Improving Physical Examination Skills

Running head: IMPROVING CLINICAL SKILLS 1
Improving Clinical Skills
An Integrated, Transformative Approach for Preclinical Students
Amanda J. Kocoloski, OMS IV
Ohio University Heritage College of Osteopathic Medicine
IMPROVING CLINICAL SKILLS 2
Why change the current Clinical Skills course?
Rationale:
Self-reflection and informal feedback from colleagues and preceptors who have interacted with OU-HCOM students on a regular basis have raised concerns about the effectiveness of the current, largely transmissive Clinical Skills curriculum. If educating students in physical examination is going to occupy time in the formal curriculum at our school, requiring time and effort from students, faculty, and support staff, why not make it into an integrated student-directed learning experience? Currently Clinical Skills labs are predominantly lecture based, with the lab session leader often relying heavily on PowerPoint to provide information covered in the required reading material. Only about a quarter of the lab time is devoted to skills practice, and this is often extremely informal, poorly organized and inefficient.
This proposal suggests a different approach. At the center of the new program is organized interaction between instructors and learners, using technology such as faculty video demonstrations, Blackboard and audience response systems to assess what learners know prior to the session and construct the learning activities appropriately. By adapting the sessions to the learners’ preparation, positive reinforcement will be provided to those completing the required work prior to class. Only reviewing the difficult or poorly understood topics with didactic instruction will leave more time for organized role-playing between learners, supervised by instructors. In class assessment tools such as writing down the muddiest point will give the instructors the opportunity to direct students to further resources for clarification and modify future activities. Assessment will be longitudinal, instead of hinging on one performance at the end of the quarter as was previously the case. With the Clinical Skills course also encompassing clinical and community experiences (CCEs) and osteopathic manipulative medicine (OMM)
IMPROVING CLINICAL SKILLS 3 training, learners have the opportunity to refine the history and physical skills they develop in the real world (CCEs) and tie it into the their longitudinal osteopathic education. At this time, these changes are directed towards the year I course. While they would be beneficial to the year II students as well, the year II course currently uses simulation and standardized patients heavily, and it is significantly more learner-centered. As a result the planned change will be implemented in the year I course, with subsequent attention to the year II course after successful implementation in year I.
For the past ten years, clinical skill development has been considered a universal learning outcome for medical education (Issenberg & McGaghie, 2002). While it may be ideal, it is not currently feasible to instruct students individually. However, there are steps that can be taken to tailor a group learning experience to more adequately meet individuals’ needs. Audience response systems have already been used to provide feedback and direction to help basic science courses address the ACGME core competencies (Gregory, Lachman, Camp, Chen & Pawlina,
2009). In the proposed course, the audience response system will be used to administer assessments at the beginning of lab sessions to not only reinforce the need to complete required preparatory activities but also help reduce didactic time and use lectures to target areas of learner deficiency. With less time spent in didactic instruction during these lab periods, there will be more time for students to use active learning to practice implementing the skills by role-playing sample cases. Even though there is significant variability in faculty assessment of student clinical performance through observation (Kogan, Conforti, Bernabeo, Iobst & Holmboe, 2011), having instructors present to offer formative feedback to learners on their performance is essential to the training process (Issenberg & McGaghie, 2002). Finally, regularly employing standardized patients who are helpful in the transition to working with real patients, particularly
IMPROVING CLINICAL SKILLS 4 when dealing with potentially sensitive issues (Barrows, 1993), will reinforce patient care skills and emphasize empathy and effective communication.
Where are the current deficiencies?
Needs Assessment Plan:
Distribute electronic surveys to students in the classes of 2012 and 2013, as well as to the clinical skills instructor of record, years I and II liaisons, primary care associates, and clerkship site assistant deans to assess competency and confidence in PE skills of incoming year III students (see Appendix)
Contact the office of Community and Clinical Experiences (responsible for scheduling clinical time for years I and II students) for names of clinical preceptors from the community who work with preclinical students on a regular basis (e.g. monthly); hold lunchtime focus group with these preceptors
Randomly sample taped encounters from 2011 summer curriculum full history and physical examinations from the class of 2013 prior to their departure for their clinical training sites. Evaluate for completeness and correctness of basic physical examination maneuvers
Perform a literature search on the topic of physical examination instruction at allopathic and osteopathic schools, including self-directed learning, integration of case-based learning, and effective assessment
Survey colleagues from other schools to assess their perceived competency and competence in PE skills prior to year 3; investigate programs with highly positive results
IMPROVING CLINICAL SKILLS 5
What are the mission, vision and values of the proposed curriculum?
