an injury to the ventral rami forming the upper brachial plexus Injuries to superior parts of the brachial plexus (C5 and C6) usually result from an excessive increase in the angle between the neck and the shoulder (Moore & Dalley 716). B. an injury to the ventral rami forming the lower brachial plexus 4. Given that the physicians suspicions are correct, and given David’s symptoms of lateral forearm numbness and weakness in the flexor compartment of the arm, which of the following muscles do you also suspect will be weakened as a result of the injury? A. pectoralis minor Innervated by the medial pectoral nerve. B. dorsal interosseous muscles of the hand Innervated by the ulnar nerve (from C8 and T1) C. infraspinatus muscle Innervated by the suprascapular nerve (from C5 and C6) D. serratus posterior superior Innervated by the 2nd-5th intercostals nerves ****** A young woman presented to her physician with a mass in the cubital fossa. It had been getting larger over the last month and the woman became worried when she began to sense tingling and numbness in her finger tips, especially when she flexed her forearm at the elbow. The contents of the cubital fossa, from medial to lateral, include the Median nerve, the brachial Artery, the Tendon of biceps brachii, and the Radial nerve. (MATR) 5. Remembering her anatomy, the physician knew exactly which of her fingers would be tingling and numb. Which ones? (Netter plate 455) A. index and middle fingers Innervated by the median nerve, which supplies cutaneous innervation to the thumb, index finger, middle finger, and half of the ring finger. B. little finger and part of the ring finger Innervated be the ulnar nerve, which is not in the cubital fossa. Realizing that the mass would have to be removed, the patient was prepped for surgery. In planning her approach, the physician used the tendon of the biceps brachii as a landmark. 6. On which side of the biceps tendon was the nerve located that was being impinged by the mass. A. medial side Medial │MATR │ Lateral B. lateral side In an effort to control the bleeding that might occur when the mass was cut free, the physician isolated the brachial artery in the cubital fossa. Anatomy K-Coop: 2003 Exam 1 Explained 4 of 20 7. On which side of the nerve (being impinged by the mass) was the brachial artery most likely to be found? A. medial side B. lateral side Medial │MATR │ Lateral 8. Did the surgeon incise the bicipital aponeurosis to gain access to the mass? A. yes The bicipital aponeurosis is a triangular membranous band that runs from the biceps tendon across the cubital fossa and merges with the antebrachial fascia covering the flexor muscles in the medial side of the forearm. (Netter plate 463, Moore and Dalley pg 721) B. no **** A (very naughty) little boy fell while running down the hall with scissors in his hand. The scissors stabbed him in the lateral side of the thorax, went entirely through the skin and were prevented from puncturing a lung by hitting a rib. The wound bled rather profusely, but the wound did not appear to be life threatening. The bleeding was controlled by pressure on the lateral side of the thorax. 9. What artery was likely responsible for the bleeding? (See Moore and Dalley 702-703, Netter plates 410, 412, 417). A. long thoracic artery B. lateral thoracic artery It descends along the lateral border of the pectoralis minor and onto the thoracic wall. C. thoracodorsal artery To latissimus dorsi muscle. D. an intercostals artery In the intercostals spaces. Several days after the accident, you notice a transient protrusion over the scapular region of the boy’s back whenever he pushes with his arms against something. Remembering your anatomy, you realize that he has also injured a nerve when he was stabbed by the scissors. This injury is to the serratus anterior muscle and is known as a winged scapula (Moore and Dalley 689). 10. What nerve did he injure? (See Moore and Dalley 691) A. thoracodorsal nerve Innervates latissimus dorsi muscle. B. lower subscapular nerve Innervates teres major and subscapularis. C. long thoracic nerve Innervates serratus anterior (Netter plate 412). D. a lateral intercostal nerve Innervates the skin of the thoracic and abdominal walls (Moore and Dalley 85). E. lateral thoracic nerve Anatomy K-Coop: 2003 Exam 1 Explained 5 of 20 **** A medical student in her Ob/Gyn roatation is trying to stay quietly in the background when suddenly several patients on the floor go into labor simultaneously. Needing all the help she can get, the attending physician hands the student a needle and instructs her to administer an epidural block to one of the patients. After a few minutes of composed panic, the student remembers the opening for administering an epidural. 