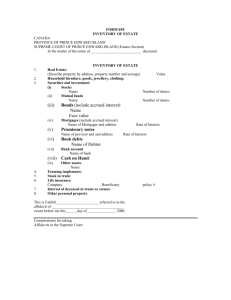
Estate Health - Ministry of Health, Nutrition Development
advertisement

1 HEALTH SERVICES DELIVERY 1.5 PROGRAMME FOR VULNERABLE POPULATIONS 1.5.1. Estate Health (as of March 2008) A Focal Point B Implementing Agencies C Target Areas & Beneficiaries Estate & Urban Health Unit, Ministry of Healthcare & Nutrition Ministry of Healthcare & Nutrition, Provincial Health Ministries of Central, Uva, Sabaragamuwa, Southern, Western and North Western Provinces. Total plantation population residing in tea, rubber & coconut estates in Central, Uva, Sabaragamuwa, Southern, Western and North Western provinces. Project Summary: The policy of the Government of Sri Lanka / Ministry of Healthcare & Nutrition is that the health services in the estate sector should be integrated into the National Health System to be on par with that of other parts of the country. The project is to improve the accessibility, availability and quality of curative care, preventive care and other public health services provision of the National Health Delivery System to the community residing in the estates to be implemented through Provincial Health Authorities. The populations benefited will not only the larger estates which are managed by private companies and SSPC & JEDB but of small holdings. The major output will include improved accessibility, availability and quality of curative, preventive and other public health services, improved health services utilization, community participation and research and its application for effective and sustainable service to the population residing in the plantation estates. 1. Justification Plantation sector is the single most important contributor to the balance of payments contributes directly and indirectly to the G.N.P. There are more than 220,000 families with about 930,000 members residing on the plantation within 6 provinces. The sector employs more than 330,000 people directly. 95% of them are labour force predominantly female workers. Most of the plantation communities are descendent of migrant from South India over 150 year ago. They were confined socially and economically to the plantation industry. The estates reminded as enclave with their system of health provision determined by the planters health scheme, which fulfilled the requirements of the ordinance which had been enacted in early part of the twentieth century with the service provision of 78 hospitals and 645 dispensaries in the estate sector, subsidized by the state with free drugs. Then health indicators for the estate population were better than the national average. Later the estate services were not considered as part of the national system after the disenfranchisement of the estate community in 1948. The administrative reports of the health department do not contain any reference to this sector after 1949 although free drug subsidy continued. There had been a progressive run down of facilities in seventies. Estate hospitals and dispensaries were not maintained, number of qualified medical personals was reduced and unqualified personals were deployed by the management to treat the sick estate workers and their families. Plantation wages were also declined in real terms. The workers families are housed in single room units provided by the management which are in unsatisfactory condition without ventilation, space, privacy and access to safe drinking water or water sanitation facilities. Lack of food security, landlessness, geographical isolation from country main stream and prolonged labour work in unfavourable environment influence their poor nutritional status and childcare practices & ill health of the families and community as a whole. Hierarchical system and social class system still existing in the plantation sector limit the development individually and socially for the development of healthy life style. The citizenship and right to vote were granted in this community subsequent to the devolution of political power to the provincial council in 1987, by which the provision of basic healthcare services to all citizens including the plantation workers is the responsibility of the Ministry of Health and the Provincial Health Authorities with community participation. The Health status of the plantation population is below the general population. The morbidity and mortality, specially the maternal and infant mortality are reported to be higher than the rest of the country due to socio economical inequity and disparity in service provisions. The government health services are far and difficult to reach. Estate workers tend to be dependent on the managers of the company for healthcare due to the patron, client relationship developed in the colonial period. Healthcare facilities are not available to the non-workers, their families, handicapped and elders living in the estates. Emergency care needs are high due to injuries and accidents and lack of MCH care. Care for emergencies tend to be delayed because of lengthy decision making process, involving family and management. Manager of the company needs to agree as it is an emergency to arrange transportation to the nearest government health facilities. Family planning services are inadequate in quality and coverage due to lack of integration of the services into the National Health System. The most neglected are the people living in small individual estates. They are not provided with healthcare by the companies, while the government health facilities are far and difficult to reach. The cost of transport, loss of days earning, language barrier and attitude of staff are the main factor influencing their poor healthcare seeking behaviour. The policy decision was taken by the government in 1990 to integrate the estate health services into the National Health System and to upgrade the health facilities to the estate population under provincial health authorities to be and par with that to other citizen in the country. As initial process of taking over the estate health services into the National Health System, 57 AMOO were trained and appointed to 54 estate health institutions with creation of new cadres for estate AMOO, under the Ministry of Health and their functions supervised by the Provincial Health Authorities. New ambulances and medical equipments supplied, building and facilities reconstructed through donors as well as state funded programmes. 50 PHM were recruited and trained by Ministry of Health, employed under the estate management and supervised by the MOOH. Recently additional MOH, PHI & PHM areas were demarcated to include the estate areas and most essential cadres of MOOH, PHMM, PHII, PHNS and other preventive sector cadres for estate areas were created under the Provincial Health Ministry. MCH, family planning, school health and other public health programmes are implemented by the Provincial Health Authorities. 