Mission:
The Ohio University Heritage College of Osteopathic Medicine Department of Family
Medicine will oversee the proposed program. The mission of this department is:
to serve as role models and teachers of undergraduate medical students at all levels of training;
to serve as trainers of postgraduate physicians;
to provide clinical services to the residents of southeastern Ohio; and
to advance research done in the setting of an osteopathic medical college
Vision:
Learners will emerge from the Clinical Skills course proficient and confident in the fundamentals of history taking and physical examination, using open and empathic communication with patients.
Values:
The Clinical Skills curriculum teaches patient history taking and osteopathic physical examination, as they are essential in the training of a competent osteopathic physician.
However, the goals of the program do not end there. Fostering the development of effective communication, integrity, empathy, compassion, professionalism, and a concern not only for the patient’s physical well being but for the individual’s emotional and psychological health as well, are core values of the program. This holistic, patient-centered approach lends itself to the training of excellent osteopathic physicians.
IMPROVING CLINICAL SKILLS 6
How will this change be approved?
Governance Plan:
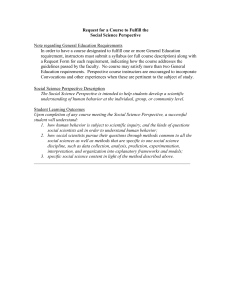
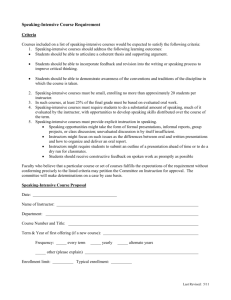
The curriculum approval process at OU-HCOM is outlined in the diagram below, with the
Clinical Skills portion enlarged. After discussing the proposed changes with the Clinical Skills
Instructor of Record, this modified curriculum would fit within the current broad framework and it would not be necessary to go through the formal change approval process. In order the implement the changes, the following steps will be taken:
Attend a monthly meeting of the Clinical Skills Committee this fall
Present the new format for labs in general, addressing notable details for any specific lab sessions
Answering committee questions, hearing and following up on suggestions
Adjusting the syllabus accordingly
Pilot with a lab this year with the class of 2015; if successful, plan for widespread implementation for the entering class of 2016
IMPROVING CLINICAL SKILLS
QuickTime™ and a
None decompressor are needed to see this picture.
QuickTime™ and a
None decompressor are needed to see this picture.
7
IMPROVING CLINICAL SKILLS 8
Who will be teaching, who will be learning, and in what context will the education take place?
Instructors:
Instructor of Record: Nicole Wadsworth D.O.
Dr. Wadsworth received her D.O. degree from Ohio University in 1997. She is currently the OU-HCOM Associate Dean of Preclinical Education in addition to the Director of the
Emergency Department at O’Bleness Hospital in Athens, OH.
As a part of Generation X she personifies the emphasis on a balanced life. Despite multiple career obligations, she routinely participates in 5Ks and triathlons and is seen regularly at community events.
Respected by students and colleagues as hard working but still approachable, Dr.
Wadsworth manages the role of both instructor and disciplinarian. Her presentations rely on learner interaction rather than PowerPoints, and she strongly promotes discussionbased sessions.
Informal collaboration with Dr. Wadsworth during the development of this curriculum plan was positive and helpful. She clearly values learner-centered education and expressed excitement over the proposed changes.
Clinical Skills Liaisons
Year I: Martha Simpson, D.O. o Previously Dr. Simpson was a nurse. She received her D.O. degree from
Kirksville College of Osteopathic Medicine in 1978, and her MBA from Ohio
University in 2000. In addition to her academic duties, she works in urgent care and is the school’s Director of HIPAA Compliance.
IMPROVING CLINICAL SKILLS 9 o Dr. Simpson is an exception to the rule. Despite being from the middle of the
Baby-Boomer Generation, she strongly values a balanced life with family as opposed to endorsing a workaholic perspective. She regularly takes vacations abroad with her family, and works hard to make sure her career obligations do not interfere. o Although intimidating to many year I students, she is clear about her expectations.
She endorses the use of technology by those proficient in its use, but does not branch into many different modalities alone. Dr. Simpson’s goal is to teach year I students to recognize normal physical exam findings. o Dr. Simpson gives the instructors flexibility when leading lab sessions, and would be amenable to implementing these proposed changes. Although I envision some skepticism on her part regarding how effective the new format will be in engaging students, I feel positive evaluation of the curriculum from learners would bring her fully onboard.