11. This opening would be the… A. ventral sacral foramina - exits for ventral rami of sacral spinal cord located on ventral surface of sacrum B. posterior sacral foramina - exits for dorsal rami of sacral spinal cord, located lateral to median sacral crest C. sacral hiatus - Epidural anesthesia is injected through the sacral hiatus, located between the sacral cornua and inferior to the median sacral crest (used as landmarks), and filled with fatty connective tissue. Anesthesia rises through the sacral canal and acts on S2 through Coccyx spinal nerves of the cauda equina causing sensation loss inferior to the block. (Netter plate 150, Moore&Dalley p. 444-445, 484) D. none of the above are correct 12. As the student inserts the needle, she is careful not to put it in too far so as to avoid… A. puncturing the lumbar cistern- The lumbar cistern is the enlargement of the subarachnoid space within the dural sac, caudal to the medullary cone, (L2-S2) containing the cauda equina. A needle inserted to far will puncture the dural sac and cause excessive anesthesia. (Moore&Dalley 482, 484) B. damaging the cauda equina- The cauda equina is located within the lumbar cistern, but not damaged by needle insertion (see lumbar puncture M&D 482) C. injecting an intervertebral disk in this area- Intervertebral disks stop at L5 and are anterior to the spinal cord (not reachable or damageable from the sacral hiatus). D. injecting the terminal end of the spinal cord- The terminal end of the spinal cord is at L1-L2, the medullary cone E. damaging the delicate denticulate ligaments- denticulate ligaments suspends the spinal cord at the most inferior between T12 and L1 nerve roots, quite far from the entrance of the sacral hiatus. **** After teaching anatomy all day every day for a couple of weeks, one of your anatomy instructors began having pain in his hip area. The pain seemed to get more intense during the day but was better in the morning. One day, while helping students turn a rather large cadaver, he felt a distinct snap followed by a sharp pain shooting down his leg. Anatomy K-Coop: 2003 Exam 1 Explained 6 of 20 13. What most likely caused the ‘snap’? A. rupture of a lumbar lamina-bone connecting pedicle to spinous process, less likely to ‘rupture’. B. rupture of a lumbar intervertebral disk- i.e. Herniation of nucleus pulposus-usually occur due to hyperflexion and in adults where discs are weakened. Usually posterolateral due to thinner part of annulus fibrosus causing herniation into cauda equina and explaining pain felt in leg. (Moore&Dalley 451) C. rupture of a lumbar vertebral body- bone of vertebra held apart by discs, less likely to ‘rupture’ 14. What structure was impinged upon to cause his leg pain? A. B. a ventral ramus contributing to the sciatic nerve-ventral rami are adjacent to the spinal cord due to discs being located ventral to the cord. a dorsal ramus contributing to the sciatic nerve Several months later, this anatomy professor decides to undergo a surgical repair of his lower back. You are observing the orthopedic surgeon doing the procedure. When the surgeon discovers you have taken anatomy, she begins to quiz you on the vertebral anatomy in the region. 15. She shows you the following picture and asks you which is a lumbar vertebra? (A, B, or C) A-Lumbar vertebra heave a large vertebral body, a thick spinous process, a medially facing superior articular process, thin transverse process and a vertebral foramen larger than that of a thoracic vertebra (Netter 147-148) She also asks you to identify the features of the vertebra labeled ‘B’. (Netter 147) A. vertebral body B. pedicle C. transverse costal facet D. transverse process E. spinous process Anatomy K-Coop: 2003 Exam 1 Explained 7 of 20 In addition to the injury to lumbar vertebra, this anatomy professor also has a pronounced stoop and an abnormal increase in the anteroposterior dimension of the thorax. 