2. Important Assumptions/ Risks/ Conditions 22 estate health institutions out of ear marked 50 institutions for upgrading have been taken over under provincial health administration from year 1995 to 2004. Some of these institutions are not able to function to the expected level because the basic facilities are not upgraded yet. There are issues related to the procedures in handing over and taking over were not satisfactorily followed and funds were not provided to the Ministry of Health for the upgrading of the facilities. The funds identified in other ministries for these purposes did not given the expected result. These constrains should be rectified and the past experienced to be considered when take over the balance 28 ear marked hospitals to the optimum benefits of the target population. There are barriers and obstacles to carry out health programme with community participation and supervision by the provincial health staff. There are shortages of qualified PHMM and PHII and other PHC staff to work in the language of the population. The PHMM employed by the company management are not providing healthcare to the non workers families living within the plantation areas and at the same time the PHMM and other MOH staff employed by Provincial Health Authorities have difficulties to reach these people and find places to reside and work . 3. Project Objective Objective Indicators To improve the accessibility, availability and quality of curative, preventive and other public health services of the NHS to the residential population in the plantation area on par with that in other area % of staff available to preventive and curative service provision to the national norm. % upgraded services % of health programmes coverage Health status indicators. Means of Verification HIS Review reports of RDHS Review reports of MOH Review reports of heads of upgrading institutions. Monitoring supervisions. Reports from community. 4. Project output / Product Outputs Indicators Means of Verification No of institutions upgraded Utilization rates of the institution Availability of proposed staff Availability of proposed other infrastructure facilities for patient care to the planned level Essential facilities for the staff. % of population covered. Review reports of RDHS Review reports of Head of the upgrading institution. Monitoring supervisions. Developed preventive and public care services by improved accessibility availability and quality on equitable basis. Availability of proposed staff % coverage of planned clinics and programmes to the targeted population in identified locations. Review reports of RDHS Review reports of MOH Monitoring supervisions. Improved community participation in healthcare development. % of planned programmes implemented with community and families in decision making process. % of health committees in estates. % of hospital development committees in estates. Reports of RDHS, MOH and heads of institutions. Reports from community. Surveys Improved accessibility availability and quality of curative care services. Improved health seeking Hospital utilization rates, behaviour and utilization Prevalence of selected health of health services using seeking behaviours. behaviour change communication. Occupational safety standards maintained in field and factory by the estate management and workers. No of estates and factories maintained occupational standards and field safety measures Rate of injuries treated hazards reported Management Information Number of divisions linked to System of the Estate sector the Management Information established. system Hospital Statistics Behavioural surveillance Returns and records of MOOH/ hospitals Workers awareness surveillance. Public complains Records 5. Related Projects: Project No. Project Title All the Primary Health care projects to the population in the country. 6. Relevant Agencies to be Coordinated: Provincial Health Ministries of Uva, Sabaragamuwa, Western, Southern and North Western 7. Monitoring & Evaluation: 1. Who? 2. When? Estate & Urban Health Unit, MDPU, PDHS, RDHS, RE, MO/MCH Monthly, Quarterly, Annually 8. Activities: 1 Activities Expected Results Conduct a situation analysis of Base line information the health services received by of availability of health care the plantation population. facilities, staff position, available services and pattern of use. Process Indicators Develop the TOR. Develop the detailed protocol. 2 Prepare an action plan for the Efficient, effective and District group formed, integration of estate health into sustainable district action action plan formulated and district health system. plan formulated for the approved. integration of estate health services. 3 Carryout advocacy and Estate Health plan Identify target group awareness on the Estate Health implemented by provincial Develop the programme integration into district health health authorities. system. 4 Provide the necessary facilities Hospitals are functioning with Identify requirements for for the curative care services by proposed staff, facilities and up grading selected hospitals. equipments to the planned level of upgrading. Residential facilities to the staff repaired/ rented/ new building. each institutions. Develop proposals. Approval from provincial authorities. 5 Conduct monthly medical clinics and arrange a system by which outreached services are provided by qualified MO to see the problematic patients. 6 Provide oral health care by Oral health care establishing outreached dental services established. services and upgrading existing clinics. Identify the locations. Develop the proposals. 7 Establish an effective referral Effective referral system between Primary care system established. institution and other health care institutions. Identify areas. Develop proposals. Approval from provincial authorities and Ministry of Healthcare & Nutrition. 8 Establish additional MOH units according to the national standard in order to strengthen the Primary Health Care Services. Identify areas. Develop proposals. Approval from provincial authorities. 9 Develop centers to provide PHC packages delivered Develop proposals antenatal, natal and post natal equitably to the population in Approval from provincial care in areas that does not have the estates. authorities. well established centers 10 In service training to health staff Improved quality of serving to the plantation service provided to population. plantation population. 11 Organization of health committees and hospital development committees in estate areas. Strengthen the Monitoring and evaluation system for estate health services development in central and regional level. 12 Specialist services/ outreached Identify locations. services Develop proposals. provided to the estate population. Functioning standard Health Units established with proposed staff, clinic facilities, vehicle and living accommodation for the staff. the Situation analysis to the identify target group and develop the programme. Improved community Functioning health awareness and participation. committees and hospital development committees in estate areas. Strengthen the process of Develop data estate health service information system development. at MOH, RDHS and central level. Periodic monitoring supervision