Year II: Maureen Clothier, D.O. o Dr. Clothier received her D.O. from the College of Osteopathic Medicine and
Surgery in Des Moines, IA in 1984. Although board certified in internal medicine, she has tailored her practice towards the care of the geriatric patient as she works in a geriatric practice and is the medical director of a local nursing home. o Although probably bridging the Baby-Boomer and X Generations, Dr. Clothier falls more into the Baby-Boomer category. She values family but often has to work late and never seems to mind taking on more responsibility.
IMPROVING CLINICAL SKILLS 10 o Dr. Clothier is strict. Students view her as disciplinarian, and one who values adherence to established rules and does not accept excuses. She holds students to high expectations she felt held to as a student. One deviation from the classic
Baby-Boomer is her eagerness to use technology in her teaching. o While her goals are learner-centered, she seems more comfortable handling details of instruction herself. With the amount of work the new curriculum will entail, especially at the beginning, this may be overwhelming. Support from other instructors will be important in making the workload manageable.
Primary Care Associates (PCAs)
I fall into this category. With the current class size of 140 students, three PCAs serve the student body year-round. Many of us are female with fewer than 25% being male in the past 5 years. My colleagues and I belong to the Millennial Generation and fit many of the generalities presented in this week’s material (“people people” who value interpersonal relationships, love technological advances, strive for perfection, but sometimes become overwhelmed with our endeavors and slip easily into a sense of entitlement). In being assistants to the IoR and Years I and II liaisons, we often adapt to and occasionally adopt some of their Baby-Boomer and Generation X mentalities.
Learners:
The entering class of 2016 will be the first group of students to go through the proposed curriculum. While this group has not yet been formed, data on the previous two entering classes is available:
IMPROVING CLINICAL SKILLS 11
Class of 2014
Approximately 120 students
84% from Ohio
15% from Ohio Appalachian counties
26% minority populations
58% female
Class of 2015
Approximately 140 students
84% from Ohio
14% from Ohio Appalachian counties
24% minority populations
45% female
Classes of 2014 and 2015
Both classes have the vast majority of students from the Millennial Generation, with a few Generation X students interspersed. There are several students with previous healthcare experience, with backgrounds as everything from patient transporter and nurses’ aide to pharmacist and physician assistant.
These groups fit the millennial mold very well. They are eager to learn interactively by doing and are largely respectful but will question authority. A group of high achievers, they strive for perfection and are extremely comfortable with using technology. There have been occasions where they have taken inappropriate venues to address concerns and often express or imply entitlement to the biggest and the best there is to offer. A common concern is the maintenance of professionalism and patient confidentiality when using social networking sites like facebook and twitter.
Context/Structure/Organization:
Clinical Skills is a longitudinal course for both year I and II students, operating through the Department of Family Medicine (DFM). Part of the DFM’s missions statement is to educate undergraduate medical students of all levels, and this includes preparing them for clinical
IMPROVING CLINICAL SKILLS 12 clerkships where they will be evaluated according the AOA Core Competencies. The course is not only composed of Clinical Skills labs. Osteopathic manipulative medicine, Case-Based
Learning (CBL) for students in the lecture based curriculum (CPC), and Clinical and Community
Experiences (CCEs) where students are out with community healthcare providers observing and practicing their physical diagnosis skills are included in Clinical Skills as well. All of these activities are mandatory. The Clinical Skills committee reports to the steering committees of both main curricula at OU-HCOM monthly (PCC and CPC).
For Clinical Skills labs students meet on average once a week (Tuesday or Thursday) for two hours, in the OMM lab or in the Clinical Training and Assessment Center (CTAC). The instructor/learner ratios are 1:6 and 1:7 for the classes of 2014 and 2015 respectively. The majority of the time the instructor leading the session is one of the liaisons or a PCA, but support instructors come from throughout the school’s adjunct faculty. There is some variability in the setup of the Clinical Skills lab sessions, but the majority of them ultimately have about 75-90 minutes of didactic learning with one session leader going through a PowerPoint, and then 15-30 minutes of poorly structured practice time. For example, in the past the medical instrumentation lab has consisted of the session leader explaining 50 PowerPoint slides, interjecting anecdotal stories when relevant. After about 90 minutes, the students organize themselves into groups of two or three, chat for about five to ten minutes, then practice the skills demonstrated by the session leader for about ten minutes as instructors walk around the room to answer questions.
Students often go through the motions once, and then leave the lab five minutes before the official end time.
Currently there is also a great deal of variability in learner assessment, with the methods depending on individual instructor preference. Some instructors will prepare paper and pencil
IMPROVING CLINICAL SKILLS 13 quizzes to assess preparation, but currently the outcome of these quizzes do not impact the course of the session. Essentially observation of learner performance by a faculty instructor during a standardized patient encounter at the end of each quarter determines whether the student passes or fails the course.