16. What is this type of shape in the spine called? A. scoliosis- abnormal lateral curvature accompanied with rotation of vertebrae B. lordosis- (hollow back, sway back) anterior rotation of pelvis producing abnormal lumbar curvature; vertebral column curves anteriorly C. kyphosis- (humpback, hunchback) characterized by abnormal increase in thoracic curvature resulting from anterior deterioration of anterior part of one or more vertebra (Moore&Dalley 434) D. pronounced secondary curvature defect- cervical and lumbar curvatures that begin to appear during the fetal period but are not obvious until infancy; caused mainly by differences in thickness between anterior and posterior parts of IV disks E. spina bifida- lamina of L5 and/or S1 fail to develop and fuse ***** A water skier coming toward the dock at the end of a great run decides to come in a little faster than normal in order to spray his onlookers with his ski. Unfortunately, he miscalculates his distance from the dock versus the speed of his approach and crashes into one of the dock support beams. He takes a direct hit on his tibial tuberosity, displacing his tibia posteriorly relative to the femur. This is a bad injury for sure. 17. Which of his cruciate ligaments was certainly torn in this accident? A. anterior cruciate ligament- Slack when knee is flexed and taut when it is fully extended, preventing posterior displacement of temur on tibia and hyperflexion. Anatomy K-Coop: 2003 Exam 1 Explained 8 of 20 B. posterior cruciate ligament- tightened during flexion, prevents anterior displacement of the femur on the tibia and hyperflexion of the knee; often torn during head-on collisions without seatbelts (Moore&Dalley620-626) Being the only person on the dock with any anatomical experience, you decide to have a look at the injury before the EMTs arrive. In addition to the displaced proximal tibia, you notice that the skier’s leg and foot are turning blue relative to his other leg. You suspect that an artery has been torn or pinched in the accident. 18. Which artery is likely to be directly injured? A. the femoral artery-main artery of the anterior thigh, enters adductor hiatus B. the popliteal artery-emerges from adductor hiatus in popliteal fossa, posterior to knee. (Netter 498-500) C. the posterior tibial artery- continuation of popliteal artery, deep to soleus muscle, inferior of knee joint D. the peroneal artery- branch of posterior tibial inferior of knee 19. Why is it that an injury like this can cause a complete lack of blood flow to the leg? A. there is no arterial anastomosis around the knee joint- for knee anastamosis see Netter 494 B. the anastomotic network around the knee joint cannot accommodate an acute occlusion of the primary artery across the knee- Popliteal artery is main blood supply for ant. tibial, post. tibial, and peroneal arteries (Netter 494) C. all of the anastomotic arteries around the knee were probably also blocked in this injury- unlikely, too many to be blocked, several go around the joint **** A very accomplished snow skier is cruising down the slopes when she loses control on a turn. The skier goes airborne off of the turn and hits a tree, with her knee fully flexed, directly on the distal end of the femur. An X-ray at the hospital confirms your suspicion that the femoral neck has been broken. The physician in charge is worried about loss of blood supply to the skier’s hip, since the supply is easily compromised in such an injury. 20. What vessel is the primary source of blood to the head and neck of the femur? A. the obturator artery- supplies head of femur through ligament of head of femur B. the medial circumflex artery- See Tony Weinhaus’ notes “between iliopsoas tendon and pectineus muscle before going posterior to femur, supplies blood to head and neck of femur” (Netter 486, 494) C. the lateral circumflex artery- anterior to femur, some blood to neck D. the inferior gluteal artery- supplies muscles of gluteal region E. the internal pudendal artery- goes to perineum with pudendal nerve Anatomy K-Coop: 2003 Exam 1 Explained 9 of 20 One artery gives rise to a branch that supplies only the head of the femur. If this artery is injured, the head of the femur may die for a lack of blood supply (aseptic vascular necrosis). 21. Which artery supplies a branch only to the head of the femur? A. the obturator artery- See Tony Weinhaus’ notes “branch of obturator passes through the ligament of the head of the femur to supply the head of the femur” (Netter 486) B. the medial circumflex artery- see explanations for Q 20 C. the lateral circumflex artery- see explanations for Q 20 D. the inferior gluteal artery- see explanations for Q 20 E. the internal pudendal artery- see explanations for Q 20 Although accidents like the one described above do happen, fractures and dislocations of the hip are relatively uncommon. This is because the hip joint is very stable and there are many muscles that pass from the pelvis to the femur that stabilize the joint. Many of these muscles are lateral rotators of the hip that attach to the greater trochanter. 22. Which of the following muscles attaches to the greater trochanter of the femur but does not laterally rotate the hip? A. gluteus maximus- inserts 1/3 gluteal tuberosity of posterior femur and 2/3 iliotibial tract B. gluteus medius- inserts on greater trochanter, abduct thigh and stablize pelvis (Netter 472-473) C. obturator internus- inserts on greater trochanter, laterally rotates thigh D. obturator externus- inserts on trochanteric fossa, laterally rotates thigh E. piriformis- inserts on greater trochanter, laterally rotates thigh A third year medical student in her surgery rotation is shadowing a vascular surgeon. One afternoon the surgeon is called for a consult on a patient who has just undergone an angioplasty via the femoral artery (PTCA). The patient’s hemoglobin level is dropping and the interventional cardiologist who did the procedure is suspicious of a femoral artery bleed. The vascular surgeon concurs and they decide to do a femoral cut-down to expose the vessel, find the source of the bleeding and close it. The surgeon feels for the femoral pulse and cuts down over the vessel. The surgeon is acutely aware that the femoral nerve must not be damaged and asks the third year student if she remembers where the nerve is located. 23. On which side of the femoral artery is the femoral nerve located? A. medial B. lateral- For the femoral sheath from lateral to medial think NAVL (nerve, artery, vein, lymph) 24. Is the femoral nerve found within the femoral sheath? A. yes B. no- For the femoral sheath the nerve is not in it, the rest of NAVL are. Anatomy K-Coop: 2003 Exam 1 Explained 10 of 20 Having cut into the femoral sheath and isolated the femoral artery, the surgeon quickly finds and repairs the bleed. She notices that the femoral artery was bleeding adjacent to what looked like the medial circumflex artery. This is unusual since the medial circumflex is usually a branch of the deep femoral. However, the surgeon was convince that this branch was the medial circumflex because of the course of this artery. 25. The medial circumflex artery passes… A. between the pectineus and adductor longus muscles B. between the pectineus and the iliopsoas muscles- This is a landmark to know, see Netter plate 470 for more info. C. between the adductor longus and brevis muscles D. superficial to pectineus and adductor longus As the surgeon was observing the medial circumflex artery, she noticed what appeared to be a protrusion of small bowel (intestine). She knew immediately that the patient had a femoral hernia. 26. Through what space does a femoral hernia pass into the femoral triangle? A. medial to the femoral sheath B. through the femoral canal C. through the inguinal canal Femoral hernia, so C is wrong, between the other two, this is just a fact to know. The occur through the femoral ring and into the the femoral canal. Femoral hernias happen most often in the ladies. **** Knowing that you are taking the Gross Anatomy course, your neighbor runs to your yard from across the street to ask you an anatomy question. She said that while giving golf lessons to her son, he accidentally struck her in the leg with a 7-iron. She then points to a bruise located two inches inferior to the head of her fibula on the lateral side of her leg. 27. When the 7-iron hit her leg, which cutaneous nerve transmitted the pain of the impact? A. tibial nerve B. posterior cutaneous nerve of the thigh C. deep peroneal nerve D. superficial peroneal nerve E. lateral sural nerve-Check out plate 520 and 522 for a picture of the cutaneous nerve supply of the legs. She knows that she cannot seem to extend her foot at the ankle. Upon performing a pinprick test, you find out that she has no sensitivity between her first two toes. Anatomy K-Coop: 2003 Exam 1 Explained 11 of 20 28. Which nerve are you certain that she has injured? A. tibial nerve B. common peroneal nerve C. deep peroneal nerve - The pin prick test in that place shows that it is the deep peroneal nerve (plate 524). D. superficial peroneal nerve E. sural nerve Upon determining