What are the broad and specific goals, and how will learners be assessed to determine competency?
National Standards:
Learners completing the Clinical Skills course will be prepared for the next level of training, specifically clerkships during their third and fourth years of medical school. The following items were taken from the OU-HCOM Evaluation of Student Clinical Performance, which is based on the seven AOA Core Competencies for osteopathic residents. Specifically, the curriculum will influence learner performance in the Patient Care domain.
Osteopathic Philosophy and Osteopathic Manipulative Medicine o Understanding and awareness of the appropriateness of OMM
Medical Knowledge o Knowledge of established and evolving biomedical, clinical, and social sciences
Patient Care o Compassionate, appropriate and effective for the promotion of health, prevention and treatment of illness, and end of life
Interpersonal and Communication Skills o Interpersonal and communication skills to establish professional relation
IMPROVING CLINICAL SKILLS 14
Professionalism o Behaviors reflect continuous professional development, ethical practice, sensitivity to diversity, and responsible attitude toward patients, profession, and society
Practice-Based Learning and Improvement o Use scientific evidence and methods to investigate, evaluate, and improve patient care practice
Systems-Based Practice o Understanding of the contexts and systems in which health care is provided
Learning Outcomes, Performance Indicators, Teaching Methods and Corresponding
Assessments:
Learning Outcome: At the end of the course, students will be able to obtain an organized, thorough medical history
Performance Indicators
At the end of the session, students will be able to:
List the components of the medical history
Teaching Methods
Required reading, discussion of difficulty or sensitive topics (e.g. sexual history)
Assessment Tools
Online Blackboard quiz prior to lab session
Schedule
(See Clinical Skills schedule)*
Prior to lab session 1
Take problem-focused and comprehensive medical histories
Role-play with partner, standardized patient encounters, tape review with instructors
Instructor check-off sheet for role-play and standardized patient encounters
Sessions 1, 5, 6, 9, 10, 13
& 14
Learning Outcome: At the end of the course, students will be able to perform an organized, focused physical examination based on the chief complaint using correct technique
Performance Indicators
At the end of the session, students will be able to:
Take temperature, blood pressure, pulse, respiration rate
Examine head, eyes, ears, nose and throat; inspect, auscultate, and palpate patient’s neck
Teaching Methods
Required reading, instructor demonstration of difficult maneuvers, roleplay with partner
Required reading, instructor demonstration of difficult maneuvers, roleplay with partner
Assessment Tools
Pre-assessment:
Audience Response
System Quiz
Post-assessment:
Instructor check-off sheet for role-play
Pre-assessment:
Audience Response
System Quiz
Post-assessment:
Instructor check-off sheet for role-play
Schedule
(See Clinical Skills schedule)*
At the beginning of session 2 prior to instruction
At the conclusion of session 2
At the beginning of session 3 prior to instruction
At the conclusion of session 3
IMPROVING CLINICAL SKILLS 15
Examine chest by inspection, auscultation, palpation and percussion
Inspect, auscultate, palpate and percuss the abdomen
Perform a musculoskeletal examination, using osteopathic screening, scanning and segmental definition techniques; inspect and palpate the vascular and lymphatic systems
Required reading, instructor demonstration of difficult maneuvers, roleplay with partner
Required reading, instructor demonstration of difficult maneuvers, roleplay with partner
Required reading, instructor demonstration of difficult maneuvers, roleplay with partner
Pre-assessment:
Audience Response
System Quiz
Post-assessment:
Instructor check-off sheet for role-play
Pre-assessment:
Audience Response
System Quiz
Post-assessment:
Instructor check-off sheet for role-play
Pre-assessment:
Audience Response
System Quiz
Post-assessment:
Instructor check-off sheet for role-play
At the beginning of session 7 prior to instruction
At the conclusion of session 7
At the beginning of session 8 prior to instruction
At the conclusion of session 8
At the beginning of session 11 prior to instruction
At the conclusion of session 11
Test mental status, cranial nerves, muscle strength, general sensation, and deep tendon reflexes
Required reading, instructor demonstration of difficult maneuvers, roleplay with partner
Pre-assessment:
Audience Response
System Quiz
Post-assessment:
Instructor check-off sheet for role-play
At the beginning of session 12 prior to instruction
At the conclusion of session 12
Learning Outcome: At the end of the course, students will be able to document subjective and objective information, assessment and management plan thoroughly, accurately and in a timely manner
Performance Indicators
At the end of the session, students will be able to:
Logically organize subjective, objective, assessment and plan sections
Complete focused SOAP note with NBOME abbreviations in 30 minutes
Teaching Methods
Required reading, roleplay with partner to collect information, construction of SOAP note
Assessment Tools