that in addition to her other symptoms, she also has no sensitivity over most of the rest of the dorsum of her foot. 29. Which nerve would you tell her that she has damaged? A. tibial nerve B. saphenous nerve C. deep peroneal nerve D. superficial peroneal nerve - Again, look at plate 524 to see the cutaneous innervation of the dorsal foot. E. sural nerve 30. Innvervation to which of the following muscles to you suspect is also affected? A. dorsal interosseous muscle B. lumbricals C. plantaris D. short head of biceps femoris E. none of the above Ok, A is wrong because that is innervated by the lateral plantar branch off the tibial nerve, B is wrong because that innervation is from the medial and lateral plantar branches of the tibial nerve. C is from the tibial nerve. D is from the peroneal nerve, but you need to remember where the neighbor was hit was below this muscle. Since none of these are right E is correct. **** Driving home from the Minnesota State Fair, a couple of fair-goers were in a one-car accident. The driver of the car was struck violently with the steering wheel just at the level of the superior pubic ramus. The attending physician tells you that this person has received a crushing injury to the femoral nerve just after it emerged from the pelvis. What do you expect the functional deficits to be in an injury of this sort? 31. Do you expect the patient to be able to extend at the knee joint? A. yes B. no - Femoral nerve does knee extension Anatomy K-Coop: 2003 Exam 1 Explained 12 of 20 32. Do you expect the patient to be able to flex at the hip joint? A. yes- That no good rascal the iliopsoas flexes the hip joint via lumbar nerves. B. no 33. Do you expect the adductor compartment to be significantly affected? A. yes B. no - That is innervated by the obturator nerve so wouldn’t be affected 34. What area of sensory innervation do you expect will be completely normal? A. skin over the anterior thigh B. skin over the lateral leg -This skin is innervated by the peroneal nerves branches. Since this isn’t part of the femoral nerve and comes out of the greater sciatic foramen it isn’t affected. C. skin over the medial leg MATCHING (#1). There are certain bony structures and location sin the body that serve as insertion points for multiple muscles. This tends to make these structures clinically, as well as anatomically, important. For the following structures, list the muscles that are attached in the spaces provided. In some cases there are actually more muscles attached than there are spaces. Just give three for credit. RECORD YOUR ANSWERS IN THE SPACE PROVIDED ON THE LEFT AND THIS SECTION WILL BE GRADED BY HAND. This question is worth a total of 4 points (you must have three correct muscles for each to get credit). coracoid process of scapula: coracobrachialis biceps brachii short head pectoralis major See Netter plate 409. greater tubercle of humerus: supraspinatus infraspinatus teres minor See Netter plate 404 pes anserinus on medial aspect of tibia: Sartorius, gracilis semitendonosus See Netter plate 472. This is a common question. Anatomy K-Coop: 2003 Exam 1 Explained 13 of 20 calcaneus bone of the foot: soleus gastrocnemius plantaris flexor digitorum brevis abductor digiti minimi abductor hallucis quadratus plantae See Netter plate 497, 515, and 516 The passenger in the car has just finished his last Pronto Pup and was holding the stick in his hand. At impact, the stick was thrust into his upper anterior thigh. The cross section of the injury is shown in the next figure. The stick punctured the deep femoral artery, accounting for the profuse bleeding in the area and continued into his medial thigh. Name the three muscles (labeled a, b, and c) that were pierced by the Pronto Pup stick. A. __Sartorius____________ B ___Pectineus___________ C. __Adductor Brevis______ OK, kids, go to Netter plate 487 and memorize it. Memorize the cross-sections for the arm as well. First get an understanding of the compartments of the legs (ie hamstrings on the back) and then go from there. For these questions, first determine if you are looking at the arm of the leg (I know this sounds basic, but people panic). Then determine if you’re proximal or distal. A good knowledge of where muscles attach and insert will also help you here. Anatomy K-Coop: 2003 Exam 1 Explained 14 of 20 MATCHING (#2). In anatomy, we often identify one structure in light of another structure that is usually found close to