Instructor critique of
SOAP note based on standardized rubric
Schedule
(See Clinical Skills schedule)*
Sessions 4, 5, 9, & 13
Learning Outcomes: At the end of the course, students will be able to:
Analyze information gathered from patient encounters to formulate logical assessments and management plans
Summarize pertinent findings from patient encounters including assessment and proposed management plan
Performance Indicators
At the end of the session, students will be able to:
Explain findings, assessment and plan to standardized patient in lay terminology
Sessions 5, 6, 9, 10, 13 &
14
Learning Outcome: At the end of the course, students will be able to interview patients on living with a chronic, debilitating disease
Performance Indicators
At the end of the session, students will be able to:
Demonstrate empathy
Teaching Methods
Standardized patient encounters, tape review with instructors
Teaching Methods
Assessment Tools
Standardized patient assessment forms and face-to-face feedback
Assessment Tools
Schedule
(See Clinical Skills schedule)*
Schedule
(See Clinical Skills schedule)*
Sessions 15 &16
Investigate coping mechanisms
Inquire about impact on
Standardized patient encounter, tape review with instructors
Standardized patient assessment forms and face-to-face feedback daily life and relationships
Develop partnership with patient
IMPROVING CLINICAL SKILLS 16
Learning Outcome: At the end of the course, students will be able to counsel patients on treatment adherence and disease management
Performance Indicators
At the end of the session, students will be able to:
Ensure patient understanding of treatment plan
Investigate barriers to patient compliance
Teaching Methods
Standardized patient encounter, tape review with instructors
Assessment Tools
Standardized patient assessment forms and face-to-face feedback
Explore motivation for change
Develop partnership with patient
*Final Clinical Skills schedule for class of 2016 will be available during the summer of 2012
Schedule
(See Clinical Skills schedule)*
Sessions 17 &18
How will the proposed plan be implemented? What barriers to implementation are expected?
Resources:
Personnel: Pivotal individuals in the implementation of this curriculum include the
Instructor of Record, years I and II liaisons, Primary Care Associates, faculty instructors,
Clinical Training and Assessment Center (CTAC) Supervisor, and standardized patients.
During the learning experiences, a member of the technical support staff will be present to monitor and answer instructors’ computer questions, as well as troubleshoot technical problems. The department of Faculty Development will also be important for the continued support and training of instructors, particularly with regard to new technology
(e.g. recent seminar on our smartphone-mediated audience response system).
Time: The course design will be piloted in the fall of 2011, giving time for the Clinical
Skills Committee to review feedback and modify the curriculum prior to full-scale implementation in the fall of 2012. FTEs will be allotted appropriately to Primary Care
Associates and faculty instructors involved in laboratory and SP exercises to ensure protected time and compensation for contribution to the course. The lab session leader,
IMPROVING CLINICAL SKILLS 17 who has to create and revise the pre-lab assessment and didactic materials, will receive twice the credit of the other instructors. Technical support staff will be given a schedule of activities at the beginning of the semester and kept abreast of any changes to the schedule in a timely manner.
Facilities: Students will have access to Learning Outcomes and Performance Indicators prior to lab, as well as required reading materials through Blackboard. Most of the experiences will take place in the OMM lab. The lab provides sufficient space for range of group sizes for the laboratory encounters (35 to 70 students). The multiple camera angles provide all students with an up-close view during instructor demonstration of exam maneuvers. The remainder of experiences will occur in the CTAC, which was remodeled in 2011. This center has 14 standardized encounter rooms, a control room with WebSP software for learner observation, a classroom for briefing and debriefing, a skills lab for technical training and assessment, a simulation mannequin and a comfortable SP lounge and changing room.
Funding: Construction of the new CTAC was made possible by a generous grant for the
Osteopathic Heritage Foundation. Budgetary allowances in addition to the grant money make the current operations of the CTAC possible, including salary for instructors and staff, skills training and assessment with a simulation mannequin and multiple SP experiences.
Support: Internal support is most relevant to this project implementation. Collaboration throughout the planning process with the Instructor of Record, various faculty instructors and Primary Care Associates has provided multiple viewpoints and solidified buy-in from key personnel. Feedback from these individuals will continue to be crucial to maintain
IMPROVING CLINICAL SKILLS 18 this investment. The indirect external support from the Osteopathic Heritage Foundation
(see “Funding” above) helped establish an optimal learning environment, mitigating much of the financial burden of creating the CTAC.
Administration: Structures, Communication and Operations:
The Clinical Skills Committee (see “Governance” section for specifics) will implement the curriculum, receive student evaluations administered by the Curriculum Coordinator and support staff, and modify course workings appropriately. Current communication between instructors and learners regarding goals and objectives for the Clinical Skills course is critically deficient. The current method through Blackboard confuses and frustrates students, and the IT department is currently debating on how to address this issue. Whether it is through an updated Blackboard system or another mode of information delivery, logistics (when and where to meet, materials needed, etc.), as well as learning expectations for the course will be clearly communicated to all instructors, learners, and support staff.
Barriers:
Poor communication between administration/instructors and learners is currently a huge hurdle for many elements of the OU-HCOM preclinical curriculum, and the Clinical
Skills course is no exception.
o The IT department is currently investigating a new mode of electronic communication, which will hopefully be addressed prior to implementation in the fall of 2012. Clear communication is essential to the success of the new curriculum.
IMPROVING CLINICAL SKILLS 19
Unsupportive attitudes from instructors who are used to more of a didactic “sage on the stage” format can halt progress and development of the new curriculum.
o Encouraging increased involvement by resistant faculty members in the planning process (e.g. attending Clinical Skills Committee meetings) and curriculum delivery (e.g. invitation to serve as lab session leader) with appropriate compensation via the FTE system will broaden perspectives and encourage investment in the new curriculum.
The possibility for financial barriers exists, particularly as the class sizes are now approximately 140 students (40% increase in the past five years).
o Yearly tuition increase has been inevitable and will likely continue. Hopefully the required increases will be modest, with the help of external grants like the recent $105,000,000 gift from the Osteopathic Heritage Foundation.
Introduction of curriculum:
Given the flexibility built into the current Clinical Skills framework, it is feasible to implement the new curriculum with a prolonged phase-in approach. Plans have been made with the session leader to introduce the format in the year I “Abdominal Exam” lab on 11/15/11 and 11/17/11. Targeted feedback will be gathered from the learners at the end of the sessions in addition to the standard quarterly evaluation, and modifications will be made by the Clinical Skills Committee to prepare for implementation in the fall of
2012.
IMPROVING CLINICAL SKILLS 20
If the proposed curriculum is implemented, how will it be evaluated? How will the curriculum be maintained and enhanced to ensure focus and the learner and prevent stagnancy?
Program Evaluation:
Before Implementation:
Expert Appraisal
Confidential Review
Preordinate:
Analysis student of achievement
Costs
Scores on external exams
Next level’s satisfaction
Course evaluations
Quality of teaching/learning
Non-preordinate:
Interviews/Focus group
Feedback from stakeholders
Final project sent to Dr. Audrey Okun-Langlais, Professor of Family
Medicine at UNECOM, and Dr. India Broyles, Masters in Medical
Education Leadership Program Director and MEL 604 Course Instructor
Final project reviewed by Nicole Wadsworth D.O., Clinical Skills Instructor of Record, Martha Simpson D.O. and Maureen Clothier D.O., Year I and II liaisons, and current Primary Care Associates to assess feasibility, provide constructive criticism and suggestions from improvement. With his strong background in medical education Stephen Davis Ph.D., Director of Faculty
Development, also asked to review project and provide feedback
Compare class of 2016* passing rate on Clinical Skills final examination
(sessions 13 &14) and OSCE at end of year III with previous class passing rates
Track standardized patient feedback, comparing it to previous (if possible) and subsequent classes
As class size remains around 140, analyze budget to evaluate feasibility of standardized patient encounters and maintenance of instructor: learner ratio of no more than 1:7 for lab sessions
Compare class of 2016 COMLEX II-PE passing rates with those of previous classes
Review class of 2016’s performance on clerkship evaluations in the domains of Patient Care and Interpersonal & Communication and compare with previous classes’ performance in these domains
Online surveys completed by students through Blackboard. Questions focus on both course and individual instructor effectiveness, asking for suggestions for improvement
Quantitative data from online course/instructor evaluations through
Blackboard completed by students each semester
Student representatives from all lab subgroups meet once a semester for focus group run by Curriculum Coordinator
Questionnaire administered yearly to Instructor of Record, liaisons, PCAs, and lab instructors about session efficiency and asking for suggestions for improvement. When applicable, feedback from clerkship directors will also be solicited
Instructor of Record and Director of Faculty Development conduct random performance audits to evaluate instructor performance
Observations/Unobtrusive measures/Samples of work
Maintenance and Enhancement:
Understanding the Curriculum: Quarterly learner evaluations of both the curriculum and instructor effectiveness are analyzed by the curriculum program analyst and
IMPROVING CLINICAL SKILLS 21 distributed to the Instructor of Record and all instructors involved in the course. Signs of learner or instructor dissatisfaction with communication methods, facilities, or logistics of the course will be addressed. Each year the Clinical Skills Committee reviews all learning outcomes and performance indicators, ensuring topics are sufficiently covered without redundancy and congruency is maintained between the outcomes and type of performance indicators used. Primary Care Associates will have weekly open office hours when students can stop in with questions or suggestions about the course. A focus group will be held once a quarter where the Instructor of Record and years I and II liaisons will meet with faculty instructors to receive their feedback on the program.