it, or in some constant relationship to it.. So, for each of the following structures, select the letter of the structure from the list in the right hand column that is BEST associated with, is represented by, or serves as a definitive landmark for, the structure listed or described in the left hand column. Use an answer only once. RECORD YOUR ANSWERS IN THE SPACE PROVIDED ON THE LEFT AND THIS SECTION WILL BE GRADED BY HAND. This question is worth a total of 5 points. __L____ pudendal nerve __D___ ulnar nerve __H___ piriformis muscle __K___ musculocutaneous nerve __G___ axillary nerve __F___ deltoid branch of thoracoacromial artery __A___ scaphoid bone __B___ deep branch of radial nerve __C___ medial pectoral nerve __I___ radial nerve A. B. C. D. E. F. G. H. I. J. K. L. anatomical snuff box supinator muscle pectoralis minor medial humeral epicondyle lateral humeral epicondyle cephalic vein quadrangular space gluteal arteries triangular interval pronator muscle coracobrachialis muscle sacrospinus ligament . ============================================================= EMBRYOLOGY ============================================================= For the following multiple choice Embryology questions, select the single best response for each of the following. Record your answer on the bubble sheet. 35. Cells that give rise to the gametes originate within: A. the primary ectoderm (epiblast) - Remember, cells of the epiblast undergo gastrulation to form the 3 primary germ layers. Key fact: Everything that becomes a baby comes from the epiblast. B. the primary endoderm (hypoblast) C. the extraembryonic mesoderm D. Heuser’s membrane E. none of the above 36. When does a primary oocyte complete its first meiotic division? A. at ovulation B. after the ovulatory surge of FSH and LH- OK… so know this: Oogonia (46, 2N) enter meiosis I and replicate to form primary oocytes (remember that there’s two stages of meiosis). A woman has all her primary oocytes by her 5th month of development. The oocytes finish meiosis I at the ovulatory surge of hormones to become secondary oocytes. Ovulation occurs when the secondary oocytes’ chromosomes align at metaphase of meiosis II. Meiosis II is not finished until fertilization. Anatomy K-Coop: 2003 Exam 1 Explained 15 of 20 C. D. E. at fertilization at 5 months of fetal life before birth 37. Which of the following is true regarding gametogenesis? A. male gametogenesis is discontinuous and results in 4 equal gametes B. the male gamete is fully mature after the process of spermiation C. the secondary oocyte arrests at the second meiotic metaphase - See the explanation for 36. With boys, at puberty, dormant primordial germ cells differentiate into type A spermatogonia which then undergo mitosis (not meiosis) to form more type As and also type B spermatogonia. Type B undergo meiosis to form a continuous supply of sperm. Meiosis never stops, it is ongoing, unlike in the female cycle. A is wrong because male gametogenesis is continuous. B is wrong because the sperm needs to undergo capacitation as well. D is wrong because the primary oocyte does not have a polar body, the secondary oocyte does. D. prior to puberty the primary oocyte and the first polar body are dormant at the first meiotic prophase E. none of the above 38. Heuser’s membrane is formed from the: A. epiblast B. hypoblast - OK, so I couldn’t find Heuser’s membrane in any of my USMLE review books, so how important can it be… Remember that epiblast = baby and Heuser’s membrane is not part of the baby. ** Heuser’s membrane = exocoelemic membrane and is derived from hypoblast which was initially formed from the inner cell mass or “embryoblast” C. epiblast and hypoblast D. embryoblast E. cytotrophoblast 39. A complete hydatidiform mole: A. causes Prader-Villi carcinoma B. has a triploid karyotype C. produces high levels of Human Chorionic Gonadotropin (hCG) - In a hydatitiform mole, something happens to the blastocyst and the embryo dies, but the trophoblast proliferates like mad. The clinical signs include preeclampsia in the first trimester, elevated HCG, and an enlarged uterus with bleeding. A is wrong because this disorder doesn’t exist. PraderVilli is a genetic abnormality. B and D are simply incorrect for this disorder. D. suggests that the paternal complement is responsible for the early development of the embryo E. all of the above Anatomy K-Coop: 2003 Exam 1 Explained 16 of 20 40. Human Chorionic Gonadotropin (hCG): A. is produced by the cytotrophoblast B. enters the maternal blood circulation - This is true… hCG is the basis of pregnancy testing (using blood). A is wrong because it is produced by the syncytiotrophoblast. C is wrong because it stimulates the production of progesterone. D is wrong for the same reason A is wrong. C. stimulates the production of estrogen D. is produced by the developing gonads E. A, B, and C 41. Metabolites and gasses travel from the mother to the developing embryo through the layers of the uteroplacental circulatory system in this order: A. synctiotrophoblast, trophoblastic lacuna, cytotrophoblast, extraembryonic mesoderm, chorionic blood vessels B. trophoblastic lacuna, cytotrophoblast, syncytiotrophoblast, extraembryonic mesoderm, chorionic blood vessels C. chorionic blood vessels, extraembryonic mesoderm, syncytiotrophoblast, cytotrophoblast, trophoblastic lacuna D. trophoblastic lacuna, syncytiotrophoblast, cytotrophoblast, extraembryonic mesoderm, chorionic blood vessels - This question will be on the test. Memorize the answer… I have no good suggestions. E. chorionic blood vessels, extraembryonic mesoderm, trophoblastic lacuna, synctiotrophoblast, cytotrophoblast 42. The chorionic membrane consists of: A. epiblast, cytotrophoblast, and syncytiotrophoblast B. hypoblast, cytotrophoblast, and syncytiotrophoblast C. extraembryonic mesoderm, cytotrophoblast, and syncytiotrophoblast - The chorionic membrane is part of what becomes the placenta. A is wrong because the epiblast becomes the baby. B is wrong because the Hypoblast becomes the yolk sac, not the placenta. D is wrong because the Heuser’s membrane comes from the hypoblast which will develop into the yolk sac D. Heuser’s membrane, extraembryonic mesoderm, and cytotrophoblast 43. The process of gastrulation causes: A. the formation f the primary ectoderm (epiblast) B. the formation of the extraembryonic mesoderm C. the formation of the definitive endoderm - Gastrulation is the process through which the epiblast differentiates into the 3 germ layers. A is wrong because it is the epiblast itself that is undergoing gastrulation. B is wrong because gastrulation forms the layers that will become the baby, not extraembryonic layers. D. B and C E. A, B, and C Anatomy K-Coop: 2003 Exam 1 Explained 17 of 20 44. The layers of the trilamina germ disc are formed from the: A. epiblast - Again, if you know anything, know this: the epiblast undergoes gastrulation to form the three primary germ layers. Epiblast = baby. Enough said B. hypoblast C. epiblast and hypoblast D. embryoblast and hypoblast E. cytotrophoblast 45. Which statement best describes the development of the neural tube? A. it develops directly from the primitive streak. B. it develops directly from the notochord. C. it develops from the ectoderm immediately dorsal to the notochord. D. it develops from the ectoderm immediately dorsal to the primitive streak. E. none of the above. A. incorrect; the primitive streak forms at the beginning of gastrulation during which the three germ layers – ectoderm, mesoderm and endoderm – form, and then it disappears. Neurolation occurs after gastrulation; this is when the neural tube forms. So the neural tube cannot directly form from the primitive streak. B. incorrect; the notochord induces the formation of the neural tube. The neural tube forms from the invagination of the ectoderm. C. correct; the notochord induces the ectoderm right above it to invaginate and form the neural tube. D. incorrect; the primitive streak regresses caudally by the end of gastrulation, and by day 26 it completely disappears. 46. Which of the following statements regarding neural crest cells are correct? A. cranial neural crest cells can give rise to cartilage and bone, but spinal (trunk) neural crest cells do not. B. cardiac neural crest cells give rise to the truncoconal septum of the heart. C. in humans, cranial neural crest cells begin to migrate prior to neural tube closure. D. all of the above. A)correct: cranial neural crest gives rise to i)dermal bones of skull ii)truncoconal septum iii)pharyngeal arch cartilages iv)odontoblasts v)some cranial nerve ganglia, while spinal neural crest produces i)preaortic ganglia, ii)adrenal medulla and iii)dorsal root ganglia and chain ganglia. Together (spinal and cranial) they also produce glial cells, schwann cells, enteric ganglia and melanocytes. B) correct; critical components of the truncoconal