Management of Change: Informal learner feedback during office hours and session debriefing and formal feedback through quarterly evaluations will be used to gather ideas for additional sessions (i.e. electronic health records etiquette training). The Clinical
Skills Committee will also generate ideas and discuss all the suggestions and possible plans for implementation at monthly meetings. Lab or SP sessions with negative learner or instructor evaluations will be dissected and improved with direction from the feedback. If evaluations remain negative, the committee may remove the activity from the course or attempt to meet the learning outcomes with alternate activities.
Faculty Development: Instructors will receive incentives for attending faculty development seminars (ideally CME credit). Weekly faculty development “tidbits” are dispersed in Rounds, the e-newsletter distributed to all OU-HCOM personnel and students. Training will be available on the WebSP and TurningPoint/audience response software at the beginning of each academic year, and as needed if an instructor should start working with the course after the start of the academic year.
IMPROVING CLINICAL SKILLS 22
Sustaining the Curriculum Team: The FTE system is used to provide protected time and salary to instructors who reduce their clinical practice to work with this course.
Instructors are encouraged to attend focus groups held every quarter (see “Understanding the Curriculum”) to voice opinions and those who wish to influence the course planning are invited to attend monthly committee meetings. Additionally the school will work on providing CME to instructors who participate as instructors in the course.
Networking, Innovation and Scholarly Activity: The Instructor of Record and years I and II liaisons will stay well connected with the AOA and NBOME to ensure congruence between program goals and expectations of learners at the next level. If other schools choose to adopt a similar curriculum, communication between schools regarding common barriers and solutions will increase the efficacy of problem solving efforts.
Opportunities for research and publications will be fostered as they arise (e.g. the impact of face-to-face SP feedback on student achievement of cognitive and affective learning outcomes). Primary Care Associates interested in medical education and curriculum development will be invited to conduct research and joint the Clinical Skills Committee.
If the curriculum is implemented and successful, how will this plan be disseminated to other target audiences that would benefit from the information?
Reasons for Dissemination: Dissemination would provide other schools that are dissatisfied with their current method of teaching physical diagnosis a well-constructed option for curricular change. Dissemination to graduate training programs will also hopefully promote increased awareness and attention to residents’ clinical skills competency.
IMPROVING CLINICAL SKILLS 23
Target Audience: Once the new Clinical Skills has been implemented at OU-HCOM, other allopathic and osteopathic medical schools would be suitable target audiences.
Because of the formal incorporation of osteopathic principles and practices into some of the sessions (e.g. musculoskeletal examination) and informally into many of the sessions, osteopathic curriculum developers are perhaps the most appropriate audience.
Content: The needs assessment plan, including the survey of current and recent learners, will be distributed to interested schools. A sample schedule including learning outcomes, performance indicators, and anticipated instructor, learner, and support staff requirements will be dispersed. The portion of the annual budget pertaining to the Clinical Skills curriculum will also be available upon request. Nice to see that there may be elements of the project that are important as well as the entire project.
Methods: Results of any research endeavors (e.g. the impact of face-to-face SP feedback on student achievement of cognitive and affective learning outcomes) will be presented at appropriate conferences (e.g. AAMC, AACOM, Generalists in Medical Education; for full list see http://www.oucom.ohiou.edu/fd/conferences.htm
) and submitted for publication in peer-reviewed journals geared towards curriculum development.
Information about the Clinical Skills curriculum and student feedback will be published on the school’s website and posted on the incoming class facebook group pages.
Resources: The CORE Research Office ( http://www.ohiocore.org/research/ ) is an excellent resource for all OU-HCOM students, providing advice on research topic selection, guidance through IRB and other approval processes, and funding opportunities for research, travel and results publication. The Office of Faculty Development
( http://www.oucom.ohiou.edu/fd/ ) aids in providing the process of networking with other
IMPROVING CLINICAL SKILLS 24 schools and organizations. Finally the Office of Medical Informatics (OMI- http://www.oucom.ohiou.edu/omi/ ) will help place information regarding the curriculum on the OU-HCOM website.
IMPROVING CLINICAL SKILLS 25
Appendix I: Needs Assessment Instrument
This survey will be distributed to the classes of 2012 and 2013, as well as colleagues from other schools (with minor adaptations in terminology)
For each of the following items, please indicate your response based on the following scale:
1- Strongly disagree 2- Disagree 3- Neither agree nor disagree 4- Agree 5- Strongly Agree
1. At the end of year II, I was confident in my physical examination skills.
1 2 3 4 5
2. I learned the majority of my physical examination skills during Clinical Skills labs.
3. Time in Clinical Skills labs was used efficiently.
4. I had adequate access to faculty preceptors during Clinical Skills lab time.
5. I regularly spent time preparing for Clinical
Skills labs.
6. Completing the required reading before class was important to my understanding of the material presented.
7. Integrating clinical cases would be an asset to Clinical Skills labs.
8. I am satisfied with the training I received in physical diagnosis during years I and II.
9. Strong physical diagnosis skills are important to me.
10. I feel prepared for the OU-HCOM and
NBOME standardized performance examinations (OSCE, COMLEX II-PE).
Please provide any additional comments:
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
1 2 3 4 5
IMPROVING CLINICAL SKILLS 26
References
Barrows, H.S. (1993). An overview of the uses of standardized patients for teaching and evaluating clinical skills. AAMC. Acad Med 68 (6), 443-51.
Berg, D., Sebastian, J., & Heudebert, G. (1994). Development, implementation, and evaluation of an advanced physical diagnosis course for senior medical students. Acad Med, 69 (9),
758-764.
Brydges, R., Carnahan, H., Safir, O., & Dubrowski, A. (2009). How effective is self-guided learning of clinical technical skills? It’s all about process. Medical Education , 43 (6), 507-
515. doi:10.1111/med.2009.43.issue-6
Chou, C.L. (2004). A fourth year medical student elective on the advanced physical examination
[Abstract]. J Gen Intern Med, 19 (s1), 83–99. doi: 10.1111/j.1525-1497.2004.S1006_2.x
Gregory, J.K., Lachman, N., Camp, C.L., Chen, L.P. & Pawlina, W. (2009). Restructuring a basic science course for core competencies: an example from anatomy teaching. Med
Teach 31 (9), 855-61 .
Haist, S.A., Griffith III, C.H., Hoellein, A.R., Talente, G., Montgomery, T., & Wilson, J.F.
(2004). Improving students’ sexual history inquiry and HIV counseling with an interactive workshop using standardized patients. J Gen Intern Med, 19 (5 Pt 2), 549-553. doi: 10.1111/j.1525-1497.2004.30204.x
Hecimovich, M.D., & Volet, S.E. (2009). Importance of building confidence in patient communication and clinical skills among chiropractic students. J Chiropr Educ, 23 (2),
151-164.
Issenberg, S.B., & McGaghie, W.C. (2002). Clinical skills training – practice makes perfect.
Medical Education , 36 (3), 210-211. doi:10.1046/j.1365-2923.2002.01157.x
IMPROVING CLINICAL SKILLS 27
Jafri, N.F., Wu, P., Stanfield, L., & Slanetz, P.J. (2008) Use of radiologic imaging to enhance physical diagnosis instruction in the preclinical curriculum . Academic Radiology, 15 (7),
942-947. doi:10.1016/j.acra.2008.01.021
Kogan, J.R., Conforti, L, Bernabeo, E., Iobst, W., & Holmboe, E. (2011). Opening the black box of clinical skills assessment via observation: a conceptual model. Medical Education , 45 ,
1048-1060. doi:10.1111/j.1365-2923.2011.04025.x
Mann, K. V. (2011). Theoretical perspectives in medical education: past experience and future possibilities. Medical Education , 45 (1), 60-68. doi:10.1111/j.1365-2923.2010.03757.x
Modica, R.F., Thundiyil, J.G., Chou, C., Diab, M., & Von Scheven, E. (2009). Teaching musculoskeletal physical diagnosis using a web-based tutorial and pathophysiologyfocused cases. Med Educ Online, 14 (13). doi: 10.3885/meo.2009.Res00301
Wenrich, M., Jackson, M.B., Scherpbier, A.J., Wolfhagen, I.H., Ramsey, P.G., & Goldstein, E.A.
(2010). Ready or not? Expectations of faculty and medical students for clinical skills preparation for clerkships. Med Educ Online, 15 . doi: 10.3402/meo.v15i0.529