septum are derived from the cardiac neural crest cells. Both the quail-chick chimera and the cell tracing experiments support this. C. correct; the cephalic neural crest cells associated with the developing brain begin to detach and migrate before closure of the cranial neuropore (opening of the neural tube), even while the neural folds are still widely open. In the spinal cord portion of the neural tube, the neural crest cells detach as the lateral lips of the tube fuse. Some neural crest cells at the caudal end of the neural tube are produced even after the caudal neuropore closes on day 26. Thus, detachment and migration of the neural crest cells occur in a craniocaudal wave, from Anatomy K-Coop: 2003 Exam 1 Explained 18 of 20 the mesencephalon to the caudal end of the spinal neural tube. (pg89 Human Embryology, 3rd Ed.) 47. The muscles of the limbs are derived from: A. neural crest mesenchyme B. splanchnopleuric mesoderm C. intermediate plate mesoderm D. paraxial mesoderm E. somatopleuric mesoderm A. incorrect; see question 46 for what neural crest cells do. B. incorrect; splanchnopleuric mesoderm (from lateral plate meso) forms the mesothelial covering of visceral organs C)incorrect; intermediate plate mesoderm forms urinary and genital systems. D) correct; paraxial mesoderm forms the axial skeleton, voluntary musculature, etc. E)incorrect. 48. During weeks 6 to 8, the lower limb will rotate A. laterally 180 degrees B. medially 90 degrees C. medially 180 degrees D. laterally 90 degrees The upper limbs rotate laterally 90 degrees, whereas the lower limbs rotate medially 90 degrees; they both rotate 90 degrees. 49. Which of the answers below correctly describe the number of cervical sclerotomes, vertebrae, and spinal nerves, respectively? A. 8, 8, and 8 B. 8, 7, and 8 C. 7, 7, and 7 D. 8, 8, and 7 E. 7, 8, and 7 Memorize this. See fig 4-3, pg 83 in Human Embryology, 3rd Edition, for how it works out. 50. The dorsal muscle mass (derived from the myotome) in the lower limb forms what type of muscles? A. extensors and abductors B. extensors and supinators C. flexors and pronators D. flexors and adductors Anatomy K-Coop: 2003 Exam 1 Explained 19 of 20 First, dorsal mass gives rise to extensors while ventral mass gives rise to flexors in both upper and lower limbs. Second, remember your legs turned 90 degrees medially during weeks 6 through 8. So before it turned, your toes were pointing in opposite directions (rotate 90 degrees laterally to get to the position) and your heels were together. Now your quads (extensors) and abductors are somewhat backwards (pointing lateral and posterior) – aligned with the dorsal muscle mass! 51. Sclerotomes give rise to the A. vertebral arches B. vertebral bodies C. costal processes D. A and B only E. A, B, and C Sclerotomes give rise to vertebral arches, vertebral bodies, base of the skull, costal processes and ultimately ribs (in thoracic region). 52. The femur bone develops from which of the following? A. somite mesoderm B. somatopleuric mesoderm C. intermediate mesoderm D. splanchnopleuric mesoderm E. sclerotome mesoderm A) incorrect; forms limb musculature. B)correct; gives rise to bones, tendons, ligaments and vasculature of limbs. C)incorrect; forms urinary system. D)incorrect; forms mesothelial covering of the visceral organs. E) I don’t know what this is…I don’t think it exists. 53. The carpal bones A. ossify before birth via endochondral ossification B. ossify before birth via mainly membranous ossification C. ossify after birth via mainly membranous ossification D. ossify after birth via endochondral ossification All bones of both the upper and lower limbs undergo endochondral ossification. Smaller carpel and tarsal bones ossify after birth. Intramembranous ossification occurs in the frontal and parietal bones of the cranium. The clavicle, however, undergoes both membranous and endochondral ossification. 54. Thalidomide A. disrupts limb development between 20 and 25 weeks. B. disrupts cell adhesion and angiogenesis in the developing limb. C. disrupts apoptosis in the necrotic zones of the developing limb. Anatomy K-Coop: 2003 Exam 1 Explained 20 of 20 D. A and B E. A and C Thalidomide exerts its effects only when taken during the sensitive period of limb morphogenesis, between about 4 and 8 weeks. It is thought to desrupt cell adhesion in the limb by downregulating cell surface adhesion receptors (integrins and selectin) or by inhibiting angiogenesis.